
A Radiomic-Based Machine Learning System to Diagnose Age-Related Macular Degeneration from Ultra-Widefield Fundus Retinography

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Image Sets
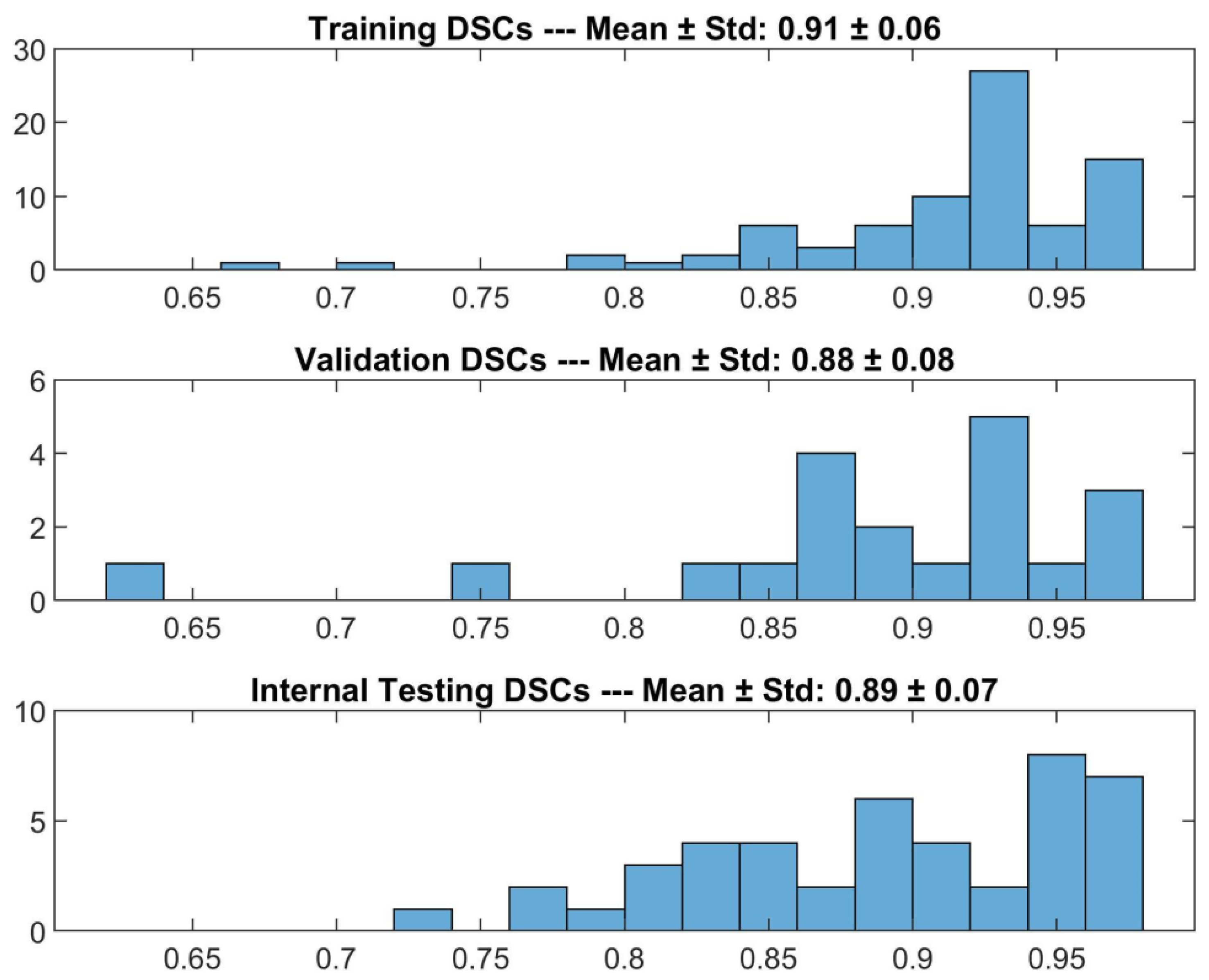
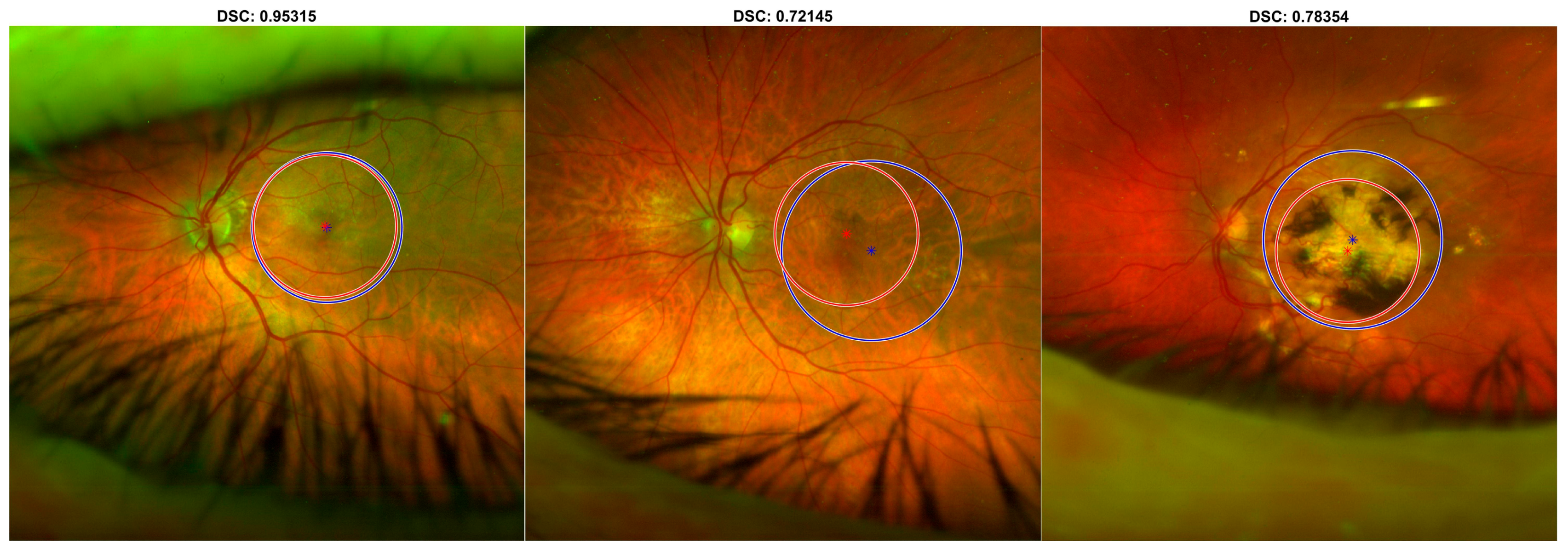
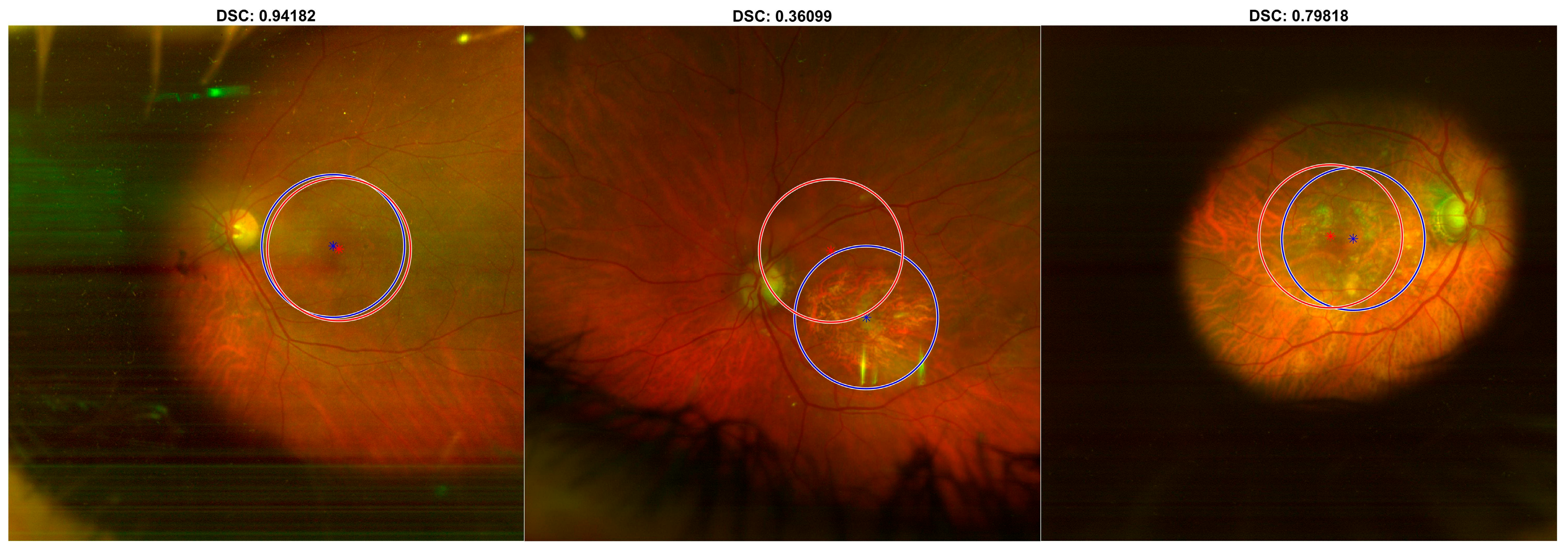
2.2. DL-Based Macular Detector
2.3. ML-Based Radiomics Model
- The manual segmentation of the ROI, performed by one expert operator, as described in the DL-based macular detector section.
- The preprocessing of pixel intensities in the ROI, which included grayscale pixel conversion and resampling, using a down-sampling scheme of 2 to 1 pixels.
- The computation of Radiomics features from the segmented ROI, belonging to different features families: Intensity-based Statistics, Intensity Histogram, Gray-Level Co-occurrence Matrix (GLCM), Gray-Level Run Length Matrix (GLRLM), Gray-Level Size Zone Matrix (GLSZM), Neighbourhood Gray Tone Difference Matrix (NGTDM), Neighbouring Gray Level Dependence Matrix (NGLDM). Their definition, computation, and nomenclature are reported in the IBSI guidelines [24]. Steps (2) and (3) were performed using the Trace4Research radiomics tool. It must be noted that Intensity Histogram features were computed after an intensity discretisation of the ROI, using a fixed number of 64 bins. Texture features (GLCM, GLRLM, GLSZM, NGTDM, NGLDM) were computed after an intensity discretisation of the ROI, using a fixed number of 64 bins.
- The selection of relevant features, addressing stability and repeatability with respect to different segmentations and test-retest study. This was evaluated by computing ICC (1,1) [26] (ICC > 0.80) and statistically comparing features obtained by data augmentation strategies. Data augmentation comprised random rotation of the original image and the segmented ROI and random manipulation of the segmented ROI.
