
Maternal and Neonatal Outcomes of Elective Induction of Labor at 39 or More Weeks: A Prospective, Observational Study


Abstract
:1. Introduction
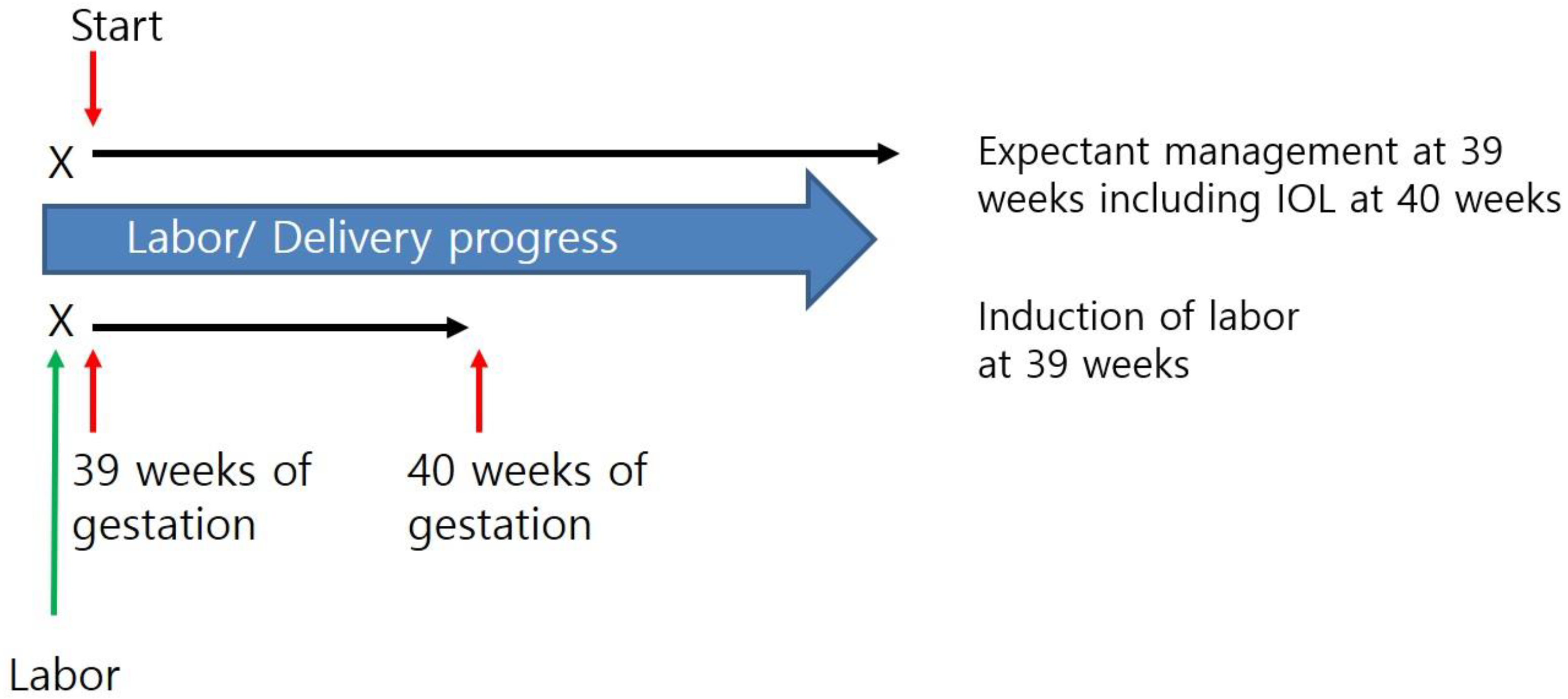
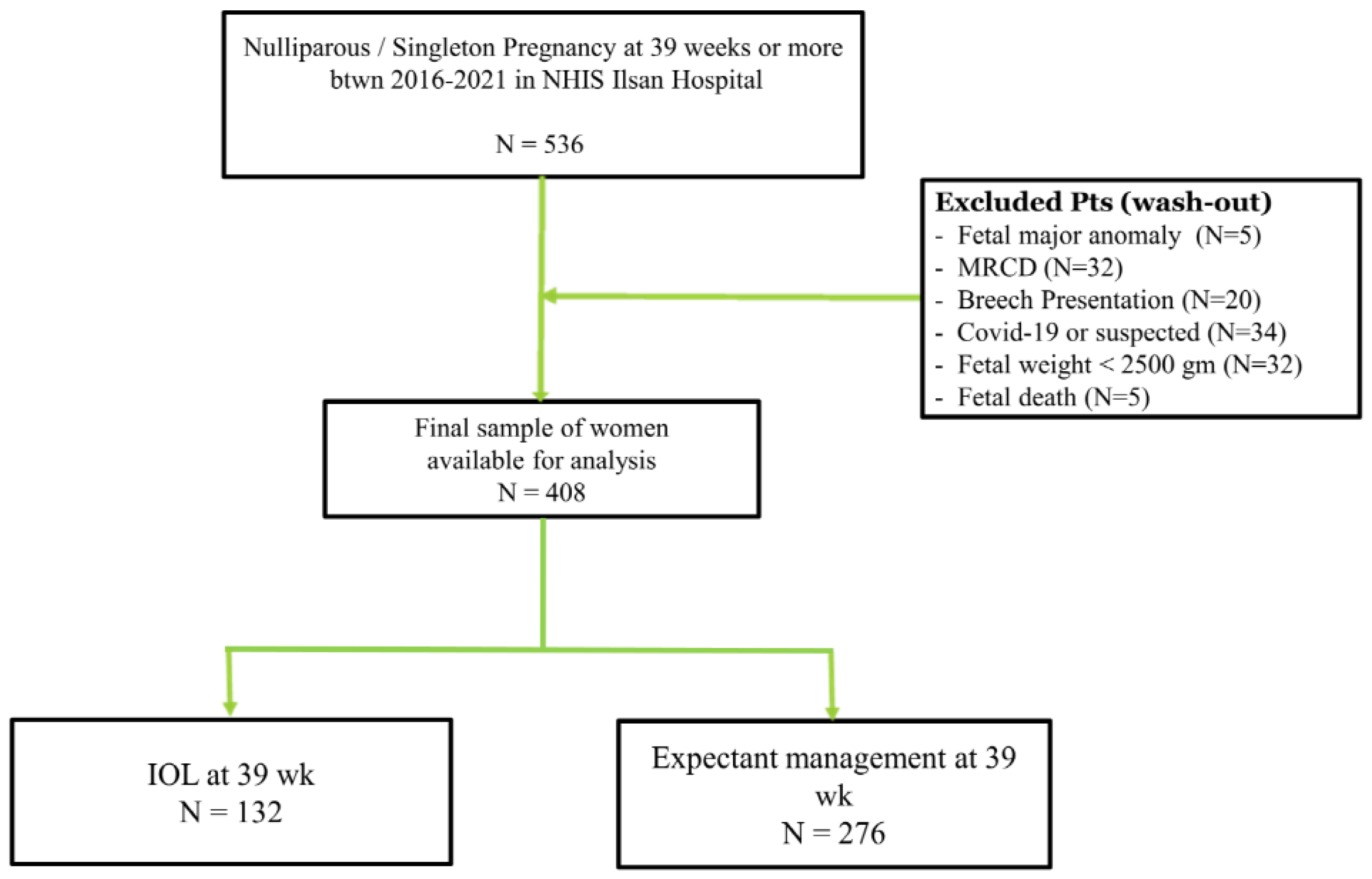
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wen, T.; Turitz, A.L. Optimizing Term Delivery and Mode of Delivery. Clin. Perinatol. 2020, 47, 799–815. [Google Scholar] [CrossRef]
- Papalia, N.; D’Souza, R.D.; Hobson, S.R. Optimal timing of labour induction in contemporary clinical practice. Best Pract. Res. Clin. Obstet. Gynaecol. 2022, 79, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Caughey, A.B.; Stotland, N.E.; Washington, A.E.; Escobar, G.J. Maternal and obstetric complications of pregnancy are associated with increasing gestational age at term. Am. J. Obstet. Gynecol. 2007, 196, 155.e1–155.e6. [Google Scholar] [CrossRef] [Green Version]
- Rydahl, E.; Eriksen, L.; Juhl, M. Effects of induction of labor prior to post-term in low-risk pregnancies: A systematic review. JBI Database Syst. Rev. Implement. Rep. 2019, 17, 170–208. [Google Scholar] [CrossRef] [PubMed]
- Alkmark, M.; Keulen, J.K.J.; Kortekaas, J.C.; Bergh, C.; van Dillen, J.; Duijnhoven, R.G.; Hagberg, H.; Mol, B.W.; Molin, M.; van der Post, J.A.M.; et al. Induction of labour at 41 weeks or expectant management until 42 weeks: A systematic review and an individual participant data meta-analysis of randomised trials. PLoS Med. 2020, 17, e1003436. [Google Scholar] [CrossRef] [PubMed]
