
Integrative Interpretation of Cardiopulmonary Exercise Tests for Cardiovascular Outcome Prediction: A Machine Learning Approach

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Retrospective Data Retrieval
2.3. Outcome Collection (Incident CV Events)
2.4. Spirometry
2.5. Cardiopulmonary Exercise Testing
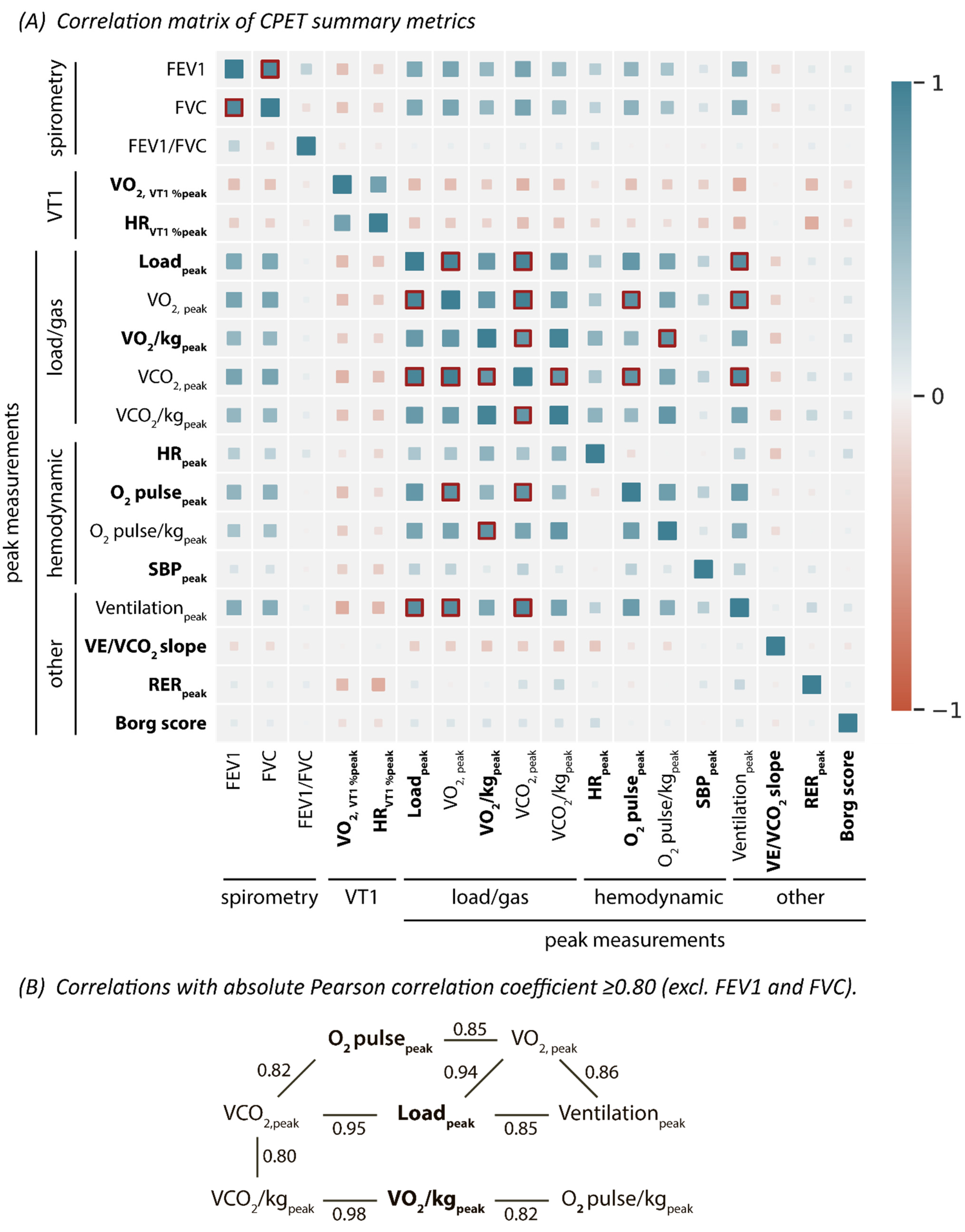
2.6. CPET Summary Metrics
2.7. Statistical Analysis
2.8. Cluster Analysis for CPET-Based Phenogrouping
2.8.1. Feature Selection
2.8.2. Model Fitting
2.9. Model Validation
3. Results
3.1. Population Characteristics
3.2. CPET-Based Phenogroups
3.2.1. Feature Selection and Phenogrouping
3.2.2. Comparing Phenogroup Characteristics
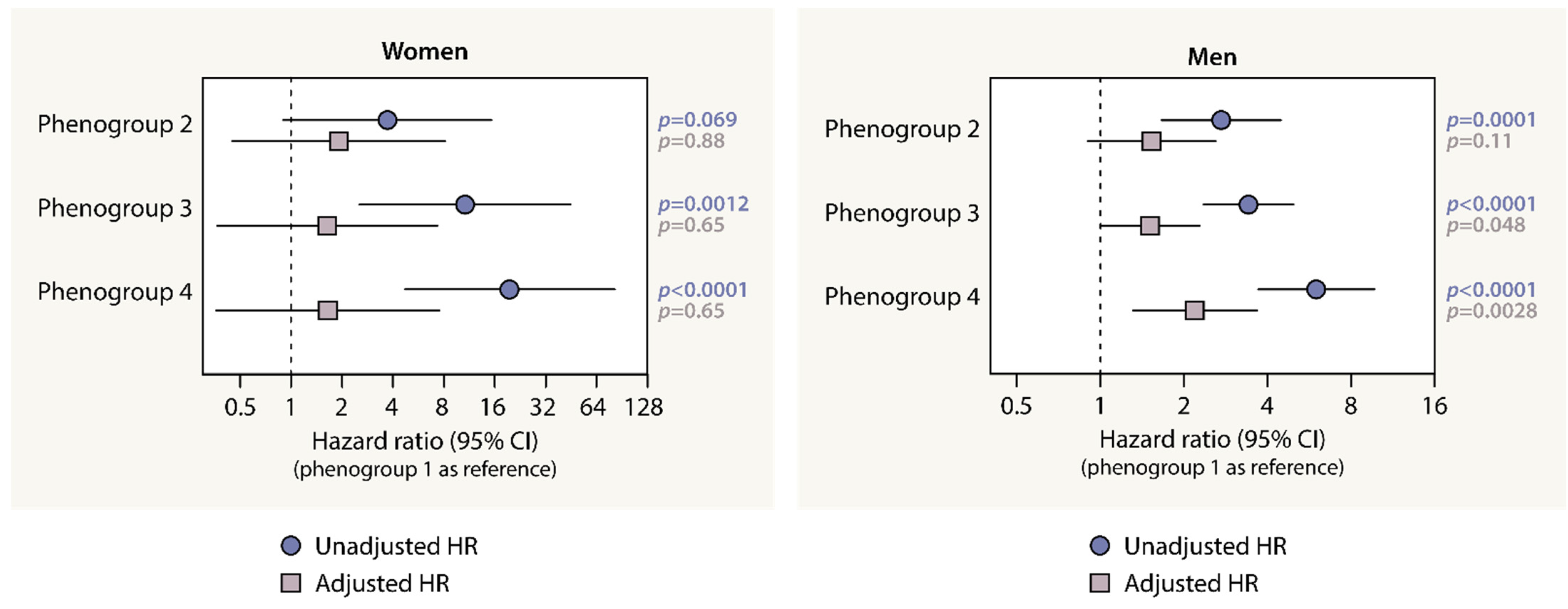
3.2.3. The Association between CV Outcome and Phenogroup Assignment
4. Discussion
4.1. Clinical Implications and Perspectives
4.2. Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Timmis, A.; Vardas, P.; Townsend, N.; Torbica, A.; Katus, H.; De Smedt, D.; Gale, C.P.; Maggioni, A.P.; Petersen, S.E.; Huculeci, R.; et al. European Society of Cardiology: Cardiovascular disease statistics 2021. Eur. Heart J. 2022, 43, 716–799. [Google Scholar] [CrossRef]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E.J.; Colvin, M.M.; Drazner, M.H.; Filippatos, G.S.; Fonarow, G.C.; Givertz, M.M.; et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of Amer. J. Am. Coll. Cardiol. 2017, 70, 776–803. [Google Scholar] [CrossRef] [PubMed]
- Ross, R.; Blair, S.N.; Arena, R.; Church, T.S.; Després, J.-P.; Franklin, B.A.; Haskell, W.L.; Kaminsky, L.A.; Levine, B.D.; Lavie, C.J.; et al. Importance of Assessing Cardiorespiratory Fitness in Clinical Practice: A Case for Fitness as a Clinical Vital Sign: A Scientific Statement From the American Heart Association. Circulation 2016, 134, e653–e699. [Google Scholar] [CrossRef] [PubMed]
