
Endoscopic Submucosal Dissection in Patients with Early Gastric Cancer in the Remnant Stomach
 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Practice of ESD and Follow-Up
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Patient and Lesion Characteristics
3.2. ESD Outcomes
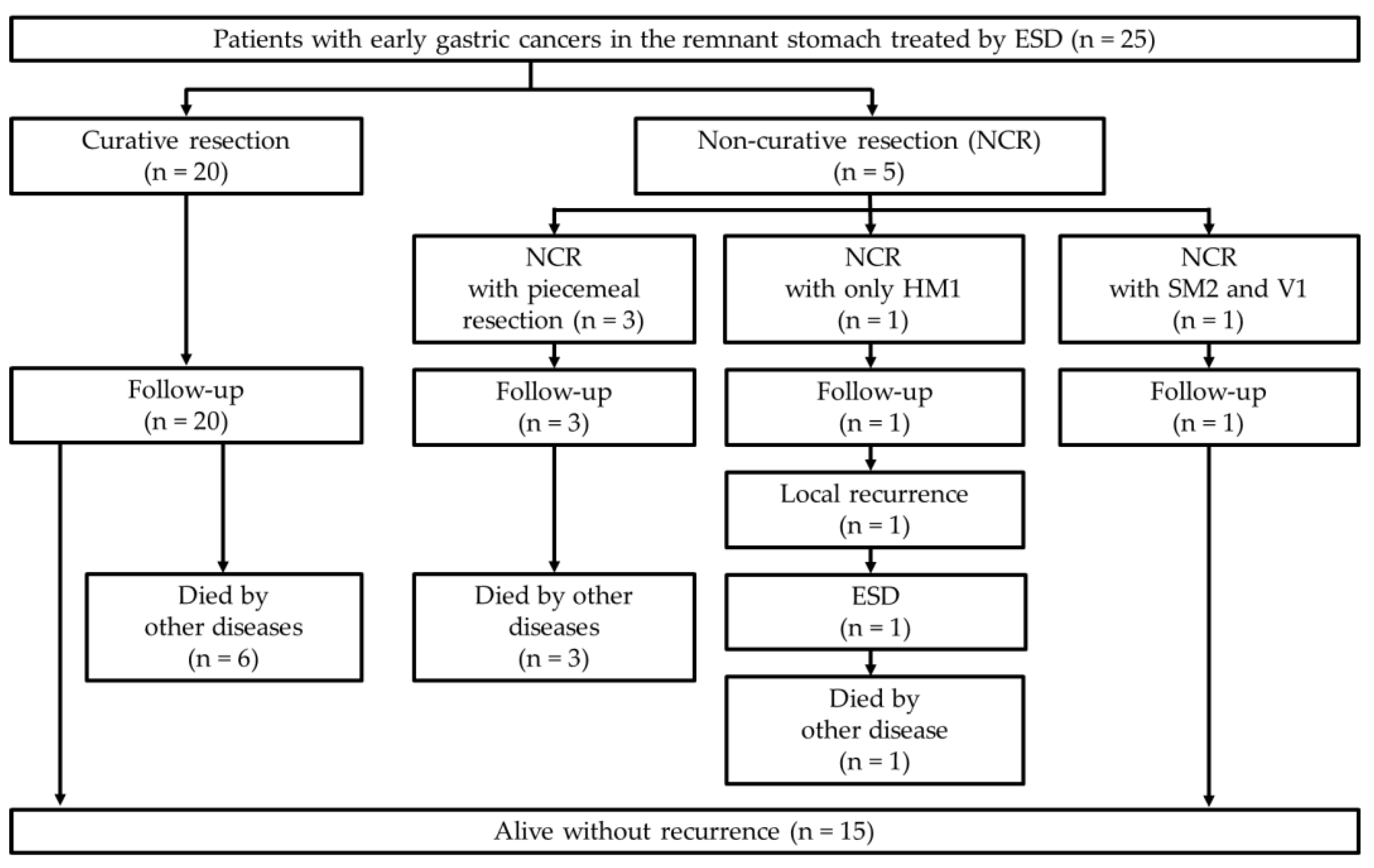
3.3. Long-Term Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Japanese Gastric Cancer Association. Japanese Classification of Gastric Carcinoma, 15th ed.; Kanehara Publisher: Tokyo, Japan, 2017. [Google Scholar]
- Hanyu, T.; Wakai, A.; Ishikawa, T.; Ichikawa, H.; Kameyama, H.; Wakai, T. Carcinoma in the remnant stomach during long-term follow-up after distal gastrectomy for gastric cancer: Analysis of cumulative incidence and associated risk factors. World J. Surg. 2018, 42, 782–787. [Google Scholar] [CrossRef] [PubMed]
- Greene, F.L. Management of gastric remnant carcinoma based on the results of a 15-year endoscopic screening program. Ann. Surg. 1996, 223, 701–706. [Google Scholar] [CrossRef] [PubMed]
- Ahn, H.S.; Kim, J.W.; Yoo, M.W.; Park, D.J.; Lee, H.J.; Lee, K.U.; Yang, H.K. Clinicopathological features and surgical outcomes of patients with remnant gastric cancer after a distal gastrectomy. Ann. Surg. Oncol. 2008, 15, 1632–1639. [Google Scholar] [CrossRef] [PubMed]
- Hirasaki, S.; Kanzaki, H.; Matsubara, M.; Fujita, K.; Matsumura, S.; Suzuki, S. Treatment of gastric remnant cancer post distal gastrectomy by endoscopic submucosal dissection using an insulation-tipped diathermic knife. World J. Gastroenterol. 2008, 14, 2550–2555. [Google Scholar] [CrossRef]
- Takenaka, R.; Kawahara, Y.; Okada, H.; Tsuzuki, T.; Yagi, S.; Kato, J.; Ohara, N.; Yoshino, T.; Imagawa, A.; Fujiki, S.; et al. Endoscopic submucosal dissection for cancers of the remnant stomach after distal gastrectomy. Gastrointest Endosc. 2008, 7, 359–363. [Google Scholar] [CrossRef]
- Lee, J.Y.; Min, B.H.; Lee, J.G.; Noh, D.; Lee, J.H.; Rhee, P.L.; Kim, J.J. Endoscopic submucosal dissection for early gastric neoplasia occurring in the remnant stomach after distal gastrectomy. Clin. Endosc. 2016, 49, 182–186. [Google Scholar] [CrossRef]
- Nonaka, S.; Oda, I.; Makazu, M.; Haruyama, S.; Abe, S.; Suzuki, H.; Yoshinaga, S.; Nakajima, T.; Kushima, R.; Saito, Y. Endoscopic submucosal dissection for early gastric cancer in the remnant stomach after gastrectomy. Gastrointest Endosc. 2013, 78, 63–72. [Google Scholar] [CrossRef]
