
The Systematic Review of Artificial Intelligence Applications in Breast Cancer Diagnosis

Abstract
:1. Introduction
AI in Breast Cancer
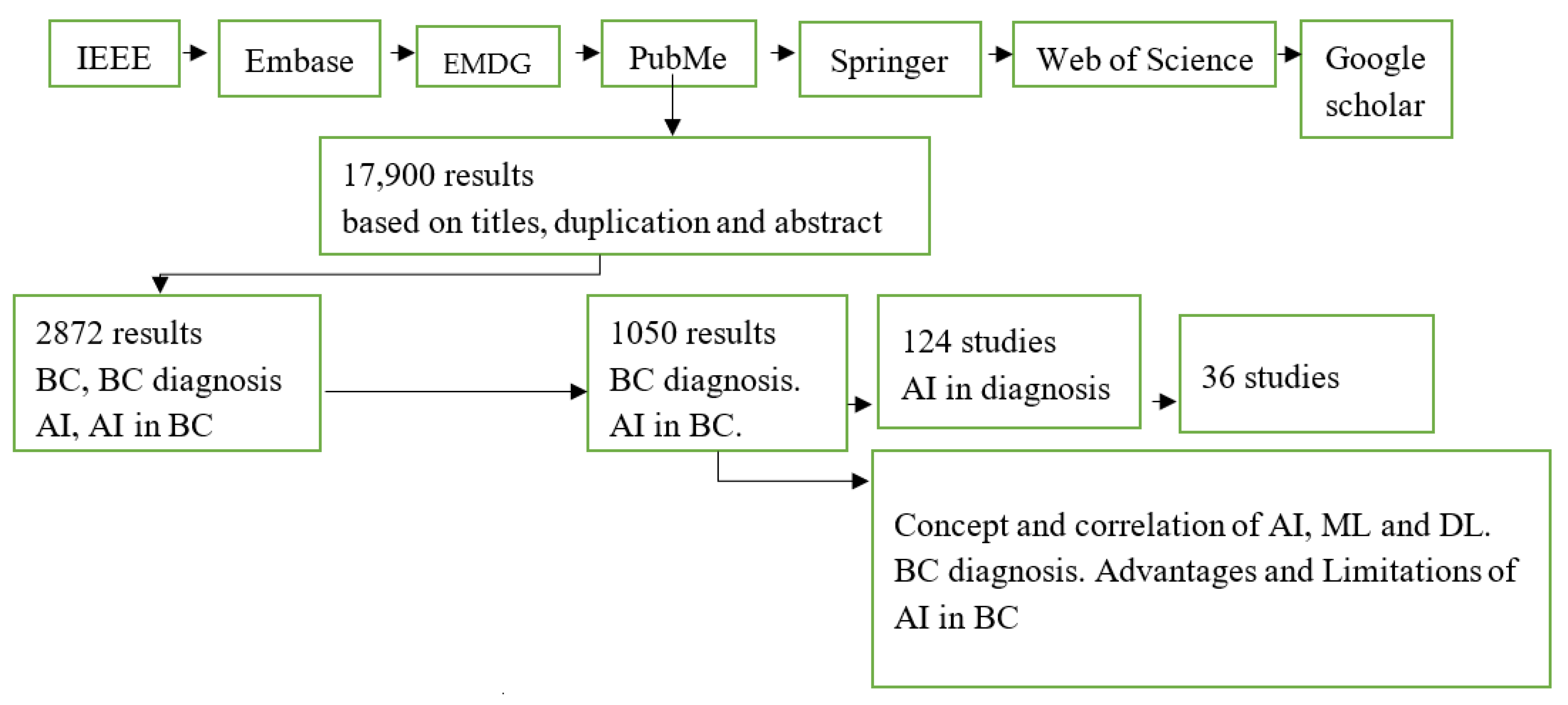
2. Methodology
3. Results and Discussion
3.1. Emerging Techniques of AI Applications in BC Diagnosis
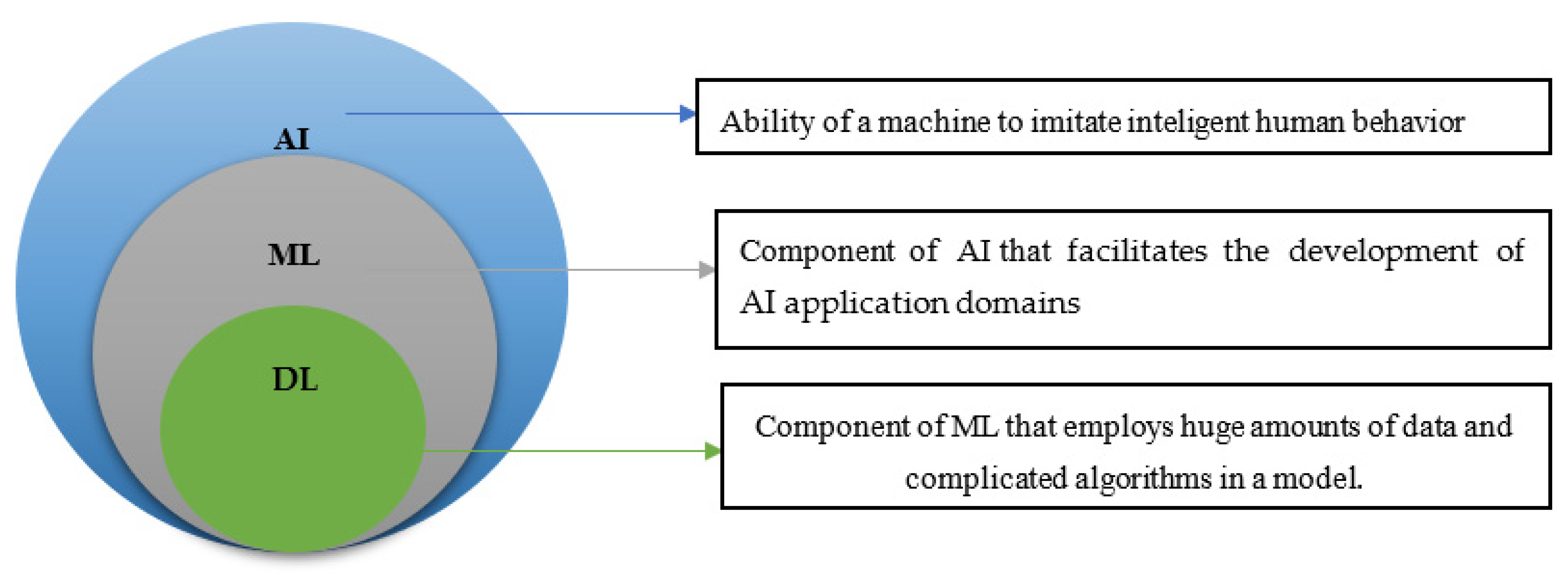
3.2. The Conception and Respective Correlations of AI, ML, and DL
3.3. BC Diagnosis Advantages
3.4. Limitation of AI in BC Diagnosis
4. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fortin, J.; Leblanc, M.; Elgbeili, G.; Cordova, M.J.; Marin, M.-F.; Brunet, A. The mental health impacts of receiving a breast cancer diagnosis: A meta-analysis. Br. J. Cancer 2021, 125, 1582–1592. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.; Naishadham, D.; Jemal, A. Cancer statistics, 2013. Cancer J. Clin. 2013, 63, 11–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beral, V.; Bull, D.; Doll, R.; Peto, R.; Reeves, G. Breast cancer and breastfeeding: Collaborative reanalysis of individual data from 47 epidemiological studies in 30 countries, including 50302 women with breast cancer and 96973 women without the disease. Lancet 2002, 360, 187–195. [Google Scholar] [CrossRef]
- Sieri, S.; Krogh, V.; Bolelli, G.; Abagnato, C.A.; Grioni, S.; Pala, V.; Evangelista, A.; Allemani, C.; Micheli, A.; Tagliabue, G.; et al. Sex Hormone Levels, Breast Cancer Risk, and Cancer Receptor Status in Postmenopausal Women: The ORDET Cohort. Cancer Epidemiology Biomarkers Prev. 2009, 18, 169–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colditz, G.A.; Kaphingst, K.A.; Hankinson, S.E.; Rosner, B. Family history and risk of breast cancer: Nurses’ health study. Breast Cancer Res. Treat. 2012, 133, 1097–1104. [Google Scholar] [CrossRef] [Green Version]