- Ezzatvar, Y.; Izquierdo, M.; Núñez, J.; Calatayud, J.; Ramírez-Vélez, R.; García-Hermoso, A. Cardiorespiratory fitness measured with cardiopulmonary exercise testing and mortality in patients with cardiovascular disease: A systematic review and meta-analysis. J. Sport Health Sci. 2021, 10, 609–619. [Google Scholar] [CrossRef] [PubMed]
- Guazzi, M.; Adams, V.; Conraads, V.; Halle, M.; Mezzani, A.; Vanhees, L.; Arena, R.; Fletcher, G.F.; Forman, D.E.; Kitzman, D.W.; et al. EACPR/AHA Joint Scientific Statement. Clinical recommendations for cardiopulmonary exercise testing data assessment in specific patient populations. Eur. Heart J. 2012, 33, 2917–2927. [Google Scholar] [CrossRef] [PubMed]
- Hedman, K.; Lindow, T.; Cauwenberghs, N.; Carlén, A.; Elmberg, V.; Brudin, L.; Ekström, M. Peak exercise SBP and future risk of cardiovascular disease and mortality. J. Hypertens. 2022, 40, 300–309. [Google Scholar] [CrossRef] [PubMed]
- Oldham, W.M.; Oliveira, R.K.F.; Wang, R.-S.; Opotowsky, A.R.; Rubins, D.M.; Hainer, J.; Wertheim, B.M.; Alba, G.A.; Choudhary, G.; Tornyos, A.; et al. Network Analysis to Risk Stratify Patients With Exercise Intolerance. Circ. Res. 2018, 122, 864–876. [Google Scholar] [CrossRef]
- Quanjer, P.H.; Stanojevic, S.; Cole, T.J.; Baur, X.; Hall, G.L.; Culver, B.H.; Enright, P.L.; Hankinson, J.L.; Ip, M.S.M.; Zheng, J.; et al. Multi-ethnic reference values for spirometry for the 3–95-yr age range: The global lung function 2012 equations. Eur. Respir. J. 2012, 40, 1324–1343. [Google Scholar] [CrossRef]
