
Hysteroscopic Endometrial Ablation: From Indications to Instrumentation and Techniques—A Call to Action
 , , , , ,
, , , , , 
Abstract
:1. Introduction
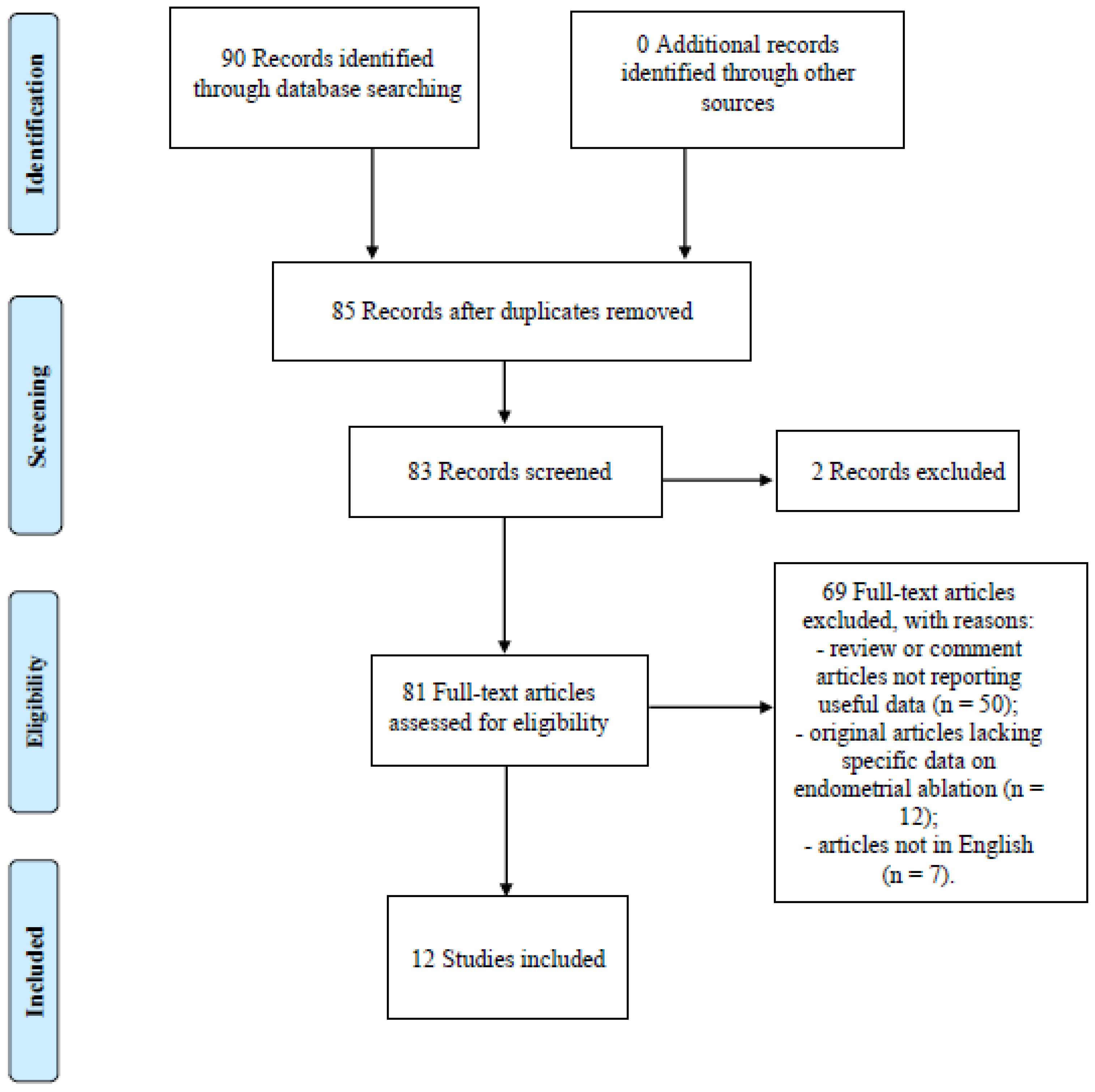
2. Materials and Methods
3. Results
4. Discussion
4.1. Clinical Indications of Endometrial Ablation: A Call to Action
4.2. Tools and Techniques
4.3. Current Indication for Complete Endometrial Ablation
4.4. Limitations and Contraindications
4.5. Future Perspectives: Endometrial Ablation for Preneoplastic Lesions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marchetti, M.; Litta, P.; Lanza, P.; Lauri, F.; Pozzan, C. The role of hysteroscopy in early diagnosis of endometrial cancer. Eur. J. Gynaecol. Oncol. 2002, 23, 151–153. [Google Scholar] [PubMed]
- Daniilidis, A.; Pantelis, A.; Dinas, K.; Angioni, S.; Carcea, F. Indications of diagnostic hysteroscopy, a brief review of the literature. Gynecol. Surg. 2012, 9, 23–28. [Google Scholar] [CrossRef]
- Luerti, M.; Vitagliano, A.; Sardo, A.D.; Angioni, S.; Garuti, G.; De Angelis, C.; Del Zoppo, S.; Dealberti, D.; Nappi, L.; Perrini, G.; et al. Effectiveness of Hysteroscopic Techniques for Endometrial Polyp Removal: The Italian Multicenter Trial. J. Minim. Invasive Gynecol. 2019, 26, 1169–1176. [Google Scholar] [CrossRef] [PubMed]
- Litta, P.; Conte, L.; De Marchi, F.; Saccardi, C.; Angioni, S. Pregnancy outcome after hysteroscopic myomectomy. Gynecol. Endocrinol. 2014, 30, 149–152. [Google Scholar] [CrossRef]
- Deutsch, A.; Sasaki, K.J.; Cholkeri-Singh, A. Resectoscopic Surgery for Polyps and Myomas: A Review of the Literature. J. Minim. Invasive Gynecol. 2017, 24, 1104–1110. [Google Scholar] [CrossRef]
- Sesti, F.; Marziali, M.; Santomarco, N. Hysteroscopic surgery for endometrial polyps using a bipolar microelectrode. Int. J. Gynaecol. Obstet. 2000, 71, 283–284. [Google Scholar] [CrossRef]
- Sardo, A.D.; Bettocchi, S.; Spinelli, M.; Guida, M.; Nappi, L.; Angioni, S.; Fernandez, L.M.; Nappi, C. Review of new office-based hysteroscopic procedures 2003–2009. J. Minim. Invasive Gynecol. 2010, 17, 436–448. [Google Scholar] [CrossRef]