- Harbeck, N.; Penault-Llorca, F.; Cortes, J.; Gnant, M.; Houssami, N.; Poortmans, P.; Ruddy, K.; Tsang, J.; Cardoso, F. Breast cancer. Nat. Rev. Dis. Primers 2019, 5, 66. [Google Scholar] [CrossRef]
- Mahmood, T.; Li, J.; Pei, Y.; Akhtar, F.; Imran, A.; Rehman, K.U. A Brief Survey on Breast Cancer Diagnostic With Deep Learning Schemes Using Multi-Image Modalities. IEEE Access 2020, 8, 165779–165809. [Google Scholar] [CrossRef]
- Chiao, J.-Y.; Chen, K.-Y.; Liao, K.Y.-K.; Hsieh, P.-H.; Zhang, G.; Huang, T.-C. Detection and classification the breast tumors using mask R-CNN on sonograms. Medicine 2019, 98, e15200. [Google Scholar] [CrossRef]
- Cruz-Roa, A.; Gilmore, H.; Basavanhally, A.; Feldman, M.; Ganesan, S.; Shih, N.N.; Tomaszewski, J.; González, F.A.; Madabhushi, A. Accurate and reproducible invasive breast cancer detection in whole-slide images: A Deep Learning approach for quantifying tumor extent. Sci. Rep. 2017, 7, srep46450. [Google Scholar] [CrossRef] [Green Version]
- Wei, T.; Kanki, T.; Chikanari, M.; Uemura, T.; Sekitani, T.; Tanaka, H. Enhanced electronic-transport modulation in single-crystalline VO2 nanowire-based solid-state field-effect transistors. Sci. Rep. 2017, 7, 17215. [Google Scholar] [CrossRef]
- Breast Cancer Facts & Statistics 2022. Available online: https://www.breastcancer.org/facts-statistics (accessed on 4 November 2022).
- Breast Cancer. Available online: https://www.who.int/news-room/fact-sheets/detail/breast-cancer (accessed on 8 November 2022).
