

Clinical Utility of Quantitative Parameters of Salivary Gland Scintigraphy for Diagnosing Burning Mouth Syndrome
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Salivary Gland Scintigraphy
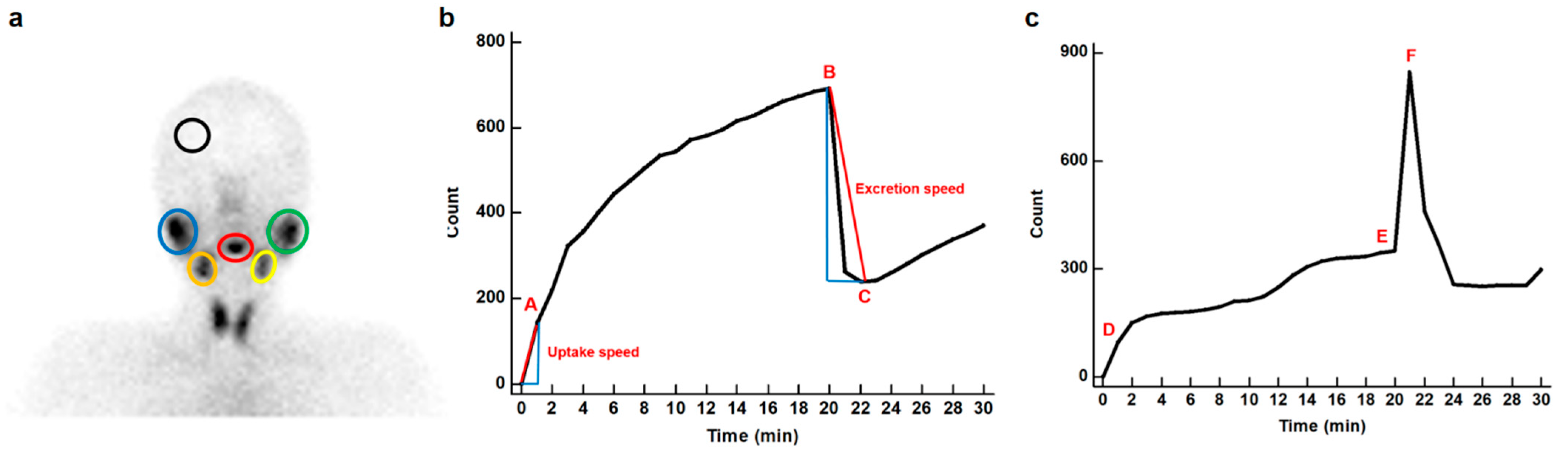
2.3. Image Data Analysis
2.4. Statistical Analysis
3. Results
3.1. Participants
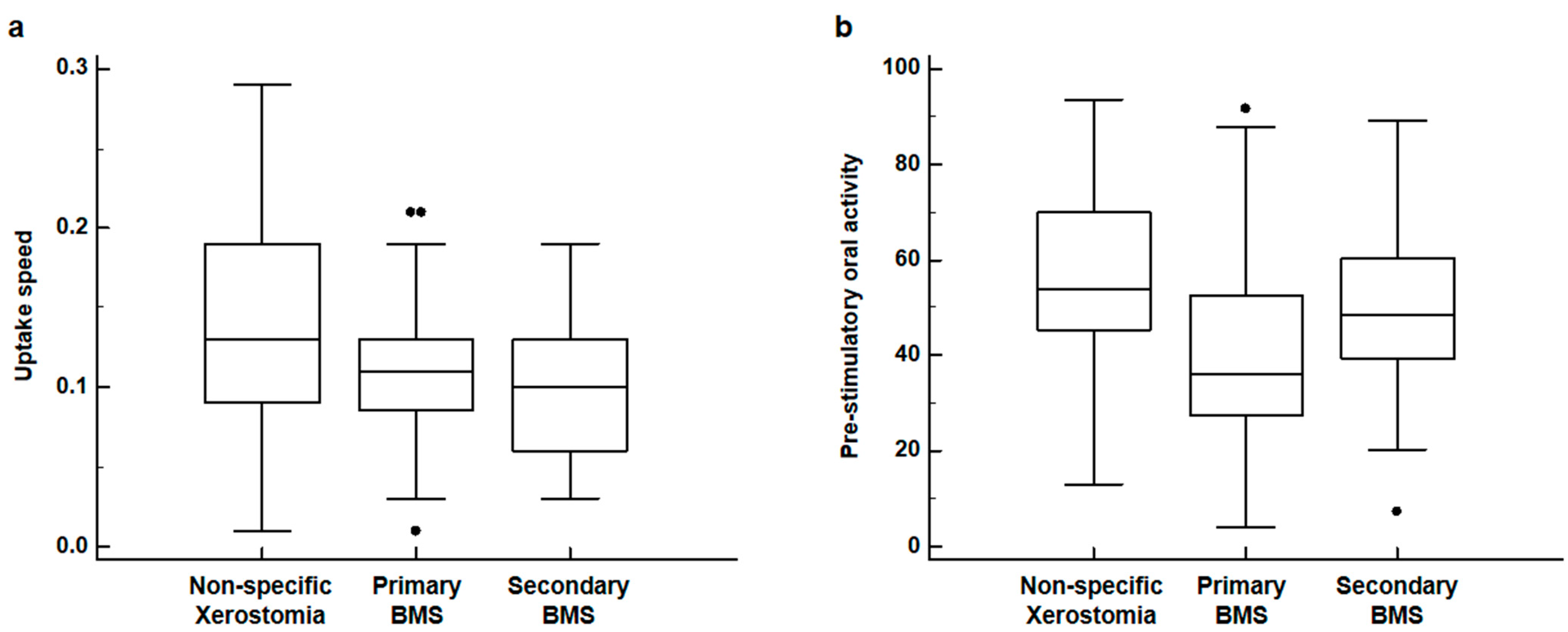
3.2. Comparison of Salivary Gland Scintigraphy Parameters
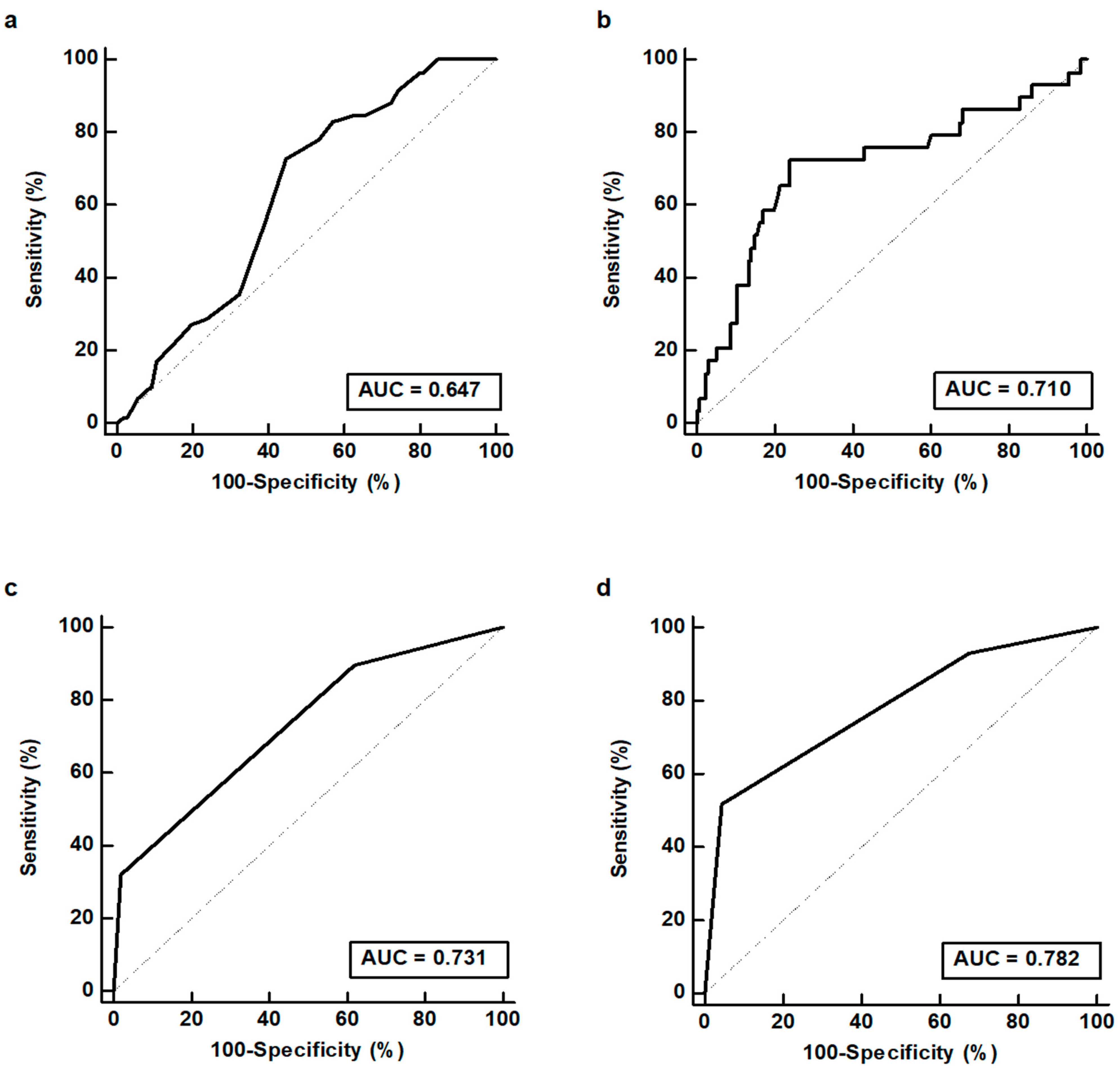
3.3. Diagnostic Ability of Salivary Gland Scintigraphy Parameters
3.4. Salivary Gland Scintigraphy Scoring System
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Teruel, A.; Patel, S. Burning mouth syndrome: A review of etiology, diagnosis, and management. Gen. Dent. 2019, 67, 24–29. [Google Scholar] [PubMed]
- Aravindhan, R.; Vidyalakshmi, S.; Kumar, M.S.; Satheesh, C.; Balasubramanium, A.M.; Prasad, V.S. Burning mouth syndrome: A review on its diagnostic and therapeutic approach. J. Pharm. Bioallied Sci. 2014, 6, S21–S25. [Google Scholar] [CrossRef] [PubMed]
- Scala, A.; Checchi, L.; Montevecchi, M.; Marini, I.; Giamberardino, M.A. Update on burning mouth syndrome: Overview and patient management. Crit. Rev. Oral Biol. Med. 2003, 14, 275–291. [Google Scholar] [CrossRef] [PubMed]
- Bender, S.D. Burning Mouth Syndrome. Dent. Clin. N. Am 2018, 62, 585–596. [Google Scholar] [CrossRef]
- Yilmaz, Z.; Renton, T.; Yiangou, Y.; Zakrzewska, J.; Chessell, I.P.; Bountra, C.; Anand, P. Burning mouth syndrome as a trigeminal small fibre neuropathy: Increased heat and capsaicin receptor TRPV1 in nerve fibres correlates with pain score. J. Clin. Neurosci. 2007, 14, 864–871. [Google Scholar] [CrossRef]
- Puhakka, A.; Forssell, H.; Soinila, S.; Virtanen, A.; Röyttä, M.; Laine, M.; Tenovuo, O.; Teerijoki-Oksa, T.; Jääskeläinen, S.K. Peripheral nervous system involvement in primary burning mouth syndrome--results of a pilot study. Oral Dis. 2016, 22, 338–344. [Google Scholar] [CrossRef]
