
Evaluation of NAG, NGAL, and KIM-1 as Prognostic Markers of the Initial Evolution of Kidney Transplantation
 and
and
Abstract
:1. Introduction
2. Materials and Methods
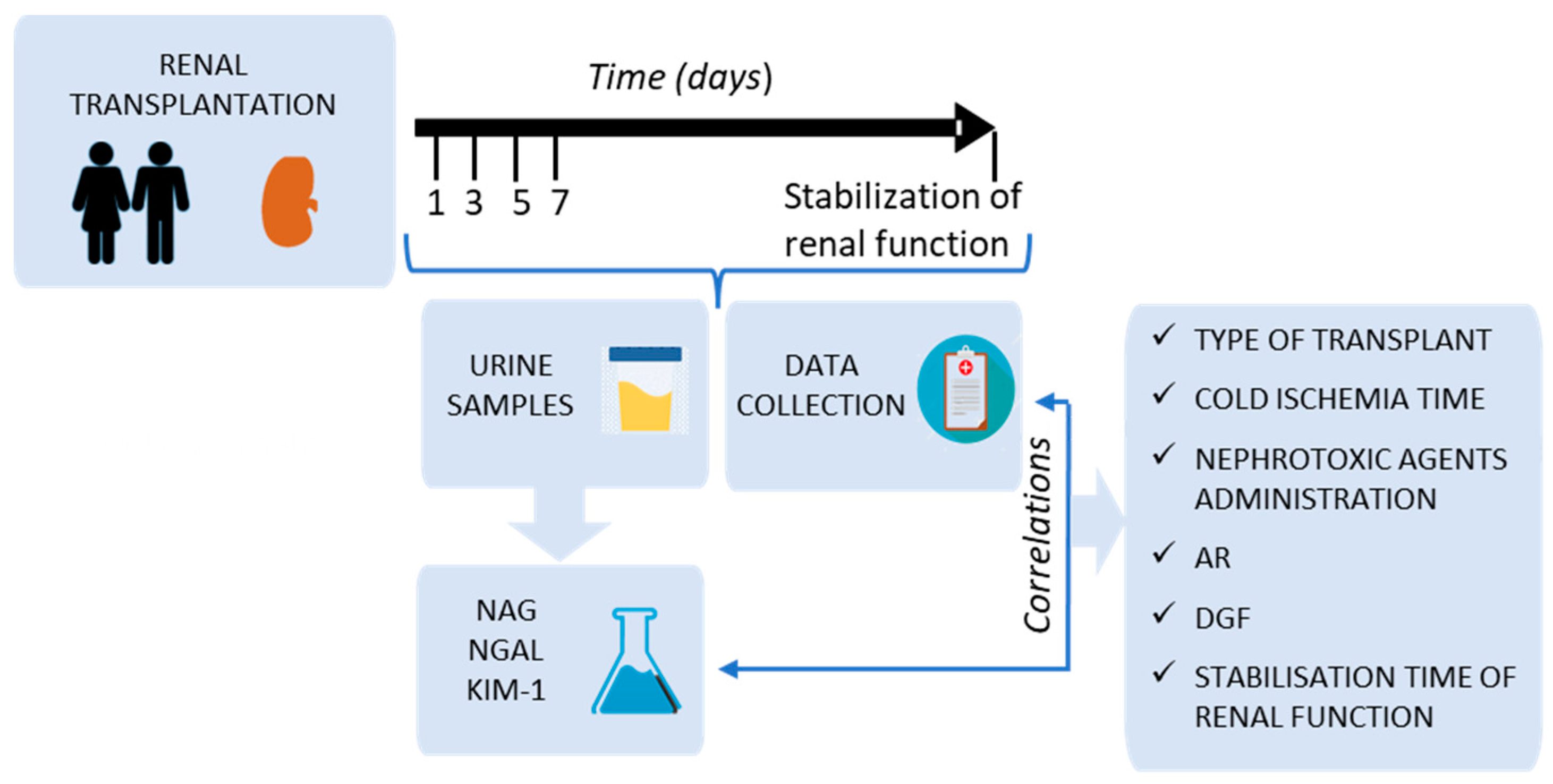
2.1. Study Design
2.2. Study Variables
2.3. Patient Data Collection
2.4. Collection and Processing of Urine Samples
2.5. Analysis of Urine Samples
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics and Type of Transplant
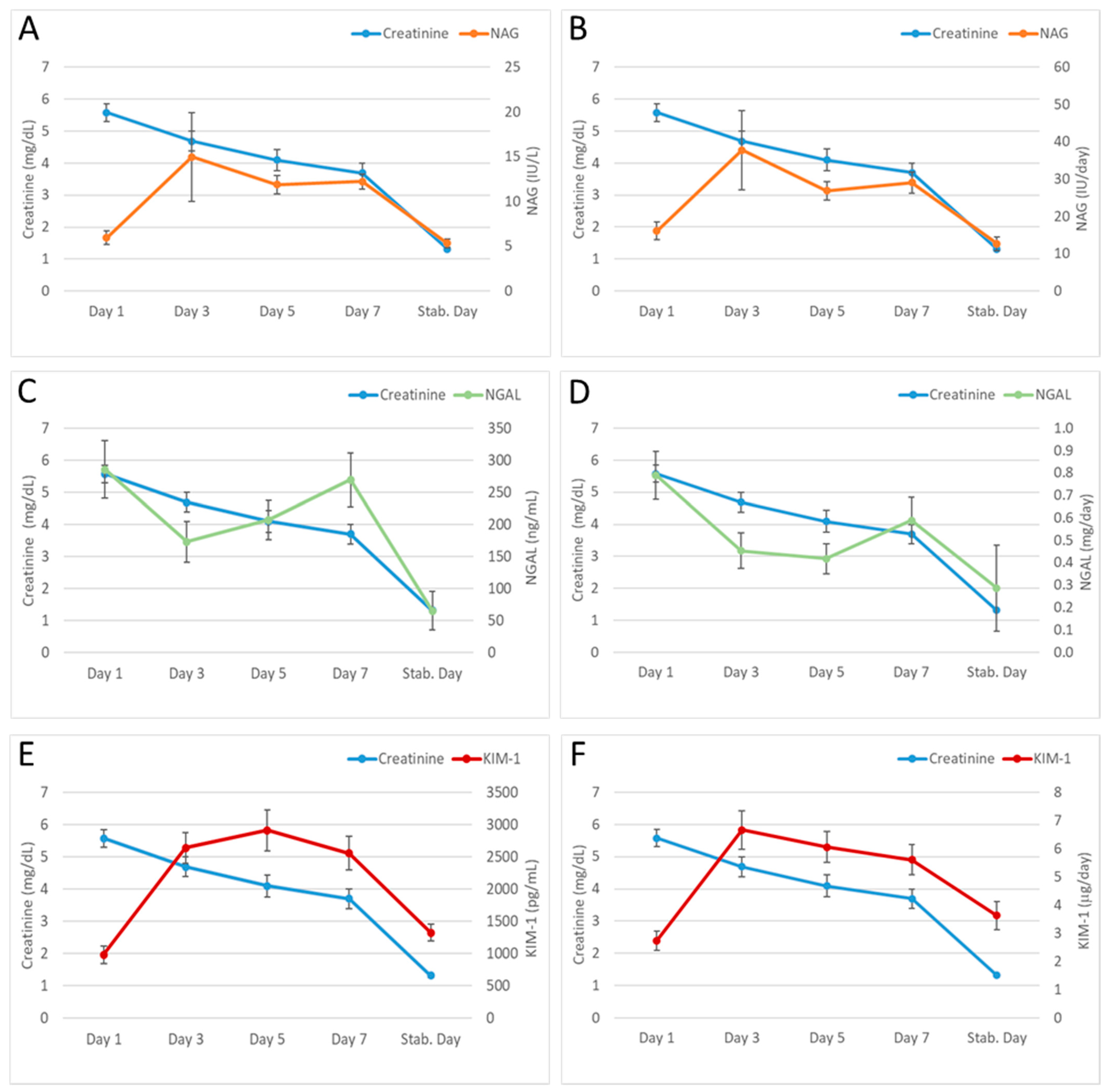
3.2. Evolution of the Urinary Biomarkers (NAG, NGAL and KIM-1) and Serum Creatinine after Transplantation
3.3. Relationship between Urinary Biomarkers (NAG, NGAL, and KIM-1) and the Main Events in the Immediate Post-Transplantation
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lamb, E.J. United Kingdom Guidelines for Chronic Kidney Disease. Scand. J. Clin. Lab. Investig. Suppl. 2008, 241, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Barry, J.M. Renal Transplantation in 2016. Indian J. Urol. 2016, 32, 175–177. [Google Scholar] [CrossRef] [PubMed]
- Myers, B.D. Cyclosporine Nephrotoxicity. Kidney Int. 1986, 30, 964–974. [Google Scholar] [CrossRef] [PubMed]
- Marcen, R.; Navarro, J.F.; Mampaso, F.; Orofino, L.; Gonzalo, A.; Teruel, J.L.; Ortuño, J. Recurrence of Focal-Segmental Glomerulosclerosis in Kidney Transplant Patients on Ciclosporin. Nephron 1994, 68, 497–499. [Google Scholar] [CrossRef]