- Guazzi, M.; Arena, R.; Halle, M.; Piepoli, M.F.; Myers, J.; Lavie, C.J. 2016 Focused Update: Clinical Recommendations for Cardiopulmonary Exercise Testing Data Assessment in Specific Patient Populations. Circulation 2016, 133, e694–e711. [Google Scholar] [CrossRef] [Green Version]
- Fletcher, G.F.; Ades, P.A.; Kligfield, P.; Arena, R.; Balady, G.J.; Bittner, V.A.; Coke, L.A.; Fleg, J.L.; Forman, D.E.; Gerber, T.C.; et al. Exercise Standards for Testing and Training. Circulation 2013, 128, 873–934. [Google Scholar] [CrossRef]
- Beaver, W.L.; Wasserman, K.; Whipp, B.J. A new method for detecting anaerobic threshold by gas exchange. J. Appl. Physiol. 1986, 60, 2020–2027. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.; Nichols, S.; Ingle, L. A clinician’s guide to cardiopulmonary exercise testing 1: An introduction. Br. J. Hosp. Med. 2015, 76, 192–195. [Google Scholar] [CrossRef] [PubMed]
- Koch, B.; Schaper, C.; Ittermann, T.; Spielhagen, T.; Dorr, M.; Volzke, H.; Opitz, C.F.; Ewert, R.; Glaser, S. Reference values for cardiopulmonary exercise testing in healthy volunteers: The SHIP study. Eur. Respir. J. 2008, 33, 389–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaumont, M.; Forton, K.; Gillet, A.; Tcheutchoua Nzokou, D.; Lamotte, M. How Does the Method Used to Measure the VE/VCO2 Slope Affect Its Value? A Cross-Sectional and Retrospective Cohort Study. Healthcare 2023, 11, 1292. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Pedregosa, F.; Michel, V.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Vanderplas, J.; Cournapeau, D.; Pedregosa, F.; Varoquaux, G.; et al. Scikit-learn: Machine learning in python. J. Mach. Learn. Res. 2011, 12, 2825–2830. Available online: http://scikit-learn.sourceforge.net (accessed on 9 December 2020).