- Nappi, L.; Pontis, A.; Sorrentino, F.; Greco, P.; Angioni, S. Hysteroscopic metroplasty for the septate uterus with diode laser: A pilot study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 206, 32–35. [Google Scholar] [CrossRef] [Green Version]
- Nappi, L.; Sorrentino, F.; Angioni, S.; Pontis, A.; Litta, P.; Greco, P. Feasibility of hysteroscopic endometrial polypectomy using a new dual wavelengths laser system (DWLS): Preliminary results of a pilot study. Arch. Gynecol. Obstet. 2017, 295, 3–7. [Google Scholar] [CrossRef]
- Nappi, L.; Sorrentino, F.; Angioni, S.; Pontis, A.; Greco, P. The use of laser in hysteroscopic surgery. Minerva Ginecol. 2016, 68, 722–726. [Google Scholar]
- D’Alterio, M.N.; Scicchitano, F.; Fanni, D.; Faa, G.; Laganà, A.S.; Noventa, M.; Sorrentino, F.; Nappi, L.; Angioni, S. Ex vivo myolysis with dual wavelengths diode laser system: Macroscopic and histopathological examination. Clin. Exp. Obstet. Gynecol. 2021, 48, 875–882. [Google Scholar] [CrossRef]
- Vitale, S.G.; Laganà, A.S.; Török, P.; Lasmar, R.B.; Carugno, J.; Palumbo, M.; Tesarik, J. Virtual sonographic hysteroscopy in assisted reproduction: A retrospective cost-effectiveness analysis. Int. J. Gynaecol. Obstet. 2022, 156, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Chiofalo, B.; Palmara, V.; Vilos, G.A.; Pacheco, L.A.; Lasmar, R.B.; Shawki, O.; Giacobbe, V.; Alibrandi, A.; Di Guardo, F.; Vitale, S.G. Reproductive outcomes of infertile women undergoing “see and treat” office hysteroscopy: A retrospective observational study. Minim. Invasive Ther. Allied Technol. 2021, 30, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Török, P.; Molnár, S.; Herman, T.; Jashanjeet, S.; Lampé, R.; Riemma, G.; Vitale, S.G. Fallopian tubal obstruction is associated with increased pain experienced during office hysteroscopy: A retrospective study. Updates Surg. 2020, 72, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Cancer Stat Facts: Uterine Cancer: National Institutes of Health, National Cancer Institute. 2022. Available online: https://seer.cancer.gov/statfacts/html/corp.html (accessed on 1 January 2022).