- Carreño-Hernández, I.; Cassol-Spanemberg, J.; de Rivera-Campillo, E.R.; Estrugo-Devesa, A.; López-López, J. Is burning mouth syndrome a neuropathic pain disorder? A systematic review. J. Oral Facial Pain Headache 2021, 35, 218–229. [Google Scholar] [CrossRef]
- Russo, M.; Crafa, P.; Guglielmetti, S.; Franzoni, L.; Fiore, W.; Di Mario, F. Burning mouth syndrome etiology: A narrative review. J. Gastrointest. Liver Dis. 2022, 31, 223–228. [Google Scholar] [CrossRef]
- Aljanobi, H.; Sabharwal, A.; Krishnakumar, B.; Kramer, J.M. Is it Sjögren’s syndrome or burning mouth syndrome? Distinct pathoses with similar oral symptoms. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2017, 123, 482–495. [Google Scholar] [CrossRef]
- Lee, Y.C.; Hong, I.K.; Na, S.Y.; Eun, Y.G. Evaluation of salivary function in patients with burning mouth syndrome. Oral Dis. 2015, 21, 308–313. [Google Scholar] [CrossRef]
- Aitken-Saavedra, J.; Tarquinio, S.B.; da Rosa, W.O.; Gomes, A.P.; da Silva, A.F.; Fernandez, M.S.; Moreira, A.G.; Maturana-Ramirez, A.; Vasconcellos, A.C. Salivary characteristics may be associated with burning mouth syndrome? J. Clin. Exp. Dent. 2021, 13, e542–e548. [Google Scholar] [CrossRef] [PubMed]
- Castillo-Felipe, C.; Franco-Martínez, L.; Tvarijonaviciute, A.; Lopez-Jornet, P.; Lamy, E. Proteomics-based identification of salivary changes in patients with burning mouth syndrome. Biology 2021, 10, 392. [Google Scholar] [CrossRef] [PubMed]
- Aitken-Saavedra, J.; Tarquinio, S.B.; Kinalski, M.; Haubman, D.; Martins, M.W.; Vasconcelos, A.C. Salivary characteristics in burning mouth syndrome: A systematic review. Minerva Dent. Oral Sci. 2022, 71, 233–241. [Google Scholar] [CrossRef]
- Chen, Y.C.; Chen, H.Y.; Hsu, C.H. Recent Advances in Salivary Scintigraphic Evaluation of Salivary Gland Function. Diagnostics 2021, 11, 1173. [Google Scholar] [CrossRef]
- Vinagre, F.; Santos, M.J.; Prata, A.; da Silva, J.C.; Santos, A.I. Assessment of salivary gland function in Sjögren’s syndrome: The role of salivary gland scintigraphy. Autoimmun. Rev. 2009, 8, 672–676. [Google Scholar] [CrossRef]
