
The Association of Organ Preservation Fluid Pathogens with Early Infection-Related Events after Kidney Transplantation
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Microbial Culture
2.3. Early Infection-Related Events, Pathogen-Related Items and Preemptive Antibiotic Therapy
2.4. Infection Prophylaxis and Immunosuppression
2.5. Statistical Analysis
3. Results
3.1. Donor and Recipient Characteristics
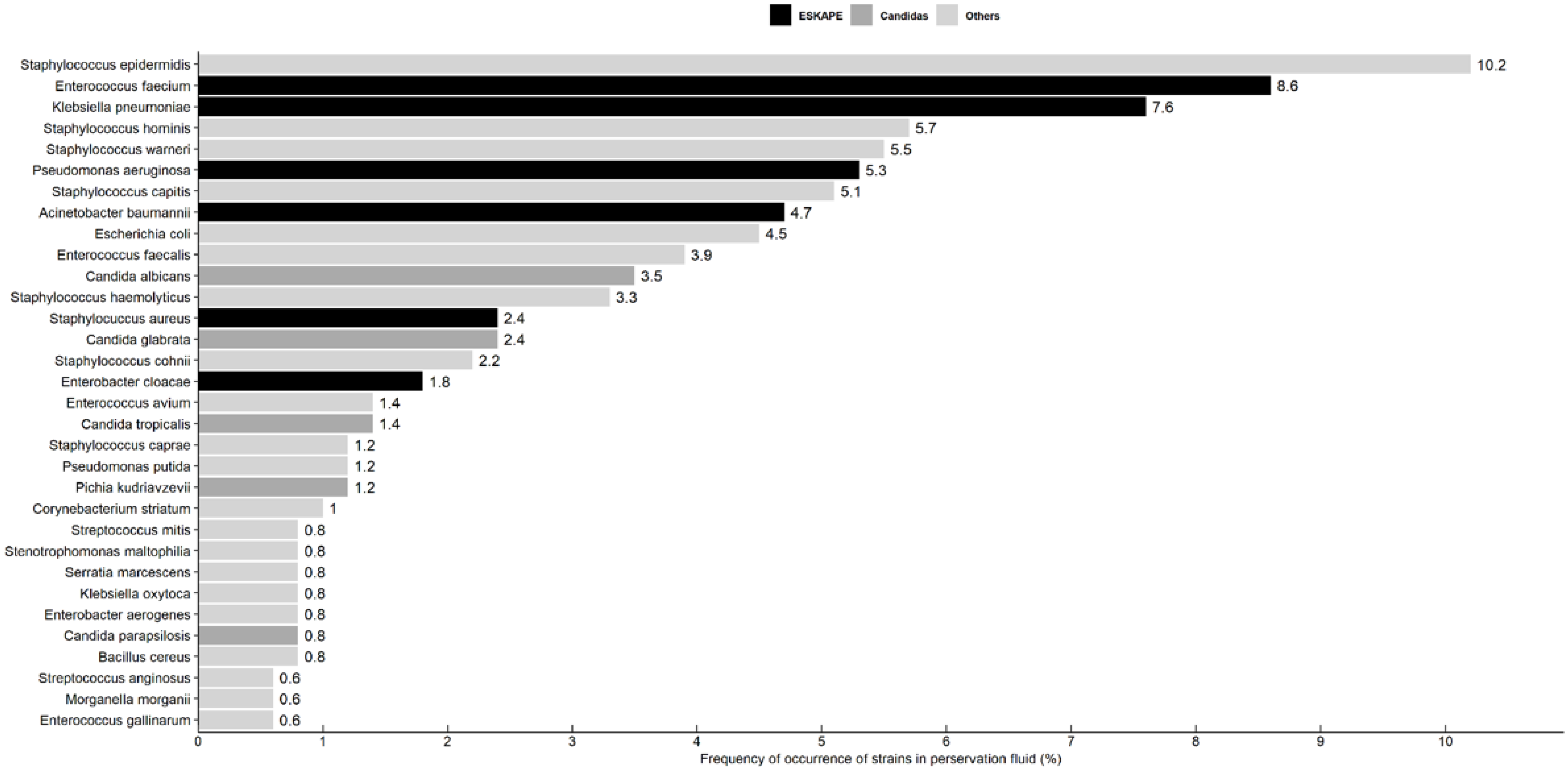
3.2. Microbial Profile of Kidney Graft Preservation Fluid
3.3. Incidence of Early Infection-Related Events According to Positive Versus Negative Preservation Fluid Cultures
3.4. Early Infection-Related Events According to Microbes
3.5. Antimicrobial Resistance in Preservation Fluid and Early Infection-Related Events
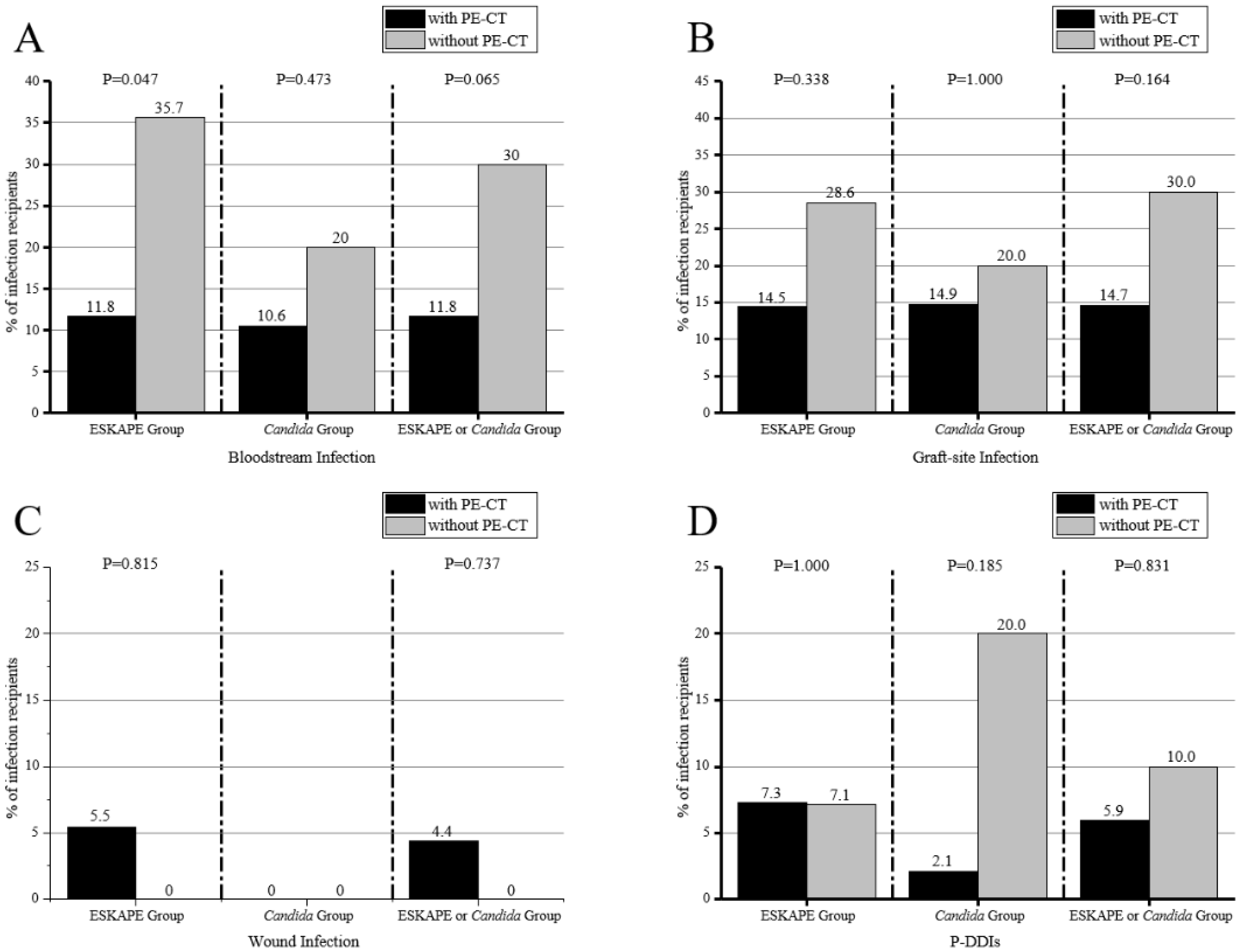
3.6. Preemptive Antibiotic Therapy against ESKAPE or Candida and Early Infection-Related Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Corbel, A.; Ladrière, M.; Le Berre, N.; Durin, L.; Rousseau, H.; Frimat, L.; Thilly, N.; Pulcini, C. Microbiological epidemiology of preservation fluids in transplanted kidney: A nationwide retrospective observational study. Clin. Microbiol. Infect. 2020, 26, 475–484. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Wang, R.; Peng, W.; Huang, H.; Liu, G.; Yang, Q.; Zhou, J.; Zhang, X.; Lv, J.; Lei, W.; et al. Incidence, distribution and clinical relevance of microbial contamination of preservation solution in deceased kidney transplant recipients: A retrospective cohort study from China. Clin. Microbiol. Infect. 2019, 25, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Yahav, D.; Manuel, O. Clinical relevance of preservation-fluid contamination in solid-organ transplantation: A call for mounting the evidence. Clin. Microbiol. Infect. 2019, 25, 536–537. [Google Scholar] [CrossRef] [PubMed]
- Oriol, I.; Lladó, L.; Vila, M.; Baliellas, C.; Tubau, F.; Sabé, N.; Fabregat, J.; Carratalà, J. The Etiology, Incidence, and Impact of Preservation Fluid Contamination during Liver Transplantation. PLoS ONE 2016, 11, e0160701. [Google Scholar] [CrossRef]
