
Update on Corneal Confocal Microscopy Imaging

 , and
, and
Abstract
:1. Introduction
2. Normal Cornea Observed with Confocal Microscopy
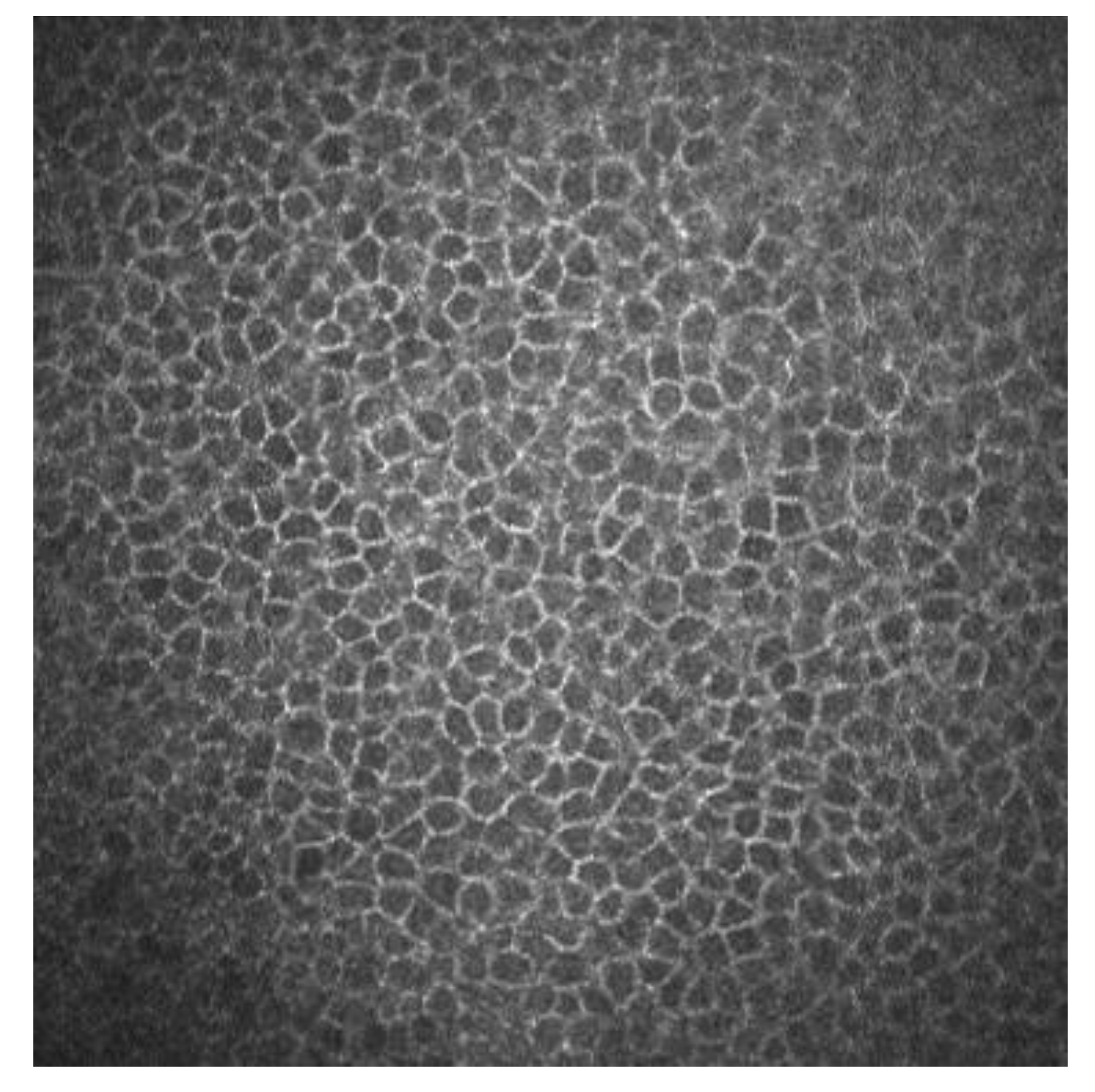
2.1. Corneal Epithelium
2.2. Sub-Basal Nerves
2.3. Bowman’s Layer
2.4. Corneal Stroma
2.5. Descemet Membrane
2.6. Endothelium
3. Some Applications of IVCM Images
3.1. Corneal Laser Refractive Surgery
3.1.1. Corneal Wound Healing
3.1.2. Nerve Regeneration after Refractive Surgery
3.1.3. Ocular Surface Pathologies
3.1.4. Dry Eye Disease (DED)
3.2. Small Fiber Neuropathies
3.3. Diabetic Neuropathy
3.4. Neuroborreliosis in Lyme Disease
4. COVID-19
5. Dementia
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Patel, D.V.; McGhee, C.N. Mapping of the normal human corneal sub-Basal nerve plexus by in vivo laser scanning confocal microscopy. Investig. Ophthalmol. Vis. Sci. 2005, 46, 4485–4488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masters, B.R.; Böhnke, M. Confocal microscopy of the human cornea in vivo. Int. Ophthalmol. 2001, 23, 199–206. [Google Scholar] [CrossRef]
- Mustonen, R.K.; McDonald, M.B.; Srivannaboon, S.; Tan, A.L.; Doubrava, M.W.; Kim, C.K. Normal human corneal cell populations evaluated by in vivo scanning slit confocal microscopy. Cornea 1998, 17, 485–492. [Google Scholar] [CrossRef] [PubMed]
- Masters, B.R.; Thaer, A.A. In vivo human corneal confocal microscopy of identical fields of subepithelial nerve plexus, basal epithelial, and wing cells at different times. Microsc. Res. Tech. 1994, 29, 350–356. [Google Scholar] [CrossRef]
- Popper, M.; Morgado, A.M.; Quadrado, M.J.; Van Best, J.A. Corneal cell density measurement in vivo by scanning slit confocal microscopy: Method and validation. Ophthalmic. Res. 2004, 36, 270–276. [Google Scholar] [CrossRef]
- Oliveira-Soto, L.; Efron, N. Morphology of corneal nerves in soft contact lens wear. A comparative study using confocal microscopy. Ophthalmic. Physiol. Opt. 2003, 23, 163–174. [Google Scholar] [CrossRef]
- Cruzat, A.; Qazi, Y.; Hamrah, P. In Vivo Confocal Microscopy of Corneal Nerves in Health and Disease. Ocul. Surf. 2017, 15, 15–47. [Google Scholar] [CrossRef] [Green Version]
- Zhivov, A.; Stave, J.; Vollmar, B.; Guthoff, R. In vivo confocal microscopic evaluation of Langerhans cell density and distribution in the normal human corneal epithelium. Graefes Arch. Clin. Exp. Ophthalmol. 2005, 243, 1056–1061. [Google Scholar] [CrossRef]
- Imre, L.; Nagymihály, A. Reliability and reproducibility of corneal endothelial image analysis by in vivo confocal microscopy. Graefes Arch. Clin. Exp. Ophthalmol. 2001, 239, 356–360. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S.E.; Mohan, R.R.; Hong, J.W.; Lee, J.S.; Choi, R. The wound healing response after laser in situ keratomileusis and photorefractive keratectomy: Elusive control of biological variability and effect on custom laser vision correction. Arch. Ophthalmol. 2001, 119, 889–896. [Google Scholar] [CrossRef]