- Ehrenthal, D.B.; Jiang, X.; Strobino, D.M. Labor induction and the risk of a cesarean delivery among nulliparous women at term. Obstet. Gynecol. 2010, 116, 35–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiesewetter, B.; Lehner, R. Maternal outcome monitoring: Induction of labor versus spontaneous onset of labor-a retrospective data analysis. Arch. Gynecol. Obstet. 2012, 286, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Visconti, F.; Quaresima, P.; Rania, E.; Palumbo, A.R.; Micieli, M.; Zullo, F.; Venturella, R.; Di Carlo, C. Difficult caesarean section: A literature review. Eur J. Obstet. Gynecol. Reprod. Biol. 2020, 246, 72–78. [Google Scholar] [CrossRef]
- ACOG. Practice Bulletin No. 107: Induction of Labor. Obstet. Gynecol. 2009, 114, 386–397. [Google Scholar] [CrossRef]
- Grobman, W.A. Labor Induction vs. Expectant Management of Low-Risk Pregnancy. N. Engl. J. Med. 2018, 379, 2278–2279. [Google Scholar] [CrossRef]
- ACOG. Clinical Guidance for Integration of the Findings of The ARRIVE Trial: Labor Induction Versus Expectant Management in Low-Risk Nulliparous Women. Available online: https://www.acog.org/clinical/clinical-guidance/practice-advisory/articles/2018/08/clinical-guidance-for-integration-of-the-findings-of-the-arrive-trial (accessed on 15 October 2022).
