
Usefulness of Practitioner-Led Pancreatic Cancer Screening

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics Approval
2.2. Data Collection
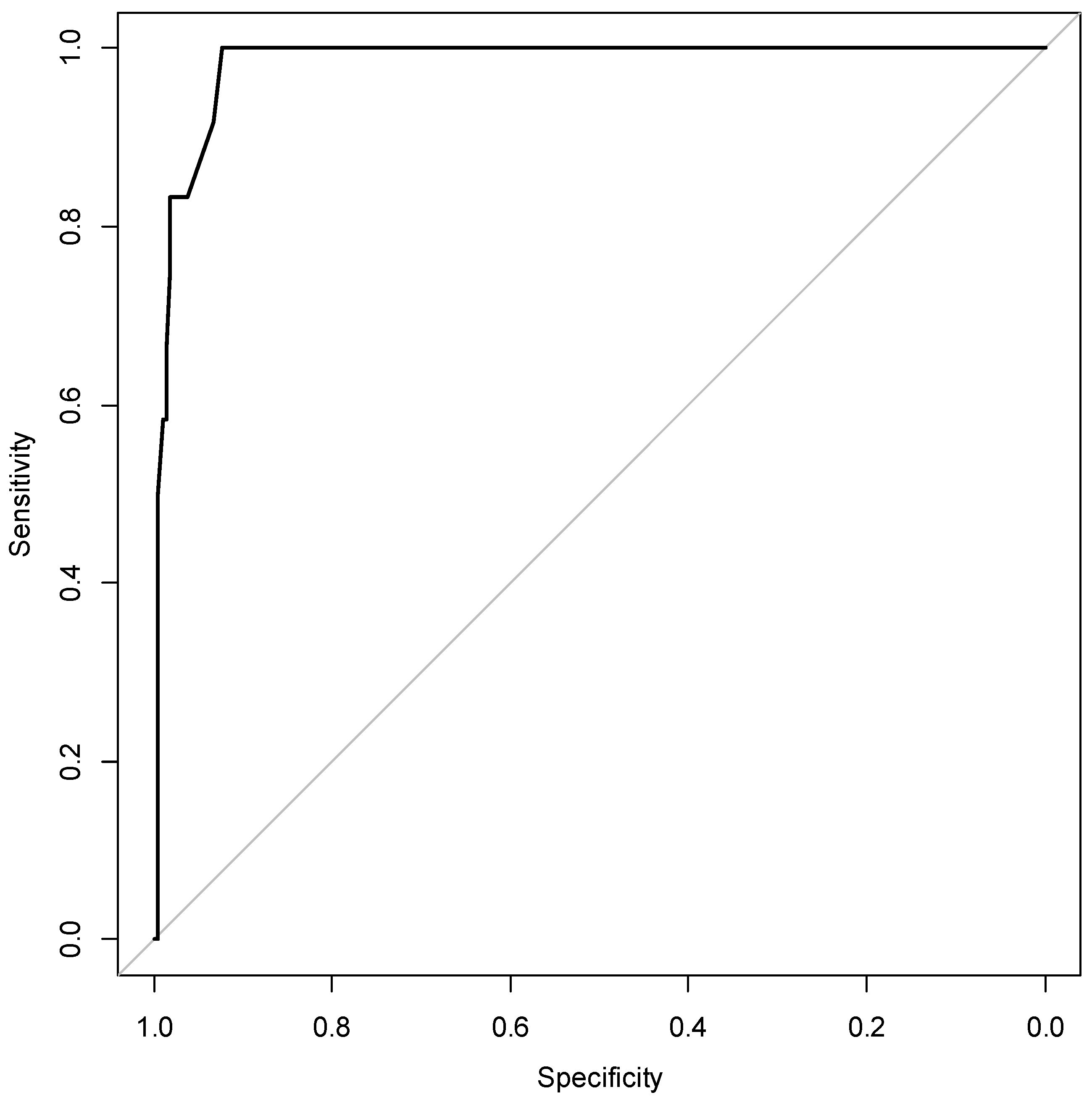
2.3. Statistical Analyses
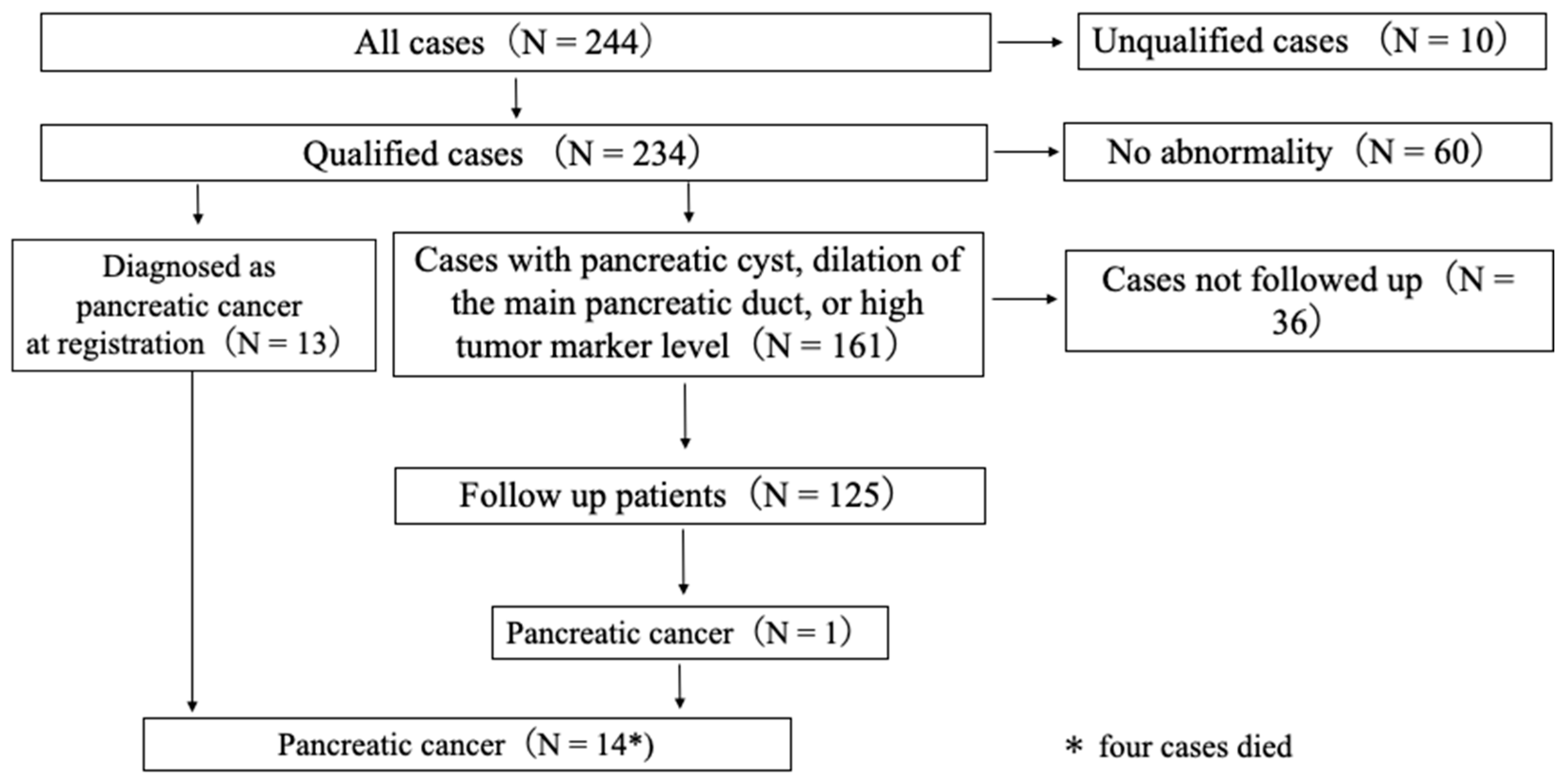
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics. CA. Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Egawa, S.; Toma, H.; Ohigashi, H.; Okusaka, T.; Nakao, A.; Hatori, T.; Maguchi, H.; Yanagisawa, A.; Tanaka, M. Japan pancreatic cancer registry; 30th year anniversary: Japan pancreas society. Pancreas 2012, 41, 985–992. [Google Scholar] [CrossRef] [PubMed]
- Kanno, A.; Masamune, A.; Hanada, K.; Maguchi, H.; Shimizu, Y.; Ueki, T.; Hasebe, O.; Ohtsuka, T.; Nakamura, M.; Takenaka, M.; et al. Multicenter study of early pancreatic cancer in Japan. Pancreatology 2018, 18, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Egawa, S.; Takeda, Y.; Akada, M.; Abe, H.; Yokoyama, T.; Motoi, F.; Fukuyama, S.; Sunamura, M.; Matsuno, S. Small pancreatic cancer: From the national pancreatic cancer registry. Pancreas 2005, 31, 11. [Google Scholar] [CrossRef]
- Sakamoto, H.; Harada, S.; Nishioka, N.; Maeda, K.; Kurihara, T.; Sakamoto, T.; Higuchi, K.; Kitano, M.; Takeyama, Y.; Kogire, M.; et al. A social program for the early detection of pancreatic cancer: The Kishiwada Katsuragi Project. Oncology 2017, 93 (Suppl. S1), 89–97. [Google Scholar] [CrossRef]
- Kurihara, K.; Hanada, K.; Shimizu, A. endoscopic ultrasonography diagnosis of early pancreatic cancer. Diagnostics 2020, 10, 1086. [Google Scholar] [CrossRef]
- Yazumi, S.; Kudo, Y.; Kurita, A. A screening strategy for detecting early pancreatic cancer. Nihon Shokakibyo Gakkai Zasshi 2018, 115, 338–349. [Google Scholar] [CrossRef]
- Tanno, S.; Nakano, Y.; Koizumi, K.; Sugiyama, Y.; Nakamura, K.; Sasajima, J.; Nishikawa, T.; Mizukami, Y.; Yanagawa, N.; Fujii, T.; et al. Pancreatic ductal adenocarcinomas in long-term follow-up patients with branch duct intraductal papillary mucinous neoplasms. Pancreas 2010, 39, 36–40. [Google Scholar] [CrossRef]