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA A Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef]
- Iqbal, M.J.; Javed, Z.; Sadia, H.; Qureshi, I.A.; Irshad, A.; Ahmed, R.; Malik, K.; Raza, S.; Abbas, A.; Pezzani, R.; et al. Clinical applications of artificial intelligence and machine learning in cancer diagnosis: Looking into the future. Cancer Cell Int. 2021, 21, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Prevedello, L.M.; Halabi, S.S.; Shih, G.; Wu, C.C.; Kohli, M.D.; Chokshi, F.H.; Erickson, B.J.; Kalpathy-Cramer, J.; Andriole, K.P.; Flanders, A.E. Challenges Related to Artificial Intelligence Research in Medical Imaging and the Importance of Image Analysis Competitions. Radiol. Artif. Intell. 2019, 1, e180031. [Google Scholar] [CrossRef] [PubMed]
- Nazir, A.; Khan, R.A. A novel combinatorial optimization based feature selection method for network intrusion detection. Comput. Secur. 2020, 102, 102164. [Google Scholar] [CrossRef]
- Crenn, A.; Meyer, A.; Konik, H.; Khan, R.A.; Bouakaz, S. Generic Body Expression Recognition Based on Synthesis of Realistic Neutral Motion. IEEE Access 2020, 8, 207758–207767. [Google Scholar] [CrossRef]
- Memon, J.; Sami, M.; Khan, R.A.; Uddin, M. Handwritten Optical Character Recognition (OCR): A Comprehensive Systematic Literature Review (SLR). IEEE Access 2020, 8, 142642–142668. [Google Scholar] [CrossRef]
- Marinovich, M.L.; Wylie, E.; Lotter, W.; Pearce, A.; Carter, S.M.; Lund, H.; Waddell, A.; Kim, J.G.; Pereira, G.F.; Lee, C.I.; et al. Artificial intelligence (AI) to enhance breast cancer screening: Protocol for population-based cohort study of cancer detection. BMJ Open 2022, 12, e054005. [Google Scholar] [CrossRef]
- Jaliaawala, M.S.; Khan, R.A. Can autism be catered with artificial intelligence-assisted intervention technology? A comprehensive survey. Artif. Intell. Rev. 2018, 53, 1039–1069. [Google Scholar] [CrossRef] [Green Version]
- Sun, P.; Feng, Y.; Chen, C.; Dekker, A.; Qian, L.; Wang, Z.; Guo, J. An AI model of sonographer’s evaluation+ S-Detect + elastography + clinical information improve the preoperative identification of benign and malignant breast masses. Front. Oncol. 2022, 12, 1022441. [Google Scholar] [CrossRef]
- Sharma, S.; Mehra, R. Conventional Machine Learning and Deep Learning Approach for Multi-Classification of Breast Cancer Histopathology Images—A Comparative Insight. J. Digit. Imaging 2020, 33, 632–654. [Google Scholar] [CrossRef]
- Burt, J.R.; Torosdagli, N.; Khosravan, N.; Raviprakash, H.; Mortazi, A.; Tissavirasingham, F.; Hussein, S.; Bagci, U. Deep learning beyond cats and dogs: Recent advances in diagnosing breast cancer with deep neural networks. Br. J. Radiol. 2018, 91, 20170545. [Google Scholar] [CrossRef] [PubMed]
- Buckner, C.A.; Lafrenie, R.; Dénommée, J.; Caswell, J.; Want, D.; Gan, G.; Leong, Y.; Bee, P.; Chin, E.; Teh, A.; et al. We are IntechOpen, the world’s leading publisher of Open Access books Built by scientists, for scientists TOP 1 %. Intech 2016, 11, 13, no. tourism. Available online: https://www.intechopen.com/books/advanced-biometric-technologies/liveness-detection-in-biometrics (accessed on 3 December 2022).
- Goyal, S.; Srivastava, B.R. Review of Artificial Intelligence Applicability of Various Diagnostic Modalities, their Advantages, Limitations, and Overcoming the Challenges in Breast Imaging. Int. J. Sci. Study 2021, 9, 16–21. [Google Scholar]
- Rodriguez-Ruiz, A.; Lång, K.; Gubern-Merida, A.; Broeders, M.; Gennaro, G.; Clauser, P.; Helbich, T.H.; Chevalier, M.; Tan, T.; Mertelmeier, T.; et al. Stand-Alone Artificial Intelligence for Breast Cancer Detection in Mammography: Comparison With 101 Radiologists. Gynecol. Oncol. 2019, 111, 916–922. [Google Scholar] [CrossRef]
- Liu, K.-L.; Wu, T.; Chen, P.-T.; Tsai, Y.M.; Roth, H.; Wu, M.-S.; Liao, W.-C.; Wang, W. Deep learning to distinguish pancreatic cancer tissue from non-cancerous pancreatic tissue: A retrospective study with cross-racial external validation. Lancet Digit. Health 2020, 2, e303–e313. [Google Scholar] [CrossRef]
- Balakrishnan, G.; Zhao, A.; Sabuncu, M.R.; Guttag, J.; Dalca, A.V. VoxelMorph: A Learning Framework for Deformable Medical Image Registration. IEEE Trans. Med. Imaging 2019, 38, 1788–1800. [Google Scholar] [CrossRef] [Green Version]
- Ronneberger, O.; Fischer, P.; Brox, T. U-net: Convolutional networks for biomedical image segmentation. In International Conference on Medical Image Computing and Computer-Assisted Intervention; Springer: Cham, Switzerland, 2015; Volume 9351, pp. 234–241. [Google Scholar] [CrossRef]
- Breast Cancer|Early Detection and Screening|CancerCare. Available online: https://www.cancercare.org/publications/82-breast_cancer_understanding_risk_factors_and_screening (accessed on 3 December 2022).
- Breast Cancer Early Detection—National Breast Cancer Foundation. Available online: https://www.nationalbreastcancer.org/early-detection-of-breast-cancer/ (accessed on 3 December 2022).
- Huang, S.; Yang, J.; Fong, S.; Zhao, Q. Artificial intelligence in cancer diagnosis and prognosis: Opportunities and challenges. Cancer Lett. 2019, 471, 61–71. [Google Scholar] [CrossRef]
- Witowski, J.; Heacock, L.; Reig, B.; Kang, S.K.; Lewin, A.; Pysarenko, K.; Patel, S.; Samreen, N.; Rudnicki, W.; Łuczyńska, E.; et al. Improving breast cancer diagnostics with DL for MRI. Sci. Transl. Med. 2 2022, 14, eabo4802. [Google Scholar] [CrossRef]
- Cole, E.B.; Zhang, Z.; Marques, H.S.; Nishikawa, R.M.; Hendrick, R.E.; Yaffe, M.J.; Padungchaichote, W.; Kuzmiak, C.; Chayakulkheeree, J.; Conant, E.F.; et al. Assessing the Stand-Alone Sensitivity of Computer-Aided Detection with Cancer Cases From the Digital Mammographic Imaging Screening Trial. AJR Am. J. Roentgenol. 2012, 199, W392. [Google Scholar] [CrossRef] [Green Version]
- Díaz, O.; Rodríguez-Ruiz, A.; Gubern-Mérida, A.; Martí, R.; Chevalier, M. Are artificial intelligence systems useful in breast cancer screening programs? Radiologia 2021, 63, 236–244. [Google Scholar] [CrossRef]
- Trister, A.D.; Buist, D.S.M.; Lee, C.I. Will Machine Learning Tip the Balance in Breast Cancer Screening? JAMA Oncol. 2017, 3, 1463. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Cui, G.; Luo, Y.; Guo, Y.; Zhao, L.; Wang, Y.; Subasi, A.; Dogan, S.; Tuncer, T. Artificial Intelligence-Based Breast Cancer Diagnosis Using Ultrasound Images and Grid-Based Deep Feature Generator. Int. J. Gen. Med. 2022, 15, 2271–2282. [Google Scholar] [CrossRef] [PubMed]
- Goyal, S. Essentials of Abdomino-Pelvic Sonography: A Handbook for Practitioners; CRC Press: Boca Raton, FL, USA, 2020; Available online: https://www.routledge.com/Essentials-of-Abdomino-Pelvic-Sonography-A-Handbook-for-Practitioners/Goyal/p/book/9780367572303 (accessed on 3 December 2022).
