

Similar Sensitivity of SARS-CoV-2 Detection in Oropharyngeal/Nasopharyngeal and Saliva Samples on the Hologic Panther Platform
 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Ethics Statement
2.2. Setting, Study Design and Participants
2.3. Sample Collection and Processing
2.4. SARS-CoV-2 Detection Using the Aptima EP-TMA SARS-CoV-2 Assay
2.5. SARS-CoV-2 Detection Using the Aptima RT-TMA SARS-CoV-2/Flu Assay
2.6. Statistical Analysis
3. Results
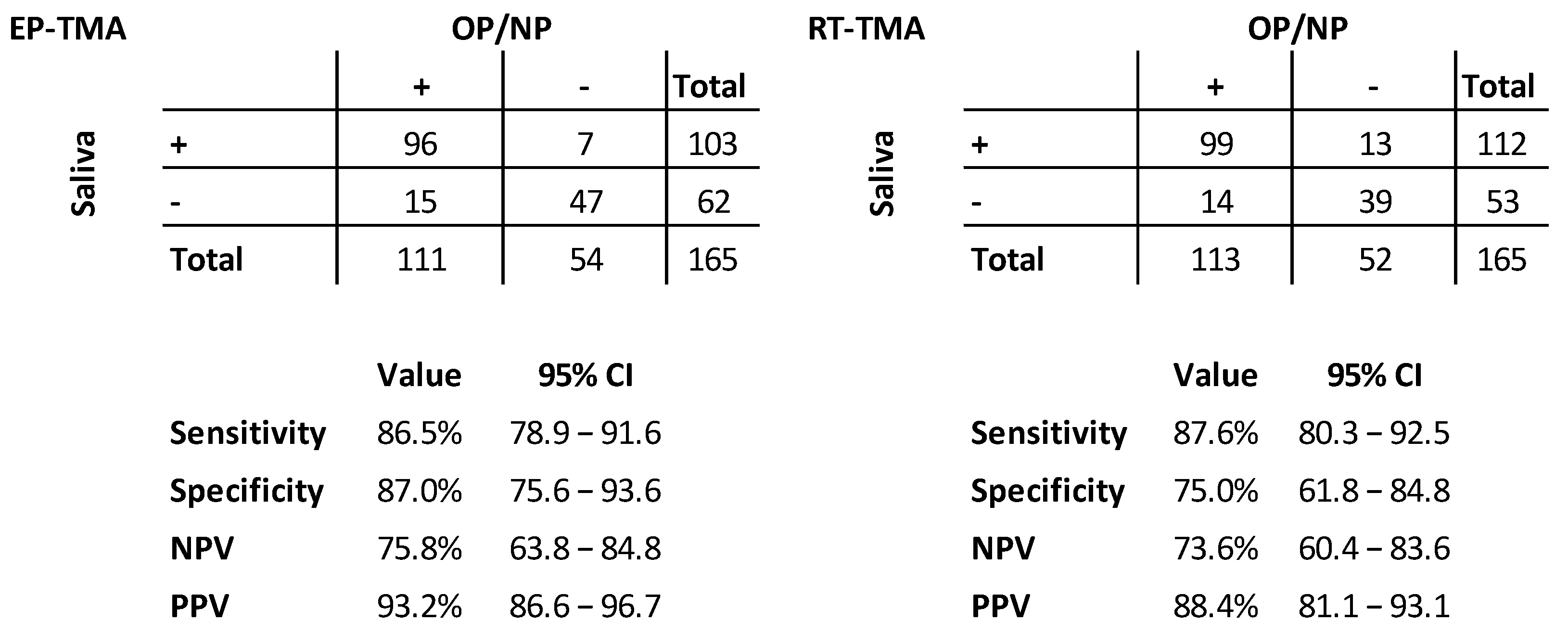
3.1. Clinical Validation Results
3.2. Discordant Analysis
3.3. Influenza Testing Results with RT-TMA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wikramaratna, P.S.; Paton, R.S.; Ghafari, M.; Lourenço, J. Estimating the false-negative test probability of SARS-CoV-2 by RT-PCR. Eurosurveillance 2020, 25, 2000568. [Google Scholar] [CrossRef]
- Lee, R.A.; Herigon, J.C.; Benedetti, A.; Pollock, N.R.; Denkinger, C.M. Performance of Saliva, Oropharyngeal Swabs, and Nasal Swabs for SARS-CoV-2 Molecular Detection: A Systematic Review and Meta-analysis. J. Clin. Microbiol. 2021, 59, e02881-20. [Google Scholar] [CrossRef] [PubMed]
- Bastos, M.L.; Perlman-Arrow, S.; Menzies, D.; Campbell, J.R. The Sensitivity and Costs of Testing for SARS-CoV-2 Infection with Saliva Versus Nasopharyngeal Swabs. Ann. Intern. Med. 2021, 174, 501–510. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, Y.; Furuchi, M.; Kamimoto, A.; Honda, K.; Matsumura, H.; Kobayashi, R. Saliva-based PCR tests for SARS-CoV-2 detection. J. Oral Sci. 2020, 62, 350–351. [Google Scholar] [CrossRef] [PubMed]
- Bland, J.; Kavanaugh, A.; Hong, L.K.; Perez, O.; Kadkol, S.S. A Multiplex One-Step RT-qPCR Protocol to Detect SARS-CoV-2 in NP/OP Swabs and Saliva. Curr. Protoc. 2021, 1, e145. [Google Scholar] [CrossRef] [PubMed]
- Bruxvoort, K.; Tenggardjaja, C.F.; Slezak, J.; Gullett, J.C.; Broder, B.; Park, C.H.; Aragones, M.; Mercado, C.; Wong, K.; McLaren, S.; et al. Variation in SARS-CoV-2 molecular test sensitivity by specimen types in a large sample of emergency department patients. Am. J. Emerg. Med. 2021, 50, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Tsang, N.N.Y.; So, H.C.; Ng, K.Y.; Cowling, B.J.; Leung, G.M.; Ip, D.K.M. Diagnostic performance of different sampling approaches for SARS-CoV-2 RT-PCR testing: A systematic review and meta-analysis. Lancet Infect. Dis. 2021, 21, 1233–1245. [Google Scholar] [CrossRef] [PubMed]
- Butler-Laporte, G.; Lawandi, A.; Schiller, I.; Yao, M.C.; Dendukuri, N.; McDonald, E.G.; Lee, T.C. Comparison of Saliva and Nasopharyngeal Swab Nucleic Acid Amplification Testing for Detection of SARS-CoV-2. JAMA Intern. Med. 2021, 181, 353. [Google Scholar] [CrossRef] [PubMed]