- Banfield, J.D.; Raftery, A.E. Model-Based Gaussian and Non-Gaussian Clustering. Biometrics 1993, 49, 803. [Google Scholar] [CrossRef]
- Sabovčik, F.; Cauwenberghs, N.; Vens, C.; Kuznetsova, T. Echocardiographic phenogrouping by machine learning for risk stratification in the general population. Eur. Heart J. Digit. Health 2021, 2, 390–400. [Google Scholar] [CrossRef]
- Deng, H.; Han, J. Probabilistic Models for Clustering. In Data Clustering Algorithms and Applications; Aggarwal, C., Reddy, C., Eds.; Taylor & Francis Group, LLC: Boca Raton, FL, USA, 2018; pp. 61–81. ISBN 9781466558229. [Google Scholar]
- Cauwenberghs, N.; Sabovčik, F.; Magnus, A.; Haddad, F.; Kuznetsova, T. Proteomic profiling for detection of early-stage heart failure in the community. ESC Heart Fail. 2021, 8, 2928–2939. [Google Scholar] [CrossRef]
- Marbac, M.; Sedki, M. VarSelLCM: An R/C++ package for variable selection in model-based clustering of mixed-data with missing values. Bioinformatics 2019, 35, 1255–1257. [Google Scholar] [CrossRef]
- Nadruz, W.J.; West, E.; Sengeløv, M.; Santos, M.; Groarke, J.D.; Forman, D.E.; Claggett, B.; Skali, H.; Shah, A.M. Prognostic Value of Cardiopulmonary Exercise Testing in Heart Failure With Reduced, Midrange, and Preserved Ejection Fraction. J. Am. Heart Assoc. 2017, 6, e006000. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.; Jung, J.-H.; Kwon, W.; Ohn, C.; Lee, M.; Kim, D.-W.; Kim, T.-S.; Park, M.-W.; Cho, J.S. The prognostic value of cardiopulmonary exercise testing and HFA-PEFF in patients with unexplained dyspnea and preserved left ventricular ejection fraction. Int. J. Cardiol. 2023, in press. [Google Scholar] [CrossRef]
- Cahalin, L.P.; Chase, P.; Arena, R.; Myers, J.; Bensimhon, D.; Peberdy, M.A.; Ashley, E.; West, E.; Forman, D.E.; Pinkstaff, S.; et al. A meta-analysis of the prognostic significance of cardiopulmonary exercise testing in patients with heart failure. Heart Fail. Rev. 2013, 18, 79–94. [Google Scholar] [CrossRef]
- Cauwenberghs, N.; Haddad, F.; Daubert, M.A.; Chatterjee, R.; Salerno, M.; Mega, J.L.; Heidenreich, P.; Hernandez, A.; Amsallem, M.; Kobayashi, Y.; et al. Clinical and Echocardiographic Diversity Associated With Physical Fitness in the Project Baseline Health Study: Implications for Heart Failure Staging. J. Card. Fail. 2023, in press. [CrossRef]
- Inbar, O.; Inbar, O.; Reuveny, R.; Segel, M.J.; Greenspan, H.; Scheinowitz, M. A Machine Learning Approach to the Interpretation of Cardiopulmonary Exercise Tests: Development and Validation. Pulm. Med. 2021, 2021, 5516248. [Google Scholar] [CrossRef] [PubMed]
