

Evaluation of Different Registration Algorithms to Reduce Motion Artifacts in CT-Thermography (CTT)
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
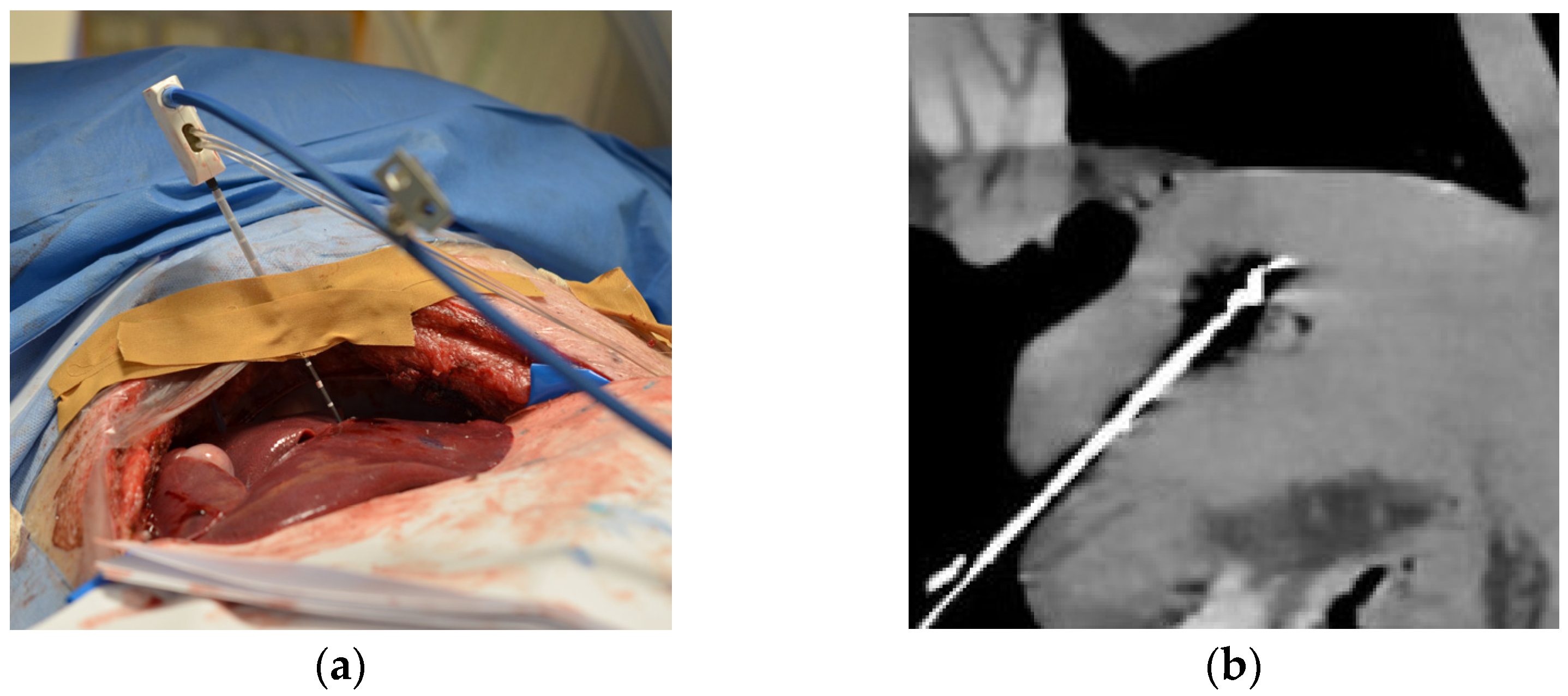
2.1. Experimental Setup and Protocol
2.2. Image Reconstruction and Registration
2.3. Image Rating
2.4. Quantitative Analysis
2.5. Statistics
3. Results
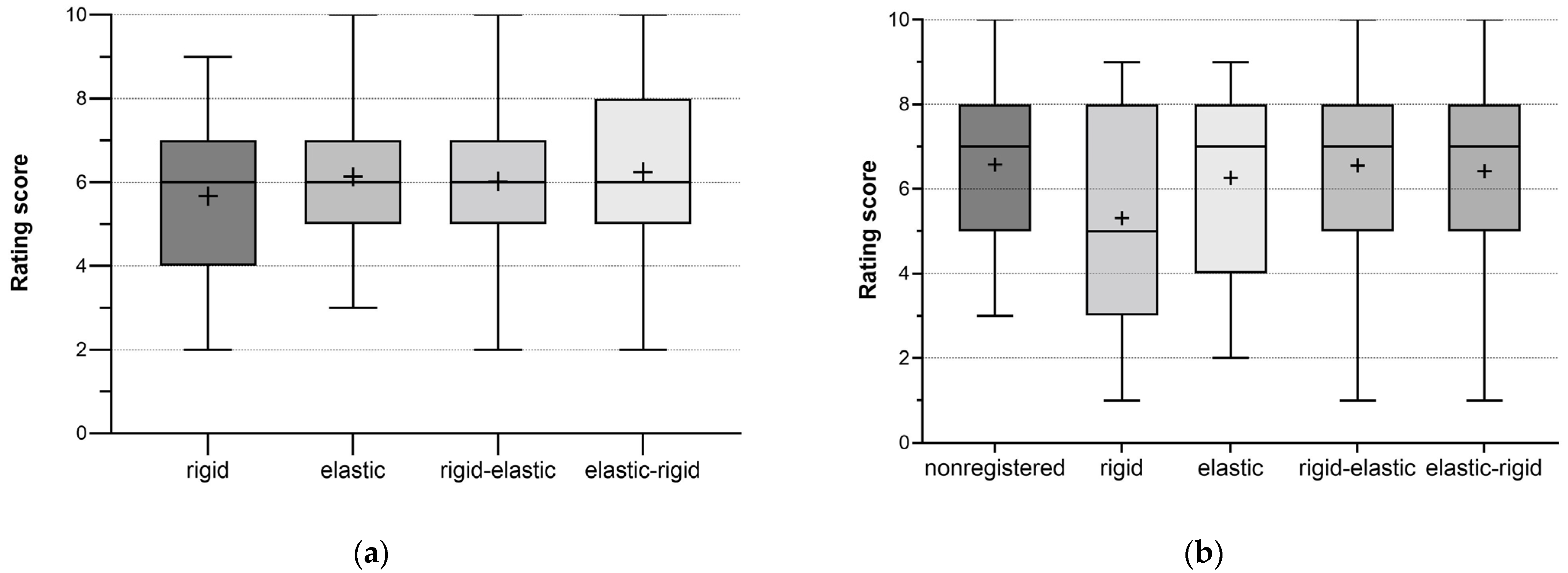
3.1. Subjective Assessment of Image Registration
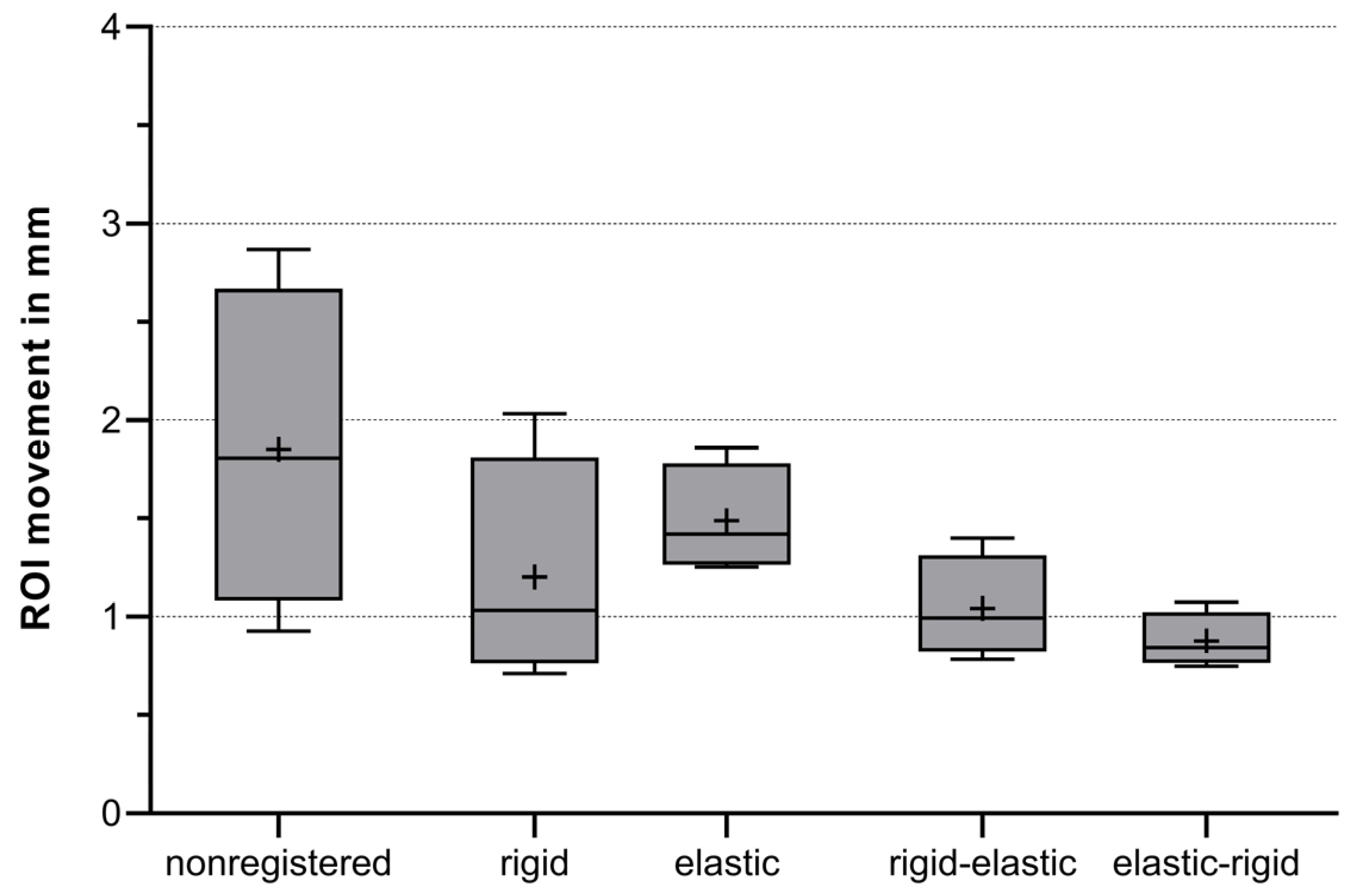
3.2. Quantitative Analysis
4. Discussion
5. Summary
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abitabile, P.; Hartl, U.; Lange, J.; Maurer, C.A. Radiofrequency ablation permits an effective treatment for colorectal liver metastasis. Eur. J. Surg. Oncol. EJSO 2007, 33, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Izzo, F.; Granata, V.; Grassi, R.; Fusco, R.; Palaia, R.; Delrio, P.; Carrafiello, G.; Azoulay, D.; Petrillo, A.; Curley, S.A. Radiofrequency Ablation and Microwave Ablation in Liver Tumors: An Update. Oncologist 2019, 24, e990–e1005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruners, P.; Levit, E.; Penzkofer, T.; Isfort, P.; Ocklenburg, C.; Schmidt, B.; Schmitz-Rode, T.; Günther, R.W.; Mahnken, A.H. Multi-slice computed tomography: A tool for non-invasive temperature measurement? Int. J. Hyperth. 2010, 26, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Seror, O.; Lepetit-Coiffé, M.; Quesson, B.; Trillaud, H.; Moonen, C.T.W. Quantitative magnetic resonance temperature mapping for real-time monitoring of radiofrequency ablation of the liver: An ex vivo study. Eur. Radiol. 2006, 16, 2265–2274. [Google Scholar] [CrossRef]
- Fani, F.; Schena, E.; Saccomandi, P.; Silvestri, S. CT-based thermometry: An overview. Int. J. Hyperth. 2014, 30, 219–227. [Google Scholar] [CrossRef]