- Lee, J.; Kang, B.J.; Kim, S.H.; Park, G.E. Evaluation of Computer-Aided Detection (CAD) in Screening Automated Breast Ultrasound Based on Characteristics of CAD Marks and False-Positive Marks. Diagnostics 2022, 12, 583. [Google Scholar] [CrossRef]
- Parvathavarthini, S.; Visalakshi, N.K.; Shanthi, S. Breast Cancer Detection using Crow Search Optimization based Intuitionistic Fuzzy Clustering with Neighborhood Attraction. Asian Pac. J. Cancer Prev. 2019, 20, 157–165. [Google Scholar] [CrossRef] [Green Version]
- Abdel-Zaher, A.M.; Eldeib, A.M. Breast cancer classification using deep belief networks. Expert Syst. Appl. 2016, 46, 139–144. [Google Scholar] [CrossRef]
- Karabatak, M. A new classifier for breast cancer detection based on Naïve Bayesian. Measurement 2015, 72, 32–36. [Google Scholar] [CrossRef]
- Zafiropoulos, E.; Maglogiannis, I.; Anagnostopoulos, I. A support vector machine approach to breast cancer diagnosis and prognosis. IFIP Int. Fed. Inf. Process. 2006, 204, 500–507. [Google Scholar] [CrossRef]
- Shah, S.M.; Khan, R.A.; Arif, S.; Sajid, U. Artificial intelligence for breast cancer analysis: Trends & directions. Comput. Biol. Med. 2022, 142, 105221. [Google Scholar] [CrossRef]
- Dileep, G.; Gyani, S.G.G. Artificial Intelligence in Breast Cancer Screening and Diagnosis. Cureus 2022, 14, e30318. [Google Scholar] [CrossRef]
- Shah, R.; Rosso, K.; Nathanson, S.D. Pathogenesis, prevention, diagnosis and treatment of breast cancer. World J. Clin. Oncol. 2014, 5, 283–298. [Google Scholar] [CrossRef] [Green Version]
- What Is Breast Cancer Screening?|CDC. Available online: https://www.cdc.gov/cancer/breast/basic_info/screening.htm (accessed on 3 December 2022).
- Zhang, Y.-N.; Xia, K.-R.; Li, C.-Y.; Wei, B.-L.; Zhang, B. Review of Breast Cancer Pathologigcal Image Processing. BioMed Res. Int. 2021, 2021, 1994764. [Google Scholar] [CrossRef] [PubMed]
- Maintz, J.; Viergever, M.A. A survey of medical image registration. Med Image Anal. 1998, 2, 1–36. [Google Scholar] [CrossRef] [PubMed]
- Hill, D.L.G.; Batchelor, P.G.; Holden, M.; Hawkes, D.J. Medical image registration. Phys. Med. Biol. 2001, 46, R1–R45. [Google Scholar] [CrossRef] [PubMed]
- Younis, Y.S.; Ali, A.H.; Alhafidhb, O.K.S.; Yahia, W.B.; Alazzam, M.B.; Hamad, A.A.; Meraf, Z. Early Diagnosis of Breast Cancer Using Image Processing Techniques. J. Nanomater 2022, 2022, 2641239. [Google Scholar] [CrossRef]
- Kooi, T.; Litjens, G.; van Ginneken, B.; Gubern-Mérida, A.; Sánchez, C.I.; Mann, R.; den Heeten, A.; Karssemeijer, N. Large scale deep learning for computer aided detection of mammographic lesions. Med. Image Anal. 2017, 35, 303–312. [Google Scholar] [CrossRef]
- Xue, P.; Wang, J.; Qin, D.; Yan, H.; Qu, Y.; Seery, S.; Jiang, Y.; Qiao, Y. Deep learning in image-based breast and cervical cancer detection: A systematic review and meta-analysis. NPJ Digit. Med. 2022, 5, 19. [Google Scholar] [CrossRef]
- Freeman, K.; Geppert, J.; Stinton, C.; Todkill, D.; Johnson, S.; Clarke, A.; Taylor-Phillips, S. Use of artificial intelligence for image analysis in breast cancer screening programmes: Systematic review of test accuracy. BMJ 2021, 374, n1872. [Google Scholar] [CrossRef]
- Mendes, J.; Domingues, J.; Aidos, H.; Garcia, N.; Matela, N. AI in Breast Cancer Imaging: A Survey of Different Applications. J. Imaging 2022, 8, 228. [Google Scholar] [CrossRef]
- Ozsahin, I.; Uzun Ozsahin, D. Applied Machine Learning and Multi-criteria Decision-making in Healthcare; Bentham Science Publishers: Sharjah, United Arab Emirates, 2021; ISBN 9781681088716. [Google Scholar]
- Pandey, D.; Yin, X.; Wang, H.; Su, M.-Y.; Chen, J.-H.; Wu, J.; Zhang, Y. Automatic and fast segmentation of breast region-of-interest (ROI) and density in MRIs. Heliyon 2018, 4, e01042. [Google Scholar] [CrossRef] [Green Version]
- The American Cancer Society. Available online: http://www.cancer.org (accessed on 27 May 2020).