- Hanson, K.E.; Barker, A.P.; Hillyard, D.R.; Gilmore, N.; Barrett, J.W.; Orlandi, R.R.; Shakir, S.M. Self-Collected Anterior Nasal and Saliva Specimens versus Health Care Worker-Collected Nasopharyngeal Swabs for the Molecular Detection of SARS-CoV-2. J. Clin. Microbiol. 2020, 58, e01824-20. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html (accessed on 7 October 2020).
- Pham, J.; Meyer, S.; Nguyen, C.; Williams, A.; Hunsicker, M.; McHardy, I.; Gendlina, I.; Goldstein, D.Y.; Fox, A.S.; Hudson, A.; et al. Performance Characteristics of a High-Throughput Automated Transcription-Mediated Amplification Test for SARS-CoV-2 Detection. J. Clin. Microbiol. 2020, 58, e01669-20. [Google Scholar] [CrossRef] [PubMed]
- Trémeaux, P.; Lhomme, S.; Abravanel, F.; Raymond, S.; Mengelle, C.; Mansuy, J.-M.; Izopet, J. Evaluation of the Aptima™ transcription-mediated amplification assay (Hologic®) for detecting SARS-CoV-2 in clinical specimens. J. Clin. Virol. 2020, 129, 104541. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, D.; Sasidharan, A.; Abdulhamid, A.; Orosco, E.M.; Watts, J.L.; Schuster, J.E.; Myers, A.L.; Weddle, G.; Selvarangan, R. Diagnostic Yield of Saliva for SARS-CoV-2 Molecular Testing in Children. J. Pediatr. Infect. Dis. Soc. 2021, 10, 967–969. [Google Scholar] [CrossRef] [PubMed]
- Gorzalski, A.J.; Tian, H.; Laverdure, C.; Morzunov, S.; Verma, S.C.; VanHooser, S.; Pandori, M.W. High-Throughput Transcription-mediated amplification on the Hologic Panther is a highly sensitive method of detection for SARS-CoV-2. J. Clin. Virol. 2020, 129, 104501. [Google Scholar] [CrossRef] [PubMed]
- Schneider, M.; Iftner, T.; Ganzenmueller, T. Evaluation of the analytical performance and specificity of a SARS-CoV-2 transcription-mediated amplification assay. J. Virol. Methods 2021, 294, 114182. [Google Scholar] [CrossRef] [PubMed]
- Callahan, C.; Ditelberg, S.; Dutta, S.; Littlehale, N.; Cheng, A.; Kupczewski, K.; McVay, D.; Riedel, S.; Kirby, J.E.; Arnaout, R. Saliva is Comparable to Nasopharyngeal Swabs for Molecular Detection of SARS-CoV-2. Microbiol. Spectr. 2021, 9, e0016221. [Google Scholar] [CrossRef] [PubMed]
- Defêche, J.; Azarzar, S.; Mesdagh, A.; Dellot, P.; Tytgat, A.; Bureau, F.; Gillet, L.; Belhadj, Y.; Bontems, S.; Hayette, M.-P.; et al. In-Depth Longitudinal Comparison of Clinical Specimens to Detect SARS-CoV-2. Pathogens 2021, 10, 1362. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Zhao, J.; Peng, J.; Li, X.; Deng, X.; Geng, Z.; Shen, Z.; Guo, F.; Zhang, Q.; Jin, Y.; et al. Detection of SARS-CoV-2 in saliva and characterization of oral symptoms in COVID-19 patients. Cell Prolif. 2020, 53, e12923. [Google Scholar] [CrossRef] [PubMed]
