

Cellular Concentration of Survivin and Caspase 3 in Habitual Tobacco Chewers with and without Oral Squamous Cell Carcinoma in South Indian Rural Population—A Case Control Study
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Methods
2.2.1. Sample Collection
2.2.2. Buccal Tissue Sample Analysis
2.2.3. Human Survivin Assay
2.2.4. Human Cysteinyl Aspartate Specific Proteinase 3 (Caspase 3) Assay
2.3. Statistical Analysis
3. Results
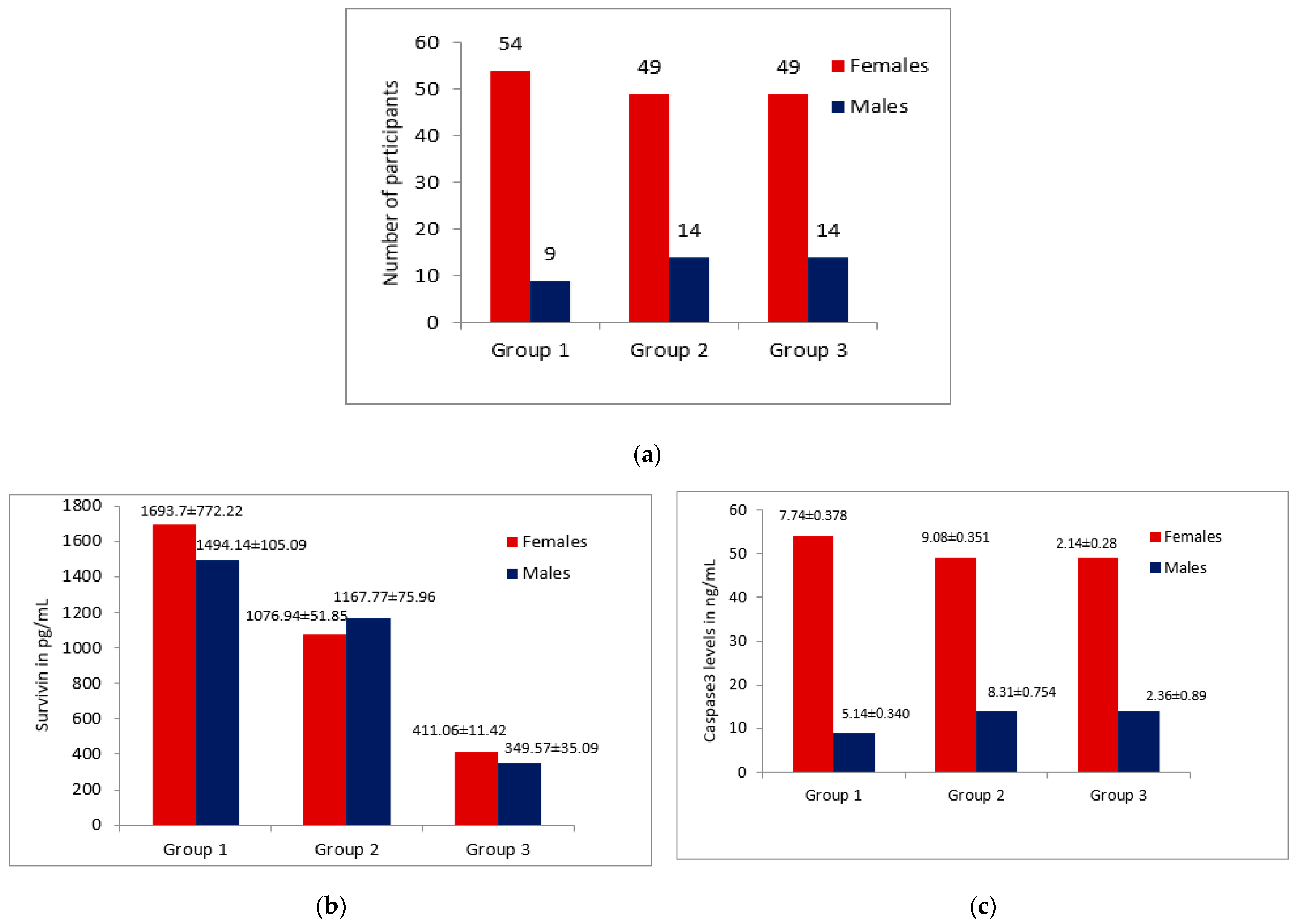
3.1. Patients Characteristic Details
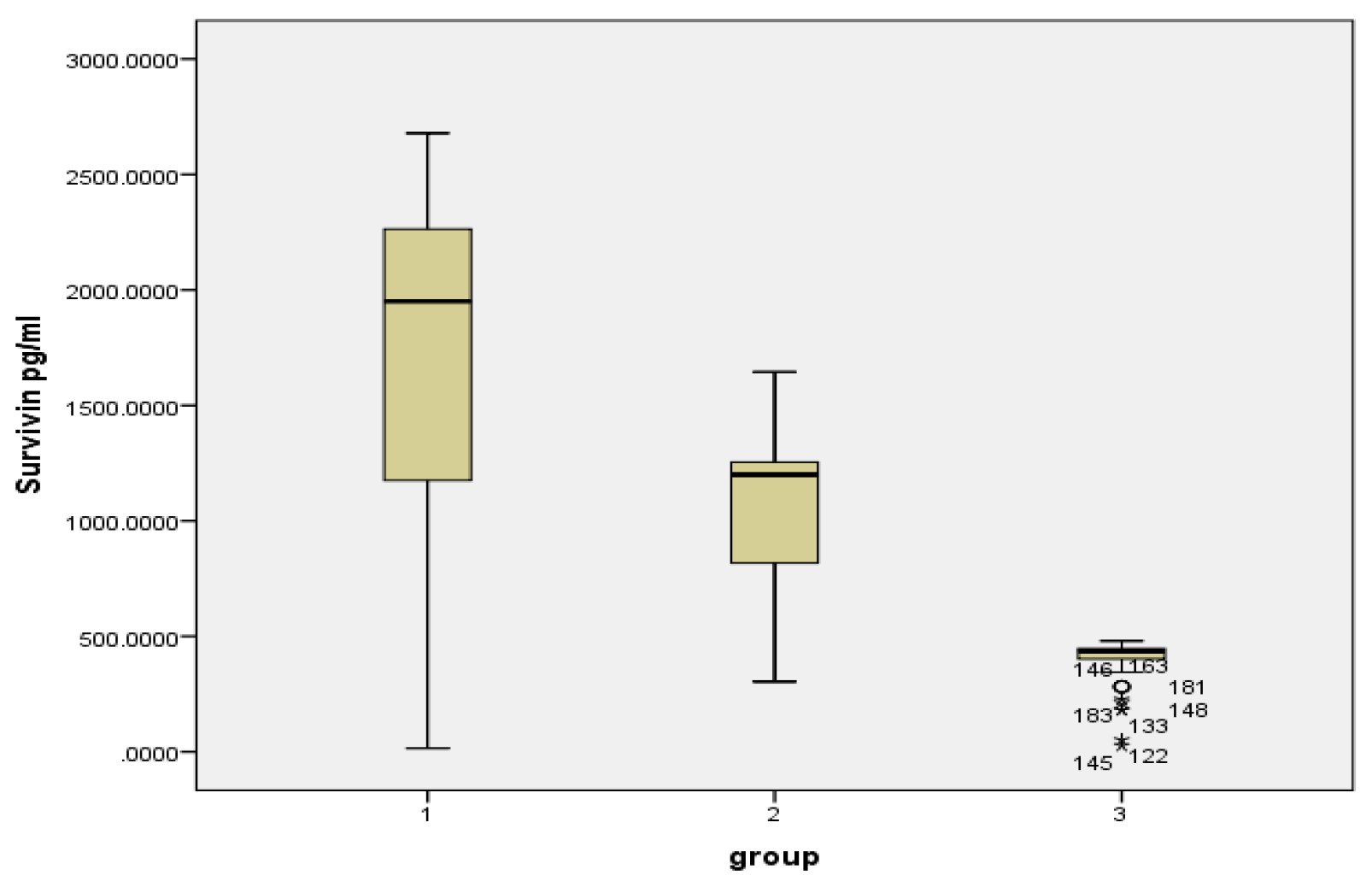
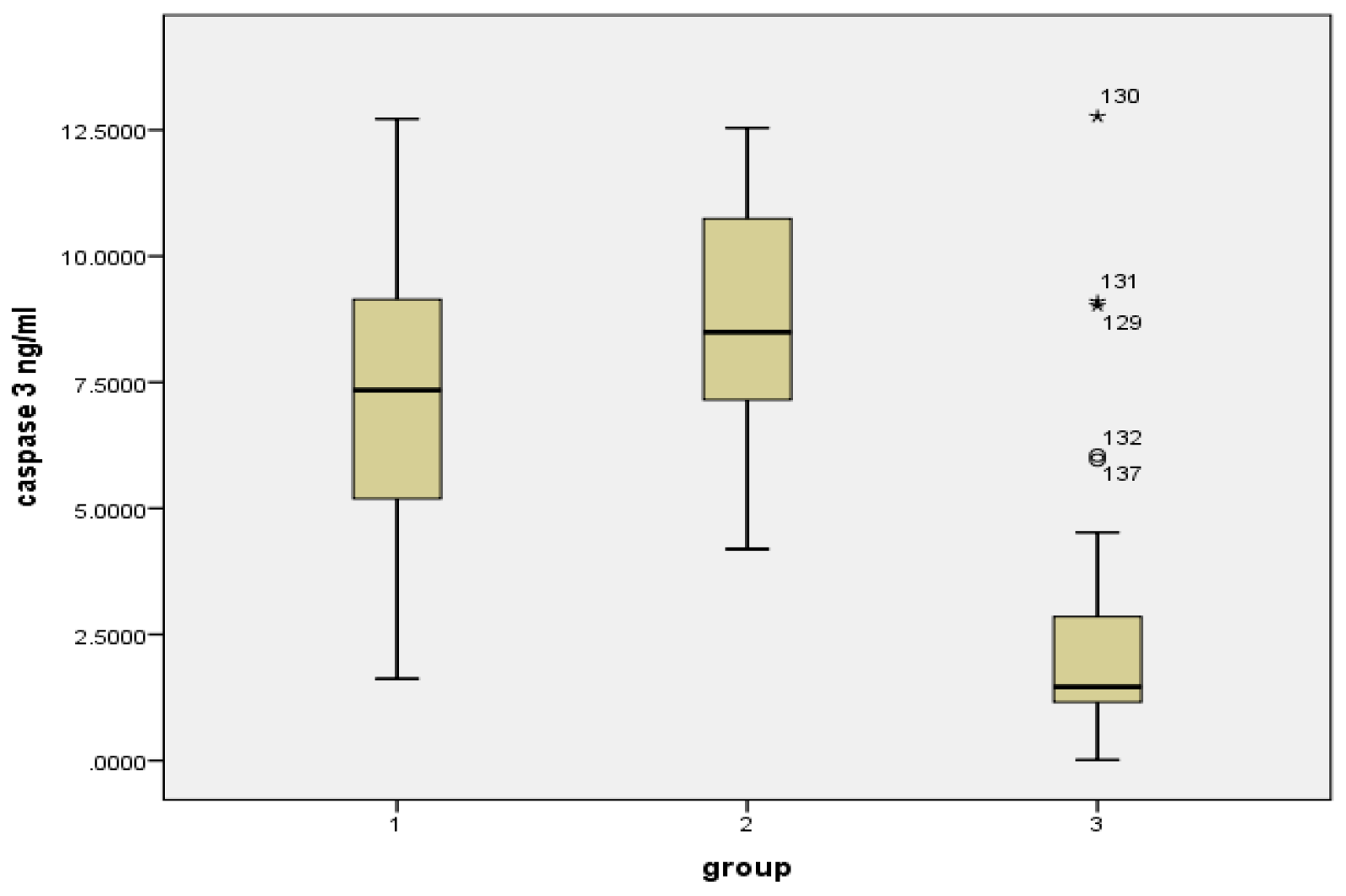
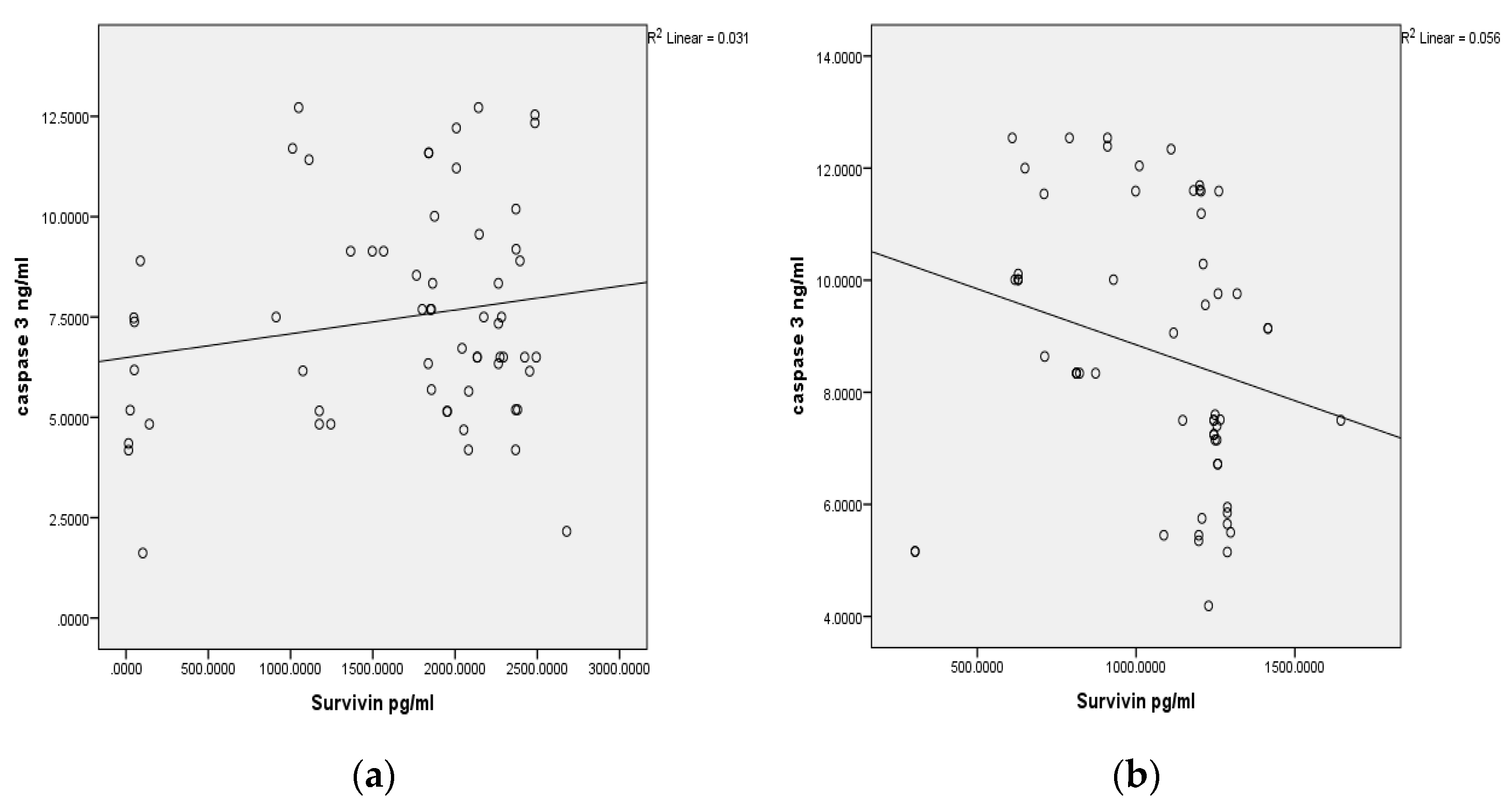
3.2. Survivin and Caspase 3 Analysis
4. Discussion
5. Conclusions
6. Limitations of the Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Campo-Trapero, J.; Cano-Sanchez, J.; Palacios-Sanchez, B.; Sanchez-Gutierrez, J.J.; Gonzalez-Moles, M.A.; BasconesMartinez, A. Update on Molecular Pathology in Oral Cancer and Precancer. Anticancer Res. 2008, 28, 1197–1206. [Google Scholar]