- Uehara, H.; Nakaizumi, A.; Ishikawa, O.; Iishi, H.; Tatsumi, K.; Takakura, R.; Ishida, T.; Takano, Y.; Tanaka, S.; Takenaka, A. Development of ductal carcinoma of the pancreas during follow-up of branch duct intraductal papillary mucinous neoplasm of the pancreas. Gut 2008, 57, 1561–1565. [Google Scholar] [CrossRef]
- Permert, J.; Larsson, J.; Fruin, A.B.; Tatemoto, K.; Herrington, M.K.; von Schenck, H.; Adrian, T.E. Islet hormone secretion in pancreatic cancer patients with diabetes. Pancreas 1997, 15, 60–68. [Google Scholar] [CrossRef]
- Permert, J.; Ihse, I.; Jorfeldt, L.; von Schenck, H.; Arnqvist, H.J.; Larsson, J. Improved glucose metabolism after subtotal pancreatectomy for pancreatic cancer. Br. J. Surg. 1993, 80, 1047–1050. [Google Scholar] [CrossRef] [PubMed]
- Pannala, R.; Leimess, J.B.; Bamlet, W.R.; Basu, A.; Petersen, G.M.; Chari, S.T. Prevalence and clinical profile of pancreatic cancer-associated diabetes mellitus. Gastroenterology 2008, 134, 981–987. [Google Scholar] [CrossRef] [PubMed]
- Chari, S.T.; Leibson, C.L.; Rabe, K.G.; Ransom, J.; de Andrade, M.; Petersen, G.M. Probability of pancreatic cancer following diabetes: A population-based study gastroenterology. Gastroenterology 2005, 129, 504–511. [Google Scholar] [CrossRef] [PubMed]
- Carstensen, B.; Read, S.H.; Friis, S.; Sund, R.; Keskimäki, I.; Svensson, A.-M.; Ljung, R.; Wild, S.H.; Kerssens, J.J.; Harding, J.L.; et al. Cancer incidence in persons with type 1 diabetes: A five-country study of 9000 cancers in type 1 diabetic individuals. Diabetologia 2016, 59, 980–988. [Google Scholar] [CrossRef]
- Ben, Q.W.; Xu, M.J.; Ning, X.Y.; Liu, J.; Hong, S.Y.; Huang, W.; Zhang, H.G.; Li, Z.S. Diabetes mellitus and risk of pancreatic cancer: A meta-analysis of cohort studies. Eur. J. Cancer 2011, 47, 1928–1937. [Google Scholar] [CrossRef]