- Rice, L.B. Federal funding for the study of antimicrobial resistance in nosocomial pathogens: No ESKAPE. J. Infect. Dis. 2008, 197, 1079–1081. [Google Scholar] [CrossRef]
- Saad, E.J.; Fernández, P.; Azua, A.E.; Ellena, V.; Diz, C.; Giordano, G.; Borgogno, P.; Nuñez, S.; Sarmantano, D.; Guzman, A.; et al. Infections in the first year after renal transplant. Med. B Aires 2020, 80, 611–621. [Google Scholar]
- Lewis, J.D.; Sifri, C.D. Multidrug-Resistant Bacterial Donor-Derived Infections in Solid Organ Transplantation. Curr. Infect. Dis. Rep. 2016, 18, 18. [Google Scholar] [CrossRef]
- Kovacs, C.S., Jr.; Koval, C.E.; van Duin, D.; De Morais, A.G.; Gonzalez, B.E.; Avery, R.K.; Mawhorter, S.D.; Brizendine, K.D.; Cober, E.D.; Miranda, C.; et al. Selecting suitable solid organ transplant donors: Reducing the risk of donor-transmitted infections. World J. Transplant. 2014, 4, 43–56. [Google Scholar] [CrossRef]
- Ma, Y.X.; Wang, C.Y.; Li, Y.Y.; Li, J.; Wan, Q.Q.; Chen, J.H.; Tay, F.R.; Niu, L.N. Considerations and Caveats in Combating ESKAPE Pathogens against Nosocomial Infections. Adv. Sci. 2020, 7, 1901872. [Google Scholar] [CrossRef]
- Chu, L.; Ye, Q.F.; Wan, Q.Q.; Zhou, J.D. Mortality Predictors in Acute Respiratory Distress Syndrome Renal Transplant Recipients With ESKAPE/rESKAPE Pneumonia. Transplant. Proc. 2015, 47, 2450–2455. [Google Scholar] [CrossRef]
- Bodro, M.; Sabé, N.; Tubau, F.; Llado, L.; Baliellas, C.; Roca, J.; Cruzado, J.M.; Carratala, J. Risk factors and outcomes of bacteremia caused by drug-resistant ESKAPE pathogens in solid-organ transplant recipients. Transplantation 2013, 96, 843–849. [Google Scholar] [CrossRef] [PubMed]
- Le Berre, N.; Ladrière, M.; Corbel, A.; Remen, T.; Durin, L.; Frimat, L.; Thilly, N.; Pulcini, C. Antibiotic therapy in case of positive cultures of kidney transplant preservation fluid: A nationwide survey of prescribing practices. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 915–921. [Google Scholar] [CrossRef] [PubMed]
- Meier, R.P.H.; Andrey, D.O.; Sun, P.; Niclauss, N.; Bédat, B.; Demuylder-Mischler, S.; Borot, S.; Benhamou, P.-Y.; Wojtusciszyn, A.; Buron, F.; et al. Pancreas preservation fluid microbial contamination is associated with poor islet isolation outcomes—A multi-centre cohort study. Transpl. Int. 2018, 31, 917–929. [Google Scholar] [CrossRef] [PubMed]