- Booker, J.; Howarth, D.; Taylor, L.; Voutnis, D.; Sutherland, D. Appropriate utilization of semi-quantitative analysis in salivary scintigraphy. Nucl. Med. Commun. 2004, 25, 1203–1210. [Google Scholar] [CrossRef]
- Son, H.; Lee, S.M.; Yoon, R.G.; Lee, H.; Lee, I.; Kim, S.; Chung, W.Y.; Lee, J.W. Effect of selenium supplementation for protection of salivary glands from iodine-131 radiation damage in patients with differentiated thyroid cancer. Hell. J. Nucl. Med. 2017, 20, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Wu, J.; Zhao, L.; Liu, W.; Wei, J.; Hu, Z.; Hao, B.; Wu, H.; Sun, L.; Chen, H. Quantitative evaluation of salivary gland scintigraphy in Sjögren’s syndrome: Comparison of diagnostic efficacy and relationship with pathological features of the salivary glands. Ann. Nucl. Med. 2020, 34, 289–298. [Google Scholar] [CrossRef]
- Lee, Y.C.; Song, R.; Yang, Y.J.; Eun, Y.G. Prevalence and Predictors of Sjögren’s Syndrome in Patients with Burning Mouth Symptoms. J. Oral Facial Pain Headache 2018, 32, 91–96. [Google Scholar] [CrossRef]
- Nadal, M.; Levy, M.; Bakhsh, A.; Joly, A.; Maruani, A.; Vaillant, L.; Erra, B.; Samimi, M. Salivary scintigraphy for Sjögren’s syndrome in patients with xerostomia: A retrospective study. Oral Dis 2018, 24, 552–560. [Google Scholar] [CrossRef]
- The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia 2013, 33, 629–808. [CrossRef] [PubMed]
- Rouleau, T.S.; Shychuk, A.J.; Kayastha, J.; Lockhart, P.B.; Nussbaum, M.L.; Brennan, M.T. A retrospective, cohort study of the prevalence and risk factors of oral burning in patients with dry mouth. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2011, 111, 720–725. [Google Scholar] [CrossRef] [PubMed]
- Bujang, M.A.; Adnan, T.H. Requirements for minimum sample size for sensitivity and specificity analysis. J. Clin. Diagn Res. 2016, 10, YE01–YE06. [Google Scholar] [CrossRef] [PubMed]
