
Three-Dimensional Analysis of Alveolar Bone Morphological Characteristics in Skeletal Class II Open Bite Malocclusion: A Cone-Beam Computed Tomography Study
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Selection and Grouping of Sample
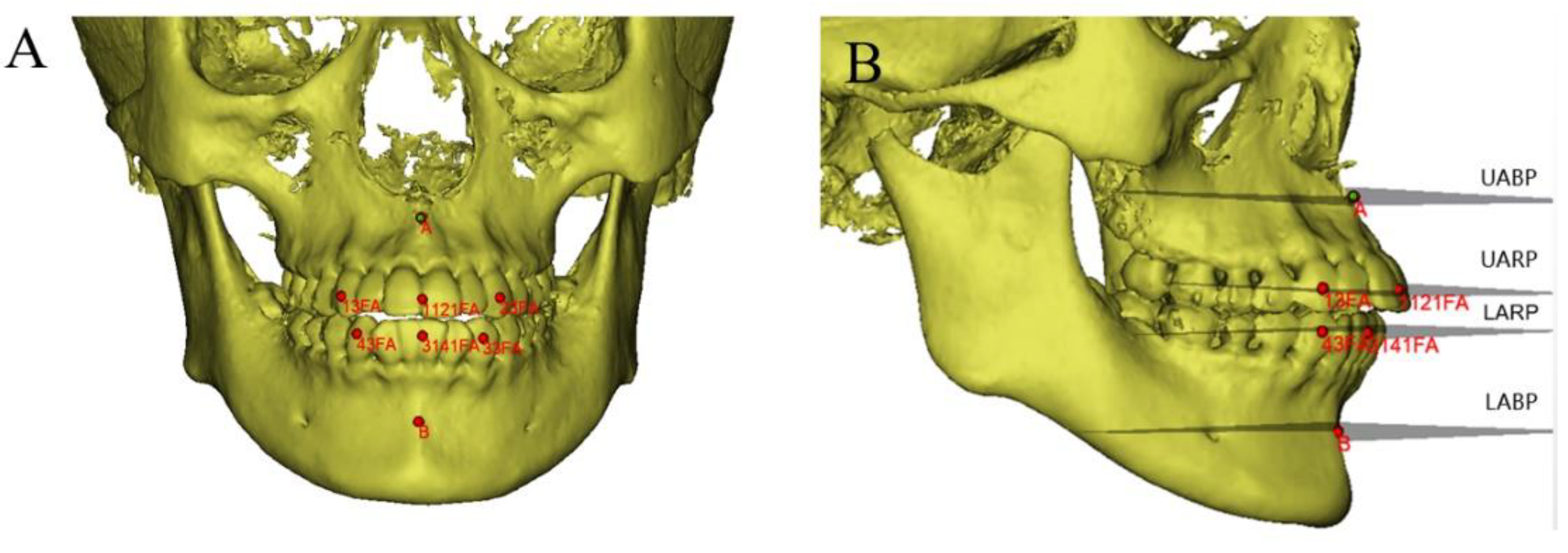
2.2. Acquisition of Imaging Data and Maxillofacial 3D Reconstruction
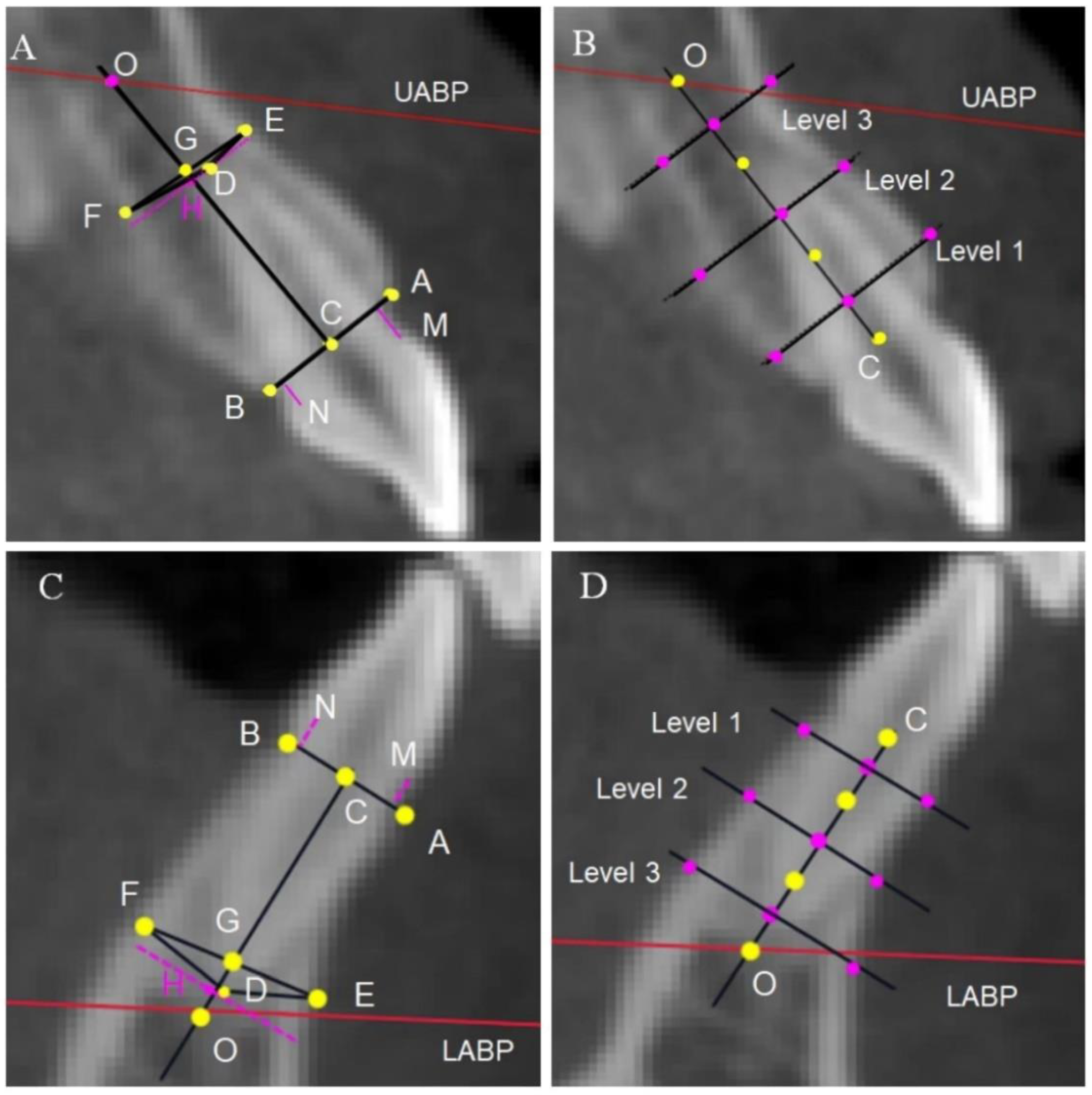
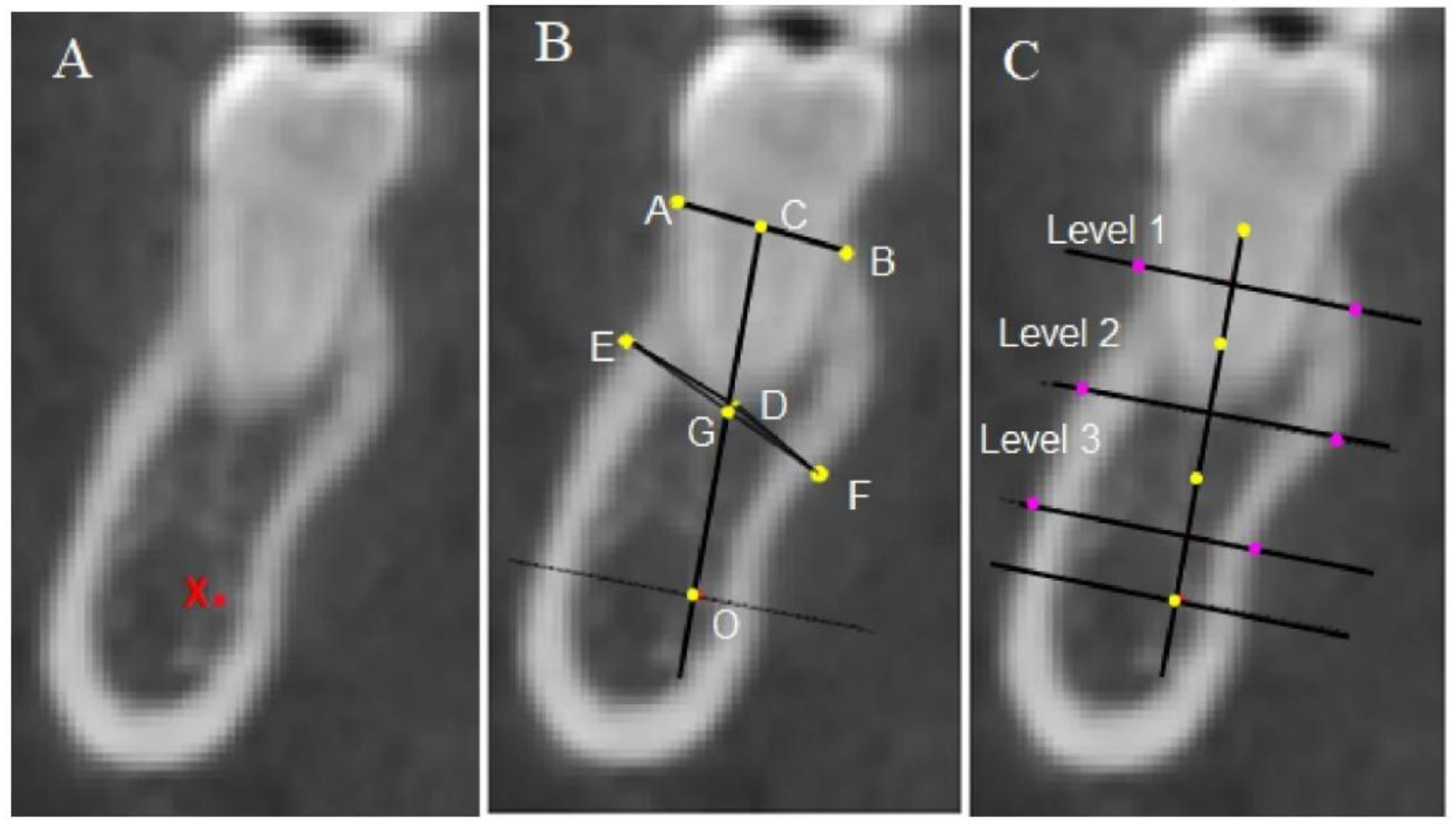
2.3. Measurement Methods and Items
2.4. Statistical Analysis
3. Results
3.1. Sample
3.2. Comparative Description of Cranial–Maxillary Relationships
3.3. Alveolar Features of Central Incisors
3.4. Alveolar Bone Morphological Characteristics
3.5. Correlation Analysis of Anterior Overbite
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Subtelny, J.D.; Sakuda, M. Open-bite: Diagnosis and treatment. Am. J. Orthod. 1964, 50, 337–358. [Google Scholar] [CrossRef]
- Michl, P.; Broniš, T.; Jurásková Sedlatá, E.; Heinz, P.; Pink, R.; Šebek, J.; Mottl, R.; Dvořák, Z.; Tvrdý, P. Anterior open bite—Diagnostics and therapy. Acta Chir. Plast. 2021, 63, 181–184. [Google Scholar] [CrossRef]
- Rohit, K. Open bite malocclusion: An overview. J. Oral Health Craniofacial Sci. 2018, 3, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Tavares, C.A.E.; Allgayer, S. Open bite in adult patients. Dent. Press J. Orthod. 2019, 24, 69–78. [Google Scholar] [CrossRef] [Green Version]
- Franzotti Sant’Anna, E.; Carneiro da Cunha, A.; Paludo Brunetto, D.; Franzotti Sant’Anna, C. Camouflage of a high-angle skeletal Class II open-bite malocclusion in an adult after mini-implant failure during treatment. Am. J. Orthod. Dentofac. Orthop. Off. Publ. Am. Assoc. Orthod. Its Const. Soc. Am. Board Orthod. 2017, 151, 583–597. [Google Scholar] [CrossRef]
- Nahoum, H.I.; Horowitz, S.L.; Benedicto, E.A. Varieties of anterior open-bite. Am. J. Orthod. 1972, 61, 486–492. [Google Scholar] [CrossRef]
- Ellis, E., III; McNamara, J.A., Jr.; Lawrence, T.M. Components of adult Class II open-bite malocclusion. J. Oral Maxillofac. Surg. 1985, 43, 92–105. [Google Scholar] [CrossRef]
- Marzouk, E.S.; Abdallah, E.M.; El-Kenany, W.A. Molar Intrusion in Open-bite Adults Using Zygomatic Miniplates. Int. J. Orthod. Milwaukee Wis 2015, 26, 47–54. [Google Scholar] [CrossRef]
- Shirasaki, K.; Ishihara, Y.; Komori, H.; Yamashiro, T.; Kamioka, H. Comprehensive approach to simultaneous molar intrusion and canine retraction in the treatment of Class II anterior open bite using miniscrew anchorage. Dent. Press J. Orthod. 2020, 25. [Google Scholar] [CrossRef]