- Ranghino, A.; Diena, D.; Simonato, F.; Messina, M.; Burdese, M.; Piraina, V.; Fop, F.; Segoloni, G.P.; Biancone, L. Clinical impact of bacterial contamination of perfusion fluid in kidney transplantation. Springerplus 2016, 5, 7. [Google Scholar] [CrossRef]
- Levesque, E.; Paugam-Burtz, C.; Saliba, F.; Khoy-Ear, L.; Merle, J.-C.; Jung, B.; Stecken, L.; Ferrandiere, M.; Mihaila, L.; Botterel, F. Fungal complications after Candida preservation fluid contamination in liver transplant recipients. Transpl. Int. 2015, 28, 1308–1316. [Google Scholar] [CrossRef]
- Yansouni, C.P.; Dendukuri, N.; Liu, G.; Fernandez, M.; Frenette, C.; Paraskevas, S.; Sheppard, D.C. Positive cultures of organ preservation fluid predict postoperative infections in solid organ transplantation recipients. Infect. Control Hosp. Epidemiol. 2012, 33, 672–680. [Google Scholar] [CrossRef]
- Karuthu, S.; Blumberg, E.A. Common infections in kidney transplant recipients. Clin. J. Am. Soc. Nephrol. 2012, 7, 2058–2070. [Google Scholar] [CrossRef]
- Control CfD, Prevention. Bloodstream infection event (central line-associated bloodstream infection and non-central line-associated bloodstream infection). Device Assoc. Modul. BSI 2017, 1–38. [Google Scholar]
- Berríos-Torres, S.I.; Umscheid, C.A.; Bratzler, D.W.; Leas, B.; Stone, E.C.; Kelz, R.R.; Reinke, C.E.; Morgan, S.; Solomkin, J.S.; Mazuski, J.E.; et al. Centers for disease control and prevention guideline for the prevention of surgical site infection, 2017. JAMA Surg. 2017, 152, 784–791. [Google Scholar] [CrossRef]
- Gould, C.V.; Umscheid, C.A.; Agarwal, R.K.; Kuntz, G.; Pegues, D.A.; Committee HICPA. Guideline for prevention of catheter-associated urinary tract infections 2009. Infect. Control Hosp. Epidemiol. 2010, 31, 319–326. [Google Scholar] [CrossRef]
- Kalil, A.C.; Metersky, M.L.; Klompas, M.; Muscedere, J.; Sweeney, D.A.; Palmer, L.B.; Napolitano, L.M.; O’Grady, N.P.; Bartlett, J.G.; Carratalà, J.; et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin. Infect. Dis. 2016, 63, e61–e111. [Google Scholar] [CrossRef] [PubMed]