- Nishiyama, S.; Miyawaki, S.; Yoshinaga, Y. A study to standardize quantitative evaluation of parotid gland scintigraphy in patients with Sjögren’s syndrome. J. Rheumatol. 2006, 33, 2470–2474. [Google Scholar]
- Dugonjić, S.; Stefanović, D.; Ethurović, B.; Spasić-Jokić, V.; Ajdinović, B. Evaluation of diagnostic parameters from parotid and submandibular dynamic salivary glands scintigraphy and unstimulated sialometry in Sjögren’s syndrome. Hell. J. Nucl. Med. 2014, 17, 116–122. [Google Scholar]
- Aung, W.; Murata, Y.; Ishida, R.; Takahashi, Y.; Okada, N.; Shibuya, H. Study of quantitative oral radioactivity in salivary gland scintigraphy and determination of the clinical stage of Sjögren’s syndrome. J. Nucl. Med. 2001, 42, 38–43. [Google Scholar]
- Klasser, G.D.; Grushka, M.; Su, N. Burning Mouth Syndrome. Oral Maxillofac. Surg. Clin. N. Am. 2016, 28, 381–396. [Google Scholar] [CrossRef]
- López-Jornet, P.; Collado, Y.; Zambudio, A.; Pons-Fuster, E.; Castillo Felipe, C.; Tvarijonaviciute, A. Chemosensory Function in Burning Mouth Syndrome a Comparative Cross-Sectional Study. Nutrients 2021, 13, 722. [Google Scholar] [CrossRef]
- Eliav, E.; Kamran, B.; Schaham, R.; Czerninski, R.; Gracely, R.H.; Benoliel, R. Evidence of chorda tympani dysfunction in patients with burning mouth syndrome. J. Am. Dent. Assoc. 2007, 138, 628–633. [Google Scholar] [CrossRef]
- Bartoshuk, L.M.; Catalanotto, F.; Hoffman, H.; Logan, H.; Snyder, D.J. Taste damage (otitis media, tonsillectomy and head and neck cancer), oral sensations and BMI. Physiol. Behav. 2012, 107, 516–526. [Google Scholar] [CrossRef]
- Ferreira, J.N.; Hoffman, M.P. Interactions between developing nerves and salivary glands. Organogenesis 2013, 9, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Poon, R.; Su, N.; Ching, V.; Darling, M.; Grushka, M. Reduction in unstimulated salivary flow rate in burning mouth syndrome. Br. Dent. J. 2014, 217, E14. [Google Scholar] [CrossRef] [PubMed]