- SMFM Statement on Elective Induction of Labor in Low-Risk Nulliparous Women at Term: The ARRIVE Trial. Am. J. Obstet. Gynecol. 2019, 221, B2–B4. [CrossRef] [PubMed] [Green Version]
- Statistics Korea. Birth Statistics in 2021. Available online: http://kostat.go.kr/portal/eng/pressReleases/8/1/index.board?bmode=read&bSeq=&aSeq=420358&pageNo=1&rowNum=10&navCount=10&currPg=&searchInfo=&sTarget=title&sTxt= (accessed on 15 October 2022).
- Song, J.E.; Ahn, J.A.; Lee, S.K.; Roh, E.H. Factors related to low birth rate among married women in Korea. PLoS ONE 2018, 13, e0194597. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.H.; Lee, J.; Lee, S.A.; Jung, Y.W. Impact of Maternal Age on Singleton Pregnancy Outcomes in Primiparous Women in South Korea. J. Clin. Med. 2022, 11, 969. [Google Scholar] [CrossRef] [PubMed]
- OECD. Health at a Glance 2013. Available online: https://www.oecd-ilibrary.org/social-issues-migration-health/health-at-a-glance-2013_health_glance-2013-en (accessed on 31 October 2022).
- Reis, F.M.; Gervasi, M.T.; Florio, P.; Bracalente, G.; Fadalti, M.; Severi, F.M.; Petraglia, F. Prediction of successful induction of labor at term: Role of clinical history, digital examination, ultrasound assessment of the cervix, and fetal fibronectin assay. Am. J. Obstet. Gynecol. 2003, 189, 1361–1367. [Google Scholar] [CrossRef]
- Jung, Y.W.; Pak, H.; Lee, I.; Kim, E.H. The Effect of Diagnosis-Related Group Payment System on Quality of Care in the Field of Obstetrics and Gynecology among Korean Tertiary Hospitals. Yonsei Med. J. 2018, 59, 539–545. [Google Scholar] [CrossRef]
- Tsai, T.C.; Joynt, K.E.; Orav, E.J.; Gawande, A.A.; Jha, A.K. Variation in surgical-readmission rates and quality of hospital care. N. Engl. J. Med. 2013, 369, 1134–1142. [Google Scholar] [CrossRef] [Green Version]
- Saccone, G.; Della Corte, L.; Maruotti, G.M.; Quist-Nelson, J.; Raffone, A.; De Vivo, V.; Esposito, G.; Zullo, F.; Berghella, V. Induction of labor at full-term in pregnant women with uncomplicated singleton pregnancy: A systematic review and meta-analysis of randomized trials. Acta Obstet. Gynecol. Scand. 2019, 98, 958–966. [Google Scholar] [CrossRef] [Green Version]
- Freret, T.S.; Woods, G.T.; James, K.E.; Kaimal, A.J.; Clapp, M.A. Incidence of and Risk Factors for Failed Induction of Labor Using a Contemporary Definition. Obstet. Gynecol. 2021, 137, 497–504. [Google Scholar] [CrossRef]
- Grobman, W.A.; Caughey, A.B. Elective induction of labor at 39 weeks compared with expectant management: A meta-analysis of cohort studies. Am. J. Obstet. Gynecol. 2019, 221, 304–310. [Google Scholar] [CrossRef]
- Souter, V.; Painter, I.; Sitcov, K.; Caughey, A.B. Maternal and newborn outcomes with elective induction of labor at term. Am. J. Obstet. Gynecol. 2019, 220, 273.e1–273.e11. [Google Scholar] [CrossRef]
- Zhu, J.; Xue, L.; Shen, H.; Zhang, L.; Lu, D.; Wang, Y.; Zhang, Y.; Zhang, J. Labor induction in China: A nationwide survey. BMC Pregnancy Childbirth 2022, 22, 463. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Induction of Labor (n = 132) | Expectant Management (n = 276) | p-Value |
|---|---|---|---|
