
An Anatomical Template for the Normalization of Medical Images of Adult Human Hands
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Hand Imaging
2.3. Template Creation Workflow
| Listing 1. Linux shell command used for running the ANTs template creation script noted in Figure 1. This script, <antsMultivariateTemplateConstruction.sh>, is publicly available at https://github.com/stnava/ANTs/blob/master/Scripts/, accessed on 1 June 2023. Each indented line represents a command line argument. See the script for an explanation of the arguments. The argument <inputHandImages> contains the list of the 27 NIfTI images of the hand from which the hand template was constructed. See text for additional details. |
| antsMultivariateTemplateConstruction2.sh \ |
| -d 3 \ -o ./Template/T_ \ -r 0 \ -n 0 \ -w 1 \ -k 1 \ -q 100 × 70 × 0 × 0 \ -f 6 × 4 × 2 × 1 \ -s 2 × 1 × 0 × 0vox \ -g 0.25 \ -i 4 \ -c 2 \ -j 8 \ -m CC [4] \ -t BSplineSyN \ -y 0 \ $inputHandImages |
3. Results
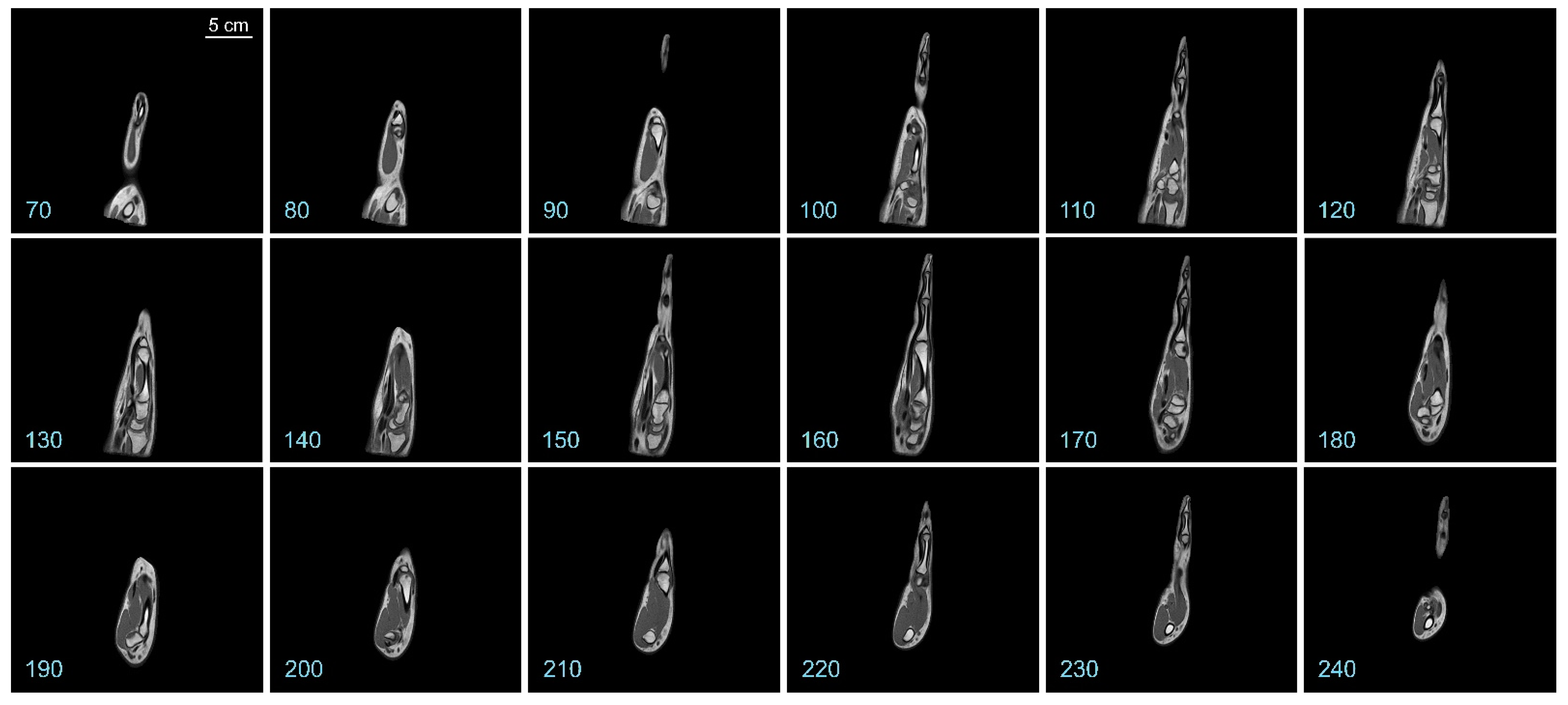
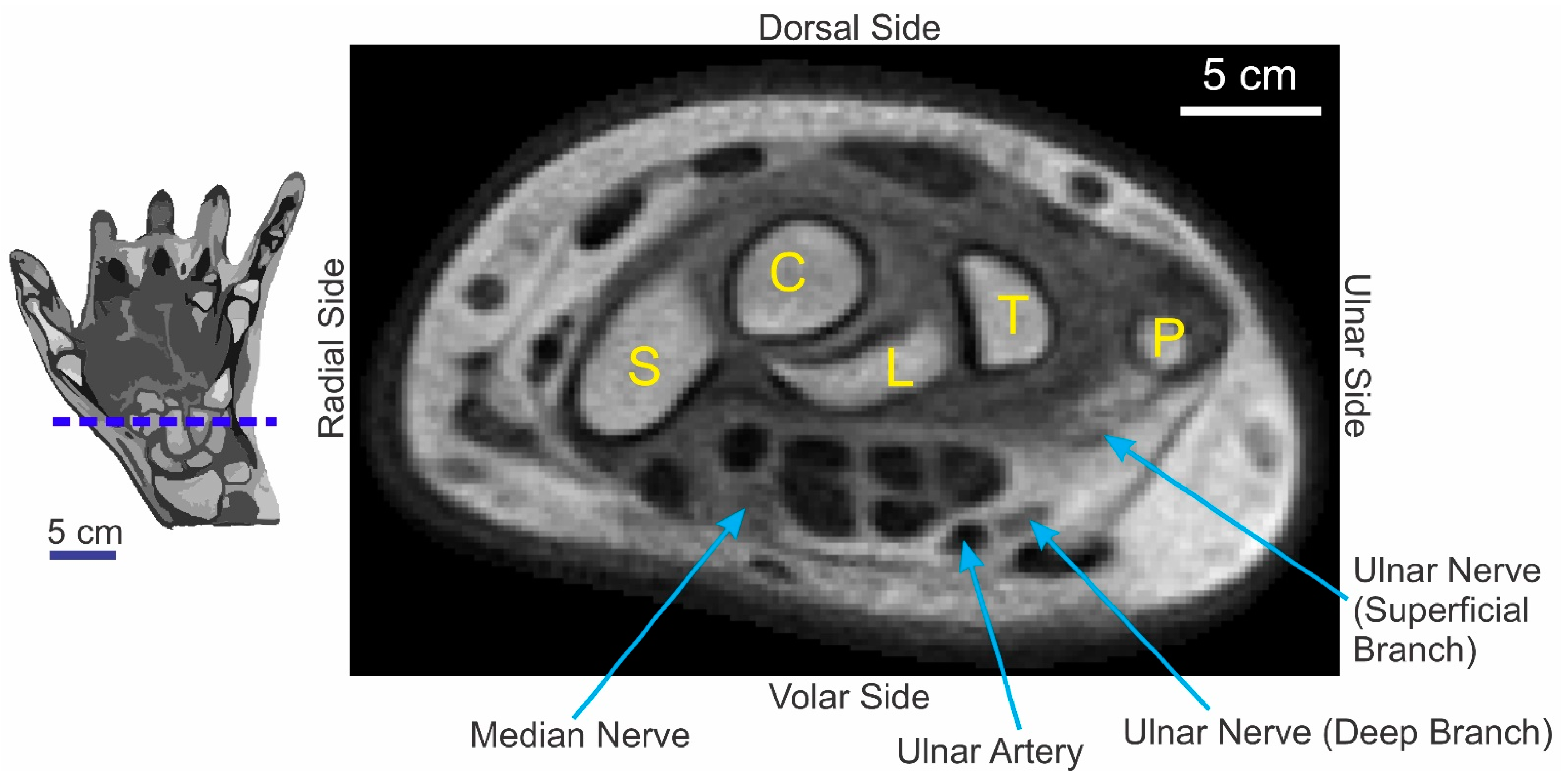
3.1. Overview of the Hand Template
3.2. Physical Quality of the Template Image
4. Discussion
4.1. The Potential Utility and Impact of a Hand Template
4.2. Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Evans, A.C.; Janke, A.L.; Collins, D.L.; Baillet, S. Brain templates and atlases. Neuroimage 2012, 62, 911–922. [Google Scholar] [CrossRef] [PubMed]
- Tustison, N.J.; Cook, P.A.; Holbrook, A.J.; Johnson, H.J.; Muschelli, J.; Devenyi, G.A.; Duda, J.T.; Das, S.R.; Cullen, N.C.; Gillen, D.L.; et al. The ANTsX ecosystem for quantitative biological and medical imaging. Sci. Rep. 2021, 11, 9068. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.H. Frontiers of Medical Imaging; World Scientific: Hackensack, NJ, USA, 2015. [Google Scholar]
- Kolekar, M.H.; Kumar, V. Biomedical Signal and Image Processing in Patient Care; IGI Global: Hershey, PA, USA, 2018. [Google Scholar]