- Shane, A.L.; Mody, R.K.; Crump, J.A.; Tarr, P.I.; Steiner, T.S.; Kotloff, K.; Langley, J.M.; Wanke, C.; Warren, C.A.; Cheng, A.C.; et al. 2017 Infectious Diseases Society of America Clinical Practice Guidelines for the Diagnosis and Management of Infectious Diarrhea. Clin. Infect. Dis. 2017, 65, e45–e80. [Google Scholar] [CrossRef] [Green Version]
- Garzoni, C.; Ison, M.G. Uniform definitions for donor-derived infectious disease transmissions in solid organ transplantation. Transplantation 2011, 92, 1297–1300. [Google Scholar] [CrossRef] [PubMed]
- Tong, L.; Hu, X.-G.; Huang, F.; Huang, S.-W.; Li, L.-F.; Tang, Z.-X.; Yao, J.-Y.; Xu, J.-H.; Zhu, Y.-P.; Chen, Y.-H.; et al. Clinical Impacts and Outcomes With Possible Donor-Derived Infection in Infected Donor Liver Transplantation: A Single-Center Retrospective Study in China. J. Infect. Dis. 2020, 221 (Suppl. 2), S164–S173. [Google Scholar] [CrossRef] [PubMed]
- Becker, K.; Heilmann, C.; Peters, G. Coagulase-negative staphylococci. Clin. Microbiol. Rev. 2014, 27, 870–926. [Google Scholar] [CrossRef] [PubMed]
- Magiorakos, A.-P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef]
- Oriol, I.; Sabe, N.; Càmara, J.; Berbel, D.; Ballesteros, M.A.; Escudero, R.; Lopez-Medrano, F.; Linares, L.; Len, O.; Silva, J.T.; et al. The Impact of Culturing the Organ Preservation Fluid on Solid Organ Transplantation: A Prospective Multicenter Cohort Study. Open Forum Infect Dis. 2019, 6, ofz180. [Google Scholar] [CrossRef]
- Sawinski, D.; Blumberg, E.A. Infection in Renal Transplant Recipients. Chronic Kidney Dis. Dial. Transplant. 2019, 621, e6. [Google Scholar] [CrossRef]
- Grossi, P.A. Donor-derived infections, lessons learnt from the past, and what is the future going to bring us. Curr. Opin. Organ Transplant. 2018, 23, 417–422. [Google Scholar] [CrossRef]
- Sotiropoulos, G.C.; Steinmann, J.; Stern, S.; Raduenz, S.; Machairas, N.; Rath, P.M.; Saner, F.H.; Paul, A.; Gallinat, A. Donor Leucocytosis Predicts Bacterial and Fungal Contamination of the Preservation Solution in Visceral Organ Transplantation. Prog. Transplant. 2018, 28, 24–28. [Google Scholar] [CrossRef]