- Sakr, S.; Elshawi, R.; Ahmed, A.M.; Qureshi, W.T.; Brawner, C.A.; Keteyian, S.J.; Blaha, M.J.; Al-Mallah, M.H. Comparison of machine learning techniques to predict all-cause mortality using fitness data: The Henry ford exercIse testing (FIT) project. BMC Med. Inform. Decis. Mak. 2017, 17, 174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakr, S.; Elshawi, R.; Ahmed, A.; Qureshi, W.T.; Brawner, C.; Keteyian, S.; Blaha, M.J.; Al-Mallah, M.H. Using machine learning on cardiorespiratory fitness data for predicting hypertension: The Henry Ford ExercIse Testing (FIT) Project. PLoS ONE 2018, 13, e0195344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, T.; Pencina, M.J.; Schulte, P.J.; O’Brien, E.; Whellan, D.J.; Piña, I.L.; Kitzman, D.W.; Lee, K.L.; O’Connor, C.M.; Felker, G.M. Clinical Implications of Chronic Heart Failure Phenotypes Defined by Cluster Analysis. J. Am. Coll. Cardiol. 2014, 64, 1765–1774. [Google Scholar] [CrossRef] [Green Version]
- Ntalianis, E.; Sabovčik, F.; Cauwenberghs, N.; Kouznetsov, D.; Daels, Y.; Claus, P.; Kuznetsova, T. Unsupervised Time-Series Clustering of Left Atrial Strain for Cardiovascular Risk Assessment. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2023, in press. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Men (n = 1188) | Women (n = 1092) | p Value |
|---|---|---|---|
| Age and anthropometrics | |||
| Age, years | 55.9 ± 13.0 | 47.5 ± 13.7 | <0.0001 |
| Weight, kg | 86.0 ± 14.7 | 71.0 ± 14.5 | <0.0001 |
| Height, cm | 176.2 ± 7.1 | 165.2 ± 7.0 | <0.0001 |
| BMI, kg/m2 | 27.7 ± 4.4 | 26.1 ± 5.3 | <0.0001 |
| Medical history | |||
| Hypertension, n (%) | 858 (72.2) | 452 (41.4) | <0.0001 |
| Diabetes mellitus type I or II, n (%) | 166 (14.0) | 57 (5.2) | <0.0001 |
| Chronic kidney disease, n (%) | 59 (5.0) | 24 (2.2) | 0.0006 |
| Obstructive pulmonary disease, n(%) | 45 (3.8) | 44 (4.0) | 0.85 |
| CV disease, n (%) | 732 (61.6) | 205 (18.8) | <0.0001 |
| CV intervention, n (%) | 702 (59.1) | 164 (15.0) | <0.0001 |
| Medication | |||
| Antihypertensive drugs, n (%) | 730 (61.4) | 327 (29.9) | <0.0001 |
| Lipid-lowering drugs, n (%) | 779 (65.6) | 251 (23.0) | <0.0001 |
| Anti-thrombotic drugs, n (%) | 755 (63.6) | 233 (21.3) | <0.0001 |
| Antidiabetic drugs, n (%) | 142 (12.0) | 56 (5.1) | <0.0001 |
| Spirometry * | |||
| FEV1, L | 3.6 ± 0.8 | 2.8 ± 0.6 | <0.0001 |
| FEV1 %predicted | 103.8 ± 16.3 | 103.8 ± 17.6 | 0.97 |
| FVC, L | 4.7 ± 0.9 | 3.6 ± 0.7 | 0.0085 |
| FVC %predicted | 106.9 ± 15.2 | 111.7 ± 17.1 | <0.0001 |
| FEV1/FVC (%) | 77.3 ± 7.6 | 78.3 ± 8.2 | 0.0085 |
| CPET data at rest | |||
| HR, bpm | 71.8 ± 13.6 | 80.2 ± 14.3 | <0.0001 |
| SBP, mmHg | 127.1 ± 19.6 | 118.3 ± 19.0 | <0.0001 |
| DBP, mmHg | 78.2 ± 11.6 | 76.9 ± 11.5 | 0.0061 |
| CPET data at peak | |||
| Load, watt | 191.9 ± 50.2 | 131.3 ± 37.2 | <0.0001 |
| VO2, mL/min | 2143 ± 597 | 1473 ± 380 | <0.0001 |
| VO2 per kg, mL/kg/min | 25.3 ± 7.5 | 21.3 ± 6.0 | <0.0001 |