- da Silva, R.C.M.; Marinho, L.C.N.; Silva, D.N.D.A.; de Lima, K.C.; Pirih, F.Q.; Martins, A.R.L.D.A. Saliva as a possible tool for the SARS-CoV-2 detection: A review. Travel Med. Infect. Dis. 2020, 38, 101920. [Google Scholar] [CrossRef] [PubMed]
- Swets, M.C.; Russell, C.D.; Harrison, E.M.; Docherty, A.B.; Lone, N.; Girvan, M.; Hardwick, H.E.; Visser, L.G.; Openshaw, P.J.M.; Groeneveld, G.H.; et al. SARS-CoV-2 co-infection with influenza viruses, respiratory syncytial virus, or adenoviruses. Lancet 2022, 399, 1463–1464. [Google Scholar] [CrossRef] [PubMed]
- Landry, M.L.; Criscuolo, J.; Peaper, D.R. Challenges in use of saliva for detection of SARS CoV-2 RNA in symptomatic outpatients. J. Clin. Virol. 2020, 130, 104567. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Age Groups | Positive Public Health Testing | Number Tested Public Health Testing | % Pos Public Health Testing | Positive Study Population | Number Tested Study Population | % Pos Study Population |
|---|---|---|---|---|---|---|
| <12 year | 507 | 794 | 63.9% | 0 | 0 | - |
| 12–17 year | 575 | 934 | 61.6% | 2 | 3 | 66.7% |
| 18–29 year | 2202 | 3580 | 61.5% | 18 | 38 | 47.4% |
| 30–39 year | 1870 | 2749 | 68.0% | 19 | 33 | 57.6% |
| 40–49 year | 1544 | 2274 | 67.9% | 28 | 38 | 73.7% |
| 50–59 year | 1652 | 2517 | 65.6% | 28 | 46 | 60.9% |
| 60–69 year | 1090 | 1587 | 68.7% | 16 | 20 | 80.0% |
| 70–79 year | 669 | 937 | 71.4% | 6 | 7 | 85.7% |
| >79 year | 174 | 249 | 69.9% | 1 | 2 | 50.0% |
| Total | 10,283 | 15,621 | 65.8% | 118 | 187 | 63.1% |
| TMA Neg | TMA Pos | Total | OR (Univariable) | ||
|---|---|---|---|---|---|
| Age | Median (IQR) | 37.0 (26.0 to 50.5) | 48.0 (34.0 to 57.0) | 46.0 (31.5 to 56.0) | 1.03 (1.01–1.05, p = 0.015) |
| Time since symptom onset | Median (IQR) | 1.0 (1.0 to 2.0) | 1.0 (1.0 to 2.0) | 1.0 (1.0 to 2.0) | 0.98 (0.76–1.29, p = 0.905) |
| Number of days earlier infection | Median (IQR) | 156.0 (63.8 to 386.8) | 327.5 (124.2 to 456.2) | 279.5 (103.8 to 438.2) | 1.00 (1.00–1.01, p = 0.181) |
| Earlier infection | No | 35 (68.6) | 114 (83.8) | 149 (79.7) | - |
| Yes | 16 (31.4) | 22 (16.2) | 38 (20.3) | 0.42 (0.20–0.90, p = 0.024) | |
| Sex | Female | 29 (56.9) | 74 (54.4) | 103 (55.1) | - |
| Male | 22 (43.1) | 62 (45.6) | 84 (44.9) | 1.10 (0.58–2.13, p = 0.764) | |
| Cold | No | 16 (31.4) | 41 (30.1) | 57 (30.5) | - |
| Yes | 35 (68.6) | 95 (69.9) | 130 (69.5) | 1.06 (0.52–2.10, p = 0.871) | |
| Sore throat | No | 19 (37.3) | 46 (33.8) | 65 (34.8) | - |
| Yes | 32 (62.7) | 90 (66.2) | 122 (65.2) | 1.16 (0.59–2.26, p = 0.661) | |
| Cough | No | 34 (66.7) | 71 (52.2) | 105 (56.1) | - |
| Yes | 17 (33.3) | 65 (47.8) | 82 (43.9) | 1.83 (0.95–3.65, p = 0.078) | |
| Headache | No | 34 (66.7) | 71 (52.2) | 105 (56.1) | - |