- Sakamoto, H.; Kitano, M.; Suetomi, Y.; Maekawa, K.; Takeyama, Y.; Kudo, M. Utility of contrast-enhanced endoscopic ultrasonography for diagnosis of small pancreatic carcinomas. Ultrasound Med. Biol. 2008, 34, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Krishna, S.G.; Rao, B.B.; Ugbarugba, E.; Shah, Z.K.; Blaszczak, A.; Hinton, A.; Conwell, D.L.; Hart, P.A. Diagnostic performance of endoscopic ultrasound for detection of pancreatic malignancy following an indeterminate multidetector CT scan: A systemic review and meta-analysis. Surg. Endosc. 2017, 31, 4558–4567. [Google Scholar] [CrossRef]
- Iiboshi, T.; Hanada, K.; Fukuda, T.; Yonehara, S.; Sasaki, T.; Chayama, K. Value of cytodiagnosis using endoscopic nasopancreatic drainage for early diagnosis of pancreatic cancer: Establishing a new method for the early detection of pancreatic carcinoma in situ. Pancreas 2012, 41, 523–529. [Google Scholar] [CrossRef]
- Takeda, Y.; Matsumoto, K.; Kurumi, H.; Koda, H.; Yamashita, T.; Onoyama, T.; Kawata, S.; Horie, Y.; Isomoto, H. Efficacy and safety of pancreatic juice cytology by using synthetic secretin in the diagnosis of pancreatic ductal adenocarcinoma. Dig. Endosc. 2018, 30, 771–776. [Google Scholar] [CrossRef]
- Matsumoto, K.; Takeda, Y.; Onoyama, T.; Kawata, S.; Kurumi, H.; Koda, H.; Yamashita, T.; Isomoto, H. Endoscopic ultrasound-guided fine-needle aspiration biopsy—Recent topics and technical tips. World J. Clin. Cases 2019, 7, 1775–1783. [Google Scholar] [CrossRef]
- Matsumoto, K.; Hara, K.; Yasuda, I.; Itoi, T.; Kurumi, H.; Matsumoto, S.; Doi, S.; Honjo, M.; Takeda, Y.; Shibuya, J.; et al. Usefulness of a target sample check illuminator in the detection of target specimens in endoscopic ultrasound-guided fine-needle biopsy samples: Multicenter prospective study. Dig. Endosc. 2021, 33, 970–976. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, K.; Takeda, Y.; Harada, K.; Horie, Y.; Yashima, K.; Murawaki, Y. Effect of pancreatic juice cytology and/or endoscopic ultrasound-guided fine-needle aspiration biopsy for pancreatic tumor. J. Gastroenterol. Hepatol. 