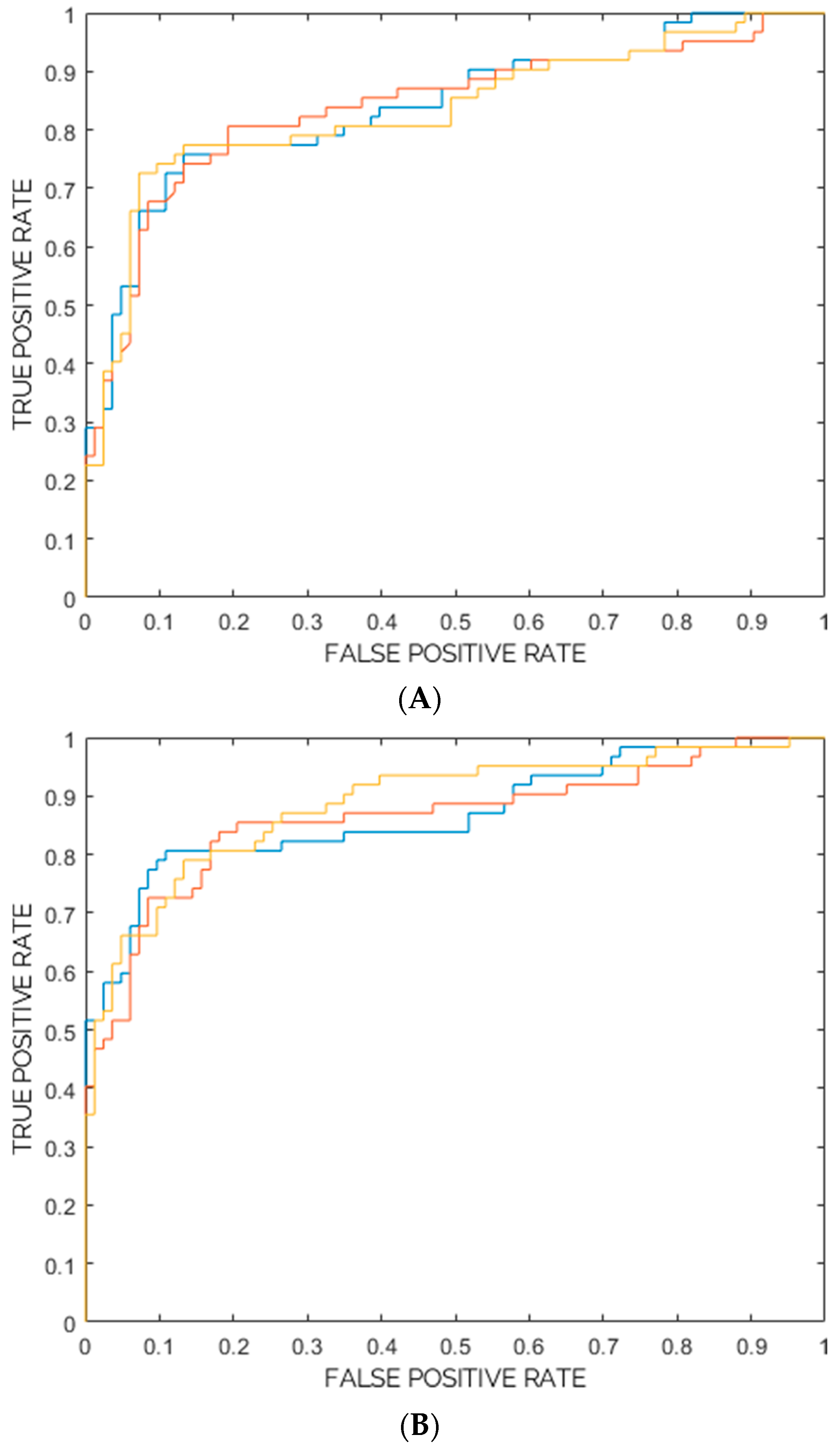
- The training, validation, and internal testing of two supervised machine-learning models, using a nested 10-fold cross-validation approach. The first model’s architecture was an ensemble of three ensemble models, each composed of 100 random-forest classifiers combined with Gini index and majority-vote rule. The second model’s architecture was an ensemble of three ensemble models, each composed of 100 support vector machines (SVM) combined with principal components analysis, Fisher Discriminant Ratio, and majority-vote rule. The minority class (“AMD”) was oversampled by adaptive synthetic sampling method (ADASYN) [27]. The performances of the two models were measured in terms of mean Accuracy, Sensitivity, Specificity, Positive Predictive Value (PPV), Negative Predictive Value (NPV) (defined by Equations (3)–(7)), Area Under the Receiver Operating Characteristic Curve (ROC-AUC) [28], and also by evaluating the 95% confidence intervals (CI). Among the two models, the one with the highest ROC-AUC was chosen as the best classification model.
2.4. Statistical Analysis
3. Results
3.1. DL-Based Macular Detector
3.2. Radiomic-Based ML Model
3.3. Statistical Analysis
3.4. Classification Result
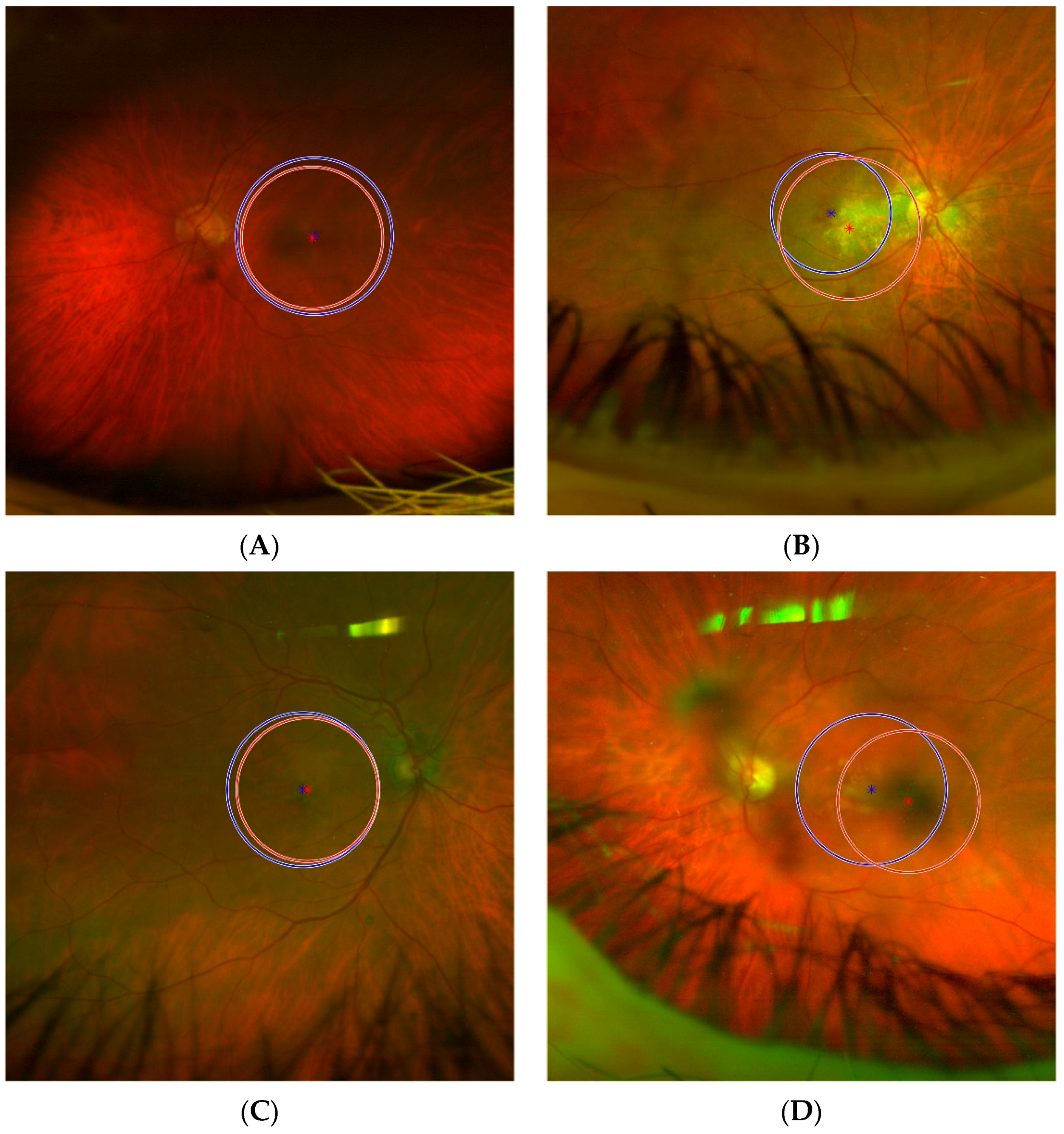
- (A)
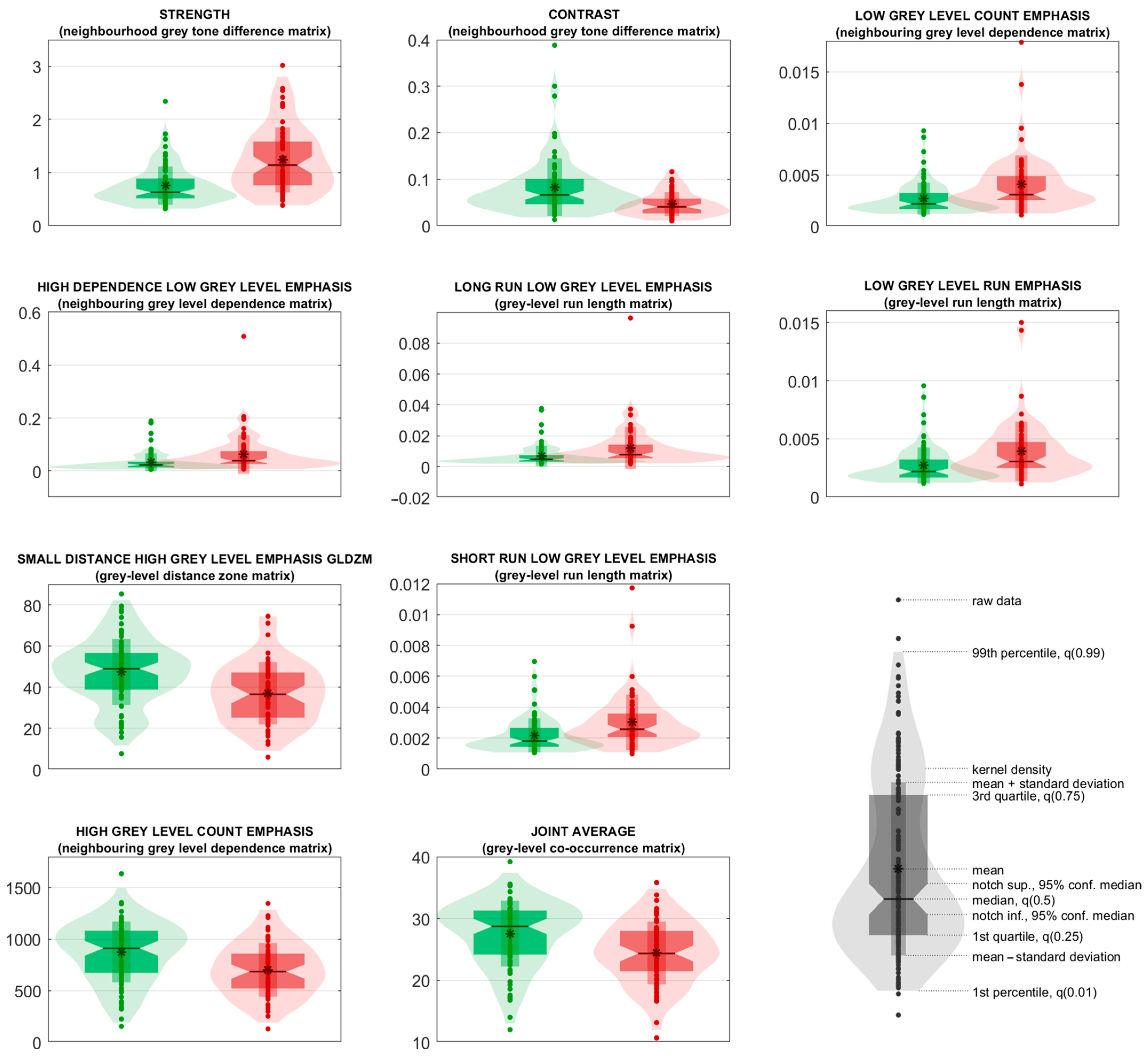
- In Figure 8A, an example of a True Positive, i.e., “AMD” classified as “AMD”, is shown. It is noteworthy that none of the 10 top predictors (reported in Table 3) excessively deviates from the expected distribution for “AMD” class (such distributions are graphically reported in Figure 7 and are computed excluding the external testing set). The ROI obtained from the DL-based automatic detector is characterised by the following feature values (percentile/difference with the mean in standard deviations units):
- Strength: 0.973489 (40°/−0.4σ)
- Contrast: 0.071115 (82°/0.9σ)
- Low Grey Level Count Emphasis: 0.00284707 (40°/−0.4σ)
- High Dependence Low Grey Level Emphasis: 0.025812 (25°/−0.5σ)
- Long Run Low Grey Level Emphasis: 0.00564284 (28°/−0.5σ)
- Low Grey Level Run Emphasis: 0.00285426 (45°/−0.4σ)
- Small Distance High Grey Level Emphasis: 34.7584 (44°/−0.2σ)
- Short Run Low Grey Level Emphasis: 0.00241731 (46°/−0.3σ)