- Morales, J.M.; Andres, A.; Rengel, M.; Rodicio, J.L. Influence of Cyclosporin, Tacrolimus and Rapamycin on Renal Function and Arterial Hypertension after Renal Transplantation. Nephrol. Dial. Transplant. 2001, 16 (Suppl. S1), 121–124. [Google Scholar] [CrossRef]
- Wu, Q.; Wang, X.; Nepovimova, E.; Wang, Y.; Yang, H.; Kuca, K. Mechanism of Cyclosporine A Nephrotoxicity: Oxidative Stress, Autophagy, and Signalings. Food Chem. Toxicol. 2018, 118, 889–907. [Google Scholar] [CrossRef]
- Danovitch, G.M. Handbook of Kidney Transplantation; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2009; ISBN 978-0-7817-9374-2. [Google Scholar]
- Abu Jawdeh, B.G.; Govil, A. Acute Kidney Injury in Transplant Setting: Differential Diagnosis and Impact on Health and Health Care. Adv. Chronic. Kidney Dis. 2017, 24, 228–232. [Google Scholar] [CrossRef]
- Yarlagadda, S.G.; Coca, S.G.; Formica, R.N.; Poggio, E.D.; Parikh, C.R. Association between Delayed Graft Function and Allograft and Patient Survival: A Systematic Review and Meta-Analysis. Nephrol. Dial. Transplant. 2009, 24, 1039–1047. [Google Scholar] [CrossRef]
- Siedlecki, A.; Irish, W.; Brennan, D.C. Delayed Graft Function in the Kidney Transplant. Am. J. Transplant. 2011, 11, 2279–2296. [Google Scholar] [CrossRef]
- Lechevallier, E.; Dussol, B.; Luccioni, A.; Thirion, X.; Vacher-Copomat, H.; Jaber, K.; Brunet, P.; Leonetti, F.; Lavelle, O.; Coulange, C.; et al. Posttransplantation Acute Tubular Necrosis: Risk Factors and Implications for Graft Survival. Am. J. Kidney Dis. 1998, 32, 984–991. [Google Scholar] [CrossRef]
