
Low-Cost Point-of-Care Monitoring of ALT and AST Is Promising for Faster Decision Making and Diagnosis of Acute Liver Injury

 , , , and
, , , and
Abstract
:1. Introduction
2. Hypothesis: Robust and Rapid Method for ALT Diagnosis at the Point-of-Care Testing for Monitoring Liver Damage and Function
3. Evaluation of Hypothesis: Point-of-Care Test for Diagnosis and Monitoring Liver Function Using ALT and AST Enzymes
4. Consequences of the Hypothesis and Discussion
5. Conclusions and Future Prospects

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Analyte | Analytical Method | Materials Used | Detection Range | LOD | Reference |
|---|---|---|---|---|---|
| ALT/AST | Hydrogel-Colorimetric | Au-decorated CoAl-layered double oxide (Au/LDO) | - | 15 U/L (ALT) 10 U/L (AST) | [44] |
| ALT | Paper-based Colorimetry | 2,4-dinitrophenyl hydrazine | 20–140 U/L | 4.12 U/L | [45] |
| ALT | Paper-based Colorimetry | ALT assay Chemistry * | 40–200 U/L | 53 U/L | [41] |
| AST | Paper-based Colorimetry | AST assay Chemistry ** | 40–200 | 84 U/L | [41] |
| ALT | Paper-based Colorimetry | Inkjet Printer | 5.38–8.61 | N/A | [21] |
| AST | Paper-based Colorimetry | Inkjet Printer | 5.4–91.2 | N/A | [21] |
| ALT | Colorimetry | B-doped core–shell Fe@BC nanozyme/L-alanine and α-ketoglutarate | 10–1000 | 4 U/L | [34] |
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ohgo, H.; Yokoyama, H.; Hirose, H.; Kawabe, H.; Saito, I.; Tomita, K.; Hibi, T. Significance of ALT/AST Ratio for Specifying Subjects with Metabolic Syndrome in Its Silent Stage. Diabetes Metab. Syndr. Clin. Res. Rev. 2009, 3, 3–6. [Google Scholar] [CrossRef]