- High Grey Level Count Emphasis: 751.594 (58°/0.2σ)
- Joint Average: 25.3098 (55°/0.2σ)
- (B)
- In Figure 8B, an example of a True Negative, i.e., “Negative” classified as “Negative”, is shown. As with the previous case, in Figure 8A, all the 10 top predictors have reasonable values considering the expected distribution for “Negative” class. The values (percentile/standard deviations from the mean) are:
- Strength: 0.578356 (37°/−0.5σ)
- Contrast: 0.0518532 (31°/−0.5σ)
- Low Grey Level Count Emphasis: 0.0014604 (10°/−0.8σ)
- High Dependence Low Grey Level Emphasis: 0.00893454 (6°/−0.7σ)
- Long Run Low Grey Level Emphasis: 0.00237348 (5°/−0.7σ)
- Low Grey Level Run Emphasis: 0.00148348 (12°/−0.8σ)
- Small Distance High Grey Level Emphasis: 46.9358 (48°/0.0σ)
- Short Run Low Grey Level Emphasis: 0.00132314 (14°/−0.8σ)
- High Grey Level Count Emphasis: 1062.12 (71°/0.6σ)
- Joint Average: 31.6357 (80°/0.8σ)
- (C)
- In Figure 8C, an example of a False Positive, i.e., “Negative” classified as “AMD”, is shown. Almost all the 10 top predictors have values that greatly deviate from the expected distribution for “Negative” class, with five predictors assuming values over the 100° percentile, i.e., values outside of the range the predictors had in the training set. This explains why the classification model is deceived and its prediction is wrong. The values (percentile/standard deviations from the mean) are:
- Strength: 2.80782 (>100°/5.7σ)
- Contrast: 0.0186873 (1°/−1.0σ)
- Low Grey Level Count Emphasis: 0.0103925 (>100°/5.0σ)
- High Dependence Low Grey Level Emphasis: 0.224731 (>100°/5.6σ)
- Long Run Low Grey Level Emphasis: 0.0419334 (>100°/5.3σ)
- Low Grey Level Run Emphasis: 0.00976493 (>100°/4.5σ)
- Small Distance High Grey Level Emphasis: 17.2006 (3°/−1.9σ)
- Short Run Low Grey Level Emphasis: 0.00681908 (99°/4.2σ)
- High Grey Level Count Emphasis: 343.866 (6°/−1.8σ)
- Joint Average: 16.7826 (3°/−2.0σ)
- (D)
- In Figure 8D, an example of a False Negative, i.e., “AMD” classified as “Negative”, is shown. The first ranked predictor (strength) has a value under the 1° percentile and some more predictors have values at the boundaries of the distribution expected for the “AMD” class. Once again, these outlier values explain why the prediction is wrong. The values (percentile/standard deviations from the mean) are:
- Strength: 0.376468 (<1°/−1.4σ)
- Contrast: 0.0840939 (89°/1.5σ)
- Low Grey Level Count Emphasis: 0.00187011 (12°/−0.8σ)
- High Dependence Low Grey Level Emphasis: 0.00931938 (3°/−0.7σ)
- Long Run Low Grey Level Emphasis: 0.00277563 (7°/−0.7σ)
- Low Grey Level Run Emphasis: 0.00189526 (13°/−0.8σ)
- Small Distance High Grey Level Emphasis: 26.2522 (28°/−0.7σ)
- Short Run Low Grey Level Emphasis: 0.00172662 (17°/−0.7σ)
- High Grey Level Count Emphasis: 851.997 (70°/0.6σ)
- Joint Average: 28.0738 (75°/0.7σ)
4. Discussion
- NGTDM Strength: quantifies the strength of the texture; the greater the strength, the easier it is to identify and clearly see the primitives of the texture, i.e., its fundamental patterns, structures, and elements. This feature can take high values in case of large primitives (even if low-contrasted) and in case of highly-contrasted primitives (even if small) [35].
- NGTDM Contrast: quantifies how quickly the intensity values change across adjacent regions; the greater the contrast, the less smooth is the texture.
- NGLDM Low Grey Level Count Emphasis: quantifies the degree at which large dark regions are present in the image; high values of this feature indicate greater presence of such regions.
- NGLDM High Dependence Low Grey Level Emphasis: quantifies the dependence of dark regions; high values indicate that dark pixels tend to be in the same neighbourhoods.
- GLRLM Long Run Low Grey Level Emphasis: quantifies the abundance of dark and long linear structures; the darker and/or the longer the structure, the greater the contribution to this feature is.
- GLRLM Low Grey Level Run Emphasis: quantifies the abundance of linear structures, regardless of their length; the higher the value, the more linear structures are present in the image.
- GLDZM Small Distance High Grey Level Emphasis: quantifies the presence of bright regions with small distance from the ROI’s borders; very bright and very peripheral regions contribute to high values of this feature.
- GLRLM Short Run Low Grey Level Emphasis: similar to GLRLM Long Run Low Grey Level Emphasis, but small dark regions are emphasised.
- NGLDM High Grey Level Count Emphasis: similar to NGLDM Low Grey Level Count Emphasis, but large bright regions are emphasised.