| VO2 percentage predicted, % | 89.9 ± 19.5 | 88.6 ± 18.3 | 0.083 |
| HR, bpm | 147.9 ± 24.7 | 156.2 ± 23.9 | <0.0001 |
| HR percentage predicted, % | 90.0 ± 12.4 | 90.5 ± 11.2 | 0.36 |
| O2 pulse, mL/beat | 14.5 ± 3.0 | 9.5 ± 2.0 | <0.0001 |
| O2 pulse/kg, mL/beat | 0.17 ± 0.04 | 0.14 ± 0.03 | <0.0001 |
| SBP, mmHg | 181.9 ± 28.6 | 159.1 ± 28.4 | <0.0001 |
| VE, L/min | 82.8 ± 23.1 | 54.0 ± 13.7 | <0.0001 |
| VE/VCO2 slope | 28.6 ± 4.4 | 28.1 ± 4.4 | 0.011 |
| RER | 1.18 ± 0.08 | 1.16 ± 0.08 | <0.0001 |
| Borg score | 15.9 ± 1.6 | 16.0 ± 1.8 | 0.24 |
| Adjusted Models | ||||||||
|---|---|---|---|---|---|---|---|---|
| Unadjusted Model | Clinical Covariables | Clinical Covariables + VO2/kgpeak | Clinical Covariables + % Predicted VO2, peak | |||||
| HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Females | ||||||||
| Phenogroup 2 | 3.72 (0.90–15.3) | 0.069 | 1.92 (0.45–8.17) | 0.88 | 1.79 (0.40–7.94) | 0.77 | 2.55 (0.66–9.78) | 0.17 |
| Phenogroup 3 | 10.7 (2.54–44.9) | 0.0012 | 1.64 (0.46–7.36) | 0.65 | 1.54 (0.33–7.12) | 0.55 | 2.19 (0.55–8.66) | 0.26 |
| Phenogroup 4 | 19.6 (4.71–81.8) | <0.0001 | 1.65 (0.36–7.50) | 0.65 | 1.51 (0.31–7.33) | 0.51 | 2.51 (0.60–10.6) | 0.21 |
| Males | ||||||||
| Phenogroup 2 | 2.72 (1.66–4.46) | 0.0001 | 1.53 (0.90–2.60) | 0.11 | 1.19 (0.69–2.07) | 0.52 | 1.52 (0.85–2.71) | 0.15 |
| Phenogroup 3 | 3.42 (2.36–4.95) | <0.0001 | 1.51 (1.00–2.27) | 0.048 | 1.30 (0.84–2.01) | 0.24 | 1.54 (1.00–2.37) | 0.051 |
| Phenogroup 4 | 5.99 (3.70–9.70) | <0.0001 | 2.19 (1.31–3.66) | 0.0028 | 1.76 (1.00–3.07) | 0.048 | 2.09 (1.20–3.67) | 0.0098 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cauwenberghs, N.; Sente, J.; Van Criekinge, H.; Sabovčik, F.; Ntalianis, E.; Haddad, F.; Claes, J.; Claessen, G.; Budts, W.; Goetschalckx, K.; et al. Integrative Interpretation of Cardiopulmonary Exercise Tests for Cardiovascular Outcome Prediction: A Machine Learning Approach. Diagnostics 2023, 13, 2051. https://doi.org/10.3390/diagnostics13122051
Cauwenberghs N, Sente J, Van Criekinge H, Sabovčik F, Ntalianis E, Haddad F, Claes J, Claessen G, Budts W, Goetschalckx K, et al. Integrative Interpretation of Cardiopulmonary Exercise Tests for Cardiovascular Outcome Prediction: A Machine Learning Approach. Diagnostics. 2023; 13(12):2051. https://doi.org/10.3390/diagnostics13122051
Chicago/Turabian StyleCauwenberghs, Nicholas, Josephine Sente, Hanne Van Criekinge, František Sabovčik, Evangelos Ntalianis, Francois Haddad, Jomme Claes, Guido Claessen, Werner Budts, Kaatje Goetschalckx, and et al. 2023. "Integrative Interpretation of Cardiopulmonary Exercise Tests for Cardiovascular Outcome Prediction: A Machine Learning Approach" Diagnostics 13, no. 12: 2051. https://doi.org/10.3390/diagnostics13122051