- De Oliveira, D.M.P.; Forde, B.M.; Kidd, T.J.; Harris, P.N.A.; Schembri, M.A.; Beatson, S.A.; Paterson, D.L.; Walker, M.J. Antimicrobial Resistance in ESKAPE Pathogens. Clin. Microbiol. Rev. 2020, 33. [Google Scholar] [CrossRef] [PubMed]
- Aslam, S.; Rotstein, C. Candida infections in solid organ transplantation: Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13623. [Google Scholar] [CrossRef] [PubMed]
- El-Bandar, N.; Kroy, D.C.; Fuller, T.F.; Kramer, J.; Liefeldt, L.; Budde, K.; Blobel, C.; Miller, K.; Friedersdorff, F. Development of Graft-Site Candidiasis in 3 Solid Organ Transplant Recipients from the Same Donor. Am. J. Case Rep. 2017, 18, 777–781. [Google Scholar] [CrossRef] [PubMed]
- Stern, S.; Bezinover, D.; Rath, P.M.; Paul, A.; Saner, F.H. Candida Contamination in Kidney and Liver Organ Preservation Solution: Does It Matter? J. Clin. Med. 2021, 10, 2022. [Google Scholar] [CrossRef] [PubMed]
- Cervera, C.; van Delden, C.; Gavaldà, J.; Welte, T.; Akova, M.; Carratalà, J. Multidrug-resistant bacteria in solid organ transplant recipients. Clin. Microbiol. Infect. 2014, 20 (Suppl. 7), 49–73. [Google Scholar] [CrossRef]
- Saha, M.; Sarkar, A. Review on Multiple Facets of Drug Resistance: A Rising Challenge in the 21st Century. J. Xenobiotics 2021, 11, 197–214. [Google Scholar] [CrossRef]
- Plantinga, N.L.; Wittekamp, B.H.; van Duijn, P.J.; Bonten, M.J. Fighting antibiotic resistance in the intensive care unit using antibiotics. Future Microbiol. 2015, 10, 391–406. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Preservation Fluid Cultures | ||||
|---|---|---|---|---|
| All (N = 808) | Positive (n = 329) | Negative (n = 479) | p Value a | |
| Recipients | ||||
| Age, years, mean ± SD | 38.6 ± 17.4 | 39.0 ± 17.4 | 38.3 ± 17.4 | 0.401 |
| Male, n (%) | 508 (62.9) | 206 (62.6) | 302 (63.1) | 0.900 |
| Blood types, n (%) | 0.446 | |||
| O | 295 (36.5) | 116 (35.3) | 179 (37.4) | |
| B | 197 (24.4) | 88 (26.8) | 109 (22.8) | |
| A | 241 (29.8) | 99 (30.1) | 142 (29.7) | |
| AB | 75 (9.3) | 26 (7.9) | 49 (10.2) | |