- Bressem, K.K.; Vahldiek, J.L.; Erxleben, C.; Poch, F.; Hiebl, B.; Lehmann, K.; Hamm, B.; Niehues, S.M. Instant Outcome Evaluation of Microwave Ablation with Subtraction CT in an In Vivo Porcine Model. Investig. Radiol. 2019, 54, 333–339. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [Green Version]
- Du, H.; Tan, X.; Cheng, L.; Zhang, B.; Wang, D. Application and Evaluation of a 64-Slice CT Three-Dimensional Fusion Technique in the Determination of the Effective Ablation Margin after Radiofrequency Ablation of Hepatocellular Carcinoma. Comput. Math. Methods Med. 2022, 2022, 6898233. [Google Scholar] [CrossRef]
- Pandeya, G.D.; Greuter, M.J.W.; Schmidt, B.; Flohr, T.; Oudkerk, M. Assessment of thermal sensitivity of CT during heating of liver: An ex vivo study. Br. J. Radiol. 2012, 85, e661–e665. [Google Scholar] [CrossRef] [Green Version]
- Pohlan, J.; Kress, W.; Hermann, K.G.; Mews, J.; Kroes, M.; Hamm, B.; Diekhoff, T. Computed Tomography Thermography for Ablation Zone Prediction in Microwave Ablation and Cryoablation: Advantages and Challenges in an Ex Vivo Porcine Liver Model. J. Comput. Assist. Tomogr. 2020, 44, 744–749. [Google Scholar] [CrossRef]
- Heinrich, A.; Schenkl, S.; Buckreus, D.; Güttler, F.V.; Teichgräber, U.K.M. CT-based thermometry with virtual monoenergetic images by dual-energy of fat, muscle and bone using FBP, iterative and deep learning-based reconstruction. Eur. Radiol. 2022, 32, 424–431. [Google Scholar] [CrossRef] [PubMed]
- Precup, C.G.; Gonganau-Nitu, D.; Scurtu, R.R.; Dindelegan, G.; Biro, A.; Soritau, O.; Crişan, C.; Serban, O.; Pufu, G.; Ciuce, C. Assessement by laser Doppler of the peripheral tumour perfusion after radiofrequency ablation for colorectal liver mestasis--experimental study. Chirurgia 2010, 105, 71–76. [Google Scholar]