- Mark Lingen, W. Screening for Oral Premalignancy and cancer: What Platform and Which Biomarkers? Cancer Prev. Res. 2010, 3, 1056–1059. [Google Scholar] [CrossRef]
- Rani, M.; Bonu, S.; Jha, P.; Nguyen, S.N.; Jamjoum, L. Tobacco use in India: Prevalence and predictors of smoking and chewing in a national cross sectional household survey. Tob. Control 2003, 12, e4. [Google Scholar] [CrossRef]
- Cheraghlou, S.; Schettino, A.; Zogg, C.K.; Judson, B.L. Changing prognosis of oral cancer: An analysis of survival and treatment between 1973 and 2014. Laryngoscope 2018, 128, 2762–2769. [Google Scholar] [CrossRef]
- Kalyani, R.; Das, S.; Bindra Singh, M.S.; Kumar, H. Cancer profile in the department of pathology of sridevarajurs medical college, Kolar: A ten years study. Indian J. Cancer 2010, 47, 160–165. [Google Scholar] [CrossRef]
- Lohia, N.; Bhatnagar, S.; Singh, S.; Prashar, M.; Subramananiam, A.; Viswanath, S.; Sahu, P.K.; Rai, A. Survival trends in oral cavity cancer patients treated with surgery and adjuvant radiotherapy in a tertiary center of Northern India: Where do we stand compared to th e developed world? SRM J. Res. Dent. Sci. 2019, 10, 26–31. [Google Scholar]