- Dawson, D.G.; Kramer, T.R.; Grossniklaus, H.E.; Waring, G.O., 3rd; Edelhauser, H.F. Histologic, ultrastructural, and immunofluorescent evaluation of human laser-assisted in situ keratomileusis corneal wounds. Arch. Ophthalmol. 2005, 123, 741–756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuominen, I.S.; Tervo, T.M.; Teppo, A.M.; Valle, T.U.; Grönhagen-Riska, C.; Vesaluoma, M.H. Human tear fluid PDGF-BB, TNF-alpha and TGF-beta1 vs corneal haze and regeneration of corneal epithelium and subbasal nerve plexus after PRK. Exp. Eye Res. 2001, 72, 631–641. [Google Scholar] [CrossRef] [PubMed]
- Torricelli, A.A.; Santhanam, A.; Wu, J.; Singh, V.; Wilson, S.E. The corneal fibrosis response to epithelial-stromal injury. Exp. Eye Res. 2016, 142, 110–118. [Google Scholar] [CrossRef] [Green Version]
- de Benito-Llopis, L.; Canadas, P.; Drake, P.; Hernandez-Verdejo, J.L.; Teus, M.A. Keratocyte density 3 months, 15 months, and 3 years after corneal surface ablation with mitomycin C. Am. J. Ophthalmol. 2012, 153, 17–23. [Google Scholar] [CrossRef]
- McLaren, J.W.; Bourne, W.M.; Maguire, L.J.; Patel, S.V. Changes in Keratocyte Density and Visual Function Five Years After Laser In Situ Keratomileusis: Femtosecond Laser Versus Mechanical Microkeratome. Am. J. Ophthalmol. 2015, 160, 163–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Benito Llopis, L.; Drake, P.; Cañadas, P.; Hernandez-Verdejo, J.L.; Teus, M.A. Keratocyte density after laser-assisted subepithelial keratectomy with mitomycin C. Am. J. Ophthalmol. 2010, 150, 642–649. [Google Scholar] [CrossRef]
- Erie, J.C.; McLaren, J.W.; Hodge, D.O.; Bourne, W.M. Recovery of corneal subbasal nerve density after PRK and LASIK. Am. J. Ophthalmol. 2005, 140, 1059–1064. [Google Scholar] [CrossRef]
- Cañadas, P.; Garcia-Gonzalez, M.; Gros-Otero, J.; Rodriguez-Perez, I.; Cañones-Zafra, R.; Teus, M.A. Effect of Laser-assisted Subepithelial Keratectomy with Mitomycin C on Corneal Optical Density Measured with Confocal Microscopy. Optom. Vis. Sci. 2021, 98, 350–354. [Google Scholar] [CrossRef]
- Netto, M.V.; Mohan, R.R.; Sinha, S.; Sharma, A.; Dupps, W.; Wilson, S.E. Stromal haze, myofibroblasts, and surface irregularity after PRK. Exp. Eye Res. 2006, 82, 788–797. [Google Scholar] [CrossRef] [Green Version]
- Chang, S.W. Corneal keratocyte apoptosis following topical intraoperative mitomycin C in rabbits. J. Refract. Surg. 2005, 21, 446–453. [Google Scholar] [CrossRef]