- Sousa, R.L.D.S.; Ertty, E.; Portes, M.I.P.; Meloti, F.; Cardoso, M.D.A. Miniplate Anchorage for Correction of Skeletal Anterior Open Bite in an Adult. J. Clin. Orthod. JCO 2021, 55, 175–184. [Google Scholar] [CrossRef]
- Shetty, P.S.; Deshpande, R.S.; Gajaduhada, J.G.; Khan, W.Z.; Prajapat, P.P. A zygomatic miniplate as skeletal anchorage for correction of severe skeletal anterior open bite. J. Clin. Orthod. JCO 2020, 54, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Iwasa, A.; Horiuchi, S.; Kinouchi, N.; Izawa, T.; Hiasa, M.; Kawai, N.; Yasue, A.; Hassan, A.H.; Tanaka, E. Skeletal anchorage for intrusion of bimaxillary molars in a patient with skeletal open bite and temporomandibular disorders. J. Orthod. Sci. 2017, 6, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Laranjo, F. Cephalometric study of the upper airways and dentoalveolar height in open bite patients. Int. Orthod. 2014, 12, 467–482. [Google Scholar] [CrossRef] [PubMed]
- Tsang, W.-M.; Cheung, L.-K.; Samman, N. Cephalometric characteristics of anterior open bite in a southern Chinese population. Am. J. Orthod. Dentofac. Orthop. 1998, 113, 165–172. [Google Scholar] [CrossRef]
- Sassouni, V.; Nanda, S. Analysis of dentofacial vertical proportions. Am. J. Orthod. 1964, 50, 801–823. [Google Scholar] [CrossRef]
- Frost, D.E.; Fonseca, R.J.; Turvey, T.A.; Hall, D.J. Cephalometric diagnosis and surgical-orthodontic correction of apertognathia. Am. J. Orthod. 1980, 78, 657–669. [Google Scholar] [CrossRef]
- Sghaireen, M.G.; Srivastava, K.C.; Shrivastava, D.; Ganji, K.K.; Patil, S.R.; Abuonq, A.; Mousa, M.A.; Dar-Odeh, N.; Sghaireen, G.M.; Kamal, M.A.; et al. A CBCT Based Three-Dimensional Assessment of Mandibular Posterior Region for Evaluating the Possibility of Bypassing the Inferior Alveolar Nerve While Placing Dental Implants. Diagn. Basel Switz. 2020, 10, E406. [Google Scholar] [CrossRef]
- Islam, Z.U.; Shaikh, A.J.; Fida, M. Dentoalveolar Heights in Vertical and Sagittal Facial Patterns. J. Coll. Physicians Surg. Pak. 2016, 26, 753–757. [Google Scholar] [CrossRef]
- Kucera, J.; Marek, I.; Tycova, H.; Baccetti, T. Molar height and dentoalveolar compensation in adult subjects with skeletal open bite. Angle Orthod. 2011, 81, 564–569. [Google Scholar] [CrossRef]
- Arriola-Guillén, L.E.; Flores-Mir, C. Molar heights and incisor inclinations in adults with Class II and Class III skeletal open-bite malocclusions. Am. J. Orthod. Dentofac. Orthop. 2014, 145, 325–332. [Google Scholar] [CrossRef]