- Ogan, K.; Roberts, W.W.; Wilhelm, D.M.; Bonnell, L.; Leiner, D.; Lindberg, G.; Kavoussi, L.R.; Cadeddu, J.A. Infrared thermography and thermocouple mapping of radiofrequency renal ablation to assess treatment adequacy and ablation margins. Urology 2003, 62, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.D.; Ravi, V.; Rhodes, P.; Du-Fay-de-Lavallaz, J.M.; Winterfield, J.; Allen-Proctor, M.; Wasserlauf, J.; Krishnan, K.; Trohman, R.; Sharma, P.S.; et al. Use of infrared thermography to delineate temperature gradients and critical isotherms during catheter ablation with normal and half normal saline: Implications for safety and efficacy. J. Cardiovasc. Electrophysiol. 2021, 32, 2035–2044. [Google Scholar] [CrossRef] [PubMed]
- Lewis, M.A.; Staruch, R.M.; Chopra, R. Thermometry and ablation monitoring with ultrasound. Int. J. Hyperth. 2015, 31, 163–181. [Google Scholar] [CrossRef] [Green Version]
- Zhu, M.; Sun, Z.; Ng, C.K. Image-guided thermal ablation with MR-based thermometry. Quant. Imaging Med. Surg. 2017, 7, 356–368. [Google Scholar] [CrossRef] [Green Version]
- Gao, X.; Tian, Z.; Cheng, Y.; Geng, B.; Chen, S.; Nan, Q. Experimental and numerical study of microwave ablation on ex-vivo porcine lung. Electromagn. Biol. Med. 2019, 38, 249–261. [Google Scholar] [CrossRef]
- Skornitzke, S.; Fritz, F.; Klauss, M.; Pahn, G.; Hansen, J.; Hirsch, J.; Grenacher, L.; Kauczor, H.U.; Stiller, W. Qualitative and quantitative evaluation of rigid and deformable motion correction algorithms using dual-energy CT images in view of application to CT perfusion measurements in abdominal organs affected by breathing motion. Br. J. Radiol. 2015, 88, 20140683. [Google Scholar] [CrossRef] [Green Version]