- Lederer, S.R.; Kluth-Pepper, B.; Schneeberger, H.; Albert, E.; Land, W.; Feucht, H.E. Impact of Humoral Alloreactivity Early after Transplantation on the Long-Term Survival of Renal Allografts. Kidney Int. 2001, 59, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Alachkar, N.; Rabb, H.; Jaar, B.G. Urinary Biomarkers in Acute Kidney Transplant Dysfunction. Nephron. Clin. Pract. 2011, 118, c173–c181. [Google Scholar] [CrossRef] [PubMed]
- Vaidya, V.S.; Ferguson, M.A.; Bonventre, J.V. Biomarkers of Acute Kidney Injury. Annu. Rev. Pharmacol. Toxicol. 2008, 48, 463–493. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.R.; Parikh, C.R. Biomarkers of Acute and Chronic Kidney Disease. Annu. Rev. Physiol. 2019, 81, 309–333. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, A.; Sarwal, M. Protein Biomarkers in Renal Transplantation. Expert. Rev. Proteom. 2018, 15, 41–54. [Google Scholar] [CrossRef] [PubMed]
- Emerging Biomarkers of Delayed Graft Function in Kidney Transplantation | Elsevier Enhanced Reader. Available online: https://reader.elsevier.com/reader/sd/pii/S0955470X21000355?token=4247F627F64429EF1D95A07BA01D402FCCA312443C33F32E82F0FDF3C6AECF1A42851EDD0287AA078741807F0EF960C8&originRegion=eu-west-1&originCreation=20230215174737 (accessed on 15 February 2023).