- Marchesini, G.; Moscatiello, S.; Di Domizio, S.; Forlani, G. Obesity-Associated Liver Disease. J. Clin. Endocrinol. Metab. 2008, 93, s74–s80. [Google Scholar] [CrossRef] [PubMed]
- Jalili, V.; Poorahmadi, Z.; Hasanpour Ardekanizadeh, N.; Gholamalizadeh, M.; Ajami, M.; Houshiarrad, A.; Hajipour, A.; Shafie, F.; Alizadeh, A.; Mokhtari, Z.; et al. The Association between Obesity with Serum Levels of Liver Enzymes, Alanine Aminotransferase, Aspartate Aminotransferase, Alkaline Phosphatase and Gamma-Glutamyl Transferase in Adult Women. Endocrinol. Diabetes Metab. 2022, 5, e367. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.R.; Flamm, S.L.; Di Bisceglie, A.M.; Bodenheimer, H.C.; Public Policy Committee of the American Association for the Study of Liver Disease. Serum Activity of Alanine Aminotransferase (ALT) as an Indicator of Health and Disease. Hepatology 2008, 47, 1363–1370. [Google Scholar] [CrossRef]
- Schomaker, S.; Warner, R.; Bock, J.; Johnson, K.; Potter, D.; Van Winkle, J.; Aubrecht, J. Assessment of Emerging Biomarkers of Liver Injury in Human Subjects. Toxicol. Sci. 2013, 132, 276–283. [Google Scholar] [CrossRef]
- Malakouti, M.; Kataria, A.; Ali, S.K.; Schenker, S. Elevated Liver Enzymes in Asymptomatic Patients–What Should I Do? J. Clin. Transl. Hepatol. 2017, 5, 394. [Google Scholar] [CrossRef]
- Vernon, G.; Baranova, A.; Younossi, Z. Systematic Review: The Epidemiology and Natural History of Non-alcoholic Fatty Liver Disease and Non-alcoholic Steatohepatitis in Adults. Aliment. Pharmacol. Ther. 2011, 34, 274–285. [Google Scholar] [CrossRef]
- Schindhelm, R.K.; Diamant, M.; Dekker, J.M.; Tushuizen, M.E.; Teerlink, T.; Heine, R.J. Alanine Aminotransferase as a Marker of Non-alcoholic Fatty Liver Disease in Relation to Type 2 Diabetes Mellitus and Cardiovascular Disease. Diabetes Metab. Res. Rev. 2006, 22, 437–443. [Google Scholar] [CrossRef]
