
The Association between Diabetes Mellitus, High Monocyte/Lymphocyte Ratio, and Survival in Endometrial Cancer: A Retrospective Cohort Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
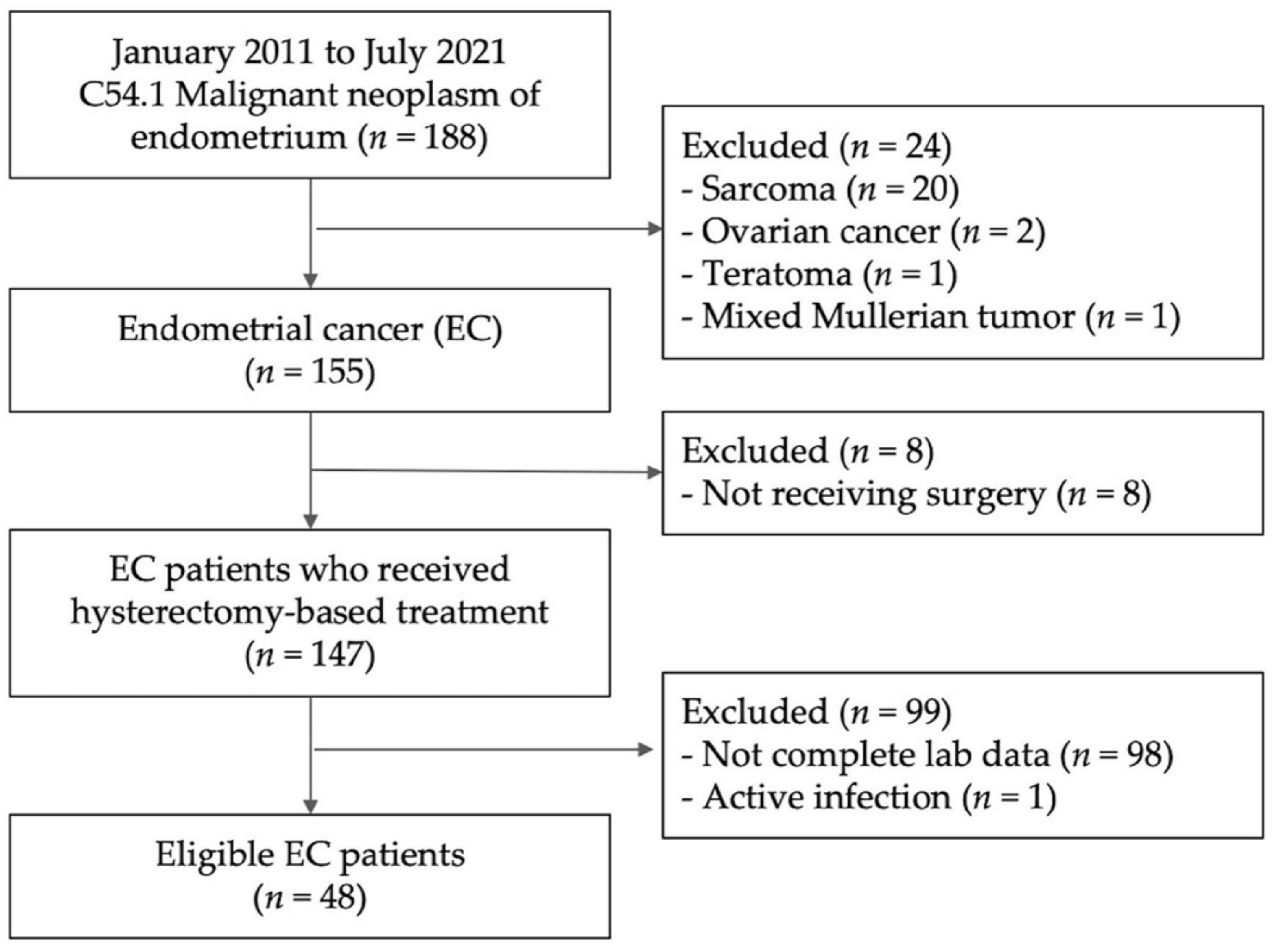
2.2. Study Population
2.3. Data Collection
2.4. MLR, NLR and PLR Calculation
2.5. Statistical Analysis
3. Results
3.1. Demographics
3.2. Cox Regression Analysis of the Factors Associated with Mortality
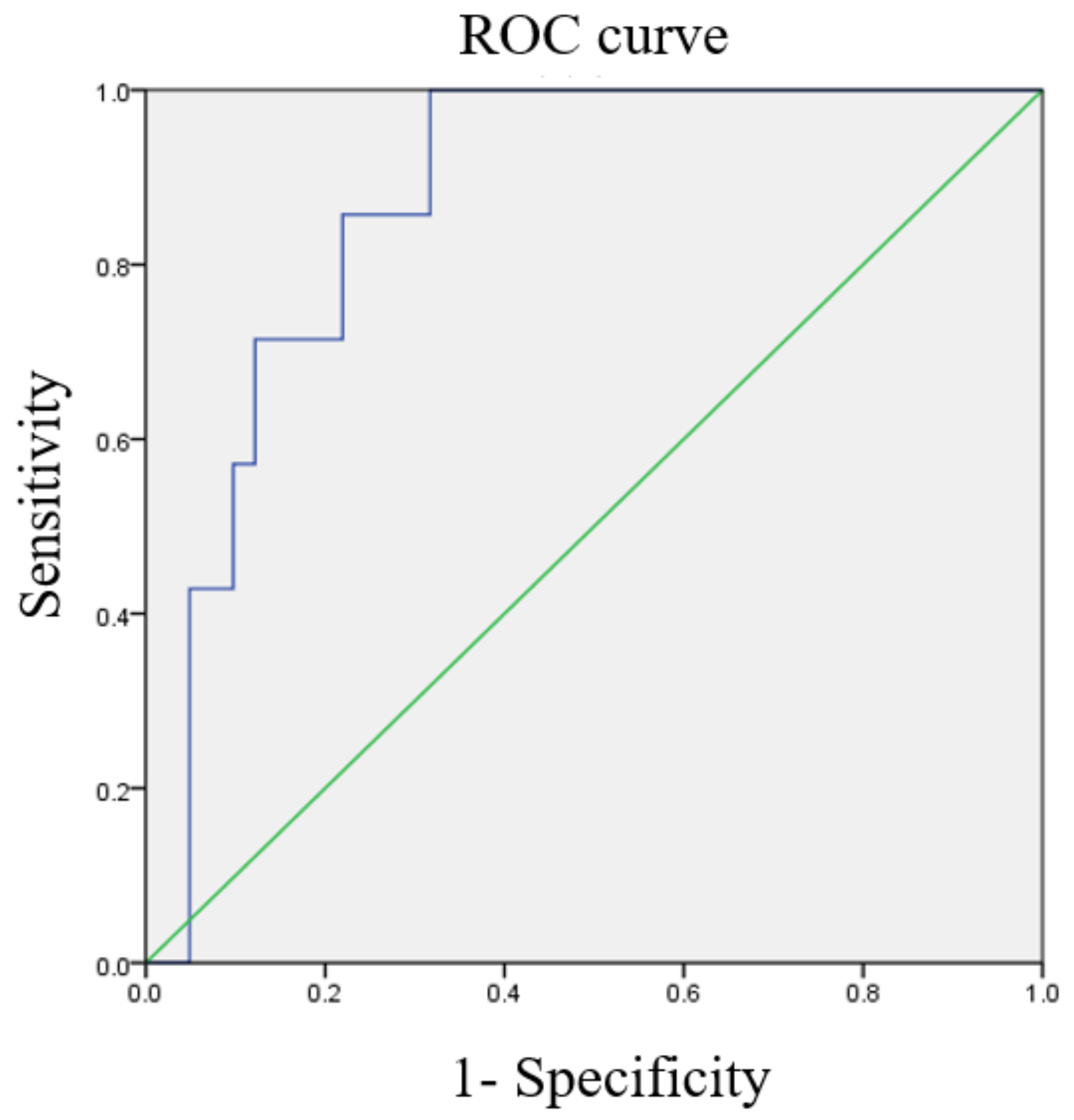
3.3. ROC Curves of Various Ratios
3.4. Comparative Characteristics of High and Low NLR/MLR/PLR Groups
3.5. OS and PFS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Clarke, M.A.; Long, B.J.; Del Mar Morillo, A.; Arbyn, M.; Bakkum-Gamez, J.N.; Wentzensen, N. Association of endometrial cancer risk with postmenopausal bleeding in women: A systematic review and meta-analysis. JAMA Intern. Med. 2018, 178, 1210–1222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morice, P.; Leary, A.; Creutzberg, C.; Abu-Rustum, N.; Darai, E. Endometrial cancer. Lancet 2016, 387, 1094–1108. [Google Scholar] [CrossRef] [PubMed]
- Sonoda, Y. Surgical treatment for apparent early stage endometrial cancer. Obstet. Gynecol. Sci. 2014, 57, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bestvina, C.M.; Fleming, G.F. Chemotherapy for endometrial cancer in adjuvant and advanced disease settings. Oncologist 2016, 21, 1250–1259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorusso, V.; Vallarelli, S.; Giotta, F. Adjuvant therapy of endometrial cancer: “Taxane or not taxane, this is the question”. Transl. Cancer Res. 2019, 8, 2220–2222. [Google Scholar] [CrossRef] [PubMed]
- Yoriki, K.; Mori, T.; Kokabu, T.; Matsushima, H.; Umemura, S.; Tarumi, Y.; Kitawaki, J. Estrogen-related receptor alpha induces epithelial-mesenchymal transition through cancer-stromal interactions in endometrial cancer. Sci. Rep. 2019, 9, 6697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasius, J.C.; Pijnenborg, J.M.A.; Lindemann, K.; Forsse, D.; van Zwol, J.; Kristensen, G.B.; Krakstad, C.; Werner, H.M.J.; Amant, F. Risk stratification of endometrial cancer patients: FIGO stage, biomarkers and molecular classification. Cancers 2021, 13, 5848. [Google Scholar] [CrossRef]