- Kuitert, R.; Beckmann, S.; van Loenen, M.; Tuinzing, B.; Zentner, A. Dentoalveolar compensation in subjects with vertical skeletal dysplasia. Am. J. Orthod. Dentofac. Orthop. 2006, 129, 649–657. [Google Scholar] [CrossRef] [PubMed]
- Teerakanok, S.; Charoemratrote, C.; Chanmanee, P. The Accuracy of Lateral Cephalogram in Representing the Anterior Maxillary Dentoalveolar Position. Diagn. Basel Switz. 2022, 12, 1840. [Google Scholar] [CrossRef] [PubMed]
- Alhujhuj, R.R.; Jouhar, R.; Ahmed, M.A.; Almujhim, A.A.; Albutayh, M.T.; Adanir, N. Evaluation of Root Canal Configuration of Maxillary and Mandibular First Molar by CBCT: A Retrospective Cross-Sectional Study. Diagnostics 2022, 12, 2121. [Google Scholar] [CrossRef] [PubMed]
- Kosumarl, W.; Patanaporn, V.; Jotikasthira, D.; Janhom, A. Distances from the root apices of posterior teeth to the maxillary sinus and mandibular canal in patients with skeletal open bite: A cone-beam computed tomography study. Imaging Sci. Dent. 2017, 47, 157–164. [Google Scholar] [CrossRef] [Green Version]
- Nahoum, H.I. Vertical proportions: A guide for prognosis and treatment in anterior open-bite. Am. J. Orthod. 1977, 72, 128–146. [Google Scholar] [CrossRef]
- Cesur, E.; Köklü, A. Evaluation of Maxillofacial Characteristics in Individuals with Anterior Open Bite Using Denture Frame Analysis. Turk J. Orthod. 2020, 33, 157–164. [Google Scholar] [CrossRef]
- Lundstrm, A.F. Malocclusion of the teeth regarded as a problem in connection with the apical base. Int. J. Orthod. Oral Surg. Radiogr. 1925, 11, 933–941. [Google Scholar] [CrossRef]
- Hee-Chan, P.; Jin-Woo, L. Study of horizontal skeletal pattern and dental arch in skeletal Class III malocclusion patients. Korean J. Orthod. 2008, 38, 358–370. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.T.; Lee, J.W. Three dimensional structural analysis between dental arch and basal bone in normal occlusion. Korean J. Orthod. 2011, 41, 224–236. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.; Skrypczak, A.; Weltman, R. Anterior maxilla alveolar ridge dimension and morphology measurement by cone beam computerized tomography (CBCT) for immediate implant treatment planning. BMC Oral Health 2015, 15, 65. [Google Scholar] [CrossRef]