- Ram, H.; Sarkar, J.; Kumar, H.; Konwar, R.; Bhatt, M.L.B.; Mohammad, S. Oral Cancer: Risk Factors and Molecular Pathogenesis. J. Maxillofac. Oral Surg. 2011, 10, 132–137. [Google Scholar] [CrossRef]
- Mishra, G.A.; Pimple, S.A.; Shastri, S.S. An Overview of the tobacco problem in India. Indian J. Med. Pediatr. Oncol. 2012, 33, 139–145. [Google Scholar] [CrossRef]
- Masthan, K.; Babu, N.A.; Dash, K.C.; Elumalai, M. Advanced Diagnostic Aids in Oral Cancer. Asian Pac. J. Cancer Prev. 2012, 13, 3573–3576. [Google Scholar] [CrossRef]
- International Agency for Research on Cancer. IARC monographs on the evaluation of carcinogenic risks to humans. In Personal Habits and Indoor Combustions; IARC: Lyon, France, 2012; Volume 100E, pp. 43–213. [Google Scholar]
- Patel, K.R.; Vajaria, B.N.; Begum, R.; Desai, A.; Patel, J.B.; Shah, F.D.; Shukla, S.N.; Patel, P.S. Prevalence of high-risk human papillomavirus type 16 and 18 in oral and cervical cancers in population from Gujarat, West India. J. Oral Pathol. Med. 2014, 43, 293–297. [Google Scholar] [CrossRef]