- Sabater, S.; Andres, I.; Lopez-Honrubia, V.; Marti-Laosa, M.M.; Castro-Larefors, S.; Berenguer, R.; Jimenez-Jimenez, E.; Sevillano, M.; Rovirosa, A.; Arenas, M. Does postoperative irradiation improve survival in early-stage endometrial cancer? Brachytherapy 2018, 17, 912–921. [Google Scholar] [CrossRef]
- Chen, Y.; Zhao, W.; Bi, F.; Pan, X.; Yin, L.; Zhao, C. Significance of TP53 mutational status-associated signature in the progression and prognosis of endometrial carcinoma. Oxid. Med. Cell. Longev. 2022, 2022, 1817339. [Google Scholar] [CrossRef]
- Han, L.N.; Han, Y.W.; Yan, P. Prognostic values of human epididymis Protein 4 expression in patients with endometrial cancer: A systematic review and meta-analysis. J. Obstet. Gynaecol. Res. 2022, 48, 2255–2269. [Google Scholar] [CrossRef]
- Jakubowska, K.; Koda, M.; Grudzińska, M.; Kańczuga-Koda, L.; Famulski, W. Monocyte-to-lymphocyte ratio as a prognostic factor in peripheral whole blood samples of colorectal cancer patients. World J. Gastroenterol. 2020, 26, 4639–4655. [Google Scholar] [CrossRef] [PubMed]
- Gong, J.; Jiang, H.; Shu, C.; Hu, M.Q.; Huang, Y.; Liu, Q.; Li, R.F. Prognostic value of lymphocyte-to-monocyte ratio in ovarian cancer: A meta-analysis. J. Ovarian Res. 2019, 12, 51. [Google Scholar] [CrossRef] [PubMed]
- Gao, F.; Hu, J.; Zhang, J.; Xu, Y. Prognostic value of peripheral blood lymphocyte/monocyte ratio in lymphoma. J. Cancer 2021, 12, 3407–3417. [Google Scholar] [CrossRef] [PubMed]
- Eo, W.K.; Kwon, S.; Koh, S.B.; Kim, M.J.; Ji, Y.I.; Lee, J.Y.; Suh, D.S.; Kim, K.H.; Kim, H.Y. The lymphocyte-monocyte ratio predicts patient survival and aggressiveness of endometrial cancer. J. Cancer 2016, 7, 538–545. [Google Scholar] [CrossRef] [Green Version]
- Njoku, K.; Agnew, H.J.; Crosbie, E.J. Impact of type 2 diabetes mellitus on endometrial cancer survival: A prospective database analysis. Front. Oncol. 2022, 12, 899262. [Google Scholar] [CrossRef]