- Newsome, P.N.; Cramb, R.; Davison, S.M.; Dillon, J.F.; Foulerton, M.; Godfrey, E.M.; Hall, R.; Harrower, U.; Hudson, M.; Langford, A. Guidelines on the Management of Abnormal Liver Blood Tests. Gut 2018, 67, 6–19. [Google Scholar] [CrossRef]
- Lippi, U.; Guidi, G. A New Colorimetric Ultramicromethod for Serum Glutamicoxalacetic and Glutamic-Pyruvic Transaminase Determination. Clin. Chim. Acta 1970, 28, 431–437. [Google Scholar] [CrossRef]
- Rodgerson, D.O.; Osberg, I.M. Sources of Error in Spectrophotometric Measurement of Aspartate Aminotransferase and Alanine Aminotransferase Activities in Serum. Clin. Chem. 1974, 20, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Paraíso, L.F.; Paula, L.; Franco, D.L.; Madurro, J.M.; Brito-Madurro, A.G. Bioelectrochemical Detection of Alanine Aminotransferase for Molecular Diagnostic of the Liver Disease. Int. J. Electrochem. Sci. 2014, 9, 1286–1297. [Google Scholar] [CrossRef]
- Xuan, G.S.; Oh, S.W.; Choi, E.Y. Development of an Electrochemical Immunosensor for Alanine Aminotransferase. Biosens. Bioelectron. 2003, 19, 365–371. [Google Scholar] [CrossRef]
- Wang, Z.; Singh, R.; Marques, C.; Jha, R.; Zhang, B.; Kumar, S. Taper-in-Taper Fiber Structure-Based LSPR Sensor for Alanine Aminotransferase Detection. Opt. Express 2021, 29, 43793–43810. [Google Scholar] [CrossRef]
- Martinez, A.W.; Phillips, S.T.; Whitesides, G.M.; Carrilho, E. Diagnostics for the Developing World: Microfluidic Paper-Based Analytical Devices. Anal. Chem. 2010, 82, 3–10. [Google Scholar] [CrossRef]