- Spadari, F.; Venesia, P.; Azzi, L.; Veronesi, G.; Costantino, D.; Croveri, F.; Farronato, D.; Tagliabue, A.; Tettamanti, L. Low basal salivary flow and burning mouth syndrome: New evidence in this enigmatic pathology. J. Oral Pathol. Med. 2015, 44, 229–233. [Google Scholar] [CrossRef] [PubMed]
- Sreebny, L.M. Saliva in health and disease: An appraisal and update. Int. Dent. J. 2000, 50, 140–161. [Google Scholar] [CrossRef] [PubMed]
- de Paula, F.; Teshima, T.H.N.; Hsieh, R.; Souza, M.M.; Nico, M.M.S.; Lourenco, S.V. Overview of Human Salivary Glands: Highlights of Morphology and Developing Processes. Anat. Rec. 2017, 300, 1180–1188. [Google Scholar] [CrossRef]
- Inamochi, Y.; Fueki, K.; Matsuyama, Y.; Yoshida-Kohno, E.; Fujiwara, T.; Wakabayashi, N. Does oral dryness influence pressure pain sensitivity in the oral mucosa of removable denture wearers? Clin. Oral Investig. 2020, 24, 2603–2609. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameters | Primary BMS (n = 29) | Secondary BMS (n = 30) | Non-Specific Xerostomia (n = 105) | p-Value * | |
|---|---|---|---|---|---|
| Uptake ratio | Right parotid | 5.00 (3.45–5.74) | 4.29 (3.75–4.73) | 4.64 (3.78–5.85) | 0.528 |
| Left parotid | 4.78 (3.81–5.82) | 4.72 (4.16–5.13) | 5.05 (3.87–5.95) | 0.822 | |
| Right submandibular | 3.52 (2.97–4.30) | 3.49 (3.06–3.93) | 3.88 (3.08–4.43) | 0.360 | |
| Left submandibular | 3.58 (2.95–4.25) | 3.56 (3.17–3.83) | 3.79 (3.05–4.40) | 0.493 | |
| Maximum accumulation | Right parotid | 76.3 (68.1–82.3) | 80.6 (72.9–88.1) | 76.6 (69.9–84.9) | 0.233 |
| Left parotid | 78.0 (66.8–84.8) | 81.3 (72.7–87.5) | 79.3 (68.9–86.2) | 0.438 | |
| Right submandibular | 48.8 (39.8–66.0) | 61.5 (48.3–74.0) | 57.0 (38.5–71.0) | 0.193 | |
| Left submandibular | 50.6 (40.3–67.2) | 62.1 (49.6–77.8) | 58.6 (40.0–72.5) | 0.225 | |
| Ejection fraction | Right parotid | 43.8 (24.6–47.4) | 31.2 (23.3–36.8) | 33.3 (21.6–46.3) | 0.389 |
| Left parotid | 39.4 (24.5–46.5) | 32.3 (20.8–39.4) | 31.2 (18.5–41.2) | 0.345 | |