- Nappi, L.; Angioni, S.; De Feo, V.; Greco, P.; Stabile, G.; Greco, F.; D’Alterio, M.N.; Sorrentino, F. Diagnostic accuracy of hysteroscopy vs. dilation and curettage (D&C) for atypical endometrial hyperplasia in patients performing hysterectomy or serial follow-up. Clin. Exp. Obstet. Gynecol. 2022, 49, 24. [Google Scholar]
- Quintana-Bertó, R.; Padilla-Iserte, P.; Gil-Moreno, A.; Oliver-Pérez, R.; Coronado, P.J.; Martín-Salamanca, M.B.; Pantoja-Garrido, M.; Lorenzo, C.; Cazorla, E.; Gilabert-Estellés, J.; et al. Oncological safety of hysteroscopy in endometrial cancer. Int. J. Gynecol. Cancer, 2022; Epub ahead of print. [Google Scholar] [CrossRef]
- Vitale, S.G.; Riemma, G.; Haimovich, S.; Carugno, J.; Pacheco, L.A.; Perez-Medina, T.; Parry, J.P.; Török, P.; Tesarik, J.; Della Corte, L.; et al. Risk of endometrial cancer in asymptomatic postmenopausal women in relation to ultrasonographic endometrial thickness: Systematic review and diagnostic test accuracy meta-analysis. Am. J. Obstet. Gynecol. 2022; Epub ahead of print. [Google Scholar] [CrossRef]
- Emanuel, M.H.; Wamsteker, K. The Intra Uterine Morcellator: A new hysteroscopic operating technique to remove intrauterine polyps and myomas. J. Minim. Invasive Gynecol. 2005, 12, 62–66. [Google Scholar] [CrossRef]
- Van Dongen, H.; Emanuel, M.H.; Wolterbeek, R.; Trimbos, J.B.; Jansen, F.W. Hysteroscopic morcellator for removal of intrauterine polyps and myomas: A randomized controlled pilot study among residents in training. J. Minim. Invasive Gynecol. 2008, 15, 466–471. [Google Scholar] [CrossRef]
- Litta, P.; Nappi, L.; Florio, P.; Mencaglia, L.; Franchini, M.; Angioni, S. Proposal of a modified transcervical endometrial resection (TCER) technique for menorrhagia treatment. Feasibility, efficacy, and patients’ acceptability. Gynecol. Surg. 2014, 11, 165–171. [Google Scholar] [CrossRef] [Green Version]
- Hamerlynck, T.W.; Dietz, V.; Schoot, B.C. Clinical implementation of the hysteroscopic morcellator for removal of intrauterine myomas and polyps. A retrospective descriptive study. Gynecol. Surg. 2011, 8, 193–196. [Google Scholar] [CrossRef] [Green Version]
- Kumar, V.; Chodankar, R.; Gupta, J.K. Endometrial ablation for heavy menstrual bleeding. Womens Health 2016, 12, 45–52. [Google Scholar] [CrossRef]
- Vitale, S.G.; Watrowski, R.; Barra, F.; D’Alterio, M.N.; Carugno, J.; Sathyapalan, T.; Kahramanoglu, I.; Reyes-Muñoz, E.; Lin, L.T.; Urman, B.; et al. Abnormal Uterine Bleeding in Perimenopausal Women: The Role of Hysteroscopy and Its Impact on Quality of Life and Sexuality. Diagnostics 2022, 12, 1176. [Google Scholar] [CrossRef] [PubMed]
- Van den Brink, M.J.; Saaltink, A.L.; Groenhof, F.; Kollen, B.J.; Berger, M.Y.; Lisman-van Leeuwen, Y.; Dekker, J.H. Incidence and treatment of heavy menstrual bleeding in general practice. Fam. Pract. 2017, 34, 673–678. [Google Scholar] [CrossRef] [PubMed]
- Munro, M.G.; Critchley, H.O.; Broder, M.S.; Fraser, I.S.; FIGO Working Group on Menstrual Disorders. FIGO classification system (PALM-COEIN) for causes of abnormal uterine bleeding in nongravid women of reproductive age. Int. J. Gynaecol. Obstet. 2011, 113, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Benetti-Pinto, C.L.; Rosa, E.S.A.; Yela, D.A.; Soares Junior, J.M. Abnormal Uterine Bleeding. Rev. Bras. Ginecol. Obstet. 2017, 39, 358–368. [Google Scholar] [CrossRef] [Green Version]
- Baethge, C.; Goldbeck-Wood, S.; Mertens, S. SANRA-a scale for the quality assessment of narrative review articles. Res. Integr. Peer Rev. 2019, 4, 5. [Google Scholar] [CrossRef] [Green Version]