- Balaram, P.; Nalinakumar, K.R.; Abraham, E.; Balan, A.; Hareendran, N.K.; Bernard, H.-U.; Chan, S.-Y. Human papillomaviruses in 91 oral cancers from Indian betel quid chewers–High prevalence and multiplicity of infections. Int. J. Cancer 1995, 61, 450–454. [Google Scholar] [CrossRef]
- Elango, K.J.; Suresh, A.; Erode, E.M.; Subhadradevi, L.; Ravindran, H.K.; Iyer, S.K.; Iyer, S.K.R.; Kuriakose, M.A. Role of human papilloma virus in oral tongueSquamous cell carcinoma. Asian Pac. J. Cancer Prev. 2011, 12, 889–896. [Google Scholar] [PubMed]
- He, S.; Chakraborty, R.; Ranganathan, S. Proliferation and Apoptosis Pathways and Factors in Oral Squamous Cell Carcinoma. Int. J. Mol. Sci. 2022, 23, 1562. [Google Scholar] [CrossRef]
- Rajesh, D.; Mohiyuddin, S.M.; Kutty, A.V.; Balakrishna, S. Prevalence of human papillomavirus in oral squamous cell carcinoma: A rural teaching hospital-based cross-sectional study. Indian J. Cancer 2017, 54, 498–501. [Google Scholar]