- Modat, M.; Ourselin, S. Image Processing, Computer Vision, Pattern Recognition, and Graphics 8545. In Biomedical Image Registration: 6th International Workshop, WBIR 2014, London, UK, 7–8 July 2014; Springer International Publishing: Cham, Switterland, 2014. [Google Scholar] [CrossRef]
- Schaefer, G.; Hassanien, A.E.; Jiang, J. Computational Intelligence in Medical Imaging: Techniques and Applications; Chapman & Hall/CRC: Boca Raton, FL, USA, 2009. [Google Scholar]
- Jones, L.A.; Lederman, S.J. Human Hand Function; Oxford University Press: Oxford, UK; New York, NY, USA, 2006. [Google Scholar]
- Wilgis, E.F.S. The Wonder of the Human Hand: Care and Repair of the Body’s Most Marvelous Instrument; Johns Hopkins University Press: Baltimore, MD, USA, 2014. [Google Scholar]
- Mountcastle, V.B. The Sensory Hand: Neural Mechanisms of Somatic Sensation; Harvard University Press: Cambridge, UK, 2005. [Google Scholar]
- Mountcastle, V.B. Medical Physiology, 14th ed.; C. V. Mosby Co.: St. Louis, MO, USA, 1980. [Google Scholar]
- Calvert, G.; Spence, C.; Stein, B.E. The Handbook of Multisensory Processes; MIT Press: Cambridge, UK, 2004. [Google Scholar]
- Bow, J. Life with Juvenile Idiopathic Arthritis; Childs World: Mankato, MN, USA, 2018. [Google Scholar]
- Peterson, M.D.L.S.; Cavallo, A.L. Mayo Clinic Guide to Arthritis: Managing Joint Pain for an Active Life, 1st. ed.; Mayo Clinic Press: Rochester, MN, USA, 2020. [Google Scholar]
- Robinson, L.S.; Brown, T.; O’Brien, L. Capturing the costs of acute hand and wrist injuries: Lessons learnt from a prospective longitudinal burden of injury study. Hand Ther. 2020, 25, 119–129. [Google Scholar] [CrossRef]
- de Putter, C.E.; Selles, R.W.; Polinder, S.; Panneman, M.J.; Hovius, S.E.; van Beeck, E.F. Economic impact of hand and wrist injuries: Health-care costs and productivity costs in a population-based study. J. Bone Joint Surg. Am. 2012, 94, e56. [Google Scholar] [CrossRef] [PubMed]