- GLCM Joint Average: quantifies the smoothness of the regions in the image; high values indicate the presence of coarse regions.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Friedman, D.S.; O’Colmain, B.J.; Muñoz, B.; Tomany, S.C.; McCarty, C.; De Jong, P.T.V.M.; Nemesure, B.; Mitchell, P.; Kempen, J.; Congdon, N. Prevalence of age-related macular degeneration in the United States. Arch. Ophthalmol. 2004, 122, 564–572. [Google Scholar] [CrossRef] [PubMed]
- Green, W.R.; Enger, C. Age-related macular degeneration histopathologic studies. The 1992 Lorenz E. Zimmerman Lecture. Ophthalmology 1993, 100, 1519–1535. [Google Scholar] [CrossRef] [PubMed]
- Spaide, R.F.; Jaffe, G.J.; Sarraf, D.; Freund, K.B.; Sadda, S.R.; Staurenghi, G.; Waheed, N.K.; Chakravarthy, U.; Rosenfeld, P.J.; Holz, F.G.; et al. Consensus Nomenclature for Reporting Neovascular Age-Related Macular Degeneration Data. Ophthalmology 2020, 127, 616–636. [Google Scholar] [CrossRef] [PubMed]
- Cheung, L.K.; Eaton, A. Age-Related Macular Degeneration. Pharmacotherapy 2013, 33, 838–855. [Google Scholar] [CrossRef]
- Gheorghe, A.; Mahdi, L.; Musat, O. Age-Related Macular Degeneration. Rom. J. Ophthalmol. 2015, 59, 74–77. [Google Scholar] [PubMed]
- Bressler, N.M. Verteporfin therapy of subfoveal choroidal neovascularization in age-related macular degeneration: Two-year results of a randomized clinical trial including lesions with occult with no classic choroidal neovascularization-verteporfin in photodynamic therapy report 2. Am. J. Ophthalmol. 2002, 133, 168–169. [Google Scholar] [CrossRef] [PubMed]
- Macular Photocoagulation Study Group. Laser Photocoagulation of Subfoveal Neovascular Lesions of Age-Related Macular Degeneration: Updated Findings From Two Clinical Trials. Arch. Ophthalmol. 1993, 111, 1200–1209. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, P.J.; Brown, D.M.; Heier, J.S.; Boyer, D.S.; Kaiser, P.; Chung, C.Y.; Kim, R.Y. Ranibizumab for Neovascular Age-Related Macular Degeneration. N. Engl. J. Med. 2006, 355, 1419–1431. [Google Scholar] [CrossRef]
- Dugel, P.U.; Koh, A.; Ogura, Y.; Jaffe, G.J.; Schmidt-Erfurth, U.; Brown, D.M.; Gomes, A.V.; Warburton, J.; Weichselberger, A.; Holz, F.G. HAWK and HARRIER: Phase 3, Multicenter, Randomized, Double-Masked Trials of Brolucizumab for Neovascular Age-Related Macular Degeneration. Ophthalmology 2020, 127, 72–84. [Google Scholar] [CrossRef]
- Khanani, A.M.; Guymer, R.H.; Basu, K.; Boston, H.; Heier, J.S.; Korobelnik, J.-F.; Kotecha, A.; Lin, H.; Silverman, D.; Swaminathan, B.; et al. TENAYA and LUCERNE. Ophthalmol. Sci. 2021, 1, 100076. [Google Scholar] [CrossRef]
- Lucente, A.; Taloni, A.; Scorcia, V.; Giannaccare, G. Widefield and Ultra-Widefield Retinal Imaging: A Geometrical Analysis. Life 2023, 13, 202. [Google Scholar] [CrossRef] [PubMed]
- Choudhry, N.; Duker, J.S.; Freund, K.B.; Kiss, S.; Querques, G.; Rosen, R.; Sarraf, D.; Souied, E.H.; Stanga, P.E.; Staurenghi, G.; et al. Classification and Guidelines for Widefield Imaging. Ophthalmol. Retin. 2019, 3, 843–849. [Google Scholar] [CrossRef] [PubMed]
- Nuzzi, R.; Boscia, G.; Marolo, P.; Ricardi, F. The Impact of Artificial Intelligence and Deep Learning in Eye Diseases: A Review. Front. Med. 2021, 8, 710329. [Google Scholar] [CrossRef] [PubMed]
- Balyen, L.; Peto, T. Promising Artificial Intelligence-Machine Learning-Deep Learning Algorithms in Ophthalmology. Asia-Pacific J. Ophthalmol. (Phila.) 2019, 8, 264–272. [Google Scholar] [CrossRef]
- Ras, G.; Xie, N.; Van Gerven, M.; Doran, D. Explainable Deep Learning: A Field Guide for the Uninitiated. J. Artif. Intell. Res. 2022, 73, 329–397. [Google Scholar] [CrossRef]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 12 December 2016. [Google Scholar] [CrossRef]
- Huang, G.; Liu, Z.; van der Maaten, L.; Weinberger, K.Q. Densely Connected Convolutional Networks. Published Online 28 January 2018. Available online: http://arxiv.org/abs/1608.06993 (accessed on 29 August 2023).