- Arriola-Guillén, L.E.; Flores-Mir, C. Anterior maxillary dentoalveolar and skeletal cephalometric factors involved in upper incisor crown exposure in subjects with Class II and III skeletal open bite. Angle Orthod. 2015, 85, 72–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baysal, A.; Ucar, F.I.; Buyuk, S.K.; Ozer, T.; Uysal, T. Alveolar bone thickness and lower incisor position in skeletal Class I and Class II malocclusions assessed with cone-beam computed tomography. Korean J. Orthod. 2013, 43, 134–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsumoto, M.A.N.; Romano, F.L.; Ferreira, J.T.L.; Valério, R.A. Open bite: Diagnosis, treatment and stability. Braz. Dent. J. 2012, 23, 768–778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haining, J.; Ying, D. Alveolar Bone Morphology of Anterior Teeth in Adult Skeletal Class Ⅱ Malocclusions Assessed with Cone-Beam CT; The Fourth Military Medical University: Xi’an, China, 2014. (In Chinese) [Google Scholar]
- Isaacson, J.R.; Isaacson, R.J.; Speidel, T.M.; Worms, F.W. Extreme variation in vertical facial growth and associated variation in skeletal and dental relations. Angle Orthod. 1971, 41, 219–229. [Google Scholar] [CrossRef]
- Choi, Y.J.; Kim, D.J.; Nam, J.; Chung, C.J.; Kim, K.H. Cephalometric configuration of the occlusal plane in patients with anterior open bite. Am. J. Orthod Dentofacial Orthop. 2016, 149, 391–400. [Google Scholar] [CrossRef]
- Lopez-Gavito, G.; Wallen, T.R.; Little, R.M.; Joondeph, D.R. Anterior open-bite malocclusion: A longitudinal 10-year postretention evaluation of orthodontically treated patients. Am. J. Orthod. 1985, 87, 175–186. [Google Scholar] [CrossRef]
- Valarelli, F.P.; Silva, M.F.A.; Imai, L.; Janson, G.; Freitas, K.M.S. Strategies for compensatory orthodontic treatment of adult skeletal open bite. J. Clin. Orthod. JCO 2021, 55, 419–428. [Google Scholar] [CrossRef]
- Yilmaz, H.N.; Alakus, E.; Erdem, B.; Kucukkeles, N. Effect of piezocision on molar intrusion in open-bite treatment using a modified MEAW technique. J. Orofac. Orthop. Fortschr. Kieferorthopadie OrganOfficial J. Dtsch. Ges. Kieferorthopadie 2021, 82, 163–174. [Google Scholar] [CrossRef]
- Shuka, M.; Araújo, E.A.; Mccray, J.F.; Guilherme, T.; Beom, K.K. Cephalometric evaluation of adult anterior open bite non-extraction treatment with Invisalign. Dent. Press J. Orthod. 2017, 22, 30–38. [Google Scholar] [CrossRef] [Green Version]
- Pikdoken, L.; Erkan, M.; Usumez, S. Gingival response to mandibular incisor extrusion. Am. J. Orthod Dentofacial Orthop. 2009, 135, 143.e9–143.e13. [Google Scholar] [CrossRef]