- Rosberg, H.E.; Carlsson, K.S.; Cederlund, R.I.; Ramel, E.; Dahlin, L.B. Costs and outcome for serious hand and arm injuries during the first year after trauma—A prospective study. BMC Public Health 2013, 13, 501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, L.S.; Sarkies, M.; Brown, T.; O’Brien, L. Direct, indirect and intangible costs of acute hand and wrist injuries: A systematic review. Injury 2016, 47, 2614–2626. [Google Scholar] [CrossRef] [PubMed]
- Michas, F. Most Common Radiology Procedures in the U.S. for 2018, by Total Charges, 2020th ed.; Statista Inc.: New York, NY, USA, 2020. [Google Scholar]
- Strobel, S.; Spitz, L.; Marks, S.D. Hospital for Sick Children (London England). In Great Ormond Street Handbook of Paediatrics, 2nd ed.; CRC Press Taylor & Francis Group: Boca Raton, FL, USA, 2016. [Google Scholar]
- Shattuck, D.W.; Mirza, M.; Adisetiyo, V.; Hojatkashani, C.; Salamon, G.; Narr, K.L.; Poldrack, R.A.; Bilder, R.M.; Toga, A.W. Construction of a 3D probabilistic atlas of human cortical structures. Neuroimage 2008, 39, 1064–1080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhalerao, G.V.; Parlikar, R.; Agrawal, R.; Shivakumar, V.; Kalmady, S.V.; Rao, N.P.; Agarwal, S.M.; Narayanaswamy, J.C.; Reddy, Y.C.J.; Venkatasubramanian, G. Construction of population-specific Indian MRI brain template: Morphometric comparison with Chinese and Caucasian templates. Asian J. Psychiatr. 2018, 35, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Avants, B.B.; Duda, J.T.; Kilroy, E.; Krasileva, K.; Jann, K.; Kandel, B.T.; Tustison, N.J.; Yan, L.; Jog, M.; Smith, R.; et al. The pediatric template of brain perfusion. Sci. Data 2015, 2, 150003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seidlitz, J.; Sponheim, C.; Glen, D.; Ye, F.Q.; Saleem, K.S.; Leopold, D.A.; Ungerleider, L.; Messinger, A. A population MRI brain template and analysis tools for the macaque. Neuroimage 2018, 170, 121–131. [Google Scholar] [CrossRef] [PubMed]
- Avants, B.B.; Yushkevich, P.; Pluta, J.; Minkoff, D.; Korczykowski, M.; Detre, J.; Gee, J.C. The optimal template effect in hippocampus studies of diseased populations. Neuroimage 2010, 49, 2457–2466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bart, E.; Hegdé, J. (Eds.) Deep Learning in Biological, Computer, and Neuromorphic Systems; Frontiers Media SA: Lausanne, Switzerland, 2019. [Google Scholar]