| Right submandibular | 19.8 (10.7–30.9) | 21.7 (10.3–33.0) | 26.3 (14.0–34.7) | 0.165 | |
| Left submandibular | 18.5 (8.2–30.7) | 19.2 (8.5–27.4) | 25.0 (13.7–31.9) | 0.195 | |
| Uptake speed | Right parotid | 0.25 (0.14–0.29) | 0.17 (0.10–0.22) | 0.21 (0.13–0.31) | 0.123 |
| Left parotid | 0.19 (0.14–0.28) | 0.17 (0.10–0.24) | 0.20 (0.10–0.30) | 0.420 | |
| Right submandibular | 0.13 (0.11–0.17) | 0.12 (0.07–0.13) | 0.14 (0.09–0.20) | 0.138 | |
| Left submandibular | 0.11 (0.08–0.13) | 0.10 (0.06–0.13) | 0.13 (0.09–0.19) | 0.024 | |
| Excretion speed | Right parotid | 0.51 (0.22–0.72) | 0.38 (0.21–0.57) | 0.42 (0.23–0.73) | 0.692 |
| Left parotid | 0.50 (0.25–0.64) | 0.38 (0.23–0.59) | 0.36 (0.23–0.61) | 0.678 | |
| Right submandibular | 0.27 (0.09–0.50) | 0.37 (0.21–0.59) | 0.44 (0.18–0.64) | 0.159 | |
| Left submandibular | 0.26 (0.08–0.49) | 0.32 (0.11–0.47) | 0.35 (0.18–0.66) | 0.294 | |
| Pre-stimulatory oral activity | 36.0 (27.3–52.7) | 48.6 (39.2–60.3) | 53.8 (45.2–69.9) | <0.001 | |
| Post-stimulatory oral activity | 59.2 (46.4–65.7) | 63.0 (54.4–72.3) | 63.5 (49.1–75.6) | 0.238 | |
| Parameters | BMS | Primary BMS | |||
|---|---|---|---|---|---|
| AUC | 95% CI | AUC | 95% CI | ||
| Uptake ratio | Right parotid | 0.532 | 0.452–0.610 | 0.518 | 0.438–0.596 |
| Left parotid | 0.527 | 0.447–0.605 | 0.509 | 0.429–0.587 | |
| Right submandibular | 0.566 | 0.486–0.643 | 0.536 | 0.457–0.614 | |
| Left submandibular | 0.549 | 0.470–0.627 | 0.512 | 0.433–0.591 | |
| Maximum accumulation | Right parotid | 0.522 | 0.442–0.600 | 0.560 | 0.480–0.637 |
| Left parotid | 0.524 | 0.445–0.602 | 0.536 | 0.457–0.614 | |
| Right submandibular | 0.520 | 0.441–0.599 | 0.567 | 0.487–0.644 | |
| Left submandibular | 0.529 | 0.449–0.607 | 0.553 | 0.473–0.630 | |
| Ejection fraction | Right parotid | 0.504 | 0.425–0.583 | 0.567 | 0.488–0.644 |
| Left parotid | 0.548 | 0.469–0.626 | 0.566 | 0.487–0.622 | |
| Right submandibular | 0.585 | 0.505–0.661 | 0.575 | 0.496–0.651 | |
| Left submandibular | 0.584 | 0.505–0.661 | 0.553 | 0.473–0.630 | |