| Age (year) | 32.6 ± 4.7 | 31.7 ± 4.2 | 0.060 |
| Gestational age (weeks) | 39.0 | 39.6 ± 0.5 | <0.001 * |
| Weight gain in pregnancy | 12.1 ± 6.0 | 12.9 ± 5.5 | 0.194 |
| BMI | |||
| BMI in pre-pregnancy | 22.0 ± 3.9 | 21.1 ± 2.7 | 0.004 * |
| BMI in term | 27.1 ± 4.2 | 26.2 ± 3.3 | 0.021 * |
| Bishop Score ** at admission | 3.8 ± 1.6 | 4.1 ± 1.8 | 0.170 |
| Cervix length (mm) at admission | 20.1 ± 0.88 | 18.6 ± 8.6 | 0.132 |
| Variables | Induction of Labor (n = 132) | Expectant Management (n = 276) | p-Value |
|---|---|---|---|
| Cesarean section | 24 (18.2) | 44 (15.9) | 0.570 |
| Operative vaginal delivery | 21 (18.9) | 41 (17.2) | 0.700 |
| Length of hospital stay (day) | 4.1 ± 1.3 | 4.0 ± 1.3 | 0.244 |
| Time from admission to delivery (min) | 835 ± 527 | 717 ± 469 | 0.040 * |
| Time for second stage labor (min) | 69 ± 54 | 76 ± 51 | 0.276 |
| Delivery within 12 h | 58 (53.7) | 142 (61.2) | 0.191 |
| Decrease in Hgb after delivery (g/dL) | 1.7 ± 2.1 | 1.8 ± 1.7 | 0.526 |
| Transfusion | 3 (2.3) | 13 (4.7) | 0.235 |
| Embolization | 2 (1.5) | 1 (0.4) | 0.202 |
| Readmission ** | 4 (3.0) | 17 (6.2) | 0.181 |
| Outpatient visits *** > 2 | 73 (55.3) | 154 (55.8) | 0.925 |
| Variables | Induction of Labor (n = 132) | Expectant Management (n = 276) | p-Value |
|---|---|---|---|
| Fetal body weight (gm) | 3233 ± 376 | 3304 ± 341 | 0.057 |
| FBW > 3500 gm | 34 (25.8) | 75 (27.2) | 0.762 |
| Apgar score | |||
| AS at 5 min | 8.2 ± 1.1 | 8.1 ± 1.4 | 0.421 |
| AS at 5 min < 7 | 1 (0.8) | 15 (5.4) | 0.023 * |
| NICU admission | 65 (49.2) | 101 (36.6) | 0.015 * |
| Intubation | 3 (2.3) | 9 (3.3) | 0.581 |
| Meconium-stained amniotic fluid | 18 (13.6) | 51 (18.5) | 0.222 |
| Odds Ratio (95% CI) | ||||
|---|---|---|---|---|
| Unadjusted OR | p-Value | Adjusted OR | p-Value | |
| Induction of labor at 39 weeks | 0.83 (0.48–1.44) | 0.507 | 0.64 (0.28–1.45) | 0.280 |
| Induction of Labor | Expectant Management | |
|---|---|---|
| Maternal outcome | ||
| Cesarean section | Similar | Similar |
| Time from admission to delivery | Shorter | Longer |
| Time for second stage labor | Similar | Similar |
| Postpartum hemorrhage | Similar | Similar |
| Readmission * | Similar | Similar |
| Neonatal outcome | ||
| AS at 5 min <7 | Lower | Higher |
| NICU admission | Higher | Lower |
| Intubation | Similar | Similar |
| Meconium-stained amniotic fluid | Similar | Similar |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.; Cha, D.H.; Park, C.W.; Kim, E.H. Maternal and Neonatal Outcomes of Elective Induction of Labor at 39 or More Weeks: A Prospective, Observational Study. Diagnostics 2023, 13, 38. https://doi.org/10.3390/diagnostics13010038
Lee S, Cha DH, Park CW, Kim EH. Maternal and Neonatal Outcomes of Elective Induction of Labor at 39 or More Weeks: A Prospective, Observational Study. Diagnostics. 2023; 13(1):38. https://doi.org/10.3390/diagnostics13010038
Chicago/Turabian StyleLee, Soobin, Dong Hyun Cha, Cho Won Park, and Eui Hyeok Kim. 2023. "Maternal and Neonatal Outcomes of Elective Induction of Labor at 39 or More Weeks: A Prospective, Observational Study" Diagnostics 13, no. 1: 38. https://doi.org/10.3390/diagnostics13010038