- Ojima, T.; Takifuji, K.; Nakamura, M.; Nakamori, M.; Katsuda, M.; Iida, T.; Hayata, K.; Iwahashi, M.; Yamaue, H. Endoscopic submucosal dissection for gastric tumors in various types of remnant stomach. Endoscopy 2014, 46, 645–649. [Google Scholar] [CrossRef]
- Yabuuchi, Y.; Kakushima, N.; Takizawa, K.; Tanaka, M.; Kawata, N.; Yoshida, M.; Kishida, Y.; Ito, S.; Imai, K.; Ishiwatari, H.; et al. Short- and long-term outcomes of endoscopic submucosal dissection for early gastric cancer in the remnant stomach after gastrectomy. J. Gastroenterol. 2019, 54, 511–520. [Google Scholar] [CrossRef]
- Tanaka, S.; Toyonaga, T.; Morita, Y.; Fujita, T.; Yoshizaki, T.; Kawara, F.; Wakahara, C.; Obata, D.; Sakai, A.; Ishida, T.; et al. Endoscopic submucosal dissection for early gastric cancer in anastomosis site after distal gastrectomy. Gastric Cancer 2014, 17, 371–376. [Google Scholar] [CrossRef]
- Nishide, N.; Ono, H.; Kakushima, N.; Takizawa, K.; Tanaka, M.; Matsubayashi, H.; Yamaguchi, Y. Clinical outcomes of endoscopic submucosal dissection for early gastric cancer in remnant stomach or gastric tube. Endoscopy. 2012, 44, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2018 (5th edition). Gastric Cancer 2021, 24, 1–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, J.; Hikichi, T.; Watanabe, K.; Hashimoto, M.; Kato, T.; Takagi, T.; Suzuki, R.; Sugimoto, M.; Takasumi, M.; Sato, Y.; et al. Efficacy of sodium carboxymethylcellulose compared to sodium hyaluronate as submucosal injectant for gastric endoscopic submucosal dissection: A randomized controlled trial. Digestion 2021, 102, 753–759. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, K.; Hikichi, T.; Nakamura, J.; Takagi, T.; Suzuki, R.; Sugimoto, M.; Waragai, Y.; Kikuchi, H.; Konno, N.; Asama, H.; et al. Endoscopic submucosal dissection for early gastric cancer in very elderly patients age 85 or older. Endosc. Int. Open 2017, 5, E17–E24. [Google Scholar] [CrossRef] [Green Version]
- Kikuchi, H.; Hikichi, T.; Watanabe, K.; Nakamura, J.; Takagi, T.; Suzuki, R.; Sugimoto, M.; Waragai, Y.; Konno, N.; Asama, H.; et al. Efficacy and safety of sedation during endoscopic submucosal dissection of gastric cancers using a comparative trial of propofol versus midazolam. Endosc. Int. Open 2018, 6, E51–E57. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, K.; Hikichi, T.; Sato, M.; Nakamura, J.; Obara, K.; Ohira, H. Change in gastric emptying eight weeks after endoscopic submucosal dissection in patients with early gastric cancer. Endosc. Int. Open 2016, 4, E597–E602. [Google Scholar] [CrossRef] [Green Version]