- Akan, B.; Ünal, B.K.; Şahan, A.O.; Kızıltekin, R. Evaluation of anterior open bite correction in patients treated with maxillary posterior segment intrusion using zygomatic anchorage. Am. J. Orthod. Dentofac. Orthop. Off. Publ. Am. Assoc. Orthod. Its Const. Soc. Am. Board Orthod. 2020, 158, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Akbaydogan, L.C.; Akin, M. Cephalometric evaluation of intrusion of maxillary posterior teeth by miniscrews in the treatment of open bite—ScienceDirect. Am. J. Orthod. Dentofac. Orthop. 2022, 161, 621–627. [Google Scholar] [CrossRef] [PubMed]
- Baek, M.-S.; Choi, Y.-J.; Yu, H.-S.; Lee, K.-J.; Kwak, J.; Park, Y.-C. Long-term stability of anterior open-bite treatment by intrusion of maxillary posterior teeth. Am. J. Orthod. Dentofac. Orthop. 2010, 138, 396.e1–396.e9. [Google Scholar] [CrossRef] [PubMed]
- Alsafadi, A.S.; Alabdullah, M.M.; Saltaji, H.; Abdo, A.; Youssef, M. Effect of molar intrusion with temporary anchorage devices in patients with anterior open bite: A systematic review. Prog. Orthod. 2016, 17, 9. [Google Scholar] [CrossRef] [Green Version]
- Scheffler, N.R.; Proffit, W.R.; Phillips, C. Outcomes and stability in patients with anterior open bite and long anterior face height treated with temporary anchorage devices and a maxillary intrusion splint. Am. J. Orthod. Dentofac. Orthop. 2014, 146, 594–602. [Google Scholar] [CrossRef] [Green Version]
- Sugawara, J.; Baik, U.B.; Umemori, M.; Takahashi, I.; Mitani, H. Treatment and posttreatment dentoalveolar changes following intrusion of mandibular molars with application of a skeletal anchorage system (SAS) for open bite correction. Int. J. Adult Orthodon. Orthognath. Surg. 2002, 17, 243. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group 1 | Group 2 | Group 3 | p Value | |
|---|---|---|---|---|
| Number | 29 | 29 | 24 | |
| Age (y; median (Q1~Q3)) | 18 (15.5~21.5) | 20 (15~23) | 21 (17.25~22) | NS b |
| Gender (female/total) | 22/29 | 20/29 | 21/24 | 0.278 c |
| Group 1 (Class II; OB) | Group 2 (Class II; NOB) | Group 3 (Class I; NOB) | p (Group) | Comparison Between Groups | |||
|---|---|---|---|---|---|---|---|
| 1 vs. 2 | 1 vs. 3 | 2 vs. 3 | |||||
| SNA | 80.43 ± 4.02 | 82.98 ± 2.76 | 81.11 ± 2.63 | 0.011 * | 0.003 ** | 0.444 | 0.039 * |
| SNB | 73.82 ± 3.85 | 76.3 ± 3.17 | 78.18 ± 2.31 | 0.000 † | 0.004 ** | 0.000 † | 0.038 * |
| ANB | 6 (5.5~7.6) | 6.4 (5.45~7.7) | 3.2 (2.13~3.88) | 0.000 † | 1.000 | 0.000 † | 0.000 † |
| SN-GoGn | 43.3 (40.1~46.15) | 35 (32.4~36.95) | 33.5 (32.93~35.8) | 0.000 † | 0.000 † | 0.000 † | 1.000 |
| OB | −2.79 ± 1.78 | 4.19 ± 1.4 | 2.67 ± 1.22 | 0.000 † | 0.000 † | 0.000 † | 0.000 † |
| OJ | 5.5 (3.9~7) | 5 (3.8~6.95) | 3.4 (2.25~3.75) | 0.000 † | 1.000 | 0.000 † | 0.000 † |