- Tustison, N.J.; Avants, B.B. Explicit B-spline regularization in diffeomorphic image registration. Front. Neuroinform. 2013, 7, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maga, A.M.; Tustison, N.J.; Avants, B.B. A population level atlas of Mus musculus craniofacial skeleton and automated image-based shape analysis. J. Anat. 2017, 231, 433–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, S.J.; Santamaria, A.J.; Sanchez, F.J.; Villamil, L.M.; Pinheiro Saraiva, P.; Rodriguez, J.; Nunez-Gomez, Y.; Opris, I.; Solano, J.P.; Guest, J.D.; et al. In vivo Population Averaged Stereotaxic T2w MRI Brain Template for the Adult Yucatan Micropig. Front. Neuroanat. 2020, 14, 599701. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Wei, Y.; Wong, K.K.L. A Generative Adversarial Network technique for high-quality super-resolution reconstruction of cardiac magnetic resonance images. Magn. Reson. Imaging 2022, 85, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Miao, J.; Huang, F.; Narayan, S.; Wilson, D.L. A new perceptual difference model for diagnostically relevant quantitative image quality evaluation: A preliminary study. Magn. Reson. Imaging 2013, 31, 596–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miao, J.; Huo, D.; Wilson, D.L. Quantitative image quality evaluation of MR images using perceptual difference models. Med. Phys. 2008, 35, 2541–2553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tian, C.; Fei, L.; Zheng, W.; Xu, Y.; Zuo, W.; Lin, C.W. Deep learning on image denoising: An overview. Neural Netw. 2020, 131, 251–275. [Google Scholar] [CrossRef] [PubMed]
- Toennies, K.D. Guide to Medical Image Analysis: Methods and Algorithms. In Advances in Computer Vision and Pattern Recognition, 2nd ed.; Springer: London, UK, 2017. [Google Scholar] [CrossRef]