- Hikichi, T.; Sato, M.; Watanabe, K.; Nakamura, J.; Takagi, T.; Suzuki, R.; Sugimoto, M.; Waragai, Y.; Kikuchi, H.; Konno, N.; et al. Oral rabeprazole administration on a procedure day suppresses bleeding after endoscopic submucosal dissection for gastric neoplasms. Fukushima J. Med. Sci. 2014, 60, 68–74. [Google Scholar] [CrossRef] [Green Version]
- Hashimoto, M.; Hikichi, T.; Nakamura, J.; Watanabe, K.; Takasumi, M.; Kato, T.; Suzuki, R.; Sugimoto, M.; Irie, H.; Takagi, T.; et al. Clinical characteristics of intramucosal gastric cancers with lymphovascular invasion resected by endoscopic submucosal dissection. Digestion 2021, 102, 546–553. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Hatta, W.; Gotoda, T.; Oyama, T.; Kawata, N.; Takahashi, A.; Yoshifuku, Y.; Hoteya, S.; Nakagawa, M.; Hirano, M.; Esaki, M.; et al. A scoring system to stratify curability after endoscopic submucosal dissection for early gastric cancer: “eCura system”. Am. J. Gastroenterol. 2017, 112, 874–881. [Google Scholar] [CrossRef]
- Iwai, N.; Dohi, O.; Naito, Y.; Inada, Y.; Fukui, A.; Takayama, S.; Ogita, K.; Terasaki, K.; Nakano, T.; Ueda, T.; et al. Impact of the Charlson comorbidity index and prognostic nutritional index on prognosis in patients with early gastric cancer after endoscopic submucosal dissection. Dig. Endosc. 2018, 30, 616–623. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients/lesions, n | 25/27 * |
| Age, median (range) | 74 (63–89) |
| Sex, male/female | 19/6 |
| Height, median (range), m | 1.59 (1.35–1.76) |
| Weight, median (range), kg | 49.7 (35.2–74.6) |
| Body mass index, median (range) | 20.0 (16.1–25.8) |
| Anti-H. pylori IgG antibodies (positive/negative/not tested) | 8/16/1 |
| Intake of antithrombotics, n (%) | 6 (24) |
| Charlson comorbidity index (low/medium/high/very high) | 14/9/2/0 |
| Cause leading to gastrectomy, n (%) | |
| Gastric cancer | 20 (80) |
| Gastric ulcer | 2 (8) |
| Duodenal ulcer | 1 (4) |
| Gastric polyp | 1 (4) |
| IPMC | 1 (4) |
| Type of gastrectomy, n (%) | |
| Distal | 21 (84) |
| Proximal | 3 (12) |
| Pancreaticoduodenectomy | 1 (4) |
| Period from previous gastrectomy to index ESD, median (range), month | 168 (24–552) |
| Lesion circumference, n (%) | |
| Anterior wall | 7 (25.9) |
| Greater curvature | 3 (11.1) |