- Gao, Z.; Tian, Y.; Wang, J.; Yin, Q.; Wu, H.; Li, Y.M.; Jiang, X. A dimeric Smac/diablo peptide directly relieves caspase-3 inhibition by XIAP. Dynamic and cooperative regulation of XIAP by Smac/Diablo. J. Biol. Chem. 2007, 282, 30718–30727. [Google Scholar] [CrossRef]
- Khan, Z.; Bisen, P.S. Oncoapoptotic signaling and deregulated target genes in caners: Special reference to oral cancer. Biochim. Biophys. Acta 2013, 1836, 123–145. [Google Scholar]
- Song, Z.; Yao, X.; Wu, M. Direct interaction between survivin and Smac/DIABLO is essential for the anti-apoptotic activity of survivin during taxol-induced apoptosis. J. Biol. Chem. 2003, 278, 23130–23140. [Google Scholar] [CrossRef]
- Wheatley, S.P.; McNeish, I.A. Survivin: A protein with dual roles in mitosis and apoptosis. Int. Rev. Cytol. 2005, 247, 35–88. [Google Scholar] [CrossRef]
- Salz, W.; Eisenberg, D.; Plescia, J.; Garlick, D.S.; Weiss, R.M.; Wu, X.R. A Survivin gene signature predicts aggressive tumor behavior. Cancer Res. 2005, 65, 3531–3534. [Google Scholar] [CrossRef]
- Angelin, D.; Nair, B.J. Comparative evaluation of survivin expression in leukoplakia, lichen planus, and oralsquamous cell carcinoma: An immunohistochemical study. J. Cancer Res. Ther. 2020, 16, 569–574. [Google Scholar] [CrossRef] [PubMed]
- Khan, Z.; Khan, N.; Tiwari, R.P.; Patro, I.K.; Prasad, G.B.; Bisen, P.S. Down-regulation of Survivin by oxaliplatin diminishes radio resistance of Head and Neck Squamous carcinoma cells. Radiother. Oncol. 2010, 96, 267–273. [Google Scholar] [CrossRef]
- Mulot, C.; Stücker, I.; Clavel, J.; Beaune, P.; Loriot, M.A. Collection of human genomic DNA from buccal cells for genetics studies: Comparison between cytobrush, mouthwash, and treated card. J. Biomed. Biotechnol. 2005, 3, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Reddy, K.R. Department of Epidemiology and Biostatistics (Hospital Based Cancer Registry). Available online: http://kidwai.kar.nic.in/statistics.htm.downloaded (accessed on 10 October 2017).