- Thomassee, M.S.; Curlin, H.; Yunker, A.; Anderson, T.L. Predicting pelvic pain after endometrial ablation: Which preoperative patient characteristics are associated? J. Minim. Invasive Gynecol. 2013, 20, 642–647. [Google Scholar] [CrossRef]
- Soini, T.; Rantanen, M.; Paavonen, J.; Grénman, S.; Mäenpää, J.; Pukkala, E.; Gissler, M.; Hurskainen, R. Long-term Follow-up After Endometrial Ablation in Finland: Cancer Risks and Later Hysterectomies. Obstet. Gynecol. 2017, 130, 554–560. [Google Scholar] [CrossRef] [Green Version]
- Wishall, K.M.; Price, J.; Pereira, N.; Butts, S.M.; Della Badia, C.R. Postablation risk factors for pain and subsequent hysterectomy. Obstet. Gynecol. 2014, 124, 904–910. [Google Scholar] [CrossRef]
- Helleland, L.; Bergesen, L.F.; Rinnan, K.J.; Engelsen, I.B.; Hordnes, K.; Trovik, J. Endometrial ablation; less is more? Historical cohort study comparing long-term outcomes from two time periods and two treatment modalities for 854 women. PLoS ONE 2019, 14, e0219294. [Google Scholar] [CrossRef] [Green Version]
- Cooper, K.; Lee, A.; Chien, P.; Raja, E.; Timmaraju, V.; Bhattacharya, S. Outcomes following hysterectomy or endometrial ablation for heavy menstrual bleeding: Retrospective analysis of hospital episode statistics in Scotland. BJOG 2011, 118, 1171–1179. [Google Scholar] [CrossRef]
- Pinion, S.B.; EParkin, D.; Abramovich, D.R.; Naji, A.; AAlexander, D.; Russell, I.T.; Kitchener, H.C. Randomised trial of hysterectomy, endometrial laser ablation, and transcervical endometrial resection for dysfunctional uterine bleeding. BMJ 1994, 309, 979–983. [Google Scholar] [CrossRef]
- Ajao, M.O.; El-Nashar, S.A.; Khan, Z.; Hopkins, M.R.; Creedon, D.J.; Famuyide, A.O. Nonresectoscopic endometrial ablation in high-risk surgical patients: A cohort study. J. Minim. Invasive Gynecol. 2013, 20, 487–491. [Google Scholar] [CrossRef]
- Smithling, K.R.; Savella, G.; Raker, C.A.; Matteson, K.A. Preoperative uterine bleeding pattern and risk of endometrial ablation failure. Am. J. Obstet. Gynecol. 2014, 211, 556. [Google Scholar] [CrossRef]
- Clark, T.J.; Gupta, J.K. Outpatient thermal balloon ablation of the endometrium. Fertil. Steril. 2004, 82, 1395–1401. [Google Scholar] [CrossRef]
- Andersson, S.; Mints, M. Thermal balloon ablation for the treatment of menorrhagia in an outpatient setting. Acta Obstet. Gynecol. Scand. 2007, 86, 480–483. [Google Scholar] [CrossRef] [PubMed]
- Herman, M.C.; Penninx, J.P.; Mol, B.W.; Bongers, M.Y. Ten-year follow-up of a randomised controlled trial comparing bipolar endometrial ablation with balloon ablation for heavy menstrual bleeding. BJOG 2013, 120, 966–970. [Google Scholar] [CrossRef] [PubMed]
- Hokenstad, A.N.; El-Nashar, S.A.; Khan, Z.; Hopkins, M.R.; Famuyide, A.O. Endometrial Ablation in Women With Abnormal Uterine Bleeding Related to Ovulatory Dysfunction: A Cohort Study. J. Minim. Invasive Gynecol. 2015, 22, 1225–1230. [Google Scholar] [CrossRef] [PubMed]
- Angioni, S.; Pontis, A.; Nappi, L.; Sedda, F.; Sorrentino, F.; Litta, P.; Haimovich, S.; Melis, G.B. Endometrial ablation: First- vs. second-generation techniques. Minerva Ginecol. 2016, 68, 143–153. [Google Scholar] [PubMed]
- Lethaby, A.; Hickey, M. Endometrial destruction techniques for heavy menstrual bleeding: A Cochrane review. Hum. Reprod. 2002, 17, 2795–2806. [Google Scholar] [CrossRef] [Green Version]
- Bettocchi, S.; Nappi, L.; Ceci, O.; Selvaggi, L. What does ‘diagnostic hysteroscopy’ mean today? The role of the new techniques. Curr. Opin. Obstet. Gynecol. 2003, 15, 303–308. [Google Scholar] [CrossRef]
- Sowter, M.C.; Lethaby, A.; Singla, A.A. Pre-operative endometrial thinning agents before endometrial destruction for heavy menstrual bleeding. Cochrane Database Syst. Rev. 2002, CD001124. [Google Scholar] [CrossRef]