| Posterior wall | 5 (18.5) |
| Lesser curvature | 12 (44.4) |
| Suture line involvement, n (%) | 12 (44.4) |
| Anastomosis involvement, n (%) | 1 (3.7) |
| Microscopic type, n (%) | |
| 0–I | 3 (11.1) |
| 0–IIa | 13 (48.1) |
| 0–IIc | 9 (33.3) |
| Mixed | 2 (7.4) |
| Procedure time, median (range), min | 80 (42–307) |
| En bloc resection, n (%) | 24 (88.9) |
| R0 resection, n (%) | 23 (85.2) |
| Tumor diameter, median (range), mm | 12 (4-40) |
| Specimen diameter, median (range), mm | 37.5 (18–82) |
| Histologic type, n (%) | |
| pap | 2 (7.4) |
| tub1 | 23 (85.2) |
| tub2 | 2 (7.4) |
| Tumor depth, n (%) | |
| M | 24 (88.9) |
| SM1 | 2 (7.4) |
| SM2 | 1 (3.7) |
| Ulcer finding, n (%) | 2 (7.4) |
| Lymphatic invasion, n | 0 |
| Vascular invasion, n (%) | 1 (3.7) |
| Horizontal margin, n (%) | |
| Positive or unevaluated | 2 (7.4) |
| Negative | 25 (92.6) |
| Vertical margin, n (%) | |
| Positive or unevaluated | 2 (7.4) |
| Negative | 25 (92.6) |
| Curative resection, n (%) | 22 (81.5) |
| Procedure-related adverse events, n | 0 |
| Suture Line Involvement * (n = 12) | Involving Neither Suture Line Nor Anastomosis * (n = 14) | Anastomosis Involvement (n = 1) | p Value Between Lesions Involving Suture Line and Lesions Neither Involving Suture Line nor Anastomoses | |
|---|---|---|---|---|
| Tumor diameter, median (range), mm | 15.5 (7–40) | 11.0 (4–25) | 15 | 0.167 |
| Specimen diameter *, median (range), mm | 35.5 (22–55) | 35.0 (18–49) | 40 | 0.591 |
| Procedure time *, median (range), min | 93.5 (56–307) | 69 (42–210) | 80 | 0.381 |
| En bloc resection, n (%) | 11 (91.7) | 12 (85.7) | 1 | 1.000 |
| R0 resection, n (%) | 11 (91.7) | 11 (78.6) | 1 | 0.598 |
| Curative resection, n (%) | 11 (91.7) | 10 (71.4) | 1 | 0.330 |
| Age | Sex | Microscopic Type | Anastomosis or Suture Line Involvement | Depth | Tumor Diameter (mm) | Histology | Reasons of Non- Curative Resection | Additional Treatment | Recurrence | Prognosis |
|---|---|---|---|---|---|---|---|---|---|---|
| 70 | M | Mixed | None | M | - | tub1 | Piecemeal resection | None | None | Died 162 months after ESD, due to prostate cancer |
| 79 | M | 0–IIa | None | SM1 | 13 | tub2 | Piecemeal resection, VMX | None | None | Died 152 months after ESD, due to unknown cause |
| 66 | M | 0–IIc | Suture line | M | 28 | tub1 | Piecemeal resection | None | None | Died 48 months after ESD, due to unknown cause |