- Piper, J.; Ikeda, Y.; Fujisawa, Y.; Ohno, Y.; Yoshikawa, T.; O’Neil, A.; Poole, I. Objective evaluation of the correction by non-rigid registration of abdominal organ motion in low-dose 4D dynamic contrast-enhanced CT. Phys. Med. Biol. 2012, 57, 1701–1715. [Google Scholar] [CrossRef]
- Gondim Teixeira, P.A.; Hossu, G.; Lecocq, S.; Razeto, M.; Louis, M.; Blum, A. Bone marrow edema pattern identification in patients with lytic bone lesions using digital subtraction angiography-like bone subtraction on large-area detector computed tomography. Investig. Radiol. 2014, 49, 156–164. [Google Scholar] [CrossRef]
- Crum, W.R.; Hartkens, T.; Hill, D.L.G. Non-rigid image registration: Theory and practice. Br. J. Radiol. 2004, 77, S140–S153. [Google Scholar] [CrossRef] [PubMed]
- Lell, M.M.; Ditt, H.; Panknin, C.; Sayre, J.W.; Ruehm, S.G.; Klotz, E.; Tomandl, B.F.; Villablanca, J.P. Bone-subtraction CT angiography: Evaluation of two different fully automated image-registration procedures for interscan motion compensation. Am. J. Neuroradiol. 2007, 28, 1362–1368. [Google Scholar] [CrossRef] [Green Version]
- Oh, S.; Kim, S. Deformable image registration in radiation therapy. Radiat. Oncol. J. 2017, 35, 101–111. [Google Scholar] [CrossRef]
- Frackowiak, R.S.J.; Friston, K.J.; Frith, C.D.; Dolan, R.J.; Price, C.J.; Zeki, S.; Ashburner, J.T.; Penny, W.D. (Eds.) Chapter 32—Rigid Body Registration. In Human Brain Function, 2nd ed.; Academic Press: Amsterdam, The Netherlands, 2004; pp. 635–653. [Google Scholar]
- Genske, U.; Jahnke, P. Human Observer Net: A Platform Tool for Human Observer Studies of Image Data. Radiology 2022, 303, 524–530. [Google Scholar] [CrossRef]
- Ziemlewicz, T.J.; Hinshaw, J.L.; Lubner, M.G.; Knott, E.A.; Willey, B.J.; Lee, F.T., Jr.; Brace, C.L. Radiofrequency and microwave ablation in a porcine liver model: Non-contrast CT and ultrasound radiologic-pathologic correlation. Int. J. Hyperth. 2020, 37, 799–807. [Google Scholar] [CrossRef]