- Yatim, K.M.; Azzi, J.R. Novel Biomarkers in Kidney Transplantation. Semin. Nephrol. 2022, 42, 2–13. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Hansrivijit, P.; Kovvuru, K.; Kanduri, S.R.; Torres-Ortiz, A.; Acharya, P.; Gonzalez-Suarez, M.L.; Kaewput, W.; Bathini, T.; Cheungpasitporn, W. Diagnostics, Risk Factors, Treatment and Outcomes of Acute Kidney Injury in a New Paradigm. J. Clin. Med. 2020, 9, 1104. [Google Scholar] [CrossRef]
- Edelstein, C.L. Chapter Six—Biomarkers in Acute Kidney Injury. In Biomarkers of Kidney Disease, 2nd ed.; Edelstein, C.L., Ed.; Academic Press: Cambridge, MA, USA, 2017; pp. 241–315. ISBN 978-0-12-803014-1. [Google Scholar]
- Griffin, B.R.; Faubel, S.; Edelstein, C.L. Biomarkers of Drug-Induced Kidney Toxicity. Ther. Drug Monit. 2019, 41, 213–226. [Google Scholar] [CrossRef]
- Rysz, J.; Franczyk, B.; Ciałkowska-Rysz, A.; Gluba-Brzózka, A. The Effect of Diet on the Survival of Patients with Chronic Kidney Disease. Nutrients 2017, 9, 495. [Google Scholar] [CrossRef]
- Albert, C.; Zapf, A.; Haase, M.; Röver, C.; Pickering, J.W.; Albert, A.; Bellomo, R.; Breidthardt, T.; Camou, F.; Chen, Z.; et al. Neutrophil Gelatinase-Associated Lipocalin Measured on Clinical Laboratory Platforms for the Prediction of Acute Kidney Injury and the Associated Need for Dialysis Therapy: A Systematic Review and Meta-Analysis. Am. J. Kidney Dis. 2020, 76, 826–841. [Google Scholar] [CrossRef]
- Ichimura, T.; Hung, C.C.; Yang, S.A.; Stevens, J.L.; Bonventre, J.V. Kidney Injury Molecule-1: A Tissue and Urinary Biomarker for Nephrotoxicant-Induced Renal Injury. Am. J. Physiol. Renal. Physiol. 2004, 286, F552–F563. [Google Scholar] [CrossRef]
- Ichimura, T.; Brooks, C.R.; Bonventre, J.V. Kim-1/Tim-1 and Immune Cells: Shifting Sands. Kidney Int. 2012, 81, 809–811. [Google Scholar] [CrossRef]
- Gardiner, L.; Akintola, A.; Chen, G.; Catania, J.M.; Vaidya, V.; Burghardt, R.C.; Bonventre, J.V.; Trzeciakowski, J.; Parrish, A.R. Structural Equation Modeling Highlights the Potential of Kim-1 as a Biomarker for Chronic Kidney Disease. Am. J. Nephrol. 2012, 35, 152–163. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191. [CrossRef] [PubMed]
- Bonventre, J.V. Diagnosis of Acute Kidney Injury: From Classic Parameters to New Biomarkers. Contrib. Nephrol. 2007, 156, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Waikar, S.S.; Bonventre, J.V. Biomarkers for the Diagnosis of Acute Kidney Injury. Curr. Opin. Nephrol. Hypertens. 2007, 16, 557–564. [Google Scholar] [CrossRef]
- Coca, S.G.; Yalavarthy, R.; Concato, J.; Parikh, C.R. Biomarkers for the Diagnosis and Risk Stratification of Acute Kidney Injury: A Systematic Review. Kidney Int. 2008, 73, 1008–1016. [Google Scholar] [CrossRef] [PubMed]
- Nickolas, T.L.; O’Rourke, M.J.; Yang, J.; Sise, M.E.; Canetta, P.A.; Barasch, N.; Buchen, C.; Khan, F.; Mori, K.; Giglio, J.; et al. Sensitivity and Specificity of a Single Emergency Department Measurement of Urinary Neutrophil Gelatinase-Associated Lipocalin for Diagnosing Acute Kidney Injury. Ann. Intern. Med. 2008, 148, 810–819. [Google Scholar] [CrossRef]
- Singer, E.; Elger, A.; Elitok, S.; Kettritz, R.; Nickolas, T.L.; Barasch, J.; Luft, F.C.; Schmidt-Ott, K.M. Urinary Neutrophil Gelatinase-Associated Lipocalin Distinguishes Pre-Renal from Intrinsic Renal Failure and Predicts Outcomes. Kidney Int. 2011, 80, 405–414. [Google Scholar] [CrossRef]
- Srisawat, N.; Wen, X.; Lee, M.; Kong, L.; Elder, M.; Carter, M.; Unruh, M.; Finkel, K.; Vijayan, A.; Ramkumar, M.; et al. Urinary Biomarkers and Renal Recovery in Critically Ill Patients with Renal Support. Clin. J. Am. Soc. Nephrol. 2011, 6, 1815–1823. [Google Scholar] [CrossRef]
- Páginas—Registro Español de Enfermos Renales. Available online: http://www.ont.es/infesp/Paginas/RegistroEnfermosRenales.aspx (accessed on 31 August 2021).