- Chiappa, V.; Interlenghi, M.; Salvatore, C.; Bertolina, F.; Bogani, G.; Ditto, A.; Martinelli, F.; Castiglioni, I.; Raspagliesi, F. Using rADioMIcs and machine learning with ultrasonography for the differential diagnosis of myometRiAL tumors (the ADMIRAL pilot study). Radiomics and differential diagnosis of myometrial tumors. Gynecol. Oncol. 2021, 161, 838–844. [Google Scholar] [CrossRef]
- Chiappa, V.; Bogani, G.; Interlenghi, M.; Salvatore, C.; Bertolina, F.; Sarpietro, G.; Signorelli, M.; Castiglioni, I.; Raspagliesi, F. The Adoption of Radiomics and machine learning improves the diagnostic processes of women with Ovarian MAsses (the AROMA pilot study). J. Ultrasound 2021, 24, 429–437. [Google Scholar] [CrossRef]
- Redmon, J.; Farhadi, A. YOLO9000: Better, Faster, Stronger. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; IEEE: New York, NY, USA, 2017; pp. 6517–6525. [Google Scholar] [CrossRef]
- Deng, J.; Dong, W.; Socher, R.; Li, L.-J.; Li, K.; Fei-Fei, L. ImageNet: A large-scale hierarchical image database. In Proceedings of the 2009 IEEE Conference on Computer Vision and Pattern Recognition, Miami, FL, USA, 20–25 June 2009; IEEE: New York, NY, USA, 2009; pp. 248–255. [Google Scholar] [CrossRef]
- Dice, L.R. Measures of the Amount of Ecologic Association Between Species. Ecology 1945, 26, 297–302. [Google Scholar] [CrossRef]
- Cohen, J. A Coefficient of Agreement for Nominal Scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Zwanenburg, A.; Vallières, M.; Abdalah, M.A.; Aerts, H.J.W.L.; Andrearczyk, V.; Apte, A.; Ashrafinia, S.; Bakas, S.; Beukinga, R.J.; Boellaard, R.; et al. Image biomarker standardisation initiative. Radiology 2020, 295, 328–338. [Google Scholar] [CrossRef]
- Trace4—Technical Sheet. Available online: http://www.deeptracetech.com/files/TechnicalSheet__TRACE4.pdf (accessed on 9 January 2023).
- Shrout, P.E.; Fleiss, J.L. Intraclass correlations: Uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef] [PubMed]
- He, H.; Bai, Y.; Garcia, E.A.; Li, S. ADASYN: Adaptive synthetic sampling approach for imbalanced learning. In Proceedings of the 2008 IEEE International Joint Conference on Neural Networks (IEEE World Congress on Computational Intelligence), Hong Kong, China, 1–8 June 2008; IEEE: New York, NY, USA, 2008; pp. 1322–1328. [Google Scholar] [CrossRef]
- Bradley, A.P. The use of the area under the ROC curve in the evaluation of machine learning algorithms. Pattern Recognit. 1997, 30, 1145–1159. [Google Scholar] [CrossRef]
- Mann, H.B.; Whitney, D.R. On a Test of Whether one of Two Random Variables is Stochastically Larger than the Other. Ann. Math. Stat. 1947, 18, 50–60. [Google Scholar] [CrossRef]
- Bonferroni, C.E. Teoria Statistica Delle Classi e Calcolo Delle Probabilità; Seeber: Florence, Italy, 1936. [Google Scholar]
- Matsuba, S.; Tabuchi, H.; Ohsugi, H.; Enno, H.; Ishitobi, N.; Masumoto, H.; Kiuchi, Y. Accuracy of ultra-wide-field fundus ophthalmoscopy-assisted deep learning, a machine-learning technology, for detecting age-related macular degeneration. Int. Ophthalmol. 2018, 39, 1269–1275. [Google Scholar] [CrossRef] [PubMed]
- Keel, S.; Li, Z.; Scheetz, J.; Robman, L.; Phung, J.; Makeyeva, G.; Aung, K.; Liu, C.; Yan, X.; Meng, W.; et al. Development and validation of a deep-learning algorithm for the detection of neovascular age-related macular degeneration from colour fundus photographs. Clin. Exp. Ophthalmol. 2019, 47, 1009–1018. [Google Scholar] [CrossRef] [PubMed]
- Treder, M.; Lauermann, J.L.; Eter, N. Automated detection of exudative age-related macular degeneration in spectral domain optical coherence tomography using deep learning. Graefe’s Arch. Clin. Exp. Ophthalmol. 2018, 256, 259–265. [Google Scholar] [CrossRef]
- Burlina, P.M.; Joshi, N.; Pekala, M.; Pacheco, K.D.; Freund, D.E.; Bressler, N.M. Automated Grading of Age-Related Macular Degeneration From Color Fundus Images Using Deep Convolutional Neural Networks. JAMA Ophthalmol 2017, 135, 1170–1176. [Google Scholar] [CrossRef]
- Amadasun, M.; King, R. Textural features corresponding to textural properties. IEEE Trans. Syst. Man Cybern. 1989, 19, 1264–1274. [Google Scholar] [CrossRef]
- Zarbin, M.A.; Casaroli-Marano, R.P.; Rosenfeld, P.J. Age-Related Macular Degeneration: Clinical Findings, Histopathology and Imaging Techniques. Dev. Ophthalmol. 2014, 53, 1–32. [Google Scholar] [CrossRef]
- Liang, X.; Alshemmary, E.N.; Ma, M.; Liao, S.; Zhou, W.; Lu, Z. Automatic Diabetic Foot Prediction Through Fundus Images by Radiomics Features. IEEE Access 2021, 9, 92776–92787. [Google Scholar] [CrossRef]
- Du, Y.; Chen, Q.; Fan, Y.; Zhu, J.; He, J.; Zou, H.; Sun, D.; Xin, B.; Feng, D.; Fulham, M.; et al. Automatic identification of myopic maculopathy related imaging features in optic disc region via machine learning methods. J. Transl. Med. 2021, 19, 167. [Google Scholar] [CrossRef] [PubMed]