- Luu, H.M.; Klink, C.; Niessen, W.; Moelker, A.; Walsum, T. Non-Rigid Registration of Liver CT Images for CT-Guided Ablation of Liver Tumors. PLoS ONE 2016, 11, e0161600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koo, T.K.; Li, M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Clements, L.W.; Collins, J.A.; Weis, J.A.; Simpson, A.L.; Kingham, T.P.; Jarnagin, W.R.; Miga, M.I. Deformation correction for image guided liver surgery: An intraoperative fidelity assessment. Surgery 2017, 162, 537–547. [Google Scholar] [CrossRef] [PubMed]
- Chandler, A.; Wei, W.; Anderson, E.F.; Herron, D.H.; Ye, Z.; Ng, C.S. Validation of motion correction techniques for liver CT perfusion studies. Br. J. Radiol. 2012, 85, e514–e522. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Criterion | Lowest Score of 1 | Highest Score of 10 |
|---|---|---|
| Quality of the registration | poor registration quality | excellent registration quality |
| Ablation zone movement | zone moves around | zone is fixed in image |
| Ablation probe movement | probe moves around | probe fixed in image |
| Tissue distortion | distinct tissue distortions | no tissue distortions |
| Image artifacts | distinct image artifacts | no image artifacts |
| Criterion/ Registration | Registration Quality | Zone Movement | Probe Movement | Tissue Distortion | Image Artifacts |
|---|---|---|---|---|---|
| non-registered | 6.5 ± 1.9 | 6.9 ± 1.9 | 6.2 ± 1.9 | 6.8 ± 1.7 | 5.5 ± 1.8 |
| rigid | 5.6 ± 1.7 | 6.3 ± 1.9 | 5.3 ± 2.4 | 5.9 ± 2.2 | 4.8 ± 2.0 |
| elastic | 6.1 ± 1.7 | 6.7 ± 1.8 | 6.3 ± 2.1 | 6.8 ± 1.7 | 5.2 ± 1.7 |
| rigid-elastic | 6.0 ± 1.8 | 6.9 ± 1.7 | 6.6 ± 2.1 | 6.2 ± 1.9 | 4.9 ± 1.7 |
| elastic-rigid | 6.3 ± 1.8 | 6.8 ± 1.8 | 6.6 ± 2.2 | 6.4 ± 1.9 | 5.2 ± 1.8 |