- Pal-Ghosh, S.; Tadvalkar, G.; Lieberman, V.R. Transient Mitomycin C-treatment of human corneal epithelial cells and fibroblasts alters cell migration, cytokine secretion, and matrix accumulation. Sci. Rep. 2019, 9, 13905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Netto, M.V.; Mohan, R.R.; Sinha, S.; Sharma, A.; Gupta, P.C.; Wilson, S.E. Effect of prophylactic and therapeutic mitomycin C on corneal apoptosis, cellular proliferation, haze, and long-term keratocyte density in rabbits. J. Refract. Surg. 2006, 22, 562–574. [Google Scholar] [CrossRef] [Green Version]
- Dupps, W.J., Jr.; Wilson, S.E. Biomechanics and wound healing in the cornea. Exp. Eye Res. 2006, 83, 709–720. [Google Scholar] [CrossRef] [Green Version]
- Kezirian, G.M.; Stonecipher, K.G. Comparison of the IntraLase femtosecond laser and mechanical keratomes for laser in situ keratomileusis. J. Cataract Refract. Surg. 2004, 30, 804–811. [Google Scholar] [CrossRef]
- Petroll, W.M.; Bowman, R.W.; Cavanagh, H.D.; Verity, S.M.; Mootha, V.V.; McCulley, J.P. Assessment of keratocyte activation following LASIK with flap creation using the IntraLase FS60 laser. J. Refract. Surg. 2008, 24, 847–849. [Google Scholar]
- Ortiz, D.; Alió, J.L.; Piñero, D. Measurement of corneal curvature change after mechanical laser in situ keratomileusis flap creation and femtosecond laser flap creation. J. Cataract Refract. Surg. 2008, 34, 238–242. [Google Scholar] [CrossRef]
- Santhiago, M.R.; Wilson, S.E. Cellular effects after laser in situ keratomileusis flap formation with femtosecond lasers: A review. Cornea 2012, 31, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Cañadas, P.; de Benito-Llopis, L.; Hernandez-Verdejo, J.L.; Teus, M.A. Comparison of keratocyte density after femtosecond laser vs. mechanical microkeratome from 3 months up to 5 years after LASIK. Graefes Arch. Clin. Exp. Ophthalmol. 2013, 251, 2171–2179. [Google Scholar] [CrossRef] [PubMed]
- Marfurt, C.F.; Cox, J.; Deek, S.; Dvorscak, L. Anatomy of the human corneal innervation. Exp. Eye Res. 2010, 90, 478–492. [Google Scholar] [CrossRef]
- Zhang, F.; Deng, S.; Guo, N.; Wang, M.; Sun, X. Confocal comparison of corneal nerve regeneration and keratocyte reaction between FS-LASIK, OUP-SBK, and conventional LASIK. Investig. Ophthalmol. Vis. Sci. 2012, 53, 5536–5544. [Google Scholar] [CrossRef]
- Garcia-Gonzalez, M.; Cañadas, P.; Gros-Otero, J. Long-term corneal subbasal nerve plexus regeneration after laser in situ keratomileusis. J. Cataract Refract. Surg. 2019, 45, 966–971. [Google Scholar] [CrossRef]
- Lopez-De La Rosa, A.; Arroyo-Del Arroyo, C.; Cañadas, P. Are Contact Lens Discomfort or Soft Contact Lens Material Properties Associated with Alterations in the Corneal Sub-Basal Nerve Plexus? Curr. Eye Res. 2018, 43, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Cruzat, A.; Witkin, D.; Baniasadi, N. Inflammation and the nervous system: The connection in the cornea in patients with infectious keratitis. Investig. Ophthalmol. Vis. Sci. 2011, 52, 5136–5143. [Google Scholar] [CrossRef]