- Chan, H.P.; Samala, R.K.; Hadjiiski, L.M. CAD and Ai for breast cancer-recent development and challenges. Br. J. Radiol. 2020, 93, 20190580. [Google Scholar] [CrossRef]
- Sadoughi, F.; Kazemy, Z.; Hamedan, F.; Owji, L.; Rahmanikatigari, M.; Azadboni, T.T. Artificial intelligence methods for the diagnosis of breast cancer by image processing: A review. Breast Cancer Targets Ther. 2018, 10, 219–230. [Google Scholar] [CrossRef] [PubMed]
- Le, E.; Wang, Y.; Huang, Y.; Hickman, S.; Gilbert, F. Artificial intelligence in breast imaging. Clin. Radiol. 2019, 74, 357–366. [Google Scholar] [CrossRef] [PubMed]
- Shao, D.; Dai, Y.; Li, N.; Cao, X.; Zhao, W.; Cheng, L.; Rong, Z.; Huang, L.; Wang, Y.; Zhao, J. Artificial intelligence in clinical research of cancers. Briefings Bioinform. 2021, 23, bbab523. [Google Scholar] [CrossRef] [PubMed]
- Tan, M.; Zheng, B.; Ramalingam, P.; Gur, D. Prediction of Near-term Breast Cancer Risk Based on Bilateral Mammographic Feature Asymmetry. Acad. Radiol. 2013, 20, 1542–1550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiu, Y.; Wang, Y.; Yan, S.; Tan, M.; Cheng, S.; Liu, H.; Zheng, B. An initial investigation on developing a new method to predict short-term breast cancer risk based on deep learning technology. Med. Imaging 2016 Comput. Aided Diagn. 2016, 9785, 978521. [Google Scholar] [CrossRef]
- Akselrod-Ballin, A.; Chorev, M.; Shoshan, Y.; Spiro, A.; Hazan, A.; Melamed, R.; Barkan, E.; Herzel, E.; Naor, S.; Karavani, E.; et al. Predicting breast cancer by applying DL to linked health records and mammograms. Radiology 2019, 292, 331–342. [Google Scholar] [CrossRef]
- Samala, R.K.; Chan, H.-P.; Hadjiiski, L.; Helvie, M.A.; Wei, J.; Cha, K. Mass detection in digital breast tomosynthesis: Deep convolutional neural network with transfer learning from mammography. Med. Phys. 2016, 43, 6654–6666. [Google Scholar] [CrossRef] [Green Version]
- Becker, A.; Marcon, M.; Ghafoor, S.; Wurnig, M.C.; Frauenfelder, T.; Boss, A. Deep Learning in Mammography. Investig. Radiol. 2017, 52, 434–440. [Google Scholar] [CrossRef]
- Kim, E.-K.; Kim, H.-E.; Han, K.; Kang, B.J.; Sohn, Y.-M.; Woo, O.H.; Lee, C.W. Applying Data-driven Imaging Biomarker in Mammography for Breast Cancer Screening: Preliminary Study. Sci. Rep. 2018, 8, 2762. [Google Scholar] [CrossRef] [Green Version]
- Sun, D.; Wang, M.; Li, A. A Multimodal Deep Neural Network for Human Breast Cancer Prognosis Prediction by Integrating Multi-Dimensional Data. IEEE/ACM Trans. Comput. Biol. Bioinform. 2018, 16, 841–850. [Google Scholar] [CrossRef]
- Muhammad, M.; Zeebaree, D.; Brifcani, A.M.A.; Saeed, J.; Zebari, D.A. Region of Interest Segmentation Based on Clustering Techniques for Breast Cancer Ultrasound Images: A Review. J. Appl. Sci. Technol. Trends 2020, 1, 78–91. [Google Scholar] [CrossRef]
- Ribli, D.; Horváth, A.; Unger, Z.; Pollner, P.; Csabai, I. Detecting and classifying lesions in mammograms with Deep Learning. Sci. Rep. 2018, 8, 4165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiao, Z.; Gao, X.; Wang, Y.; Li, J. A parasitic metric learning net for breast mass classification based on mammography. Pattern Recognit. 2018, 75, 292–301. [Google Scholar] [CrossRef]
- Chougrad, H.; Zouaki, H.; Alheyane, O. Deep Convolutional Neural Networks for breast cancer screening. Comput. Methods Programs Biomed. 2018, 157, 19–30. [Google Scholar] [CrossRef]
- Wang, H.; Feng, J.; Zhang, Z.; Su, H.; Cui, L.; He, H.; Liu, L. Breast mass classification via deeply integrating the contextual information from multi-view data. Pattern Recognit. 2018, 80, 42–52. [Google Scholar] [CrossRef]
- Lehman, C.D.; Yala, A.; Schuster, T.; Dontchos, B.; Bahl, M.; Swanson, K.; Barzilay, R. Mammographic Breast Density Assessment Using Deep Learning: Clinical Implementation. Radiology 2019, 290, 52–58. [Google Scholar] [CrossRef] [Green Version]
- Byra, M.; Galperin, M.; Ojeda-Fournier, H.; Olson, L.; O’Boyle, M.; Comstock, C.; Andre, M. Breast mass classification in sonography with transfer learning using a deep convolutional neural network and color conversion. Med. Phys. 2018, 46, 746–755. [Google Scholar] [CrossRef]
- Fujioka, T.; Kubota, K.; Mori, M.; Kikuchi, Y.; Katsuta, L.; Kasahara, M.; Oda, G.; Ishiba, T.; Nakagawa, T.; Tateishi, U. Distinction between benign and malignant breast masses at breast ultrasound using deep learning method with convolutional neural network. Jpn. J. Radiol. 2019, 37, 466–472. [Google Scholar] [CrossRef]
- Hickman, S.E.; Woitek, R.; Le, E.P.V.; Im, Y.R.; Luxhøj, C.M.; Aviles-Rivero, A.I.; Baxter, G.C.; MacKay, J.W.; Gilbert, F.J. Machine Learning for Workflow Applications in Screening Mammography: Systematic Review and Meta-Analysis. Radiology 2022, 302, 88–104. [Google Scholar] [CrossRef]
- Myers, E.R.; Moorman, P.G.; Gierisch, J.M.; Havrilesky, L.J.; Grimm, L.; Ghate, S.V.; Davidson, B.; Mongtomery, R.C.; Crowley, M.J.; McCrory, D.C.; et al. Benefits and Harms of Breast Cancer Screening. JAMA 2015, 314, 1615–1634. [Google Scholar] [CrossRef]