- Sciubba, J.J. Oral cancer and its detection: History taking and the diagnostic phase of management. J. Am. Dent. Assoc. 2001, 132, 12S–18S. [Google Scholar] [PubMed]
- Dineshkumar, T.; Ashwini, B.K.; Rameshkumar, A.; Rajashree, P.; Ramya, R.; Rajkumar, K. Salivary and serum interleukin-6 levels in oral premalignant disorders and squamous cell carcinoma: Diagnostic value and clinicopathologic correlations. Asian Pac. J. Cancer Prev. 2016, 17, 4899–4906. [Google Scholar]
- Mahmoud, A.M.; Zekri, W.; Khorshed, E.N.; Shalaby, L.M. Prognostic significance of survivin expression in pediatric ewing sarcoma. Pediatr. Hematol. Oncol. 2021, 39, 16–27. [Google Scholar] [CrossRef] [PubMed]
- Santarelli, A.; Mascitti, M.; Lo Russo, L.; Colella, G.; Giannatempo, G.; Bambini, F.; Emanuelli, M.; Procaccini, M.; LoMuzio, L. Detection Level of Salivary Survivin in Patients with OSCC. J. Carcinog. Mutagen. 2013, S5, 1–4. [Google Scholar]
- Li, S.; Chai, L.; Cai, Z.; Jin, L.; Chen, Y.; Wu, H.; Sun, Z. Expression of Survivin and Caspase 3 in Oral Squamous Cell Carcinoma and Peritumoral Tissue. Asian Pac. J. Cancer Prev. 2012, 13, 5027–5031. [Google Scholar] [CrossRef] [PubMed]
- Jane, C.; Nerurkar, A.V.; Shirsat, N.V.; Deshpande, R.B.; Amrapurkar, A.D.; Karjodkar, F.R. Increased survivin expression in high-grade oral Squamous cell carcinoma: A study in Indian tobacco chewers. J. Oral Pathol. Med. 2006, 35, 595–601. [Google Scholar] [CrossRef]
- Gunaldi, M.; Isiksacan, N.; Kocoglu, H.; Okuturlar, Y.; Gunaldi, O.; Topcu, T.O.; Karabulut, M. The value of serum Survivin level in early diagnosis of cancer. J. Cancer Res. Ther. 2018, 14, 570–573. [Google Scholar]
- Sarela, A.I.; Verbeke, C.S.; Ramsdale, J.; Davies, C.L.; Markham, A.F.; Guillou, P.J. Expression of survivin, a novel inhibitor of apoptosis and cell cycle regulatory protein, in pancreatic adenocarcinoma. Br. J. Cancer 2002, 86, 886–892. [Google Scholar] [CrossRef]
- Ikeguchi, M.; Kaibara, N. Survivin messenger RNA expression is a good prognostic biomarker for oesophageal carcinoma. Br. J. Cancer 2002, 87, 883–887. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, K.; Iwamoto, S.; Gon, G.; Nohara, T.; Iwamoto, M.; Tanigawa, N. Expression of survivin and its relationship to loss of apoptosis in breast carcinomas. Clin. Cancer Res. 2000, 6, 127–134. [Google Scholar] [PubMed]
- Sanner, T.; Grimsrud, T.K. Nicotine: Carcinogenicity and effects on response to cancer treatment—A review. Front. Oncol. 2015, 5, 196. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, P.; Kinkade, R.; Joshi, B.; DeCook, C.; Haura, E.; Chellappan, S. Nicotine inhibits apoptosis induced bychemotherapeutic drugs by up-regulating XIAP and survivin. Proc. Natl. Acad. Sci. USA 2006, 103, 6332–6337. [Google Scholar] [CrossRef]