| N-S-Ar | 124.8 (121.2~127.5) | 124.9 (122.4~126.55) | 126.45 (125.23~129.78) | 0.056 | / | / | / |
| S-Ar-Go | 153.3 (149~158.15) | 150.9 (148.4~155.1) | 146.95 (145~151.03) | 0.007 ** | 1.000 | 0.007 ** | 0.056 |
| Ar-Go-Me | 126.96 ± 6.09 | 119.18 ± 4.83 | 119.11 ± 5.2 | 0.000 † | 0.000 † | 0.000 † | 0.964 |
| Jarabac’s sum | 405.6 (401~408.9) | 396.4 (393~398.4) | 393.65 (392.45~396.3) | 0.000 † | 0.000 † | 0.000 † | 1.000 |
| Ar-Go-N | 44.42 ± 3.39 | 43.76 ± 2.88 | 44.23 ± 3.44 | 0.731 | 0.443 | 0.837 | 0.599 |
| N-Go-Me | 82.53 ± 4.47 | 75.4 ± 3.33 | 74.87 ± 3.1 | 0.000 † | 0.000 † | 0.000 † | 0.607 |
| S-Go/N-Me% | 58.1 (56.5~62.45) | 63.4 (61.85~64.9) | 63.7 (62.2~64.88) | 0.000 † | 0.001 ** | 0.001 ** | 1.000 |
| ANS-ME/N-Me% | 56.25 ± 1.24 | 54.22 ± 1.15 | 54.68 ± 1.69 | 0.000 † | 0.000 † | 0.000 † | 0.222 |
| IMPA | 95.06 ± 5.29 | 100.93 ± 4.71 | 96.95 ± 4.64 | 0.000 † | 0.000 † | 0.167 | 0.004 ** |
| FMA | 33.64 ± 5.68 | 26.43 ± 3.65 | 23.88 ± 3.93 | 0.000 † | 0.000 † | 0.000 † | 0.045 * |
| U1-L1 | 113.05 ± 8.77 | 119.15 ± 8.36 | 123.32 ± 5.08 | 0.000 † | 0.003 ** | 0.000 † | 0.054 |
| U1-SN | 106.91 ± 7.61 | 104.02 ± 6.7 | 104.93 ± 4.28 | 0.228 | 0.093 | 0.270 | 0.612 |
| Group 1 (Class II; OB) | Group 2 (Class II; NOB) | Group 3 (Class I; NOB) | p (Group) | Comparison Between Groups | |||
|---|---|---|---|---|---|---|---|
| 1 vs. 2 | 1 vs. 3 | 2 vs. 3 | |||||
| A1-height | 15.35 (13.53~17.81) | 15.73 (14.57~16.83) | 15.65 (14.15~18.06) | 0.747 | / | / | / |
| A1-thickness | 8.05 ± 1.29 | 9.25 ± 1.11 | 8.96 ± 1.01 | 0.000 † | 0.000 † | 0.005 ** | 0.355 |
| A1-UBH | 2.33 ± 0.51 | 2.07 ± 0.41 | 2.00 ± 0.41 | 0.020 * | 0.031 * | 0.009 ** | 0.574 |
| A1-LBH | 1.71 (1.40~2.03) | 1.73 (1.50~1.95) | 1.34 (1.21~1.52) | 0.000 † | 1.000 | 0.002 ** | 0.001 ** |
| A1-OH | 6.23 ± 2.14 | 5.27 ± 1.60 | 6.64 ± 1.97 | 0.242 | 0.331 | 0.451 | 0.095 |
| C1-height | 12.51 (10.85~14.77) | 14.77 (12.69~17.11) | 14.59 (13.07~15.75) | 0.038 * | 0.059 | 0.123 | 1.000 |
| C1-thickness | 6.95 ± 1.15 | 8.28 ± 1.21 | 8.58 ± 1.33 | 0.000 † | 0.000 † | 0.000 † | 0.371 |
| C1-UBH | 2.59 ± 0.50 | 2.42 ± 0.61 | 2.20 ± 0.39 | 0.027 * | 0.205 | 0.007 ** | 0.129 |
| C1-LBH | 2.33 ± 0.56 | 2.60 ± 0.50 | 2.35 ± 0.42 | 0.086 | 0.110 | 0.990 | 0.174 |
| C1-OH | 5.54 ± 2.65 | 6.07 ± 2.22 | 5.69 ± 2.25 | 0.680 | 0.393 | 0.811 | 0.565 |
| Group 1 (Class II; OB) | Group 2 (Class II; NOB) | Group 3 (Class I; NOB) | p (Group) | Comparison Between Groups | |||
|---|---|---|---|---|---|---|---|
| 1 vs. 2 | 1 vs. 3 | 2 vs. 3 | |||||