| 79 | F | 0–IIa | None | SM2 | 25 | tub2 > por | SM2, V1 | None | None | Alive for 96 months |
| 83 | M | 0–IIa | None | M | 18 | tub1 | HM1 | None | Local recurrence after 8 months (resected by ESD) | Died 12 months after the second ESD, due to lung cancer |
| Follow-up period, mean (range), month | 48 (5–162) |
| Local recurrence, n (%) | 1 (4) |
| Distant metastasis, n | 0 |
| Metachronous cancer, n | 0 |
| Death by gastric cancer, n | 0 |
| Death by other disease, n (%) | 10 (40) |
| First Author (Published Year) | No. of Patients | No. of Lesions | Mean or Median Age, Year | Lesion Located on the Suture Line, % (n) | En bloc Resection Rate, % (n) | R0 Resection Rate, % (n) | Adverse Events, % (n) | 5-Year OS Rate, % | 5-Year Cause-Specific Survival Rate, % |
|---|---|---|---|---|---|---|---|---|---|
| Hirasaki (2008) [5] | 17 | 17 | 73.1 | N/A | 100 (17) | 82.4 (14) | 17.6 (3) | N/A | N/A |
| Takenaka (2008) [6] | 30 | 31 | 73 | 38.7 (12) | 96.8 (30) | 74.2 (23) | 12.9 (4) | N/A | N/A |
| Lee (2010) [7] | 13 | 13 | 63 | 46.2 (6) | 100 (13) | 92.3 (12) | 0 | N/A | N/A |
| Nonaka (2013) [8] | 128 | 139 | 69.6 | 30.2 (42) | 94.2 (131) | 84.9 (118) | 2.9 (4) | 87.3 | 100 |
| Ojima (2014) [9] | 43 | 49 | 70 | 16.3 (8) | 100 (49) | 85.7 (42) | 14.3 (7) | N/A | N/A |
| Yabuuchi (2019) * [10] | 136 | 165 | 74 | 22.4 (37) | 95.5 (150) | 84.7 (133) | 21.0 (33) | 88.4 | 97.6 |
| Present study | 25 | 27 | 74 | 44.4 (12) | 88.9 (24) | 85.2 (23) | 0 | 71.0 | 100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murakami, M.; Hikichi, T.; Nakamura, J.; Hashimoto, M.; Kato, T.; Kobashi, R.; Yanagita, T.; Suzuki, R.; Sugimoto, M.; Sato, Y.; et al. Endoscopic Submucosal Dissection in Patients with Early Gastric Cancer in the Remnant Stomach. Diagnostics 2022, 12, 2480. https://doi.org/10.3390/diagnostics12102480
Murakami M, Hikichi T, Nakamura J, Hashimoto M, Kato T, Kobashi R, Yanagita T, Suzuki R, Sugimoto M, Sato Y, et al. Endoscopic Submucosal Dissection in Patients with Early Gastric Cancer in the Remnant Stomach. Diagnostics. 2022; 12(10):2480. https://doi.org/10.3390/diagnostics12102480
Chicago/Turabian StyleMurakami, Mai, Takuto Hikichi, Jun Nakamura, Minami Hashimoto, Tsunetaka Kato, Ryoichiro Kobashi, Takumi Yanagita, Rei Suzuki, Mitsuru Sugimoto, Yuki Sato, and et al. 2022. "Endoscopic Submucosal Dissection in Patients with Early Gastric Cancer in the Remnant Stomach" Diagnostics 12, no. 10: 2480. https://doi.org/10.3390/diagnostics12102480