- Alcázar Arroyo, R.; Orte, L.; González Parra, E.; Górriz, J.L.; Navarro, J.F.; Martín de Francisco, A.L.; Egocheaga, M.I.; Álvarez Guisasola, F. Documento de consenso SEN-semFYC sobre la enfermedad renal crónica. Nefrología 2008, 28, 273–282. [Google Scholar]
- Pascual, M.; Theruvath, T.; Kawai, T.; Tolkoff-Rubin, N.; Cosimi, A.B. Strategies to Improve Long-Term Outcomes after Renal Transplantation. N. Engl. J. Med. 2002, 346, 580–590. [Google Scholar] [CrossRef] [PubMed]
- van Timmeren, M.M.; Vaidya, V.S.; van Ree, R.M.; Oterdoom, L.H.; de Vries, A.P.J.; Gans, R.O.B.; van Goor, H.; Stegeman, C.A.; Bonventre, J.V.; Bakker, S.J.L. High Urinary Excretion of Kidney Injury Molecule-1 Is an Independent Predictor of Graft Loss in Renal Transplant Recipients. Transplantation 2007, 84, 1625–1630. [Google Scholar] [CrossRef] [PubMed]
- Emeigh Hart, S.G. Assessment of Renal Injury in Vivo. J. Pharmacol. Toxicol. Methods 2005, 52, 30–45. [Google Scholar] [CrossRef]
- Mishra, J.; Mori, K.; Ma, Q.; Kelly, C.; Barasch, J.; Devarajan, P. Neutrophil Gelatinase-Associated Lipocalin: A Novel Early Urinary Biomarker for Cisplatin Nephrotoxicity. Am. J. Nephrol. 2004, 24, 307–315. [Google Scholar] [CrossRef]
- Wang, Y.; Jia, Y.; Wang, C.; Gao, X.; Liu, Y.; Yue, B. Urinary Neutrophil Gelatinase-associated Lipocalin Rapidly Decreases in the First Week after Kidney Transplantation. J. Clin. Lab. Anal. 2020, 34, e23445. [Google Scholar] [CrossRef]
- Li, F.; Hu, L.; Zhao, X.; Ge, W.; Pan, H.; Zhang, W.; Jiang, Y.; Xu, X.; Hou, J.; Pu, J. The Value of Cystatin C and Urinary and Serum Neutrophil Gelatinase-Associated Lipocalin during the Perioperative Period of Renal Transplantation. Transl. Androl. Urol. 2019, 8, 432–441. [Google Scholar] [CrossRef]
- Bonventre, J.V. Kidney Injury Molecule-1 (KIM-1): A Urinary Biomarker and Much More. Nephrol. Dial. Transplant. 2009, 24, 3265–3268. [Google Scholar] [CrossRef]
- Salamzadeh, J.; Sahraee, Z.; Nafar, M.; Parvin, M. Delayed Graft Function (DGF) after Living Donor Kidney Transplantation: A Study of Possible Explanatory Factors. Ann. Transplant. 2012, 17, 69–76. [Google Scholar] [CrossRef]
- Loertscher, R.; Scholer, A.; Brunner, F.; Harder, F.; Thiel, G. Clinical relevance of N-acetylglucosaminidase determination in urine of kidney transplant recipients with and without cyclosporin A. Schweiz. Med. Wochenschr. 1982, 112, 1658–1664. [Google Scholar]
- Kotanko, P.; Margreiter, R.; Pfaller, W. Reduced Renal Allograft Survival Is Related to Low Urinary N-Acetyl-Beta-D-Glucosaminidase Excretion during the First Posttransplant Month. Transplantation 1996, 61, 388–392. [Google Scholar] [CrossRef] [PubMed]