- Maycock, N.J.; Jayaswal, R. Update on Acanthamoeba Keratitis: Diagnosis, Treatment, and Outcomes. Cornea 2016, 35, 713–720. [Google Scholar] [CrossRef] [PubMed]
- Tu, E.Y.; Joslin, C.E.; Sugar, J.; Booton, G.C.; Shoff, M.E.; Fuerst, P.A. The relative value of confocal microscopy and superficial corneal scrapings in the diagnosis of Acanthamoeba keratitis. Cornea 2008, 27, 764–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goh, J.W.Y.; Harrison, R.; Hau, S.; Alexander, C.L.; Tole, D.M.; Avadhanam, V.S. Comparison of In Vivo Confocal Microscopy, PCR and Culture of Corneal Scrapes in the Diagnosis of Acanthamoeba Keratitis. Cornea 2018, 37, 480–485. [Google Scholar] [CrossRef]
- Kheirkhah, A.; Satitpitakul, V.; Syed, Z.A. Factors Influencing the Diagnostic Accuracy of Laser-Scanning In Vivo Confocal Microscopy for Acanthamoeba Keratitis. Cornea 2018, 37, 818–823. [Google Scholar] [CrossRef]
- Huang, P.; Tepelus, T.; Vickers, L.A. Quantitative Analysis of Depth, Distribution, and Density of Cysts in Acanthamoeba Keratitis Using Confocal Microscopy. Cornea 2017, 36, 927–932. [Google Scholar] [CrossRef]
- Li, S.; Bian, J.; Wang, Y.; Wang, S.; Wang, X.; Shi, W. Clinical features and serial changes of Acanthamoeba keratitis: An in vivo confocal microscopy study. Eye 2020, 34, 327–334. [Google Scholar] [CrossRef]
- Chopra, R.; Mulholland, P.J.; Hau, S.C. In Vivo Confocal Microscopy Morphologic Features and Cyst Density in Acanthamoeba Keratitis. Am. J. Ophthalmol. 2020, 217, 38–48. [Google Scholar] [CrossRef]
- Craig, J.P.; Nichols, K.K.; Akpek, E.K. TFOS DEWS II Definition and Classification Report. Ocul. Surf. 2017, 15, 276–283. [Google Scholar] [CrossRef]
- Bron, A.J.; de Paiva, C.S.; Chauhan, S.K.; Bonini, S.; Gabison, E.E.; Jain, S.; Knop, E.; Markoulli, M.; Ogawa, Y.; Perez, V.; et al. TFOS DEWS II pathophysiology report. Ocul. Surf. 2017, 15, 438–510. [Google Scholar] [CrossRef]
- Willcox, M.D.P.; Argüeso, P.; Georgiev, G.A.; Holopainen, J.M.; Laurie, G.W.; Millar, T.J.; Papas, E.B.; Rolland, J.P.; Schmidt, T.A.; Stahl, U.; et al. TFOS DEWS II Tear Film Report. Ocul. Surf. 2017, 15, 366–403. [Google Scholar] [CrossRef] [Green Version]
- Kheirkhah, A.; Rahimi Darabad, R.; Cruzat, A. Corneal Epithelial Immune Dendritic Cell Alterations in Subtypes of Dry Eye Disease: A Pilot In Vivo Confocal Microscopic Study. Investig. Ophthalmol. Vis. Sci. 2015, 56, 7179–7185. [Google Scholar] [CrossRef]
- Lin, H.; Li, W.; Dong, N. Changes in corneal epithelial layer inflammatory cells in aqueous tear-deficient dry eye. Investig. Ophthalmol. Vis. Sci. 2010, 51, 122–128. [Google Scholar] [CrossRef]
- Schaumburg, C.S.; Siemasko, K.F.; De Paiva, C.S. Ocular surface APCs are necessary for autoreactive T cell-mediated experimental autoimmune lacrimal keratoconjunctivitis. J. Immunol. 2011, 187, 3653–3662. [Google Scholar] [CrossRef] [Green Version]