- Reches, M.; Mirica, K.A.; Dasgupta, R.; Dickey, M.D.; Butte, M.J.; Whitesides, G.M. Thread as a Matrix for Biomedical Assays. ACS Appl. Mater. Interfaces 2010, 2, 1722–1728. [Google Scholar] [CrossRef]
- Mirica, K.A.; Phillips, S.T.; Mace, C.R.; Whitesides, G.M. Magnetic Levitation in the Analysis of Foods and Water. J. Agric. Food Chem. 2010, 58, 6565–6569. [Google Scholar] [CrossRef]
- Chinnappan, R.; Mir, T.A.; Alsalameh, S.; Makhzoum, T.; Alzhrani, A.; Alnajrani, M.K.; Adeeb, S.; Al Eman, N.; Ahmed, Z.; Shakir, I.; et al. Emerging Biosensing Methods to Monitor Lung Cancer Biomarkers in Biological Samples: A Comprehensive Review. Cancers 2023, 15, 3414. [Google Scholar] [CrossRef]
- Cheng, C.; Martinez, A.W.; Gong, J.; Mace, C.R.; Phillips, S.T.; Carrilho, E.; Mirica, K.A.; Whitesides, G.M. Paper-based ELISA. Angew. Chem. 2010, 122, 4881–4884. [Google Scholar] [CrossRef]
- Baek, S.H.; Park, C.; Jeon, J.; Park, S. Three-Dimensional Paper-Based Microfluidic Analysis Device for Simultaneous Detection of Multiple Biomarkers with a Smartphone. Biosensors 2020, 10, 187. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.-L.; Chu, C.-H.; Tsai, S.-J.; Yang, R.-J. Aspartate Aminotransferase and Alanine Aminotransferase Detection on Paper-Based Analytical Devices with Inkjet Printer-Sprayed Reagents. Micromachines 2016, 7, 9. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.-J.; Choi, Y.-K.; Im, H.-S.; Yarimaga, O.; Yoon, E.; Kim, H.-S. Aspartate Aminotransferase (AST/GOT) and Alanine Aminotransferase (ALT/GPT) Detection Techniques. Sensors 2006, 6, 756–782. [Google Scholar] [CrossRef]
- Chinnappan, R.; Zaghloul, N.S.; AlZabn, R.; Malkawi, A.; Abdel Rahman, A.; Abu-Salah, K.M.; Zourob, M. Aptamer Selection and Aptasensor Construction for Bone Density Biomarkers. Talanta 2021, 224, 121818. [Google Scholar] [CrossRef] [PubMed]