- Kayode, A.A.; Akande, N.O.; Adegun, A.A.; Adebiyi, M.O. An automated mammogram classification system using modified support vector machine. Med. Devices: Évid. Res. 2019, 12, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Wei, M.; Du, Y.; Wu, X.; Su, Q.; Zhu, J.; Zheng, L.; Lv, G.; Zhuang, J. A Benign and Malignant Breast Tumor Classification Method via Efficiently Combining Texture and Morphological Features on Ultrasound Images. Comput. Math. Methods Med. 2020, 2020, 5894010. [Google Scholar] [CrossRef] [PubMed]
- Dutta, K.; Roy, S.; Whitehead, T.; Luo, J.; Jha, A.; Li, S.; Quirk, J.; Shoghi, K. Deep Learning Segmentation of Triple-Negative Breast Cancer (TNBC) Patient Derived Tumor Xenograft (PDX) and Sensitivity of Radiomic Pipeline to Tumor Probability Boundary. Cancers 2021, 13, 3795. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Weng, Y.; Lund, J. Applications of Explainable Artificial Intelligence in Diagnosis and Surgery. Diagnostics 2022, 12, 237. [Google Scholar] [CrossRef]
- Roy, S.; Whitehead, T.D.; Quirk, J.D.; Salter, A.; Ademuyiwa, F.O.; Li, S.; An, H.; Shoghi, K.I. Optimal co-clinical radiomics: Sensitivity of radiomic features to tumour volume, image noise and resolution in co-clinical T1-weighted and T2-weighted magnetic resonance imaging. Ebiomedicine 2020, 59, 102963. [Google Scholar] [CrossRef]
- Roy, S.; Whitehead, T.D.; Li, S.; Ademuyiwa, F.O.; Wahl, R.L.; Dehdashti, F.; Shoghi, K.I. Co-clinical FDG-PET radiomic signature in predicting response to neoadjuvant chemotherapy in triple-negative breast cancer. Eur. J. Nucl. Med. 2021, 49, 550–562. [Google Scholar] [CrossRef]
- Lambin, P.; Leijenaar, R.T.H.; Deist, T.M.; Peerlings, J.; de Jong, E.E.C.; van Timmeren, J.; Sanduleanu, S.; Larue, R.T.H.M.; Even, A.J.G.; Jochems, A.; et al. Radiomics: The bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef] [Green Version]
- Liang, W.; Yang, P.; Huang, R.; Xu, L.; Wang, J.; Liu, W.; Zhang, L.; Wan, D.; Huang, Q.; Lu, Y.; et al. A Combined Nomogram Model to Preoperatively Predict Histologic Grade in Pancreatic Neuroendocrine Tumors. Clin. Cancer Res. 2019, 25, 584–594. [Google Scholar] [CrossRef] [Green Version]
- Park, H.; Lim, Y.; Ko, E.S.; Cho, H.-H.; Lee, J.E.; Han, B.-K.; Choi, J.S.; Park, K.W. Radiomics Signature on Magnetic Resonance Imaging: Association with Disease-Free Survival in Patients with Invasive Breast Cancer. Clin. Cancer Res. 2018, 24, 4705–4714. [Google Scholar] [CrossRef] [Green Version]
- Understanding Reproducibility and Replicability—Reproducibility, and Replicability in Science—NCBI Bookshelf. Available online: https://www.ncbi.nlm.nih.gov/books/NBK547546/ (accessed on 13 December 2022).
- Kukull, W.A.; Ganguli, M. Generalizability: The trees, the forest, and the low-hanging fruit. Neurology 2012, 78, 1886–1891. [Google Scholar] [CrossRef] [Green Version]
- Duwa, B.B.; Ozsoz, M.; Al-Turjman, F. Applications of AI, IoT, IoMT, and Biosensing Devices in Curbing COVID-19. In AI-Powered IoT for COVID-19; CRC Press: Boca Raton, FL, USA, 2020; pp. 141–158. [Google Scholar] [CrossRef]
- Ibrahim, A.U.; Ozsoz, M.; Al-Turjman, F.; Coston, P.P.; Duwa, B.B. How Artificial Intelligence and IoT Aid in Fighting COVID-19. In AI-Powered IoT for COVID-19; CRC Press: Boca Raton, FL, USA, 2020; pp. 159–168. [Google Scholar] [CrossRef]
- World Health Organization. WHO Position Paper on Mammography Screening; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Lei, Y.-M.; Yin, M.; Yu, M.-H.; Yu, J.; Zeng, S.-E.; Lv, W.-Z.; Li, J.; Ye, H.-R.; Cui, X.-W.; Dietrich, C.F. Artificial Intelligence in Medical Imaging of the Breast. Front. Oncol. 2021, 11, 2892. [Google Scholar] [CrossRef] [PubMed]
- Tsantekidis, A.; Passalis, N.; Tefas, A. Deep Reinforcement Learning; McGraw-Hill: New York, NY, USA, 2022; pp. 117–129. [Google Scholar] [CrossRef]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Summers, R.M. Machine learning and radiology. Med. Image Anal. 2012, 16, 933–951. [Google Scholar] [CrossRef] [Green Version]
- Zhavoronkov, A. Artificial Intelligence for Drug Discovery, Biomarker Development, and Generation of Novel Chemistry. Mol. Pharm. 2018, 15, 4311–4313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roy, S.; Meena, T.; Lim, S.-J. Demystifying Supervised Learning in Healthcare 4.0: A New Reality of Transforming Diagnostic Medicine. Diagnostics 2022, 12, 2549. [Google Scholar] [CrossRef] [PubMed]
- Schölkopf, B.; Platt, J.; Hofmann, T. Greedy layer-wise training of deep networks. ” Adv. Neural. Inf. Process Syst. 2007, 19, 153–160. [Google Scholar]
- Ligthart, A.; Catal, C.; Tekinerdogan, B. Analyzing the effectiveness of semi-supervised learning approaches for opinion spam classification. Appl. Soft Comput. 2020, 101, 107023. [Google Scholar] [CrossRef]
- Ozsahin, D.U.; Sheshakli, S.; Kibarer, A.G.; Denker, A.; Duwa, B.B. Analysis of early stage breast cancer treatment techniques. Appl. Multi-Criteria Decis.-Mak. Theor. Healthc. Biomed. Eng. 2021, 71–80. [Google Scholar] [CrossRef]
- George, K.; Faziludeen, S.; Sankaran, P. Breast cancer detection from biopsy images using nucleus guided transfer learning and belief based fusion. Comput. Biol. Med. 2020, 124, 103954. [Google Scholar] [CrossRef]