- Panigrahi, L.; Biswal, S.; Bhoi, A.K.; Kalam, A.; Barsocchi, P. Machine Learning and AI Techniques in Interactive Medical Image Analysis; Engineering Science Reference: Hershey, PA, USA, 2023. [Google Scholar]
- Marques, P.M.d.A.; Mencattini, A.; Salmeri, M.; Rangayyan, R.M. Medical Image Analysis and Informatics: Computer-Aided Diagnosis and Therapy; Taylor & Francis: Boca Raton, FL, USA, 2017. [Google Scholar]
- Talairach, J.; Tournoux, P. Coplanar Stereotaxic Atlas of the Human Brain; Thieme: Stuttgart, Germany, 1988. [Google Scholar]
- Zilles, K.; Amunts, K. Centenary of Brodmann’s map—Conception and fate. Nat. Rev. Neurosci. 2010, 11, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.F.; Bowden, D.M.; Martin, R.F. Primate Brain Maps: Structure of the Macaque Brain. Available online: http://www.loc.gov/catdir/enhancements/fy0611/00709186-d.html (accessed on 1 June 2023).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | |
|---|---|
| Mean | 35.9 years ± 17.9 (standard deviation) |
| Range | 19.4–66.9 years |
| Demographic Distribution | |
| African American | 2 |
| Asian American | 3 |
| Caucasian | 14 |
| Latino | 2 |
| Subject Gender | Left Hand Only | Right Hand Only | Both Hands |
|---|---|---|---|
| Male | 3 | 3 | 2 |
| Female | 5 | 4 | 4 |
| Total | 8 | 7 | 12 |
| Grand Total | 27 images | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hegdé, J.; Tustison, N.J.; Parker, W.T.; Branch, F.; Yanasak, N.; Stumpo, L.A. An Anatomical Template for the Normalization of Medical Images of Adult Human Hands. Diagnostics 2023, 13, 2010. https://doi.org/10.3390/diagnostics13122010
Hegdé J, Tustison NJ, Parker WT, Branch F, Yanasak N, Stumpo LA. An Anatomical Template for the Normalization of Medical Images of Adult Human Hands. Diagnostics. 2023; 13(12):2010. https://doi.org/10.3390/diagnostics13122010
Chicago/Turabian StyleHegdé, Jay, Nicholas J. Tustison, William T. Parker, Fallon Branch, Nathan Yanasak, and Lorie A. Stumpo. 2023. "An Anatomical Template for the Normalization of Medical Images of Adult Human Hands" Diagnostics 13, no. 12: 2010. https://doi.org/10.3390/diagnostics13122010