- Kwiatkowska, E.; Domański, L.; Bober, J.; Kłoda, K.; Safranow, K.; Szymańska-Pasternak, J.; Romanowski, M.; Sulecka, A.; Pawlik, A.; Ciechanowski, K. N-Acetyl-Beta-Glucosaminidase Urine Activity as a Marker of Early Proximal Tubule Damage and a Predictor of the Long-Term Function of the Transplanted Kidneys. Acta Biochim. Pol. 2014, 61, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Ramirez-Sandoval, J.C.; Herrington, W.; Morales-Buenrostro, L.E. Neutrophil Gelatinase-Associated Lipocalin in Kidney Transplantation: A Review. Transplant. Rev. 2015, 29, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Li, M.; Chouhan, K.K.; Simon, E.E.; Hamm, L.L.; Batuman, V. Urine Free Light Chains as a Novel Biomarker of Acute Kidney Allograft Injury. Clin. Transplant. 2013, 27, 953–960. [Google Scholar] [CrossRef]
- Field, M.; Lowe, D.; Cobbold, M.; Higgins, R.; Briggs, D.; Inston, N.; Ready, A.R. The Use of NGAL and IP-10 in the Prediction of Early Acute Rejection in Highly Sensitized Patients Following HLA-Incompatible Renal Transplantation. Transpl. Int. 2014, 27, 362–370. [Google Scholar] [CrossRef]
- Haase-Fielitz, A.; Haase, M.; Devarajan, P. Neutrophil Gelatinase-Associated Lipocalin as a Biomarker of Acute Kidney Injury: A Critical Evaluation of Current Status. Ann. Clin. Biochem. 2014, 51, 335–351. [Google Scholar] [CrossRef]
- Li, Y.M.; Li, Y.; Yan, L.; Wang, H.; Wu, X.J.; Tang, J.T.; Wang, L.L.; Shi, Y.Y. Comparison of Urine and Blood NGAL for Early Prediction of Delayed Graft Function in Adult Kidney Transplant Recipients: A Meta-Analysis of Observational Studies. BMC Nephrol. 2019, 20, 291. [Google Scholar] [CrossRef]
- Pajek, J.; Škoberne, A.; Šosterič, K.; Adlešič, B.; Leskošek, B.; Bučar Pajek, M.; Osredkar, J.; Lindič, J. Non-Inferiority of Creatinine Excretion Rate to Urinary L-FABP and NGAL as Predictors of Early Renal Allograft Function. BMC Nephrol. 2014, 15, 117. [Google Scholar] [CrossRef]
- van den Akker, E.K.; Hesselink, D.A.; Manintveld, O.C.; IJzermans, J.N.M.; de Bruijn, R.W.F.; Dor, F.J.M.F. Neutrophil Gelatinase-Associated Lipocalin, but Not Kidney Injury Marker 1, Correlates with Duration of Delayed Graft Function. Eur. Surg. Res. 2015, 55, 319–327. [Google Scholar] [CrossRef]
- Michon, A.; Durrbach, A.; Gautier, J.-C.; Benain, X.; Lunven, C.; Jagerschmidt, A.; Aubert, C.; Poetz, O.; Joos, T.; Gury, T.; et al. Investigation of New Biomarkers of Kidney Injury in Renal Transplant Recipients Undergoing Graft Biopsy. Clin. Transplant. 2021, 35, 14408. [Google Scholar] [CrossRef]
- Lima, C.; de Paiva Haddad, L.B.; de Melo, P.D.V.; Malbouisson, L.M.; do Carmo, L.P.F.; D’Albuquerque, L.A.C.; Macedo, E. Early Detection of Acute Kidney Injury in the Perioperative Period of Liver Transplant with Neutrophil Gelatinase-Associated Lipocalin. BMC Nephrol. 2019, 20, 367. [Google Scholar] [CrossRef] [PubMed]
- Feldkamp, T.; Bienholz, A.; Kribben, A. Urinary Neutrophil Gelatinase-Associated Lipocalin (NGAL) for the Detection of Acute Kidney Injury after Orthotopic Liver Transplantation. Nephrol. Dial. Transplant. 2011, 26, 1456–1458. [Google Scholar] [CrossRef] [PubMed]