| Uptake speed | Right parotid | 0.554 | 0.474–0.631 | 0.537 | 0.458–0.615 |
| Left parotid | 0.542 | 0.462–0.620 | 0.513 | 0.434–0.592 | |
| Right submandibular | 0.567 | 0.487–0.644 | 0.513 | 0.433–0.591 | |
| Left submandibular | 0.647 | 0.568–0.711 | 0.586 | 0.507–0.663 | |
| Excretion speed | Right parotid | 0.517 | 0.438–0.596 | 0.523 | 0.444–0.601 |
| Left parotid | 0.530 | 0.451–0.609 | 0.552 | 0.472–0.629 | |
| Right submandibular | 0.580 | 0.500–0.656 | 0.584 | 0.505–0.660 | |
| Left submandibular | 0.574 | 0.494–0.650 | 0.561 | 0.481–0.638 | |
| Pre-stimulatory oral activity | 0.627 | 0.548–0.710 | 0.710 | 0.634–0.778 | |
| Post-stimulatory oral activity | 0.537 | 0.458–0.615 | 0.599 | 0.519–0.674 | |
| Scoring System | BMS | Primary BMS | |||
|---|---|---|---|---|---|
| BMS (+) (n = 59) | BMS (−) * (n = 105) | Primary BMS (+) (n = 29) | Primary BMS (−) † (n = 135) | Total | |
| 0 | 6 (13.0%) | 40 (87.0%) | 2 (4.3%) | 44 (95.7%) | 46 (100.0%) |
| 1 | 34 (35.1%) | 63 (64.9%) | 12 (12.4%) | 85 (87.6%) | 97 (100.0%) |
| 2 | 19 (90.5%) | 2 (9.5%) | 15 (71.4%) | 6 (28.6%) | 21 (100.0%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Byeon, H.K.; Jeong, G.C.; Kim, B.; Lee, Y.; Park, J.H.; Lee, S.M. Clinical Utility of Quantitative Parameters of Salivary Gland Scintigraphy for Diagnosing Burning Mouth Syndrome. Diagnostics 2022, 12, 2256. https://doi.org/10.3390/diagnostics12092256
Byeon HK, Jeong GC, Kim B, Lee Y, Park JH, Lee SM. Clinical Utility of Quantitative Parameters of Salivary Gland Scintigraphy for Diagnosing Burning Mouth Syndrome. Diagnostics. 2022; 12(9):2256. https://doi.org/10.3390/diagnostics12092256
Chicago/Turabian StyleByeon, Hyung Kwon, Geum Cheol Jeong, Beomsoo Kim, Yeongrok Lee, Jae Hong Park, and Sang Mi Lee. 2022. "Clinical Utility of Quantitative Parameters of Salivary Gland Scintigraphy for Diagnosing Burning Mouth Syndrome" Diagnostics 12, no. 9: 2256. https://doi.org/10.3390/diagnostics12092256