- Stevenson, W.; Chauhan, S.K.; Dana, R. Dry eye disease: An immune-mediated ocular surface disorder. Arch. Ophthalmol. 2012, 130, 90–100. [Google Scholar] [CrossRef] [Green Version]
- Barabino, S.; Chen, Y.; Chauhan, S.; Dana, R. Ocular surface immunity: Homeostatic mechanisms and their disruption in dry eye disease. Prog. Retin. Eye Res. 2012, 31, 271–285. [Google Scholar] [CrossRef] [Green Version]
- Jamali, A.; Kenyon, B.; Ortiz, G. Plasmacytoid dendritic cells in the eye. Prog. Retin. Eye Res. 2021, 80, 1008–1077. [Google Scholar] [CrossRef]
- Merola, A.; Rosso, M.; Romagnolo, A. Peripheral neuropathy as marker of severe Parkinson’s disease phenotype. Mov. Disord. 2017, 32, 1256–1258. [Google Scholar] [CrossRef]
- Donadio, V.; Incensi, A.; Leta, V. Skin nerve α-synuclein deposits: A biomarker for idiopathic Parkinson disease. Neurology 2014, 82, 1362–1369. [Google Scholar] [CrossRef] [PubMed]
- Petropoulos, I.N.; Alam, U.; Fadavi, H. Rapid automated diagnosis of diabetic peripheral neuropathy with in vivo corneal confocal microscopy. Investig. Ophthalmol. Vis. Sci. 2014, 55, 2071–2078. [Google Scholar] [CrossRef] [PubMed]
- Wang, E.F.; Misra, S.L.; Patel, D.V. In Vivo Confocal Microscopy of the Human Cornea in the Assessment of Peripheral Neuropathy and Systemic Diseases. Biomed. Res. Int. 2015, 20, 951–981. [Google Scholar] [CrossRef] [Green Version]
- Tavakoli, M.; Marshall, A.; Pitceathly, R. Corneal confocal microscopy: A novel means to detect nerve fibre damage in idiopathic small fibre neuropathy. Exp. Neurol. 2010, 223, 245–250. [Google Scholar] [CrossRef] [Green Version]
- Tavakoli, M.; Marshall, A.; Thompson, L. Corneal confocal microscopy: A novel noninvasive means to diagnose neuropathy in patients with Fabry disease. Muscle Nerve. 2009, 40, 976–984. [Google Scholar] [CrossRef] [PubMed]
- Kallinikos, P.; Berhanu, M.; O’Donnell, C.; Boulton, A.J.; Efron, N.; Malik, R.A. Corneal nerve tortuosity in diabetic patients with neuropathy. Investig. Ophthalmol. Vis. Sci. 2004, 45, 418–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Cilla, S.; Ranno, S.; Carini, E. Corneal subbasal nerves changes in patients with diabetic retinopathy: An in vivo confocal study. Investig. Ophthalmol. Vis. Sci. 2009, 50, 5155–5158. [Google Scholar] [CrossRef]
- Lim, S.H.; Ferdousi, M.; Kalteniece, A. Corneal confocal microscopy detects small fibre neurodegeneration in Parkinson’s disease using automated analysis. Sci. Rep. 2020, 10, 201–247. [Google Scholar] [CrossRef]
- Alam, U.; Jeziorska, M.; Petropoulos, I.N. Diagnostic utility of corneal confocal microscopy and intra-epidermal nerve fibre density in diabetic neuropathy. PLoS ONE 2017, 12, e0180175. [Google Scholar] [CrossRef] [Green Version]
- Dabbah, M.A.; Graham, J.; Petropoulos, I.N.; Tavakoli, M.; Malik, R.A. Automatic analysis of diabetic peripheral neuropathy using multi-scale quantitative morphology of nerve fibres in corneal confocal microscopy imaging. Med. Image Anal. 2011, 15, 738–747. [Google Scholar] [CrossRef]