- Baumal, C.R. Imaging in Diabetic Retinopathy. In Current Management of Diabetic Retinopathy; Elsevier: Amsterdam, The Netherlands, 2018; pp. 25–36. [Google Scholar] [CrossRef]
- Bhambra, N.; Antaki, F.; El Malt, F.; Xu, A.; Duval, R. Deep learning for ultra-widefield imaging: A scoping review. Graefe’s Arch. Clin. Exp. Ophthalmol. 2022, 260, 3737–3778. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Training Set | Validation Set | Internal Testing Set | |
|---|---|---|---|
| (A) | |||
| ROC-AUC (%) (95% CI) | 100 ** (99–100) | 83 ** (82–83) | 84 ** (83–84) |
| Accuracy (%) (95% CI) | 100 ** (99–100) | 78 ** (78–78) | 81 ** (78–85) |
| Sensitivity (%) (95% CI) | 100 ** (99–100) | 71 ** (68–75) | 72 ** (70–74) |
| Specificity (%) (95% CI) | 100 ** (99–100) | 83 ** (80–86) | 88 ** (83–93) |
| PPV (%) (95% CI) | 100 ** (99–100) | 78 ** (77–79) | 82 ** (75–89) |
| NPV (%) (95% CI) | 100 ** (99–100) | 81 ** (79–82) | 81 ** (79–83) |
| (B) | |||
| ROC-AUC (%) (95% CI) | 96 ** (95–97) | 90 ** (89–92) | 87 ** (84–90) |
| Accuracy (%) (95% CI) | 91 ** (88–93) | 83 ** (82–85) | 83 ** (79–86) |
| Sensitivity (%) (95% CI) | 88 ** (85–91) | 80 ** (78–82) | 77 ** (69–87) |
| Specificity (%) (95% CI) | 93 ** (90–95) | 86 ** (85–87) | 87 ** (85–89) |
| PPV (%) (95% CI) | 92 ** (89–94) | 83 ** (83–83) | 82 ** (81–83) |
| NPV (%) (95% CI) | 90 ** (87–92) | 86 ** (85–88) | 84 ** (78–89) |
| Human Operator’s Manual ROI (Variable Radius) | DL-Based Macular Detector (250 Pixels Fixed Radius) | |
|---|---|---|
| Sensitivity (%) (95% CI) | 95.4 * (89.5–98.5) | 92.6 * (85.9–96.7) |
| Specificity (%) (95% CI) | 95.3 (84.2–99.4) | 74.4 ** (58.8–86.5) |
| PPV (%) (95% CI) | 98.1 (93.3–99.8) | 90.1 ** (83.0–94.9) |
| NPV (%) (95% CI) | 89.1 (76.4–96.4) | 80.0 * (64.4–90.9) |
| Rank | Feature Family | Feature Nomenclature | Median in the AMD Class (95% CI) | Median in the Negative Class (95% CI) | Uncorrected p-Value | Corrected p-Value |
|---|---|---|---|---|---|---|
| 1 | Neighbourhood Grey Tone Difference Matrix | Strength | 1.14 (0.97–1.31) | 0.63 (0.57–0.69) | <0.005 | <0.005 |
| 2 | Neighbourhood Grey Tone Difference Matrix | Contrast | 4.08 × 10−2 (3.43 × 10−2–4.72 × 10−2) | 6.60 × 10−2 (5.62 × 10−2–7.59 × 10−2) | <0.005 | <0.005 |
| 3 | Neighbouring Grey Level Dependence Matrix | Low Grey Level Count Emphasis | 3.08 × 10−3 (2.60 × 10−3–3.56 × 10−3) | 2.17 × 10−3 (1.90 × 10−3–2.45 × 10−3) | <0.005 | <0.05 |
| 4 | Neighbouring Grey Level Dependence Matrix | High Dependence Low Grey Level Emphasis | 3.91 × 10−2 (2.88 × 10−2–4.95 × 10−2) | 2.30 × 10−2 (1.93 × 10−2–2.68 × 10−2) | <0.005 | <0.05 |
| 5 | Grey-Level Run Length Matrix | Long Run Low Grey Level Emphasis | 7.75 × 10−3 (5.90 × 10−3–9.60 × 10−3) | 4.75 × 10−3 (4.01 × 10−3–5.49 × 10−3) | <0.005 | <0.05 |
| 6 | Grey-Level Run Length Matrix | Low Grey Level Run Emphasis | 3.05 × 10−3 (2.60 × 10−3–3.51 × 10−3) | 2.18 × 10−3 (1.90 × 10−3–2.46 × 10−3) | <0.005 | <0.05 |
| 7 | Grey-Level Distance Zone Matrix | Small Distance High Grey Level Emphasis | 36.59 (31.9–41.28) | 48.98 (45.88–52.07) | <0.005 | <0.05 |
| 8 | Grey-Level Run Length Matrix | Short Run Low Grey Level Emphasis | 2.57 × 10−3 (2.26 × 10−3–2.88 × 10−3) | 1.81 × 10−3 (1.60 × 10−3–2.03 × 10−3) | <0.005 | <0.05 |
| 9 | Neighbouring Grey Level Dependence Matrix | High Grey Level Count Emphasis | 684.57 (613.66–755.47) | 910.92 (839.18–982.66) | <0.005 | <0.05 |
| 10 | Grey-Level Co-Occurrence Matrix | Joint Average | 24.35 (23.02–25.67) | 28.73 (27.48–29.97) | <0.005 | 5.72 × 10−2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Interlenghi, M.; Sborgia, G.; Venturi, A.; Sardone, R.; Pastore, V.; Boscia, G.; Landini, L.; Scotti, G.; Niro, A.; Moscara, F.; et al. A Radiomic-Based Machine Learning System to Diagnose Age-Related Macular Degeneration from Ultra-Widefield Fundus Retinography. Diagnostics 2023, 13, 2965. https://doi.org/10.3390/diagnostics13182965
Interlenghi M, Sborgia G, Venturi A, Sardone R, Pastore V, Boscia G, Landini L, Scotti G, Niro A, Moscara F, et al. A Radiomic-Based Machine Learning System to Diagnose Age-Related Macular Degeneration from Ultra-Widefield Fundus Retinography. Diagnostics. 2023; 13(18):2965. https://doi.org/10.3390/diagnostics13182965
Chicago/Turabian StyleInterlenghi, Matteo, Giancarlo Sborgia, Alessandro Venturi, Rodolfo Sardone, Valentina Pastore, Giacomo Boscia, Luca Landini, Giacomo Scotti, Alfredo Niro, Federico Moscara, and et al. 2023. "A Radiomic-Based Machine Learning System to Diagnose Age-Related Macular Degeneration from Ultra-Widefield Fundus Retinography" Diagnostics 13, no. 18: 2965. https://doi.org/10.3390/diagnostics13182965