- Alomran, N.; Chinnappan, R.; Alsolaiss, J.; Casewell, N.R.; Zourob, M. Exploring the Utility of SsDNA Aptamers Directed against Snake Venom Toxins as New Therapeutics for Snakebite Envenoming. Toxins 2022, 14, 469. [Google Scholar] [CrossRef]
- Zhou, W.; Saran, R.; Liu, J. Metal Sensing by DNA. Chem. Rev. 2017, 117, 8272–8325. [Google Scholar] [CrossRef]
- Chinnappan, R.; Ramadan, Q.; Zourob, M. An Integrated Lab-on-a-Chip Platform for Pre-Concentration and Detection of Colorectal Cancer Exosomes Using Anti-CD63 Aptamer as a Recognition Element. Biosens. Bioelectron. 2023, 220, 114856. [Google Scholar] [CrossRef] [PubMed]
- Chinnappan, R.; Rahamn, A.A.; AlZabn, R.; Kamath, S.; Lopata, A.L.; Abu-Salah, K.M.; Zourob, M. Aptameric Biosensor for the Sensitive Detection of Major Shrimp Allergen, Tropomyosin. Food Chem. 2020, 314, 126133. [Google Scholar] [CrossRef]
- Chinnappan, R.; Mir, T.A.; Alsalameh, S.; Makhzoum, T.; Adeeb, S.; Al-Kattan, K.; Yaqinuddin, A. Aptasensors Are Conjectured as Promising ALT and AST Diagnostic Tools for the Early Diagnosis of Acute Liver Injury. Life 2023, 13, 1273. [Google Scholar] [CrossRef]
- Alnajrani, M.N.; Aljohani, M.M.; Chinnappan, R.; Zourob, M.; Alsager, O.A. Highly Sensitive and Selective Lateral Flow Aptasensor for Anti-Coagulant Dabigatran Etexilate Determination in Blood. Talanta 2022, 236, 122887. [Google Scholar] [CrossRef]
- Janasek, D.; Spohn, U. Chemiluminometric Flow Injection Analysis Procedures for the Enzymatic Determination of L-Alanine, α-Ketoglutarate and L-Glutamate. Biosens. Bioelectron. 1999, 14, 123–129. [Google Scholar] [CrossRef]