2014, 29, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Conroy, T.; Hammel, P.; Hebbar, M.; Ben Abdelghani, M.; Wei, A.C.; Raoul, J.-L.; Choné, L.; Francois, E.; Artru, P.; Biagi, J.J.; et al. for the Canadian Cancer Trials Group and the Unicancer-GI–PRODIGE Group. Folfirinox or gemcitabine as adjuvant therapy for pancreatic cancer. N. Engl. J. Med. 2018, 379, 2395–2406. [Google Scholar] [CrossRef] [PubMed]
- Versteijne, E.; Suker, M.; Groothuis, K.; Akkermans-Vogelaar, J.M.; Besselink, M.G.; Bonsing, B.A.; Buijsen, J.; Busch, O.R.; Creemers, G.-J.M.; van Dam, R.M.; et al. Dutch Pancreatic Cancer Group. Preoperative chemoradiotherapy versus immediate surgery for resectable and borderline resectable pancreatic cancer: Results of the dutch randomized phase III preopanc trial. J. Clin. Oncol. 2020, 38, 1763–1773. [Google Scholar] [CrossRef]
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouché, O.; Guimbaud, R.; Bécouarn, Y.; Adenis, A.; Raoul, J.L.; Gourgou-Bourgade, S.; de la Fouchardière, C.; et al. Groupe Tumeurs Digestives of Unicancer; PRODIGE Intergroup. Folfirinox versus gemcitabine for metastatic pancreatic cancer. N. Engl. J. Med. 2011, 364, 1817–1825. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| All Cases (n = 234) | |
|---|---|
| Age, in years | |
| Median age | 71 |
| Range | 41–94 |
| Sex | |
| Male | 120 |
| Female | 114 |
| Final diagnosis | |
| Pancreatic ductal adenocarcinoma | 14 |
| Pancreatic cyst or main pancreatic duct dilatation or high tumor marker levels | 152 |
| No abnormality | 60 |
| Others | 8 |
| Age (in years), Sex | Discovery Opportunity Modality | Symptoms | Risk Factors | High Level of Tumor Maker | Abdominal US Finding | Stage (UICC) | ||
|---|---|---|---|---|---|---|---|---|
| MPD Dilatation | Pancreatic Cyst | Pancreatic Mass | ||||||
| 68 M | dyn CT | Body weight loss | Diabetes Smoking | All | − | − | − | IIA |
| 85 F | MRCP | Palpable mass | None | CA19-9 Span-1 | − | − | − | IIA |
| 71 F | US | Abdominal bloating | None | CA19-9 DUPAN2 | − | − | + | IIA |