- Gawiński, C.; Michalski, W.; Mróz, A.; Wyrwicz, L. Correlation between lymphocyte-to-monocyte ratio (LMR), neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR) and tumor-infiltrating lymphocytes (TILs) in left-sided colorectal cancer patients. Biology 2022, 11, 385. [Google Scholar] [CrossRef]
- Cheng, H.R.; Song, J.Y.; Zhang, Y.N.; Chen, Y.B.; Lin, G.Q.; Huang, G.Q.; He, J.C.; Wang, Z. High monocyte-to-lymphocyte ratio is associated with stroke-associated pneumonia. Front. Neurol. 2020, 11, 575809. [Google Scholar] [CrossRef]
- Stotz, M.; Szkandera, J.; Stojakovic, T.; Seidel, J.; Samonigg, H.; Kornprat, P.; Schaberl-Moser, R.; Seggewies, F.; Hoefler, G.; Gerger, A.; et al. The lymphocyte to monocyte ratio in peripheral blood represents a novel prognostic marker in patients with pancreatic cancer. Clin. Chem. Lab. Med. 2015, 53, 499–506. [Google Scholar] [CrossRef]
- Huang, H.; Li, L.; Luo, W.; Yang, Y.; Ni, Y.; Song, T.; Zhu, Y.; Yang, Y.; Zhang, L. Lymphocyte percentage as a valuable predictor of prognosis in lung cancer. J. Cell. Mol. Med. 2022, 26, 1918–1931. [Google Scholar] [CrossRef]
- Tsukumo, S.I.; Yasutomo, K. Regulation of CD8+ T cells and antitumor immunity by Notch signaling. Front. Immunol. 2018, 9, 101. [Google Scholar] [CrossRef]
- Takeuchi, A.; Saito, T. CD4 CTL, a cytotoxic subset of CD4+ T cells, their differentiation and function. Front. Immunol. 2017, 8, 194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coico, R. Immunology: A Short Course; John Wiley & Sons: Hoboken, NJ, USA, 2021; ISBN 9781119551577. [Google Scholar]
- Geissmann, F.; Manz, M.G.; Jung, S.; Sieweke, M.H.; Merad, M.; Ley, K. Development of monocytes, macrophages, and dendritic cells. Science 2010, 327, 656–661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Q.; Guo, N.; Zhou, Y.; Chen, J.; Wei, Q.; Han, M. The role of tumor-associated macrophages (TAMs) in tumor progression and relevant advance in targeted therapy. Acta Pharm. Sin. B 2020, 10, 2156–2170. [Google Scholar] [CrossRef] [PubMed]
- Cong, R.; Kong, F.; Ma, J.; Li, Q.; Wu, Q.; Ma, X. Combination of preoperative neutrophil-lymphocyte ratio, platelet-lymphocyte ratio and monocyte-lymphocyte ratio: A superior prognostic factor of endometrial cancer. BMC Cancer 2020, 20, 464. [Google Scholar] [CrossRef] [PubMed]