- Markoulli, M.; Flanagan, J.; Tummanapalli, S.S.; Wu, J.; Willcox, M. The impact of diabetes on corneal nerve morphology and ocular surface integrity. Ocul. Surf. 2018, 16, 45–57. [Google Scholar] [CrossRef]
- Hicks, C.W.; Selvin, E. Epidemiology of Peripheral Neuropathy and Lower Extremity Disease in Diabetes. Curr. Diab. Rep. 2019, 19, 86. [Google Scholar] [CrossRef]
- Ahmed, A.; Bril, V.; Orszag, A. Detection of diabetic sensorimotor polyneuropathy by corneal confocal microscopy in type 1 diabetes: A concurrent validity study. Diabetes Care 2012, 35, 821–828. [Google Scholar] [CrossRef] [Green Version]
- Cosmo, E.; Midena, G.; Frizziero, L.; Bruno, M.; Cecere, M.; Midena, E. Corneal Confocal Microscopy as a Quantitative Imaging Biomarker of Diabetic Peripheral Neuropathy: A Review. J. Clin. Med. 2022, 11, 5130. [Google Scholar] [CrossRef]
- Thomas, P.K. Classification, differential diagnosis, and staging of diabetic peripheral neuropathy. Diabetes 1997, 46 (Suppl. 2), S54–S57. [Google Scholar] [CrossRef]
- Carmichael, J.; Fadavi, H.; Ishibashi, F. Implementation of corneal confocal microscopy for screening and early detection of diabetic neuropathy in primary care alongside retinopathy screening: Results from a feasibility study. Front. Endocrinol. 2022, 13, 891575. [Google Scholar] [CrossRef]
- Garcia-Monco, J.C.; Benach, J.L. Lyme Neuroborreliosis: Clinical Outcomes, Controversy, Pathogenesis, and Polymicrobial Infections. Ann. Neurol. 2019, 85, 21–31. [Google Scholar] [CrossRef]
- Telford, S.R., 3rd; Goethert, H.K.; Molloy, P.J. Borrelia miyamotoi Disease: Neither Lyme Disease Nor Relapsing Fever. Clin. Lab. Med. 2015, 35, 867–882. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Graham, J.; Dabbah, M.A. Small nerve fiber quantification in the diagnosis of diabetic sensorimotor polyneuropathy: Comparing corneal confocal microscopy with intraepidermal nerve fiber density. Diabetes Care 2015, 38, 1138–1144. [Google Scholar] [CrossRef] [Green Version]
- Lukashenko, M.V.; Gavrilova, N.Y.; Bregovskaya, A.V. Corneal Confocal Microscopy in the Diagnosis of Small Fiber Neuropathy: Faster, Easier, and More Efficient Than Skin Biopsy? Pathophysiology 2021, 29, 1–8. [Google Scholar] [CrossRef]
- Scoppettuolo, P.; Borrelli, S.; Naeije, G. Neurological involvement in SARS-CoV-2 infection: A clinical systematic review. Brain Behav. Immun. Health. 2020, 5, 100094. [Google Scholar] [CrossRef] [PubMed]
- Dehghani, C.; Frost, S.; Jayasena, R. Morphometric Changes to Corneal Dendritic Cells in Individuals With Mild Cognitive Impairment. Front. Neurosci. 2020, 14, 556137. [Google Scholar] [CrossRef]