- Murji, A.; Lam, M.; Allen, B.; Richard, L.; Shariff, S.Z.; Austin, P.C.; Callum, J.; Lipscombe, L. Risks of preoperative anemia in women undergoing elective hysterectomy and myomectomy. Am. J. Obstet. Gynecol. 2019, 221, 629.e1–629.e18. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.; Raslan, M.; Ciebiera, M.; Zareba, K.; Al-Hendy, A. Current approaches to overcome the side effects of GnRH analogs in the treatment of patients with uterine fibroids. Expert. Opin. Drug Saf. 2022, 21, 477–486. [Google Scholar] [CrossRef] [PubMed]
- Zgliczynska, M.; Kocaj, K.; Szymusik, I.; Dutsch-Wicherek, M.M.; Ciebiera, M.; Kosinska-Kaczynska, K. Levonorgestrel-Releasing Intrauterine System as a Contraceptive Method in Nulliparous Women: A Systematic Review. J. Clin. Med. 2020, 9, 2101. [Google Scholar] [CrossRef]
- Marjoribanks, J.; Lethaby, A.; Farquhar, C. Surgery versus medical therapy for heavy menstrual bleeding. Cochrane Database Syst. Rev. 2003, CD003855. [Google Scholar] [CrossRef]
- Ciebiera, M.; Lozinski, T.; Wojtyla, C.; Rawski, W.; Jakiel, G. Complications in modern hysteroscopic myomectomy. Ginekol. Pol. 2018, 89, 398–404. [Google Scholar] [CrossRef] [Green Version]
- Di Spiezio Sardo, A.; Taylor, A.; Tsirkas, P.; Mastrogamvrakis, G.; Sharma, M.; Magos, A. Hysteroscopy: A technique for all? Analysis of 5000 outpatient hysteroscopies. Fertil. Steril. 2008, 89, 438–443. [Google Scholar] [CrossRef]
- Pluchino, N.; Ninni, F.; Angioni, S.; Artini, P.; Araujo, V.G.; Massimetti, G.; Genazzani, A.R.; Cela, V. Office vaginoscopic hysteroscopy in infertile women: Effects of gynecologist experience, instrument size, and distention medium on patient discomfort. J. Minim. Invasive Gynecol. 2010, 17, 344–350. [Google Scholar] [CrossRef]
- Cooper, K.G. Outpatient endometrial ablation. Best Pract. Res. Clin. Obstet. Gynaecol. 2005, 19, 713–726. [Google Scholar] [CrossRef]
- Giampaolino, P.; Della Corte, L.; Di Filippo, C.; Mercorio, A.; Vitale, S.G.; Bifulco, G. Office hysteroscopy in the management of women with postmenopausal bleeding. Climacteric 2020, 23, 369–375. [Google Scholar] [CrossRef]
- Unfried, G.; Wieser, F.; Albrecht, A.; Kaider, A.; Nagele, F. Flexible versus rigid endoscopes for outpatient hysteroscopy: A prospective randomized clinical trial. Hum. Reprod. 2001, 16, 168–171. [Google Scholar] [CrossRef] [PubMed]
- De Angelis, C.; Santoro, G.; Re, M.E.; Nofroni, I. Office hysteroscopy and compliance: Mini-hysteroscopy versus traditional hysteroscopy in a randomized trial. Hum. Reprod. 2003, 18, 2441–2445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Litta, P.; Spiller, E.; Saccardi, C.; Ambrosini, G.; Caserta, D.; Cosmi, E. Resectoscope or Versapoint for hysteroscopic metroplasty. Int. J. Gynaecol. Obstet. 2008, 101, 39–42. [Google Scholar] [CrossRef] [PubMed]
- Pellicano, M.; Guida, M.; Zullo, F.; Lavitola, G.; Cirillo, D.; Nappi, C. Carbon dioxide versus normal saline as a uterine distension medium for diagnostic vaginoscopic hysteroscopy in infertile patients: A prospective, randomized, multicenter study. Fertil. Steril. 2003, 79, 418–421. [Google Scholar] [CrossRef] [PubMed]
- Litta, P.; Cosmi, E.; Saccardi, C.; Esposito, C.; Rui, R.; Ambrosini, G. Outpatient operative polypectomy using a 5 mm-hysteroscope without anaesthesia and/or analgesia: Advantages and limits. Eur. J. Obstet. Gynecol. Reprod. Biol. 2008, 139, 210–214. [Google Scholar] [CrossRef]