| 77 F | US | Abdominal bloating | IPMN | CA19-9 Span-1 | + | + | + | IIB |
| 60 F | US | Palpable mass | Smoking | CA19-9 | − | − | + | III |
| 87 M | US | None | Diabetes | CA19-9 Span-1 | + | − | + | IA |
| 64 F | dyn CT | Body weight loss | Smoking Drinking | CA19-9 Span-1 | − | + | − | IIA |
| 76 M | dyn CT | Abdominal pain | None | CA19-9 Span-1 | + | − | − | IIA |
| 85 F | US | Abdominal pain | Diabetes | Span-1 DUPAN2 | − | − | + | IV |
| 69 M | US | None | Smoking | Span-1 DUPAN2 | + | − | + | IV |
| 68 F | US | Abdominal pain | None | None | − | − | + | IIB |
| 76 F | US | Abdominal pain | None | Span-1 DUPAN2 | + | − | + | IV |
| 66 M | US | Abdominal pain | Smoking Drinking | All | + | − | + | IV |
| 63 M | MRCP | None | IPMN | None | − | + | − | IIA |
| Odds Ratio | 95% Confidence Interval | p-Value | ||
|---|---|---|---|---|
| ×1 Abdominal pain | 1.942 | 0.259 | 14.557 | 0.518 |
| ×14 CA19-9 | 5.042 | 0.57 | 44.59 | 0.146 |
| ×15 Span-1 | 15.752 | 1.703 | 145.721 | 0.015 |
| ×16 DUPAN-II | 2.686 | 0.309 | 23.338 | 0.37 |
| ×18 Pancreatic cyst | 0.391 | 0.016 | 9.443 | 0.563 |
| ×19 Pancreatic mass | 37.534 | 3.564 | 395.254 | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsumoto, K.; Kushiyama, Y.; Izumi, A.; Ohnishi, K.; Miura, M.; Ohuchi, Y.; Hori, I.; Nakamura, T.; Hori, K.; Koshino, K.; et al. Usefulness of Practitioner-Led Pancreatic Cancer Screening. Diagnostics 2022, 12, 2257. https://doi.org/10.3390/diagnostics12092257
Matsumoto K, Kushiyama Y, Izumi A, Ohnishi K, Miura M, Ohuchi Y, Hori I, Nakamura T, Hori K, Koshino K, et al. Usefulness of Practitioner-Led Pancreatic Cancer Screening. Diagnostics. 2022; 12(9):2257. https://doi.org/10.3390/diagnostics12092257
Chicago/Turabian StyleMatsumoto, Kazuya, Yoshinori Kushiyama, Akio Izumi, Koji Ohnishi, Masahiko Miura, Yasufumi Ohuchi, Ikuko Hori, Tomonori Nakamura, Kotaro Hori, Kenji Koshino, and et al. 2022. "Usefulness of Practitioner-Led Pancreatic Cancer Screening" Diagnostics 12, no. 9: 2257. https://doi.org/10.3390/diagnostics12092257