- Douglas, K.A.A.; Douglas, V.P.; Moschos, M.M. Ocular Manifestations of COVID-19 (SARS-CoV-2): A Critical Review of Current Literature. In Vivo 2020, 34 (Suppl. 3), 1619–1628. [Google Scholar] [CrossRef]
- Odriozola, A.; Ortega, L.; Martinez, L. Widespread sensory neuropathy in diabetic patients hospitalized with severe COVID-19 infection. Diabetes Res. Clin. Pract. 2021, 172, 108631. [Google Scholar] [CrossRef]
- Lou, J.J.; Movassaghi, M.; Gordy, D. Neuropathology of COVID-19 (neuro-COVID): Clinicopathological update. Free Neuropathol. 2021, 2, 7861505. [Google Scholar]
- Ahmad, L.; Businaro, P.; Regalbuto, S. COVID-19 and Guillain-Barré syndrome: A single-center prospective case series with a 1-year follow-up. Medicine 2022, 101, e29704. [Google Scholar] [CrossRef] [PubMed]
- Faqihi, F.; Alharthy, A.; Memish, Z.A.; Kutsogiannis, D.J.; Brindley, P.G.; Karakitsos, D. Peripheral neuropathy in severe COVID-19 resolved with therapeutic plasma exchange. Clin. Case. Rep. 2020, 12, 3234–3239. [Google Scholar] [CrossRef]
- Al-Aqaba, M.A.; Fares, U.; Suleman, H.; Lowe, J.; Dua, H.S. Architecture and distribution of human corneal nerves. Br. J. Ophthalmol. 2010, 94, 784–789. [Google Scholar] [CrossRef] [Green Version]
- Patel, D.V.; McGhee, C.N. In vivo laser scanning confocal microscopy confirms that the human corneal sub-basal nerve plexus is a highly dynamic structure. Investig. Ophthalmol. Vis. Sci. 2008, 49, 3409–3412. [Google Scholar] [CrossRef] [Green Version]
- Marfurt, C.F.; Kingsley, R.E.; Echtenkamp, S.E. Sensory and sympathetic innervation of the mammalian cornea. A retrograde tracing study. Investig. Ophthalmol. Vis. Sci. 1989, 30, 461–472. [Google Scholar]
- Labetoulle, M.; Baudouin, C.; Calonge, M. Role of corneal nerves in ocular surface homeostasis and disease. Acta Ophthalmol. 2019, 97, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Ponirakis, G.; Al Hamad, H.; Sankaranarayanan, A. Association of corneal nerve fiber measures with cognitive function in dementia. Ann. Clin. Transl. Neurol. 2019, 6, 689–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chinnery, H.R.; Rajan, R.; Jiao, H. Identification of presumed corneal neuromas and microneuromas using laser-scanning in vivo confocal microscopy: A systematic review. Br. J. Ophthalmol. 2022, 106, 765–771. [Google Scholar] [CrossRef] [PubMed]
- Kolkedi, Z.; Csutak, A.; Szalai, E. Corneal Cellular and Neuroinflammatory Changes After SARS-CoV-2 Infection. Cornea 2022, 41, 879–885. [Google Scholar] [CrossRef] [PubMed]
- Bitirgen, G.; Korkmaz, C.; Zamani, A. Corneal confocal microscopy identifies corneal nerve fibre loss and increased dendritic cells in patients with long COVID. Br. J. Ophthalmol. 2021, 106, 1635–1641. [Google Scholar]
- Bitirgen, G.; Akpinar, Z.; Malik, R.A.; Ozkagnici, A. Use of Corneal Confocal Microscopy to Detect Corneal Nerve Loss and Increased Dendritic Cells in Patients with Multiple Sclerosis. JAMA Ophthalmol. 2017, 135, 777–782. [Google Scholar] [CrossRef]