- Ohmori, S.; Tanaka, Y.; Ikeda, M.; Hirota, K. A Sensitive Determination of α-Keto Acids by Gas-Liquid Chromatography and Its Application to the Assay of l-Glutamate Dehydrogenase and Aminotransferases. Anal. Biochem. 1981, 112, 204–212. [Google Scholar] [CrossRef] [PubMed]
- Rietz, B.; Guilbault, G. Fluorimetric Assay of Serum Glutamate Oxaloacetate Transaminase, Glutamate Pyruvate Transaminase and α-Hydroxybutyrate Dehydrogenàse by Solution An. Anal. Chim. Acta 1975, 77, 191–198. [Google Scholar] [CrossRef]
- Peguin, S.; Coulet, P.R.; Bardeletti, G. Pyruvate Oxidase and Oxaloacetate Decarboxylase Enzyme Electrodes: Simultaneous Determination of Transaminases with a Two-Electrode-Based Analyzer. Anal. Chim. Acta 1989, 222, 83–93. [Google Scholar] [CrossRef]
- Tian, D.; Xiang, W.; Wang, H.; Jiang, W.; Li, T.; Yang, M. Optical Assay Using B-Doped Core–Shell Fe@ BC Nanozyme for Determination of Alanine Aminotransferase. Microchim. Acta 2022, 189, 147. [Google Scholar] [CrossRef] [PubMed]
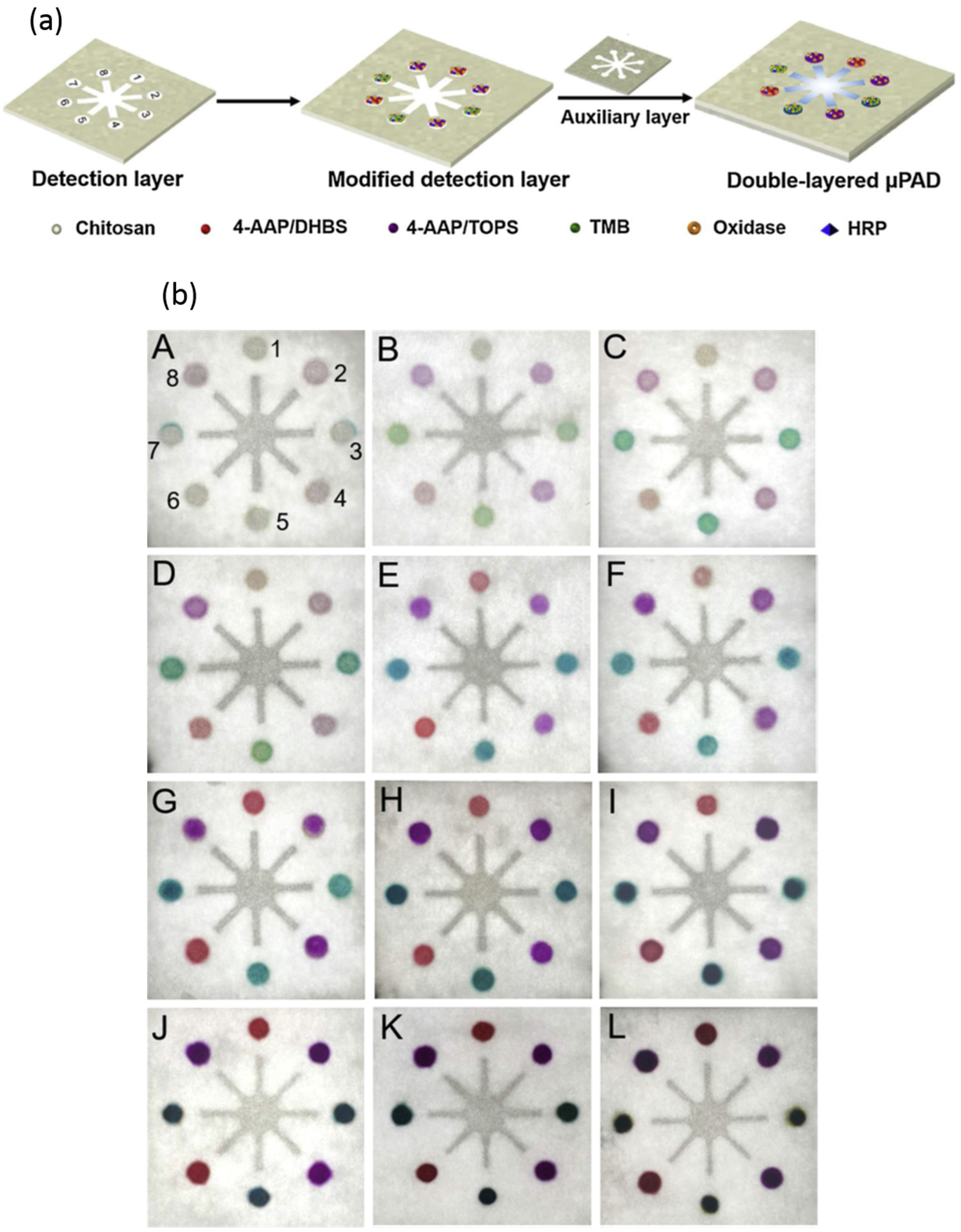
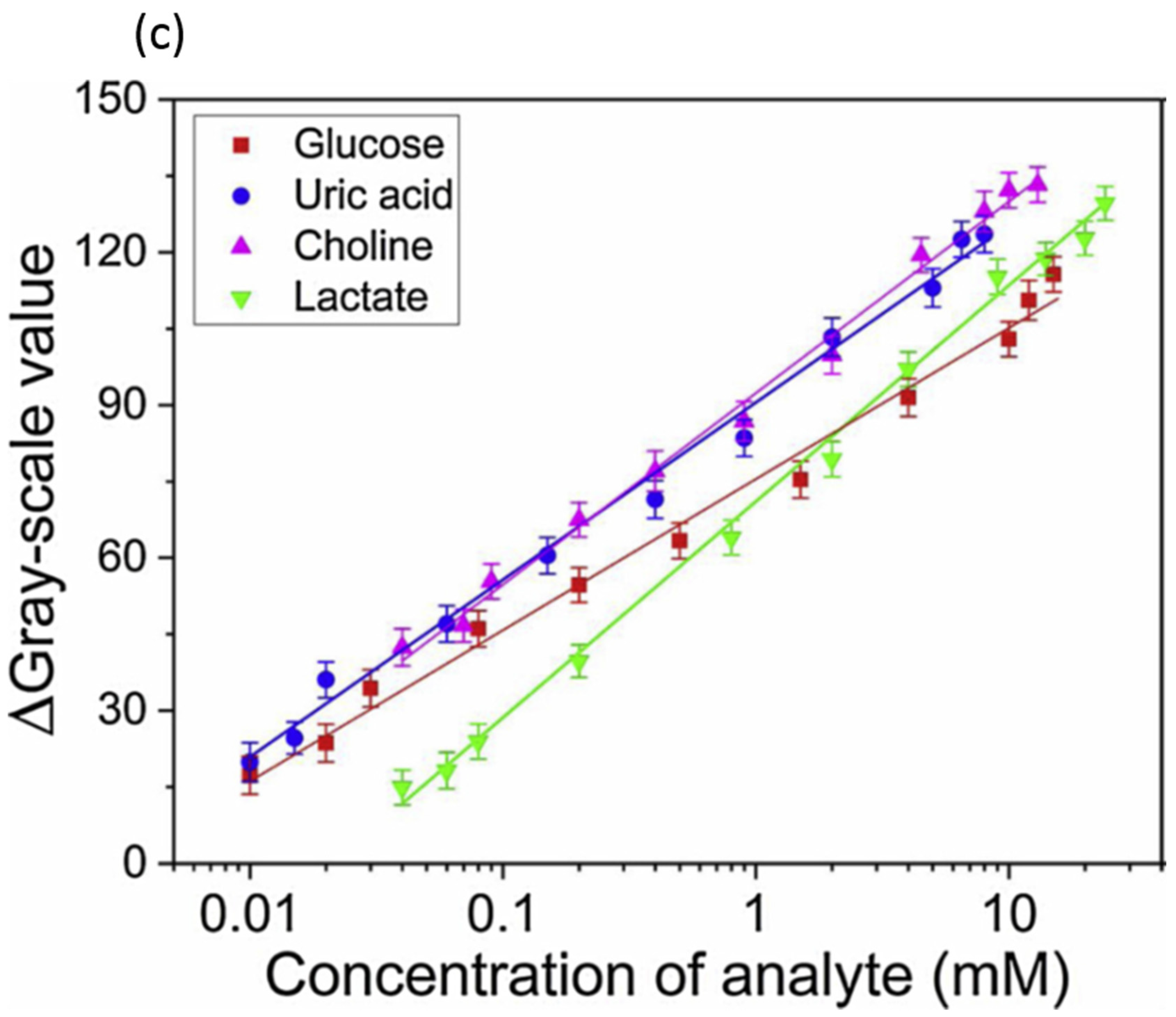
- Li, F.; Wang, X.; Liu, J.; Hu, Y.; He, J. Double-Layered Microfluidic Paper-Based Device with Multiple Colorimetric Indicators for Multiplexed Detection of Biomolecules. Sens. Actuators B Chem. 2019, 288, 266–273. [Google Scholar] [CrossRef]
- Ellerbee, A.K.; Phillips, S.T.; Siegel, A.C.; Mirica, K.A.; Martinez, A.W.; Striehl, P.; Jain, N.; Prentiss, M.; Whitesides, G.M. Quantifying Colorimetric Assays in Paper-Based Microfluidic Devices by Measuring the Transmission of Light through Paper. Anal. Chem. 2009, 81, 8447–8452. [Google Scholar] [CrossRef]