| Yes | 17 (33.3) | 65 (47.8) | 82 (43.9) | 1.83 (0.95–3.65, p = 0.078) | |
| Myalgia | No | 44 (86.3) | 104 (76.5) | 148 (79.1) | - |
| Yes | 7 (13.7) | 32 (23.5) | 39 (20.9) | 1.93 (0.83–5.07, p = 0.147) | |
| Short of breath | No | 47 (92.2) | 118 (86.8) | 165 (88.2) | - |
| Yes | 4 (7.8) | 18 (13.2) | 22 (11.8) | 1.79 (0.63–6.45, p = 0.314) | |
| Stomach ache | No | 46 (90.2) | 131 (96.3) | 177 (94.7) | - |
| Yes | 5 (9.8) | 5 (3.7) | 10 (5.3) | 0.35 (0.09–1.31, p = 0.110) | |
| Fever | No | 42 (82.4) | 115 (84.6) | 157 (84.0) | - |
| Yes | 9 (17.6) | 21 (15.4) | 30 (16.0) | 0.85 (0.37–2.09, p = 0.715) | |
| Loss of smell and taste | No | 48 (94.1) | 129 (94.9) | 177 (94.7) | - |
| Yes | 3 (5.9) | 7 (5.1) | 10 (5.3) | 0.87 (0.23–4.15, p = 0.842) | |
| Diarrhea | No | 50 (98.0) | 132 (97.1) | 182 (97.3) | - |
| Yes | 1 (2.0) | 4 (2.9) | 5 (2.7) | 1.52 (0.22–30.02, p = 0.713) | |
| Skin rash | No | 51 (100.0) | 135 (99.3) | 186 (99.5) | - |
| Yes | 0 (0.0) | 1 (0.7) | 1 (0.5) | - | |
| Eat something | No | 27 (52.9) | 71 (52.2) | 98 (52.4) | - |
| Yes | 24 (47.1) | 65 (47.8) | 89 (47.6) | 1.03 (0.54–1.97, p = 0.929) | |
| Drink something | No | 15 (29.4) | 43 (31.6) | 58 (31.0) | - |
| Yes | 36 (70.6) | 93 (68.4) | 129 (69.0) | 0.90 (0.44–1.80, p = 0.772) | |
| Brushed teeth | No | 29 (56.9) | 88 (64.7) | 117 (62.6) | - |
| Yes | 22 (43.1) | 48 (35.3) | 70 (37.4) | 0.72 (0.37–1.39, p = 0.325) | |
| Smoked | No | 44 (86.3) | 120 (88.2) | 164 (87.7) | - |
| Yes | 7 (13.7) | 16 (11.8) | 23 (12.3) | 0.84 (0.33–2.30, p = 0.716) | |
| Chewing gum | No | 44 (86.3) | 120 (88.2) | 164 (87.7) | - |
| Yes | 7 (13.7) | 16 (11.8) | 23 (12.3) | 0.84 (0.33–2.30, p = 0.716) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vahidnia, A.; Souverein, D.; Euser, S.M.; Haverkort, M.; Noordhuis, E.; van Zijl, T.Z.I.; Kalpoe, J.; Sinnige, J.C.; Herpers, B.L. Similar Sensitivity of SARS-CoV-2 Detection in Oropharyngeal/Nasopharyngeal and Saliva Samples on the Hologic Panther Platform. Diagnostics 2023, 13, 347. https://doi.org/10.3390/diagnostics13030347
Vahidnia A, Souverein D, Euser SM, Haverkort M, Noordhuis E, van Zijl TZI, Kalpoe J, Sinnige JC, Herpers BL. Similar Sensitivity of SARS-CoV-2 Detection in Oropharyngeal/Nasopharyngeal and Saliva Samples on the Hologic Panther Platform. Diagnostics. 2023; 13(3):347. https://doi.org/10.3390/diagnostics13030347
Chicago/Turabian StyleVahidnia, Ali, Dennis Souverein, Sjoerd M. Euser, Milly Haverkort, Elise Noordhuis, Thomas Z. I. van Zijl, Jayant Kalpoe, Jan C. Sinnige, and Bjorn L. Herpers. 2023. "Similar Sensitivity of SARS-CoV-2 Detection in Oropharyngeal/Nasopharyngeal and Saliva Samples on the Hologic Panther Platform" Diagnostics 13, no. 3: 347. https://doi.org/10.3390/diagnostics13030347