- Thimm, A.; Carpinteiro, A.; Oubari, S. Corneal confocal microscopy to detect early immune-mediated small nerve fibre loss in AL amyloidosis. Ann. Clin. Transl. Neurol. 2022, 9, 853–863. [Google Scholar] [CrossRef]
- Mastropasqua, L.; Nubile, M.; Lanzini, M. Epithelial dendritic cell distribution in normal and inflamed human cornea: In vivo confocal microscopy study. Am. J. Ophthalmol. 2006, 142, 736–744. [Google Scholar] [CrossRef]
- Hamrah, P.; Huq, S.O.; Liu, Y.; Zhang, Q.; Dana, M.R. Corneal immunity is mediated by heterogeneous population of antigen-presenting cells. J. Leukoc. Biol. 2003, 74, 172–178. [Google Scholar] [CrossRef] [Green Version]
- Gao, N.; Lee, P.; Yu, F.S. Intraepithelial dendritic cells and sensory nerves are structurally associated and functional interdependent in the cornea. Sci. Rep. 2016, 6, 36414. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TSCM | SSCM | LSCM | |
|---|---|---|---|
| Light source | Mercury and Xenon | Halogen | Helium and Neon laser |
| Source intensity | High | Weak | High (limited) |
| Source wavelength | 400–700 nm | 370–510 nm | 670 nm (red) |
| Illumination and light detection | Rotating Nipkow disk (64,000 holes 20–60 microns in diameter) | Two conjugate slits | Two scanning mirrors and one scanner |
| Laser beam | Permanent | Permanent | Mobile |
| Scanning | Tracking using a motorized stage | Tracking using a motorized stage | Moving the laser beam in the eye |
| Corneal Cells | Morphology | Reflectivity |
|---|---|---|
| Superficial epithelial cells | Polygonal, with different sizes | Hyperreflective nucleus surrounded by dark band |
| Winged epithelial cells | Polygonal, with different sizes | Hyperreflective without visible nucleus |
| Basal epithelial cells | Polygonal. Mosaic shape | Dark cell bodies with bright borders |
| Stromal cells (keratocytes) | Oval | Hyperreflective |
| Dendritic cells | Dendritic shape in active status. Oval shape in nonactive status | Hyperreflective |
| Nerve plexus | Lineal | Hyperreflective |
| Endothelial cells | Hexagonal shape | Bright cell bodies with dark borders |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cañadas, P.; Alberquilla García-Velasco, M.; Hernández Verdejo, J.L.; Teus, M.A. Update on Corneal Confocal Microscopy Imaging. Diagnostics 2023, 13, 46. https://doi.org/10.3390/diagnostics13010046
Cañadas P, Alberquilla García-Velasco M, Hernández Verdejo JL, Teus MA. Update on Corneal Confocal Microscopy Imaging. Diagnostics. 2023; 13(1):46. https://doi.org/10.3390/diagnostics13010046
Chicago/Turabian StyleCañadas, Pilar, Marta Alberquilla García-Velasco, José Luis Hernández Verdejo, and Miguel A. Teus. 2023. "Update on Corneal Confocal Microscopy Imaging" Diagnostics 13, no. 1: 46. https://doi.org/10.3390/diagnostics13010046