- Noviana, E.; Ozer, T.; Carrell, C.S.; Link, J.S.; McMahon, C.; Jang, I.; Henry, C.S. Microfluidic Paper-Based Analytical Devices: From Design to Applications. Chem. Rev. 2021, 121, 11835–11885. [Google Scholar] [CrossRef]
- Martinez, A.W.; Phillips, S.T.; Carrilho, E.; Thomas III, S.W.; Sindi, H.; Whitesides, G.M. Simple Telemedicine for Developing Regions: Camera Phones and Paper-Based Microfluidic Devices for Real-Time, off-Site Diagnosis. Anal. Chem. 2008, 80, 3699–3707. [Google Scholar] [CrossRef]
- Martinez, A.W.; Phillips, S.T.; Butte, M.J.; Whitesides, G.M. Patterned Paper as a Platform for Inexpensive, Low-volume, Portable Bioassays. Angew. Chem. 2007, 119, 1340–1342. [Google Scholar] [CrossRef]
- Vella, S.J.; Beattie, P.; Cademartiri, R.; Laromaine, A.; Martinez, A.W.; Phillips, S.T.; Mirica, K.A.; Whitesides, G.M. Measuring Markers of Liver Function Using a Micropatterned Paper Device Designed for Blood from a Fingerstick. Anal. Chem. 2012, 84, 2883–2891. [Google Scholar] [CrossRef]
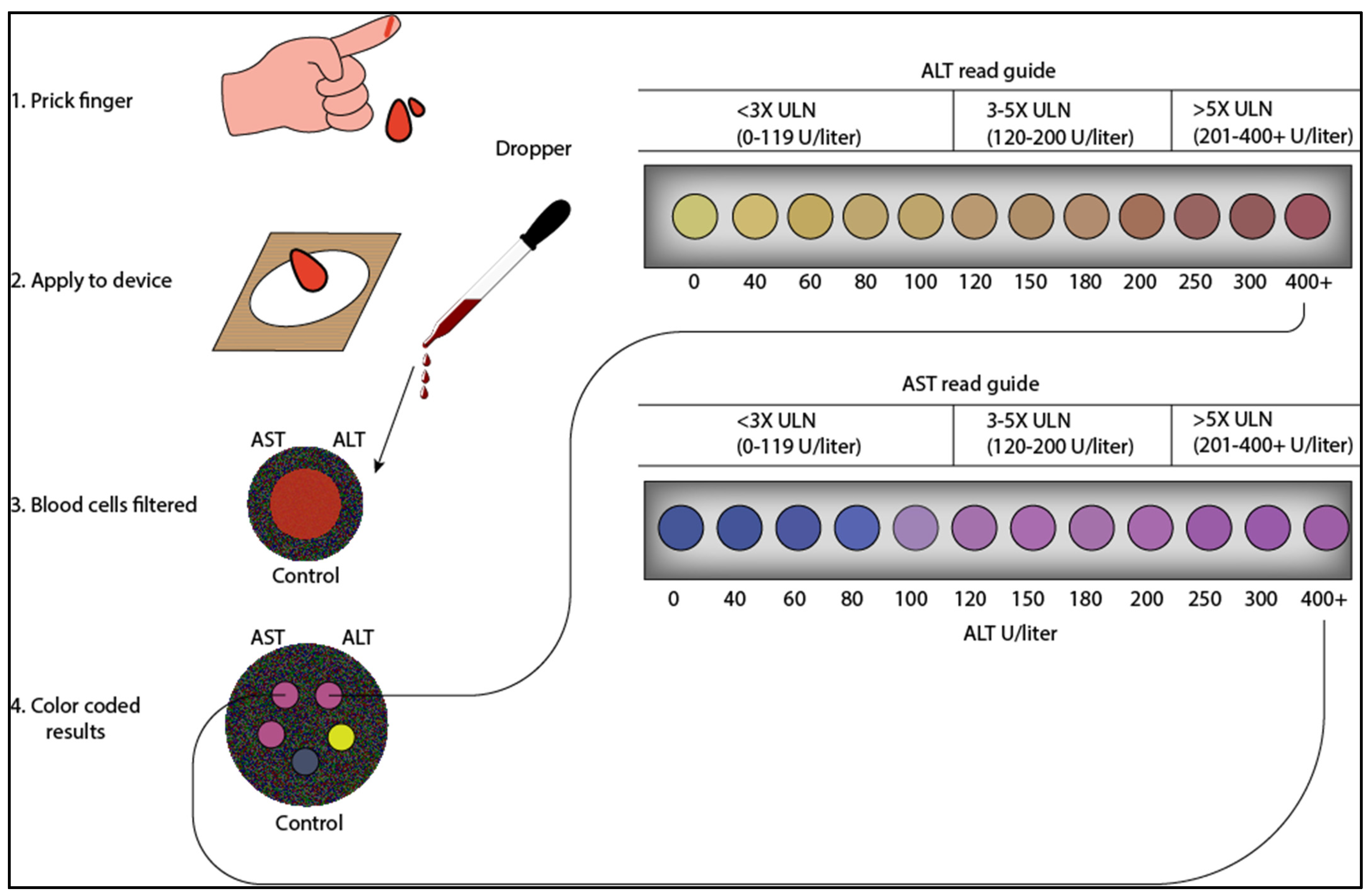
- Pollock, N.R.; Rolland, J.P.; Kumar, S.; Beattie, P.D.; Jain, S.; Noubary, F.; Wong, V.L.; Pohlmann, R.A.; Ryan, U.S.; Whitesides, G.M. A Paper-Based Multiplexed Transaminase Test for Low-Cost, Point-of-Care Liver Function Testing. Sci. Transl. Med. 2012, 4, 152ra129. [Google Scholar] [CrossRef] [PubMed]
- Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents with HIV (Department of Health and Human Services, Washington, DC 2021). 2021. Available online: https://Clinicalinfo.Hiv.Gov/Sites/Default/Files/Guidelines/Archive/AdultandAdolescentGL_2021_08_16.Pdf (accessed on 5 June 2023).
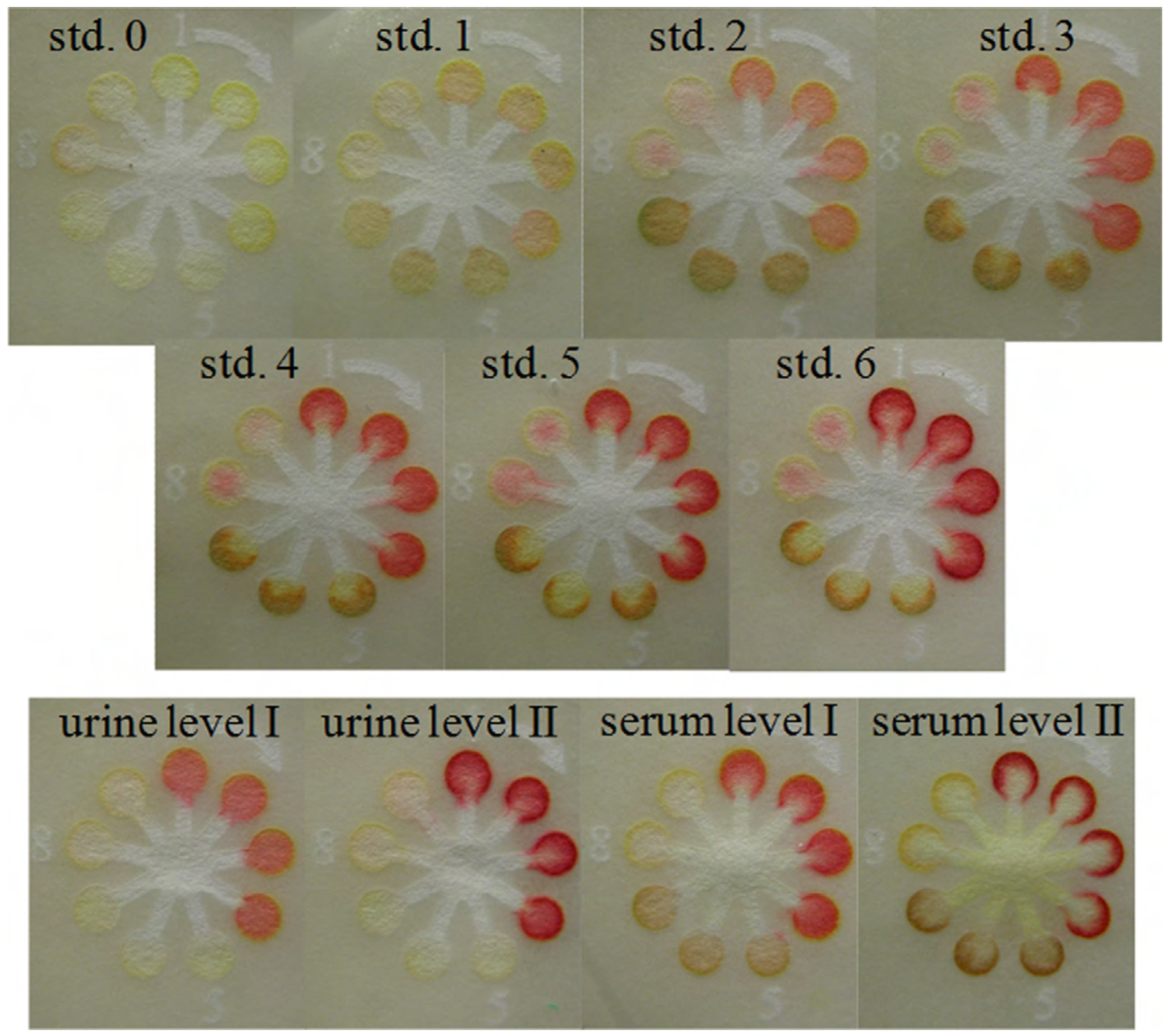