- Papalampros, P.; Gambadauro, P.; Papadopoulos, N.; Polyzos, D.; Chapman, L.; Magos, A. The mini-resectoscope: A new instrument for office hysteroscopic surgery. Acta Obstet. Gynecol. Scand. 2009, 88, 227–230. [Google Scholar] [CrossRef]
- Roy, K.K.; Lingampally, A.; Kansal, Y.; Bharti, J.; Kumar, S.; Vanamail, P.; Singhal, S.; Meena, J. A Pilot Study Comparing Hysteroscopic Adhesiolysis by Conventional Resectoscope Versus Mini-resectoscope. Oman Med. J. 2017, 32, 492–498. [Google Scholar] [CrossRef]
- Vitale, S.G.; Riemma, G.; Carugno, J.; Perez-Medina, T.; Pacheco, L.A.; Haimovich, S.; Parry, J.P.; Sardo, A.D.; De Franciscis, P. Postsurgical barrier strategies to avoid the recurrence of intrauterine adhesion formation after hysteroscopic adhesiolysis: A network meta-analysis of randomized controlled trials. Am. J. Obstet. Gynecol. 2022, 226, 487–498.e8. [Google Scholar] [CrossRef]
- Cicinelli, E.; Parisi, C.; Galantino, P.; Pinto, V.; Barba, B.; Schonauer, S. Reliability, feasibility, and safety of minihysteroscopy with a vaginoscopic approach: Experience with 6000 cases. Fertil. Steril. 2003, 80, 199–202. [Google Scholar] [CrossRef]
- Litta, P.; Leggieri, C.; Conte, L.; Dalla Toffola, A.; Multinu, F.; Angioni, S. Monopolar versus bipolar device: Safety, feasibility, limits and perioperative complications in performing hysteroscopic myomectomy. Clin. Exp. Obstet. Gynecol. 2014, 41, 335–338. [Google Scholar] [CrossRef]
- Di Spiezio Sardo, A.; Calagna, G.; Di Carlo, C.; Guida, M.; Perino, A.; Nappi, C. Cold loops applied to bipolar resectoscope: A safe “one-step” myomectomy for treatment of submucosal myomas with intramural development. J. Obstet. Gynaecol. Res. 2015, 41, 1935–1941. [Google Scholar] [CrossRef] [PubMed]
- Mazzon, I.; Favilli, A.; Grasso, M.; Horvath, S.; Di Renzo, G.C.; Gerli, S. Is Cold Loop Hysteroscopic Myomectomy a Safe and Effective Technique for the Treatment of Submucous Myomas With Intramural Development? A Series of 1434 Surgical Procedures. J. Minim. Invasive Gynecol. 2015, 22, 792–798. [Google Scholar] [CrossRef] [PubMed]
- Bettocchi, S.; Ceci, O.; Nappi, L.; Di Venere, R.; Masciopinto, V.; Pansini, V.; Pinto, L.; Santoro, A.; Cormio, G. Operative office hysteroscopy without anesthesia: Analysis of 4863 cases performed with mechanical instruments. J. Am. Assoc. Gynecol. Laparosc. 2004, 11, 59–61. [Google Scholar] [CrossRef] [PubMed]
- Vitale, S.G.; Sapia, F.; Rapisarda, A.M.C.; Valenti, G.; Santangelo, F.; Rossetti, D.; Chiofalo, B.; Sarpietro, G.; La Rosa, V.L.; Triolo, O.; et al. Hysteroscopic Morcellation of Submucous Myomas: A Systematic Review. Biomed. Res. Int. 2017, 2017, 6848250. [Google Scholar] [CrossRef]
- Vitale, S.G. The Biopsy Snake Grasper Sec. VITALE: A New Tool for Office Hysteroscopy. J. Minim. Invasive Gynecol. 2020, 27, 1414–1416. [Google Scholar] [CrossRef]
- Vitale, S.G.; Laganà, A.S.; Caruso, S.; Garzon, S.; Vecchio, G.M.; La Rosa, V.L.; Casarin, J.; Ghezzi, F. Comparison of three biopsy forceps for hysteroscopic endometrial biopsy in postmenopausal patients (HYGREB-1): A multicenter, single-blind randomized clinical trial. Int. J. Gynaecol. Obstet. 2021, 155, 425–432. [Google Scholar] [CrossRef]
- Laberge, P.; Leyland, N.; Murji, A.; Fortin, C.; Martyn, P.; Vilos, G.; Wolfman, W.; Allaire, C.; Awadalla, A.; Dunn, S.; et al. Endometrial ablation in the management of abnormal uterine bleeding. J. Obstet. Gynaecol. Can. 2015, 37, 362–379. [Google Scholar] [CrossRef]
- Abbott, J.A.; Hawe, J.; Garry, R. Quality of life should be considered the primary outcome for measuring success of endometrial ablation. J. Am. Assoc. Gynecol. Laparosc. 2003, 10, 491–495. [Google Scholar] [CrossRef]
- Duckitt, K. Menorrhagia. BMJ Clin. Evid. 2015, 2015, 0805. [Google Scholar]