| A3-height | 13.47 ± 2.62 | 14.57 ± 1.84 | 14.94 ± 2.06 | 0.043 * | 0.061 | 0.018 * | 0.547 |
| A5-height | 12.49 (10.05~14.45) | 11.25 (9.29~13.3) | 10.85 (9.31~16.18) | 0.320 | / | / | / |
| A6-height | 9.46 (8.02~12.5) | 7.9 (6.85~9.07) | 7.4 (5.84~10.56) | 0.021 * | 0.049 * | 0.052 | 1.000 |
| A7-height | 10.59 ± 2.62 | 9.93 ± 2.34 | 9.26 ± 2.58 | 0.165 | / | / | / |
| C3- height | 12.08 (10.74~14.56) | 14.32 (12.97~17.32) | 13.96 (12.13~15) | 0.012 * | 0.010 * | 0.274 | 0.796 |
| C5-height | 16.27 ± 3 | 16.84 ± 2.87 | 17.01 ± 1.98 | 0.569 | / | / | / |
| C6M-height | 15.36 ± 2.92 | 16.89 ± 2.39 | 17.01 ± 2.04 | 0.028 * | 0.023 * | 0.020 * | 0.864 |
| C6D-height | 15.2 ± 2.94 | 16.63 ± 2.31 | 16.57 ± 1.78 | 0.050 | 0.072 | 0.109 | 0.996 |
| C6-height | 15.29 ± 2.86 | 16.76 ± 2.32 | 16.79 ± 1.86 | 0.033 * | 0.023 * | 0.027 * | 0.963 |
| C7M-height | 13.43 (12.76~14.58) | 14.98 (13.85~16.23) | 14.32 (12.98~15.57) | 0.038 * | 0.031 * | 0.738 | 0.605 |
| C7D-height | 13.43 ± 2.47 | 14.78 ± 2.25 | 14.1 ± 1.66 | 0.069 | / | / | / |
| C7-height | 13.44 (12.06~14.68) | 15.24 (13.67~16.36) | 14.52 (12.98~15.2) | 0.017 * | 0.013 * | 0.418 | 0.649 |
| A3-thickness | 8.95 ± 1.16 | 10.89 ± 1.87 | 10.44 ± 1.26 | 0.000 † | 0.000 † | 0.000 † | 0.279 |
| A5-thickness | 10.83 ± 1.62 | 12.18 ± 1.27 | 12.22 ± 1.74 | 0.001 ** | 0.001 ** | 0.002 ** | 0.922 |
| A6-thickness | 14.75 ± 1.56 | 15.98 ± 1.18 | 15.18 ± 0.93 | 0.002 ** | 0.000† | 0.223 | 0.024 * |
| A7-thickness | 15.37 (14.82~16.95) | 16.8 (15.74~17.87) | 15.82 (15.55~16.57) | 0.033 * | 0.042 * | 1.000 | 0.148 |
| C3-thickness | 8.54 (7.96~9.4) | 10.12 (9.41~11.65) | 10.17 (9.49~11.1) | 0.000 † | 0.000 † | 0.000 † | 1.000 |
| C5-thickness | 10.29 (9.64~11.59) | 10.86 (10.56~12.23) | 11.52 (10.76~12.79) | 0.003 ** | 0.054 | 0.003 ** | 0.910 |
| C6M-thickness | 11.85 (10.86~12.97) | 12.94 (11.91~14.03) | 13.11 (12.34~13.93) | 0.001 ** | 0.007 ** | 0.002 ** | 1.000 |
| C6D-thickness | 12.33 ± 1.2 | 13.67 ± 1.38 | 13.72 ± 1.07 | 0.000 † | 0.000 † | 0.000 † | 0.872 |
| C7M-thickness | 13.27 (12.46~14.54) | 14.79 (13.65~15.66) | 14.96 (13.59~15.46) | 0.003 ** | 0.006 ** | 0.020 * | 1.000 |
| C7D-thickness | 13.54 (12.79~15.23) | 14.69 (13.92~15.83) | 14.86 (13.69~15.48) | 0.012 * | 0.014 * | 0.106 | 1.000 |
| Parameter | Group 1 (Class II; OB) | Group 2 (Class II; NOB) | Group 3 (Class I; NOB) | |||
|---|---|---|---|---|---|---|
| r | p | r | p | r | p | |
| U1-L1 | −0.045 | 0.815 | 0.420 * | 0.023 | 0.324 | 0.123 |