| Criterion | p Value | Minimal Rating Score (in Points) | Maximal Rating Score (in Points) |
|---|---|---|---|
| Quality of the registration | 0.206 | 5.6 | 6.5 |
| Ablation zone movement | 0.239 | 6.3 | 6.9 |
| Ablation probe movement | 0.006 | 5.3 | 6.6 |
| Tissue distortion | 0.217 | 5.9 | 6.8 |
| Image artifacts | 0.077 | 4.8 | 5.5 |
| Criterion | k-Value | 95% CI | Koo/Li-Scale |
|---|---|---|---|
| Overall | 0.810 | 0.731–0.871 | good |
| Quality of the registration | 0.772 | 0.574–0.906 | good |
| Ablation zone movement | 0.774 | 0.580–0.907 | good |
| Ablation probe movement | 0.880 | 0.768–0.952 | good |
| Tissue distortion | 0.335 | −0.047–0.691 | poor |
| Image artifacts | 0.524 | 0.194–0.792 | moderate |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kostyrko, B.; Rubarth, K.; Althoff, C.; Zibell, M.; Neizert, C.A.; Poch, F.; Torsello, G.F.; Gebauer, B.; Lehmann, K.; Niehues, S.M.; et al. Evaluation of Different Registration Algorithms to Reduce Motion Artifacts in CT-Thermography (CTT). Diagnostics 2023, 13, 2076. https://doi.org/10.3390/diagnostics13122076
Kostyrko B, Rubarth K, Althoff C, Zibell M, Neizert CA, Poch F, Torsello GF, Gebauer B, Lehmann K, Niehues SM, et al. Evaluation of Different Registration Algorithms to Reduce Motion Artifacts in CT-Thermography (CTT). Diagnostics. 2023; 13(12):2076. https://doi.org/10.3390/diagnostics13122076
Chicago/Turabian StyleKostyrko, Bogdan, Kerstin Rubarth, Christian Althoff, Miriam Zibell, Christina Ann Neizert, Franz Poch, Giovanni Federico Torsello, Bernhard Gebauer, Kai Lehmann, Stefan Markus Niehues, and et al. 2023. "Evaluation of Different Registration Algorithms to Reduce Motion Artifacts in CT-Thermography (CTT)" Diagnostics 13, no. 12: 2076. https://doi.org/10.3390/diagnostics13122076