- Cooper, J.M.; Brady, R.M. Intraoperative and early postoperative complications of operative hysteroscopy. Obstet. Gynecol. Clin. N. Am. 2000, 27, 347–366. [Google Scholar] [CrossRef]
- Gurtcheff, S.E.; Sharp, H.T. Complications associated with global endometrial ablation: The utility of the MAUDE database. Obstet. Gynecol. 2003, 102, 1278–1282. [Google Scholar] [CrossRef]
- Jansen, F.W.; Vredevoogd, C.B.; van Ulzen, K.; Hermans, J.; Trimbos, J.B.; Trimbos-Kemper, T.C. Complications of hysteroscopy: A prospective, multicenter study. Obstet. Gynecol. 2000, 96, 266–270. [Google Scholar] [CrossRef] [PubMed]
- Stachowicz, N.; Smoleń, A.; Ciebiera, M.; Łoziński, T.; Poziemski, P.; Borowski, D.; Czekierdowski, A. Risk Assessment of Endometrial Hyperplasia or Endometrial Cancer with Simplified Ultrasound-Based Scoring Systems. Diagnostics 2021, 11, 442. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, C.M.; Brito, L.G.O.; Benetti-Pinto, C.L.; Teixeira, J.C.; Yela, D.A. Is Diagnostic Hysteroscopy Safe for the Investigation of Type II Endometrial Cancer? A Retrospective Cohort Analysis. J. Minim. Invasive Gynecol. 2021, 28, 1536–1543. [Google Scholar] [CrossRef] [PubMed]
- Della Corte, L.; Vitale, S.G.; Foreste, V.; Riemma, G.; Ferrari, F.; Noventa, M.; Liberto, A.; De Franciscis, P.; Tesarik, J. Novel diagnostic approaches to intrauterine neoplasm in fertile age: Sonography and hysteroscopy. Minim. Invasive Ther. Allied Technol. 2021, 30, 288–295. [Google Scholar] [CrossRef]
- Soini, T.; Hurskainen, R.; Grénman, S.; Mäenpää, J.; Paavonen, J.; Joensuu, H.; Pukkala, E. Levonorgestrel-releasing intrauterine system and the risk of breast cancer: A nationwide cohort study. Acta Oncol. 2016, 55, 188–192. [Google Scholar] [CrossRef]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. Correction to: 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2020, 141, e773. [Google Scholar]
- Sardo, A.D.S.; De Angelis, M.C.; Della Corte, L.; Carugno, J.; Zizolfi, B.; Guadagno, E.; Gencarelli, A.; Cecchi, E.; Simoncini, T.; Bifulco, G.; et al. Should endometrial biopsy under direct hysteroscopic visualization using the grasp technique become the new gold standard for the preoperative evaluation of the patient with endometrial cancer? Gynecol. Oncol. 2020, 158, 347–353. [Google Scholar] [CrossRef]
- Di Guardo, F.; Della Corte, L.; Vilos, G.A.; Carugno, J.; Török, P.; Giampaolino, P.; Manchanda, R.; Vitale, S.G. Evaluation and treatment of infertile women with Asherman syndrome: An updated review focusing on the role of hysteroscopy. Reprod. Biomed. Online 2020, 41, 55–61. [Google Scholar] [CrossRef]


{kind=link}
| Study | Country and Year | Design | Population | Symptoms | Tools Used for EA * | Primary Outcome | Menstrual Blood Loss | Impact on Quality of Life | Duration of Surgical Procedure | Length of Hospital Stay | Time to Return to Work | Adverse Events | Requirements for Repeat Surgery °§ |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Soini [30] | Finland 1997–2014 | Retrospective cohort study | 5484 (n) | AUB Dysmenorrhea | NR | Risk of endometrial and breast cancer and the hysterectomy rate after EA | 4488 (n) NR after EA | NR | NA | NA | NA | NA | 6 (n) EA 1086 (n) Hysterectomy |
| Wishall [31] | United States of America 2003–2016 | Retrospective cohort study | 300 (n) | AUB Dysmenorrhea | Thermal balloon Radiofrequency bipolar Microwave Hydrothermal | Risk factors for postablation pain or hysterectomy | NR 23 (n) after EA | NR | NA | NA | NA | NA | 51 (n) Hysterectomy |