| A1-OH | 0.537 ** | 0.003 | −0.131 | 0.499 | 0.030 | 0.888 |
| C1-OH | 0.286 | 0.133 | 0.317 | 0.094 | 0.146 | 0.496 |
| A1-thickness | 0.432 * | 0.019 | 0.296 | 0.119 | 0.389 | 0.061 |
| A3-thickness | 0.011 | 0.954 | 0.450 * | 0.014 | 0.347 | 0.097 |
| A5-thickness | 0.048 | 0.807 | 0.490 ** | 0.007 | 0.556 ** | 0.005 |
| A6-thickness | 0.015 | 0.940 | 0.229 | 0.233 | 0.323 | 0.124 |
| A7-thickness | −0.270 | 0.157 | 0.187 | 0.331 | 0.294 | 0.163 |
| C1-thickness | −0.346 | 0.066 | 0.496 ** | 0.006 | 0.518 ** | 0.009 |
| C3-thickness | −0.264 | 0.166 | 0.149 | 0.440 | 0.364 | 0.081 |
| C5-thickness | 0.195 | 0.310 | 0.456 * | 0.013 | 0.428 * | 0.037 |
| C6M-thickness | 0.072 | 0.712 | 0.240 | 0.210 | 0.410 * | 0.046 |
| C6D-thickness | 0.089 | 0.647 | 0.211 | 0.272 | 0.407 * | 0.049 |
| C7M-thickness | −0.035 | 0.859 | 0.047 | 0.808 | 0.310 | 0.140 |
| C7D-thickness | −0.082 | 0.673 | −0.054 | 0.780 | 0.371 | 0.074 |
| A1-height | 0.541 ** | 0.002 | −0.113 | 0.561 | 0.308 | 0.143 |
| A3-height | 0.379 * | 0.043 | 0.261 | 0.172 | 0.179 | 0.403 |
| A5-height | −0.168 | 0.383 | 0.167 | 0.386 | −0.073 | 0.736 |
| A6-height | −0.521 ** | 0.004 | 0.295 | 0.121 | −0.039 | 0.856 |
| A7-height | −0.538 ** | 0.003 | 0.223 | 0.245 | −0.110 | 0.608 |
| C1-height | 0.204 | 0.288 | 0.502 ** | 0.005 | 0.323 | 0.124 |
| C3-height | 0.188 | 0.329 | 0.119 | 0.538 | 0.180 | 0.399 |
| C5-height | 0.024 | 0.901 | 0.056 | 0.774 | 0.311 | 0.139 |
| C6-height | 0.149 | 0.441 | −0.097 | 0.617 | 0.126 | 0.557 |
| C7-height | 0.158 | 0.414 | −0.009 | 0.965 | 0.273 | 0.197 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tang, Y.; Xu, J.; Hu, Y.; Huang, Y.; Liu, Y.; Daraqel, B.; Zheng, L. Three-Dimensional Analysis of Alveolar Bone Morphological Characteristics in Skeletal Class II Open Bite Malocclusion: A Cone-Beam Computed Tomography Study. Diagnostics 2023, 13, 39. https://doi.org/10.3390/diagnostics13010039
Tang Y, Xu J, Hu Y, Huang Y, Liu Y, Daraqel B, Zheng L. Three-Dimensional Analysis of Alveolar Bone Morphological Characteristics in Skeletal Class II Open Bite Malocclusion: A Cone-Beam Computed Tomography Study. Diagnostics. 2023; 13(1):39. https://doi.org/10.3390/diagnostics13010039
Chicago/Turabian StyleTang, Yingying, Jingfeng Xu, Yun Hu, Yumei Huang, Yang Liu, Baraa Daraqel, and Leilei Zheng. 2023. "Three-Dimensional Analysis of Alveolar Bone Morphological Characteristics in Skeletal Class II Open Bite Malocclusion: A Cone-Beam Computed Tomography Study" Diagnostics 13, no. 1: 39. https://doi.org/10.3390/diagnostics13010039