- Altieri, D.C. The molecular basis and potential role of Survivin in cancer diagnosis and therapy. Trend. Mol. Med. 2001, 7, 542–547. [Google Scholar] [CrossRef]
- Ham, M.; Jonathan Kaunitz, D. Gastro-duodenal mucosal defense. Curr. Opin. Gastroenterol. 2008, 24, 665–673. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Analytes | Groups | Mean ± SD | 95% Confidence Interval for Mean | p Value | |
|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||
| Survivin (pg/mL) | Group 1 | 1670.9 ± 796.21 | 1466.94 | 1874.75 | <0.001 |
| Group 2 | 1096.02 ± 346.17 | 1008.11 | 1183.93 | ||
| Group 3 | 397.5 ± 96.1 | 373.29 | 421.69 | ||
| Caspase 3 (ng/mL) | Group 1 | 7.48 ± 2.67 | 6.80 | 8.17 | <0.001 |
| Group 2 | 8.85 ± 2.41 | 8.24 | 9.46 | ||
| Group 3 | 2.27 ± 2.24 | 1.70 | 2.83 | ||
| Multiple Comparisons | |||||||
|---|---|---|---|---|---|---|---|
| Dependent Variable | (I) Group | (J) Group | Mean Difference (I–J) | Std. Error | p Value | 95% Confidence Interval | |
| Lower Bound | Upper Bound | ||||||
| Caspase 3 (ng/mL) | 1 | 2 | −1.37 * | 0.441 | 0.002 * | −2.24 | −0.50 |
| 3 | 5.22 * | 0.440 | 0.001 * | 4.35 | 6.08 | ||
| 2 | 1 | 1.37 * | 0.441 | 0.002 * | 0.50 | 2.24 | |
| 3 | 6.59 * | 0.438 | 0.001 * | 5.72 | 7.45 | ||
| 3 | 1 | −5.22 * | 0.440 | 0.001 * | −6.08 | −4.35 | |
| 2 | −6.59 * | 0.438 | 0.001 * | −7.45 | −5.72 | ||
| Survivin (pg/mL) | 1 | 2 | 574.83 * | 90.34 | 0.001 * | 396.60 | 753.07 |
| 3 | 1273.37 * | 89.96 | 0.001 * | 1095.84 | 1450.90 | ||
| 2 | 1 | −574.83 * | 90.34 | 0.001 * | −753.07 | −396.60 | |
| 3 | 698.54 * | 89.61 | 0.001 * | 521.73 | 875.34 | ||
| 3 | 1 | −1273.37 * | 89.98 | 0.001 * | −1450.90 | −1095.84 | |
| 2 | −698.54 * | 89.61 | 0.001 * | −875.34 | −521.73 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yesupatham, S.T.; Dayanand, C.D.; Azeem Mohiyuddin, S.M. Cellular Concentration of Survivin and Caspase 3 in Habitual Tobacco Chewers with and without Oral Squamous Cell Carcinoma in South Indian Rural Population—A Case Control Study. Diagnostics 2022, 12, 2249. https://doi.org/10.3390/diagnostics12092249
Yesupatham ST, Dayanand CD, Azeem Mohiyuddin SM. Cellular Concentration of Survivin and Caspase 3 in Habitual Tobacco Chewers with and without Oral Squamous Cell Carcinoma in South Indian Rural Population—A Case Control Study. Diagnostics. 2022; 12(9):2249. https://doi.org/10.3390/diagnostics12092249
Chicago/Turabian StyleYesupatham, Susanna Theophilus, C. D. Dayanand, and S. M. Azeem Mohiyuddin. 2022. "Cellular Concentration of Survivin and Caspase 3 in Habitual Tobacco Chewers with and without Oral Squamous Cell Carcinoma in South Indian Rural Population—A Case Control Study" Diagnostics 12, no. 9: 2249. https://doi.org/10.3390/diagnostics12092249