| Thomassee [29] | United States of America 2006–2010 | Retrospective cohort study | 437 (n) | AUB Dysmenorrhea | Rollerball Thermal balloon Radiofrequency bipolar | Postoperative pelvic pain | NR 66 (n) after EA | NR | NA | NA | NA | NA | 0.2 (%) EA 65 (n) Hysterectomy |
| Helleland [32] | Norway 1992–2014 | Retrospective cohort study | 135 (n) | AUB Dysmenorrhea | Radiofrequency bipolar | Efficacy of EA | 20 (n) 5 (n) after EA | Satisfaction rates 73–85 (%) | 13 min | NA | NA | 1 (technical problems) | 11 (n) Hysterectomy |
| Cooper [33] | United Kingdom 1989–2006 | Retrospective cohort study | 14,078 (n) | AUB Dysmenorrhea | NR | Risk of further gynaecological surgery and cancer | 14,078 (n) 2779 (n) after EA | NR | NA | NA | NA | NA | 379 (n) EA 2779 (n) Hysterectomy |
| Pinion [34] | United Kingdom 1990–1992 | Retrospective cohort study | 53 (n) | AUB Dysmenorrhea | Laser ablation | Efficacy of EA and Satisfaction | 26 (n) 5 (n) after EA | Satisfaction rates 70–90 (%) | 44 min | 2–5 | NA | 1 (bowel damage) | 11 (n) EA 17 (n) Hysterectomy |
| Ajao [35] | United States of America 2006–2014 | Retrospective cohort study | 634 (n) | AUB Dysmenorrhea r | Radiofrequency bipolar Thermal balloon | Safety in patients with high-risk ASA | NR NR after EA | NA | NR | NA | NA | NR | 81 (n) Hysterectomy |
| Smithling [36] | United States of America 2007–2009 | Retrospective cohort study | 968 (n) | AUB Dysmenorrhea | Radiofrequency bipolar | Risks of treatment failure | 931 (n) 40 (n) after EA | NA | NA | NA | NA | NA | 11 (n) EA 74 (n) Hysterectomy |
| Clark [37] | United Kingdom 2001–2003 | Prospective observational study | 53 (n) | AUB Dysmenorrhea | Thermal balloon | Efficacy of EA | 39 (n) 6 (n) after EA | Satisfaction rates 67 (%) | 8 min | NA | NA | 1 (balloon blockage) | 1 (n) EA 3 (n) Hysterectomy |
| Andersson [38] | Sweden 2001–2005 | Prospective observational study | 54 (n) | AUB Dysmenorrhea | Thermal balloon | Efficacy of EA | 42 (n) 8 (n) after EA | NA | 15 min | NA | NA | 3 (allergic reaction, balloon blockage, abdominal cramps) | 1 (n) Hysterectomy 3 (n) Hysteroscopical endometrial resection |
| Herman [39] | Netherlands 1999–2011 | Double-blind RCT | 126 (n) | AUB Dysmenorrhea | Thermal balloon Radiofrequency bipolar |
Thermal balloon vs. Bipolar | 126 (n) 53 (n) after EA | Satisfaction rates 77–81(%) | NA | NA | NA | NA | 21 (n) EA 2 (n) Hysterectomy |
| Hokenstad [40] | United States of America 1998–2005 | Prospective observational study | 711 (n) | AUB Dysmenorrhea | Thermal balloon Radiofrequency bipolar | Efficacy of EA | 489 (n) 66 (n) after EA | NA | NA | NA | NA | NA | 66 (n) Hysterectomy |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vitale, S.G.; Della Corte, L.; Ciebiera, M.; Carugno, J.; Riemma, G.; Lasmar, R.B.; Lasmar, B.P.; Kahramanoglu, I.; Urman, B.; Mikuš, M.; et al. Hysteroscopic Endometrial Ablation: From Indications to Instrumentation and Techniques—A Call to Action. Diagnostics 2023, 13, 339. https://doi.org/10.3390/diagnostics13030339
Vitale SG, Della Corte L, Ciebiera M, Carugno J, Riemma G, Lasmar RB, Lasmar BP, Kahramanoglu I, Urman B, Mikuš M, et al. Hysteroscopic Endometrial Ablation: From Indications to Instrumentation and Techniques—A Call to Action. Diagnostics. 2023; 13(3):339. https://doi.org/10.3390/diagnostics13030339
Chicago/Turabian StyleVitale, Salvatore Giovanni, Luigi Della Corte, Michał Ciebiera, Josè Carugno, Gaetano Riemma, Ricardo Bassil Lasmar, Bernardo Portugal Lasmar, Ilker Kahramanoglu, Bulent Urman, Mislav Mikuš, and et al. 2023. "Hysteroscopic Endometrial Ablation: From Indications to Instrumentation and Techniques—A Call to Action" Diagnostics 13, no. 3: 339. https://doi.org/10.3390/diagnostics13030339