- Dungchai, W.; Chailapakul, O.; Henry, C.S. Use of Multiple Colorimetric Indicators for Paper-Based Microfluidic Devices. Anal. Chim. Acta 2010, 674, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Mei, X.; Yang, J.; Li, Y. Hydrogel-Involved Colorimetric Platforms Based on Layered Double Oxide Nanozymes for Point-of-Care Detection of Liver-Related Biomarkers. ACS Appl. Mater. Interfaces 2022, 14, 6985–6993. [Google Scholar] [CrossRef] [PubMed]
- Resmi, P.E.; Sachin Kumar, S.; Alageswari, D.; Suneesh, P.V.; Ramachandran, T.; Nair, B.G.; Satheesh Babu, T.G. Development of a Paper-Based Analytical Device for the Colourimetric Detection of Alanine Transaminase and the Application of Deep Learning for Image Analysis. Anal. Chim. Acta 2021, 1188, 339158. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chinnappan, R.; Mir, T.A.; Alsalameh, S.; Makhzoum, T.; Alzhrani, A.; Al-Kattan, K.; Yaqinuddin, A. Low-Cost Point-of-Care Monitoring of ALT and AST Is Promising for Faster Decision Making and Diagnosis of Acute Liver Injury. Diagnostics 2023, 13, 2967. https://doi.org/10.3390/diagnostics13182967
Chinnappan R, Mir TA, Alsalameh S, Makhzoum T, Alzhrani A, Al-Kattan K, Yaqinuddin A. Low-Cost Point-of-Care Monitoring of ALT and AST Is Promising for Faster Decision Making and Diagnosis of Acute Liver Injury. Diagnostics. 2023; 13(18):2967. https://doi.org/10.3390/diagnostics13182967
Chicago/Turabian StyleChinnappan, Raja, Tanveer Ahmad Mir, Suliman Alsalameh, Tariq Makhzoum, Alaa Alzhrani, Khaled Al-Kattan, and Ahmed Yaqinuddin. 2023. "Low-Cost Point-of-Care Monitoring of ALT and AST Is Promising for Faster Decision Making and Diagnosis of Acute Liver Injury" Diagnostics 13, no. 18: 2967. https://doi.org/10.3390/diagnostics13182967