- Song, H.; Jeong, M.J.; Cha, J.; Lee, J.S.; Yoo, J.G.; Song, M.J.; Kim, J.H.; Lee, S.J.; Lee, H.N.; Yoon, J.H.; et al. Preoperative neutrophil-to-lymphocyte, platelet-to-lymphocyte and monocyte-to-lymphocyte ratio as a prognostic factor in non-endometrioid endometrial cancer. Int. J. Med. Sci. 2021, 18, 3712–3717. [Google Scholar] [CrossRef] [PubMed]
- Holub, K.; Busato, F.; Gouy, S.; Sun, R.; Pautier, P.; Genestie, C.; Morice, P.; Leary, A.; Deutsch, E.; Haie-Meder, C.; et al. Analysis of systemic inflammatory factors and survival outcomes in endometrial cancer patients staged I-III FIGO and treated with postoperative external radiotherapy. J. Clin. Med. 2020, 9, 1441. [Google Scholar] [CrossRef]
- Leng, J.; Wu, F.; Zhang, L. Prognostic significance of pretreatment neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, or monocyte-to-lymphocyte ratio in endometrial neoplasms: A systematic review and meta-analysis. Front. Oncol. 2022, 12, 734948. [Google Scholar] [CrossRef]
- Luo, J.; Beresford, S.; Chen, C.; Chlebowski, R.; Garcia, L.; Kuller, L.; Regier, M.; Wactawski-Wende, J.; Margolis, K.L. Association between diabetes, diabetes treatment and risk of developing endometrial cancer. Br. J. Cancer 2014, 111, 1432–1439. [Google Scholar] [CrossRef] [Green Version]
- Chu, D.; Wu, J.; Wang, K.; Zhao, M.; Wang, C.; Li, L.; Guo, R. Effect of Metformin Use on the Risk and Prognosis of Endometrial Cancer: A Systematic Review and Meta-Analysis. BMC Cancer 2018, 18, 438. [Google Scholar] [CrossRef] [Green Version]
- Zhu, L.; Sun, X.; Bai, W. Nomograms for predicting cancer-specific and overall survival among patients with endometrial carcinoma: A SEER based study. Front. Oncol. 2020, 10, 269. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Death | Total | p-Value | ||
|---|---|---|---|---|
| No | Yes | |||
| N | 41 | 7 | 48 | |
| Age | 55.95 ± 8.83 | 61.57 ± 7.32 | 56.77 ± 8.79 | 0.119 |
| BMI | 28.38 ± 5.13 | 30.97 ± 4.30 | 28.76 ± 5.06 | 0.215 |
| DM (%) | 11 (26.8%) | 5 (71.4%) | 16 (33.3%) | 0.033 * |