- Talo, M. Automated classification of histopathology images using transfer learning. Artif. Intell. Med. 2019, 101, 101743. [Google Scholar] [CrossRef] [Green Version]
- Yuan, J.; Hu, Z.; Mahal, B.A.; Zhao, S.D.; Kensler, K.H.; Pi, J.; Hu, X.; Zhang, Y.; Wang, Y.; Jiang, J.; et al. Integrated Analysis of Genetic Ancestry and Genomic Alterations across Cancers. Cancer Cell 2018, 34, 549–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tagliafico, A.S.; Piana, M.; Schenone, D.; Lai, R.; Massone, A.M.; Houssami, N. Overview of radiomics in breast cancer diagnosis and prognostication. Breast 2019, 49, 74–80. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author’s Name | Year | Title | Summary of Result |
|---|---|---|---|
| Kooi et al. [52] | 2017 | The advantages of Large-scale DL for CAD of breast lesions | The result showed that CNN performs better than CAD in a low sensitivity when compared. |
| Pandey et al. [57] | 2018 | The systematic and rapid segmentation of the region of interest (ROI) and breast density in MRI | The pictorial-based analysis displayed excellent segmentation in terms of accuracy, specificity, AUC, and sensitivity |
| Sadoughi et al. [60] | 2018 | AI methodology in the diagnosis of BC | The result showed that SVM has the highest accuracy (100%) when compared with various images from thermographs (99.85%), mammograms (93.69%), and ultrasound (US) (95.85%) |
| Le et al. [61] | 2019 | The use of AI in breast imaging | The transition from the traditional rule-based CAD to an enhanced embedded knowledge that reduces diagnostic error and improves radiologist accuracy. |
| Huang et al. [32] | 2020 | AI in BC, prognosis, and diagnosis | The challenges of cancer prognosis and diagnosis are dealt with using advances in AI |
| H-p et al. [59] | 2020 | Combination of AI and CAD in BC. Recent advancements and difficulties | DL employed in clinical image datasets combined with CAD provides a novelty workflow in clinical practice |
| Shah et al. [44] | 2021 | AI in detecting BC | AI showed higher diagnostic accuracy than CAD in the detection of BC in mammogram |
| Freeman et al. [54] | 2021 | Utilization of AI for image analysis in BC screening initiatives: a comprehensive assessment of the diagnostic validity | In the 3 studies, AI detects 53%, 45%, and 50% of low-risk cancer. In addition, AI detects 10%, 4%, and 0% BC data from the already screened data set used by radiologists. |
| Utilization of AI for image analysis in BC screening initiatives: a comprehensive assessment of the diagnostic validity | |||
| Shah et al. [44] | 2022 | Trend and direction in the application of AI in the diagnosis of BC | The availability of the data set makes it possible for AI to be applied using image modalities to the mammogram. |
| Nassif et al. [58] | 2022 | The use of AI BC detection | Images from histopathological BC examinations are less expensive and very common, therefor they are used in DL BC detection |
| Dileep and Gianchandani Gyani [45] | 2022 | AI application in BC screening and diagnosis | Incorporation of AI into different screening methodologies to detect breast mass, density, and segmentation. |
| Shao et al. [62] | 2022 | The application of AI to the clinical study of BC | The AI was able to classify BC according to the many kinds of data, such as plain radiographs, cancer genes, health records, pharmacological information, and biological works of literature. |
| Mendes et al. [55] | 2022 | An Overview of the Role of AI in Imaging analysis of BC and Its Various Applications | AI application in BC images using ML, DL to predict the risk of cancer, mammogram evaluation, and labeling of data set, AI showed an overview of the advantages and challenges including the potential solution during the BC imaging survey |
| Reference | Date | Task | Country | Tumor Type | Model Source | No Images/Studies | Type of Model | Size of Input/Training | Independent Test Set | Performance Validation | The Area under the Curve (AUC) | Sensitivity (%) | Specificity (%) | Accuracy (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Tan et al. [63] | 2013 | SVM classifier | USA | Breast mammogram | Gaussian kernel | 994 women | Gaussian kernel | 349 benign, 362 cancerous | NA | NA | 0.73 | NA | NA | NA |
| Qiu et al. [64] | 2016 | Classification | USA | breast | CNN | 270 | CNN, CAD | 200 cases, 70 cases | NA | NA | 0.70 | 70 | 60 | 71.4 |
| Ayelet Akselrod-Ballin [65] | 2016 | DL | Canada | Histopathologica + mammography | R-CNN | 52,936 | In house Lab | 9611 | NA | 1055 | 0.72 | 87.0 | 77.3 | 91.0 |
| Samala et al. [66] | 2016 | mass detection and classification | USA | Mammography + X-ray | SFM and DM | 28,330 | Cuda- convNet | 28,330 | 94 | NA | 0.81 | 83.0 | 91.0 | NA |
| Becker A, [67] | 2017 | Classification | Switzerland | Fibro glandular volumetric breast density. | Quantra 2.2 | 510,000 | ANN + Volpara Density | Group 1 = 95/95, Group 2 = 83/513 | NA | NA | 0.79 | 78.0 | 84.0 | 81.0 |
| Kim E.et al. [68] | 2018 | Testing ANNs | South Korea | Breast | DIB-MG mammography | 29,107 | ANN | 18 cancers and 233 controls | NA | NA | 0.99 | 73.7 versus 66.6 | 72.0 versus 92.7 | NA |