- Schaub, S.; Mayr, M.; Hönger, G.; Bestland, J.; Steiger, J.; Regeniter, A.; Mihatsch, M.J.; Wilkins, J.A.; Rush, D.; Nickerson, P. Detection of Subclinical Tubular Injury after Renal Transplantation: Comparison of Urine Protein Analysis with Allograft Histopathology. Transplantation 2007, 84, 104–112. [Google Scholar] [CrossRef]
- Kielar, M.; Dumnicka, P.; Gala-Błądzińska, A.; Będkowska-Prokop, A.; Ignacak, E.; Maziarz, B.; Ceranowicz, P.; Kuśnierz-Cabala, B. Urinary NGAL Measured after the First Year Post Kidney Transplantation Predicts Changes in Glomerular Filtration over One-Year Follow-Up. J. Clin. Med. 2020, 10, 43. [Google Scholar] [CrossRef] [PubMed]
- Song, L.; Xue, L.; Yu, J.; Zhao, J.; Zhang, W.; Fu, Y. Kidney Injury Molecule-1 Expression Is Closely Associated with Renal Allograft Damage. Bosn. J. Basic. Med. Sci. 2013, 13, 170–174. [Google Scholar] [CrossRef] [PubMed]
- Zhu, M.; Chen, Z.; Wei, Y.; Yuan, Y.; Ying, L.; Zhou, H.; Che, X.; Zhang, M.F.; Ni, Z.; Zhang, M.; et al. The Predictive Value of Urinary Kidney Injury Molecular-1 for Long-Term Graft Function in Kidney Transplant Patients: A Prospective Study. Ann. Transl. Med. 2021, 9, 244. [Google Scholar] [CrossRef]
- Jin, Z.-K.; Tian, P.-X.; Wang, X.-Z.; Xue, W.-J.; Ding, X.-M.; Zheng, J.; Ding, C.-G.; Mao, T.-C.; Duan, W.-L.; Xi, M. Kidney Injury Molecule-1 and Osteopontin: New Markers for Prediction of Early Kidney Transplant Rejection. Mol. Immunol. 2013, 54, 457–464. [Google Scholar] [CrossRef]
- Malyszko, J.; Koc-Zorawska, E.; Malyszko, J.S.; Mysliwiec, M. Kidney Injury Molecule-1 Correlates with Kidney Function in Renal Allograft Recipients. Transplant. Proc. 2010, 42, 3957–3959. [Google Scholar] [CrossRef]
- Nijboer, W.N.; Schuurs, T.A.; Damman, J.; van Goor, H.; Vaidya, V.S.; van der Heide, J.J.H.; Leuvenink, H.G.D.; Bonventre, J.V.; Ploeg, R.J. Kidney Injury Molecule-1 Is an Early Noninvasive Indicator for Donor Brain Death-Induced Injury Prior to Kidney Transplantation. Am. J. Transplant. 2009, 9, 1752–1759. [Google Scholar] [CrossRef]
- Hollmen, M.E.; Kyllönen, L.E.; Inkinen, K.A.; Lalla, M.L.T.; Salmela, K.T. Urine Neutrophil Gelatinase-Associated Lipocalin Is a Marker of Graft Recovery after Kidney Transplantation. Kidney Int. 2011, 79, 89–98. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Type of Transplant | Living Donor | Cadaveric Donor (≥55 Years) | Cadaveric Donor (<55 Years) | Double Transplant (Kidney–Pancreas) | Total/ Media ± SEM |
|---|---|---|---|---|---|
| Patients number | 9 (12.8%) | 35 (50%) | 17 (24.3%) | 9 (12.8%) | 70 (100%) |
| Sex of donor (F/M, number) | 5/4 (56/44%) | 25/10 (71/29%) | 8/9 (47/53%) | 2/7 (22/78%) | 39/31 (56/44%) |
| Age of donor (years) | 49.6 ± 3.8 | 66.6 ± 1.0 | 43.2 ± 2.6 | 35.0 ± 2.9 | 54.6 ± 1.8 |
| Sex of recipient (F/M, number) | 2/7 (22/78%) | 13/22 (37/63%) | 5/12 (29/71%) | 4/5 (44/56%) | 24/46 (34/66%) |
| Age of recipient (years) | 46.6 ± 4.6 | 66.0 ± 1.3 | 47.0 ± 3.5 | 41.3 ± 2.0 | 56.0 ± 1.8 |
| Cold ischemia time (minutes) | 88 ± 4 | 934 ± 74 | 1120 ± 45 | 817 ± 48 | 855 ± 54 |