| Hypertension (%) | 23 (56.1%) | 4 (57.1%) | 27 (56.3%) | 1.000 |
| Stage (%) | - | - | - | 0.288 |
| 1 | 28 (68.3%) | 3 (42.9%) | 31 (64.6%) | |
| 2 | 5 (12.2%) | 1 (14.3%) | 6 (12.5%) | |
| 3 | 5 (12.2%) | 2 (28.6%) | 7 (14.6%) | |
| 4 | 3 (7.3%) | 1 (14.3%) | 4 (8.3%) | |
| Histology subtype (%) | - | - | - | 0.684 |
| Mixed cell carcinoma | 4 (9.8%) | 1 (14.3%) | 5 (10.4%) | |
| Endometrioid | 32 (78.0%) | 5 (71.4%) | 37 (77.0%) | |
| Serous carcinoma | 4 (9.8%) | 1 (14.3%) | 5 (10.4%) | |
| Clear cell carcinoma | 1 (2.4%) | 0 (0.0%) | 1 (2.1%) | |
| Tumor grade (%) N = 48 | - | - | - | 0.875 |
| 1 | 21 (51.2%) | 4 (57.1%) | 25 (52.1%) | |
| 2 | 9 (22.0%) | 1 (14.3%) | 10 (20.8%) | |
| 3 | 11 (26.8%) | 2 (28.6%) | 13 (27.1%) | |
| Immunohistochemistry | ||||
| ER | 0.363 | |||
| 0 | 6 (14.6%) | 2 (28.6%) | 8 (16.7%) | |
| 1+ | 11 (26.8%) | 3 (42.9%) | 14 (29.2%) | |
| 2+ | 11 (26.8%) | 0 (0.0%) | 11 (22.9%) | |
| 3+ | 13 (31.7%) | 2 (28.6%) | 15 (31.1%) | |
| PR N = 46 | 0.681 | |||
| 0 | 5 (13.8%) | 1 (14.3%) | 6 (13.0%) | |
| 1+ | 8 (20.5%) | 3 (42.9%) | 11 (23.9%) | |
| 2+ | 10 (25.6%) | 1 (14.3%) | 11 (23.9%) | |
| 3+ | 14 (41.0%) | 2 (28.6%) | 18 (39.1%) | |
| Lymphovascular invasion (%) N = 47 | 19 (47.5%) | 5 (71.4%) | 24 (51.1%) | 0.416 |
| LN invasion (%) N = 41 | 6 (17.1%) | 2 (33.3%) | 8 (19.5%) | 0.578 |
| NLR | 3.04 ± 3.10 | 5.23 ± 2.68 | 3.36 ± 3.11 | 0.085 |
| MLR | 0.21 ± 0.15 | 0.36 ± 0.15 | 0.23 ± 0.16 | 0.018 * |
| PLR | 174.14 ± 123.41 | 191.47 ± 92.19 | 176.67 ± 118.68 | 0.725 |
| Crude | Adjusted (Model 1) | Adjusted (Model 2) | ||||
|---|---|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Age | 1.12 (0.99, 1.27) | 0.073 | 1.02 (0.88, 1.19) | 0.780 | 1.04 (0.90, 1.20) | 0.636 |
| BMI | 1.12 (0.96, 1.30) | 0.145 | ||||
| DM (Yes vs. No) | 11.89 (1.39, 102.02) | 0.024 * | 21.54 (1.34, 344.93) | 0.030 * | 8.27 (0.81, 84.25) | 0.074 |
| NLR > 3.0995 | 274.63 (0.06, 1,236,601.52) | 0.191 | ||||
| MLR > 0.2386 | 10.87 (1.30, 90.83) | 0.028 * | 16.05 (0.9, 286.66) | 0.059 | 8.88 (1.03, 76.28) | 0.046 * |
| PLR > 154.3309 | 3.34 (0.65, 17.24) | 0.150 | ||||
| Stage | - | - | - | - | ||