| Sun et al. [69] | 2018 | Multimodal DNN | China | Breast cancer | Metabric | 1980 | DNN | 1054 | NA | NA | 8.40 | 95 | 99 | 2.4 |
| Mohammed et al. [70] | 2018 | classification | Iraq | Ultrasound Breast Images | OI + ANN classifier | 1393 | ANN classifier | 900. 300 | NA | NA | NA | 79.4 | 84.76 | 82.0 |
| Ribli D. et al. [71] | 2018 | classification | Hungary | Mammograms | CNN | 86,000 | CNN | 7700, 847 | NA | NA | 0.85 | 98.7 | 99.6 | 98.7 |
| Jiao et al. [72] | 2018 | Alex Net + ImageNet | China | DL Classification | DDSM 300 images | 300 | DDSM + MIAS set | 300 | 150 | 150 | NA | NA | NA | DDSM = 97.4 MIAS = 96.7 |
| Chougrad et al. [73] | 2018 | Comparative image classification | Morroco | Mammography + X-ray | DDSM, INbreast, BCDR | 6116 | DDSM, INbreast, BCDR | 641, 688DDSM 300.300INbreast 344,300BCDR | 113 | NA | 0.99 | NA | NA | 98.2 |
| Wang H et al. [74] | 2018 | classification | China | Mammography | MV DCNN | 736 | MV-DNN, + MAP | 368 | 295 | 74 | DNN = 0.828, MAP = 0.846 | NA | NA | NA |
| Lehman et al. [75] | 2019 | Breast segment classification | USA | Breast density | DMs + ResNet18 | 27,684 | Pretrained ResNet18 | 27,684 | 5741 + 1076 | 8738 | Kappa = 0.67 | NA | NA | 77 |
| Byra et al. [76] | 2019 | Classification of Breast US | USA | Breast US | INbreastes | 582 | AUC (VGG19 + FT + ML) | 582 | 150 | 150 | 0.936 | NA | NA | NA |
| Fujioka et al. [77] | 2019 | Breast mass segmentation | Japan | Breast US | DCNN | 947 | DCNN | 480 benign, 467 cancerous | NA | NA | 0.913 | NA | NA | NA |
| E.P.V Le [78] | 2019 | classification | Uk | Breast imaging | iCAD’s Detection + ScreenPoint MedicalTranspara | 640,000 | CNN + DREAM Challenge | 318,000 | NA | NA | 0.91 0.76 | 84.0 | 91 [79] | NA |
| Kayode et al. [80] | 2019 | SVM classifier | Nigeria | Breast | GLCM | 322 | Texture Feature + SVM | 126 Normal, 60 benign, 48 malignant | NA | NA | NA | 94.5 | 91.3 | NA |
| Tomoyuki Fujioka, Kazunori Kubota et al. [77] | 2019 | Classification | Japan | Breast tumor | CNN | 1536 | CNN + Res152 | 897 malig, 639 benign | NA | NA | 0.951 | 90.9 | 87.0 | NA |
| Wei M [81] | 2020 | Classification | China | Breast tumor | Radial Range Spectrum + GLCM | 1061 | SVM classifier | 589 malignant, 472 benign | NA | NA | 0.93 | 87.0 | 87.6 | 87.3 |
| Tomoyuki Fujioka, Kazunori Kubota et al. [77] | 2020 | Differentiation | Japan | Breast cancer | CNN | 576.6 | CNN | 48 benign, 72 malignant | NA | NA | 0.93, 0.73, 0.85 | 95.8, 58.3, 91.7 | 92.5 60.4 77.1 | 92.5 65.8 79.2 |
| Reference | Country | Topic | Aim | Methods Used | Result | Limitation |
|---|---|---|---|---|---|---|
| Dutta et al., 2021 [82] | USA | The classification of Triple-Negative Breast Cancer (TNBC) using DL methodology on Patient Derived Tumor Xenograft (PDX) and Tumor Probability Boundary Sensitivity of Radiomic Pipeline | DL is used in the automated pathway for the detection and quantification of TNBC PDX tumors from nonclinical weighted (T1W) images and weighted images (T2WI) of M RI | Manual comparison of delineation with U-Net, dense U-Net, Res-Net, recurrent residual U-Net (R2UNet), and dense R2U-Net | The compared networks had a score ranging between 1% and 3% | Time intensive. Variations in the results of repeated measurements cannot be reproduced. |
| Zhang et al., 2022 [83] | UK | Diagnostic and Surgical Applications of AI that Can Be interpreted or explained | Overcome AI’s explainable or interpreted (XAI) black box identity | Literary search from databases between 2019 to 2021 | XAI is heading in several interesting directions. | Black box identity of some of the AI models |
| Roy et al., 2020 [84] | USA | Radiomic characteristics and resolution clinical weighted (T1W) image and weighted image (T2WI) from MRI | Radiomics characteristics were used in a combined clinical trial. | The study uses TNBC patients | Sixteen volume-dependent characteristics of radiomics were identified | Models used are genetically engineered PDXs are also used. |
| Roy et al., 2022 [85] | USA | Predicting response to neoadjuvant in TNBC by using a co-clinical FDG-PET (RadSig) radiomic signature | Optimization and identification of radiometric characteristics and therapeutic response | The study uses TNBC patients as well as PDXs | NB-RadSig has the highest prediction and therapeutic response. | SVM-RadSig NB-RadSig superior to Standardized uptake values of mean, maximum, and peak |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uzun Ozsahin, D.; Ikechukwu Emegano, D.; Uzun, B.; Ozsahin, I. The Systematic Review of Artificial Intelligence Applications in Breast Cancer Diagnosis. Diagnostics 2023, 13, 45. https://doi.org/10.3390/diagnostics13010045
Uzun Ozsahin D, Ikechukwu Emegano D, Uzun B, Ozsahin I. The Systematic Review of Artificial Intelligence Applications in Breast Cancer Diagnosis. Diagnostics. 2023; 13(1):45. https://doi.org/10.3390/diagnostics13010045
Chicago/Turabian StyleUzun Ozsahin, Dilber, Declan Ikechukwu Emegano, Berna Uzun, and Ilker Ozsahin. 2023. "The Systematic Review of Artificial Intelligence Applications in Breast Cancer Diagnosis" Diagnostics 13, no. 1: 45. https://doi.org/10.3390/diagnostics13010045