| AR (Incidence) | 1 (11%) | 8 (23%) | 3 (18%) | 0 (0%) | 12 (17%) |
| DGF (Incidence) | 2 (22%) | 16 (46%) | 5 (29%) | 0 (0%) | 23 (33%) |
| AR + DGF (Incidence) | 1 (11%) | 6 (17%) | 3 (18%) | 0 (0%) | 10 (14%) |
| Nephrotoxic drugs administration * (Incidence) | 0 (0%) | 8 (23%) | 3 (18%) | 2 (22%) | 13 (19%) |
| Immunosuppressive Drug | Posology | Observations |
|---|---|---|
| Basiliximab | 20 mg, days 0 and 4 | -Immunosuppression inducer; -In patients with double transplant (kidney-pancreas) it was replaced by thymoglobuline. |
| Tacrolimus | 0.1 mg/kg, every 12 h | -If age of donor or recipient was greater than 55 years, its introduction was delayed until day 4; -It was replaced by CsA in one patient. |
| Mycophenolate Mofetil | 1 g, every 12 h | -It was replaced by azathioprine in three patients. |
| 6-Methylprednisolone | 500 mg, day 1 125 mg, day 2 | -Doses were halved for diabetic patients. |
| Prednisone | 20 mg, from day 3, following a descending regimen up to 10 mg | -Doses were halved for diabetic patients. |
| Type of Transplant | AR | DGF | DGF and AR | Cold Ischemia Time | Nephrotoxic Drug Administration | Time to Renal Function Stabilisation | |||
|---|---|---|---|---|---|---|---|---|---|
| NAG | W1 | χ2 | 8.708 | 2.737 | 3.109 | 4.178 | 4.514 | 2.064 | 39.427 |
| p value | 0.191 | 0.254 | 0.211 | 0.653 | 0.341 | 0.356 | <0.001 | ||
| D3 | χ2 | 35.514 | 2.195 | 2.220 | 4.276 | 20.397 | 2.067 | 9.621 | |
| p value | <0.001 | 0.334 | 0.329 | 0.639 | <0.001 | 0.356 | 0.138 | ||
| NGAL | W1 | χ2 | 9.145 | 3.223 | 17.194 | 17.461 | 3.486 | 0.550 | 41.045 |
| p value | 0.166 | 0.200 | <0.001 | 0.008 | 0.480 | 0.760 | <0.001 | ||
| D7 | χ2 | 14.731 | 3.830 | 20.950 | 22.443 | 2.969 | 1.372 | 10.419 | |
| p value | 0.022 | 0.147 | <0.001 | 0.001 | 0.563 | 0.504 | 0.108 | ||
| KIM-1 | W1 | χ2 | 17.216 | 1.678 | 2.583 | 3.976 | 4.131 | 1.889 | 35.053 |
| p value | 0.009 | 0.432 | 0.275 | 0.680 | 0.389 | 0.389 | <0.001 | ||
| D3 | χ2 | 35.726 | 1.183 | 4.436 | 6.390 | 14.341 | 3.291 | 3.107 | |
| p value | <0.001 | 0.554 | 0.109 | 0.381 | 0.006 | 0.583 | 0.807 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tabernero, G.; Pescador, M.; Ruiz Ferreras, E.; Morales, A.I.; Prieto, M. Evaluation of NAG, NGAL, and KIM-1 as Prognostic Markers of the Initial Evolution of Kidney Transplantation. Diagnostics 2023, 13, 1843. https://doi.org/10.3390/diagnostics13111843
Tabernero G, Pescador M, Ruiz Ferreras E, Morales AI, Prieto M. Evaluation of NAG, NGAL, and KIM-1 as Prognostic Markers of the Initial Evolution of Kidney Transplantation. Diagnostics. 2023; 13(11):1843. https://doi.org/10.3390/diagnostics13111843
Chicago/Turabian StyleTabernero, Guadalupe, Moisés Pescador, Elena Ruiz Ferreras, Ana I. Morales, and Marta Prieto. 2023. "Evaluation of NAG, NGAL, and KIM-1 as Prognostic Markers of the Initial Evolution of Kidney Transplantation" Diagnostics 13, no. 11: 1843. https://doi.org/10.3390/diagnostics13111843