| 1 | Reference | NA | Reference | NA | ||
| 2 | 0.99 (0.09, 10.88) | 0.993 | 19.78 (0.66, 590.95) | 0.085 | ||
| 3 | 4.72 (0.75, 29.76) | 0.098 | 2.16 (0.24, 19.29) | 0.489 | ||
| 4 | 3.66 (0.36, 36.82) | 0.270 | 3.19 (0.25, 41.03) | 0.373 | ||
| Histology | - | - | ||||
| Mixed cell carcinoma | Reference | NA | ||||
| Endometrioid | 0.43 (0.05, 3.86) | 0.451 | ||||
| Serous carcinoma | 0.85 (0.05, 13.68) | 0.910 | ||||
| Clear cell carcinoma | 0.00 (NA) | 0.991 | ||||
| Tumor grade | - | - | ||||
| 1 | Reference | NA | ||||
| 2 | 1.05 (0.19, 5.89) | 0.957 | ||||
| 3 | 0.56 (0.06, 5.08) | 0.605 | ||||
| ER | - | - | ||||
| 0 | References | NA | ||||
| 1+ | 0.43 (0.05, 3.86) | 0.451 | ||||
| 2+ | 0.85 (0.05, 13.86) | 0.910 | ||||
| 3+ | 0.85 (0.05, 13.68) | 0.991 | ||||
| PR N = 46 | - | - | ||||
| 0 | References | NA | ||||
| 1+ | 1.33 (0.14, 12.99) | 0.808 | ||||
| 2+ | 0.41 (0.03, 6.61) | 0.520 | ||||
| 3+ | 0.27 (0.02, 4.43) | 0.361 | ||||
| Lymphovascular invasion (Yes vs. No) | 1.52 (0.28, 8.43) | 0.630 | ||||
| LN invasion (Yes vs. No) | 3.23 (0.53, 19.52) | 0.202 | ||||
| Characteristic | NLR-Low | NLR-High | p-Value | MLR-Low | MLR-High | p-Value | PLR-Low | PLR-High | p-Value |
|---|---|---|---|---|---|---|---|---|---|
| N | 33 | 15 | 31 | 17 | 28 | 20 | |||
| Age | 55.39 ± 9.39 | 59.80 ± 6.59 | 0.108 | 55.61 ± 9.75 | 58.88 ± 6.41 | 0.221 | 55.57 ± 9.47 | 58.45 ± 7.65 | 0.268 |
| BMI | 28.61 ± 5.38 | 29.09 ± 4.40 | 0.767 | 28.16 ± 5.03 | 29.85 ± 5.08 | 0.271 | 29.14 ± 4.87 | 28.23 ± 5.38 | 0.543 |
| DM (%) | 7 (21.2%) | 9 (60.0%) | 0.008 * | 9 (29.0%) | 7 (41.2%) | 0.393 | 8 (28.6%) | 8 (40.0%) | 0.408 |
| Stage (%) | 0.037 * | 0.002 * | 0.244 | ||||||
| 1 | 25 (75.8%) | 6 (40.0%) | 24 (77.4%) | 7 (41.2%) | 21 (75.0%) | 10 (50.0%) | |||
| 2 | 4 (12.1%) | 2 (13.3%) | 5 (16.1%) | 1 (5.9%) | 3 (10.7%) | 3 (15.0%) | |||
| 3 | 3 (9.1%) | 4 (26.7%) | 2 (6.5%) | 5 (29.4%) | 2 (7.1%) | 5 (25.0%) | |||
| 4 | 1 (3.0%) | 3 (20.0%) | 0 (0.0%) | 4 (23.5%) | 2 (7.1%) | 2 (10.0%) | |||
| Histology (%) | 0.096 | 0.018 * | 0.175 | ||||||
| Mixed cell carcinoma | 3 (9.1%) | 2 (13.3%) | 2 (6.5%) | 3 (17.6%) | 3 (10.7%) | 2 (10.0%) | |||
| Endometrioid | 28 (84.8%) | 9 (60.0%) | 28 (90.3%) | 9 (52.9%) | 24 (85.7%) | 13 (65.0%) | |||
| Serious carcinoma | 1 (3.0%) | 4 (26.7%) | 1 (3.2%) | 4 (23.5%) | 1 (3.6%) | 4 (20.0%) | |||
| Clear cell carcinoma | 1 (3.0%) | 0 (0.0%) | 0 (0.0%) | 1 (5.9%) | 0 (0.0%) | 1 (5.0%) | |||
| ER | 1.000 | 0.974 | 0.271 | ||||||
| 0 | 5 (15.2%) | 3 (20.0%) | 5 (16.1%) | 3 (17.6%) | 3 (10.7%) | 5 (25.0%) | |||
| 1+ | 10 (30.3%) | 4 (26.7%) | 9 (29.0%) | 5 (29.4%) | 8 (28.6%) | 6 (20.0%) | |||
| 2+ | 8 (24.2%) | 3 (20.0%) | 8 (25.8%) | 3 (17.6%) | 9 (32.1%) | 2 (10.0%) | |||
| 3+ | 10 (30.0%) | 5 (33.3%) | 9 (29.0%) | 6 (35.3%) | 8 (28.6%) | 7 (35.0%) | |||
| PR | 0.536 | 0.334 | 0.951 | ||||||
| 0 | 3 (9.7%) | 3 (20.0%) | 2 (6.9%) | 4 (23.5%) | 3 (11.5%) | 3 (15.0%) | |||
| 1+ | 7 (22.6%) | 4 (26.7%) | 6 (20.7%) | 5 (29.4%) | 6 (23.1%) | 5 (25.0%) | |||
| 2+ | 7 (22.6%) | 4 (26.7%) | 8 (27.6%) | 3 (17.6%) | 7 (26.9%) | 4 (20.0%) | |||
| 3+ | 14 (45.2%) | 4 (26.7%) | 13 (44.8%) | 5 (29.4%) | 10 (38.5%) | 8 (40.0%) | |||
| Lymphovascular invasion (%) n = 47 | 14 (43.8%) | 10 (66.7%) | 0.143 | 11 (36.7%) | 13 (76.5%) | 0.015 * | 15 (53.6%) | 9 (47.4%) | 0.676 |
| LN invasion (%) n = 41 | 3 (11.1%) | 5 (35.7%) | 0.097 | 2 (7.7%) | 6 (40.0%) | 0.035 * | 4 (16.7%) | 4 (23.5%) | 0.698 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bing, R.-S.; Tsui, W.L.; Ding, D.-C. The Association between Diabetes Mellitus, High Monocyte/Lymphocyte Ratio, and Survival in Endometrial Cancer: A Retrospective Cohort Study. Diagnostics 2023, 13, 44. https://doi.org/10.3390/diagnostics13010044
Bing R-S, Tsui WL, Ding D-C. The Association between Diabetes Mellitus, High Monocyte/Lymphocyte Ratio, and Survival in Endometrial Cancer: A Retrospective Cohort Study. Diagnostics. 2023; 13(1):44. https://doi.org/10.3390/diagnostics13010044
Chicago/Turabian StyleBing, Ruo-Shi, Wing Lam Tsui, and Dah-Ching Ding. 2023. "The Association between Diabetes Mellitus, High Monocyte/Lymphocyte Ratio, and Survival in Endometrial Cancer: A Retrospective Cohort Study" Diagnostics 13, no. 1: 44. https://doi.org/10.3390/diagnostics13010044