| Diabetes, n (%) | 40 (5.0) | 14 (4.3) | 26 (5.4) | 0.454 |
| Dialysis type, n (%) | 0.658 | |||
| Hemodialysis | 415 (51.4) | 174 (52.9) | 241 (50.3) | |
| Peritoneal dialysis | 206 (25.5) | 84 (25.5) | 122 (25.5) | |
| None | 187 (23.1) | 71 (21.6) | 116 (24.2) | |
| DGF, n (%) | 123 (15.2) | 54 (16.4) | 69 (14.4) | 0.435 |
| Donors | ||||
| Age, years, mean± SD | 30.2 ± 20.4 | 31.3 ± 20.7 | 29.4 ± 20.2 | 0.146 |
| Male, n (%) | 566 (70.1) | 233 (70.8) | 333 (69.5) | 0.802 |
| ICU stay, days, mean (IQR) | 5.5 (3.3) | 6.1 (4.0) | 5.0 (2.6) | <0.01 |
| Cause of death, n (%) | 0.131 | |||
| Traumatic injuries | 326 (40.4) | 143 (43.5) | 183 (38.2) | |
| Cerebrovascular accidents | 218 (27.0) | 88 (26.7) | 130 (27.1) | |
| Hypoxic brain injury | 38 (4.7) | 15 (4.6) | 23 (4.8) | |
| Others | 164 (20.3) | 67 (20.4) | 97 (20.3) | |
| Unknown | 62 (7.7) | 16 (4.9) | 46 (9.6) | |
| Donor type, n (%) | 0.115 | |||
| DBD | 656 (81.2) | 258 (78.4) | 398 (83.1) | |
| DCD | 122 (15.1) | 54 (16.4) | 68 (14.2) | |
| DBCD | 30 (3.7) | 17 (2.1) | 13 (1.6) | |
| Cold ischemia time in hours, mean (IQR) | 10.9 (7.0) | 11.1 (7.0) | 10.8 (7.0) | 0.385 |
| Warm ischemia time in mins, mean (IQR) | 2.5 (0.0) | 2.8 (0.0) | 2.3 (1.0) | 0.008 |
| Combined transplantation, n (%) | 26 (3.2) | 12 (3.7) | 14 (2.9) | 0.566 |
| Preservation Fluid Cultures | |||||
|---|---|---|---|---|---|
| Infection Events | Positive (n = 329) | Negative (n = 479) | p-Value | ||
| Overall infections | 91 | 27.7% | 116 | 24.2% | 0.271 |
| Pneumonia | 34 | 10.3% | 59 | 12.3% | 0.386 |
| Bloodstream infections | 34 | 10.3% | 25 | 5.2% | 0.006 |
| Wound infections | 9 | 2.7% | 5 | 1.0% | 0.070 |
| Graft-site infections | 32 | 9.7% | 22 | 4.6% | 0.004 |
| Urinary tract infections | 21 | 6.4% | 22 | 4.6% | 0.265 |
| Infectious diarrhea | 11 | 3.3% | 9 | 1.9% | 0.188 |
| P-DDIs | 12 | 3.7% | 0 | 0% | - |
| Microbes | |||||
|---|---|---|---|---|---|
| ESKAPE or Candida (n = 156) | Others (n = 173) | p-Value | |||
| Early infections | |||||
| Bloodstream infection | 22 | 14.1% | 12 | 6.9% | 0.033 |
| Wound infection | 6 | 3.8% | 3 | 1.7% | 0.317 |
| Graft-site infections | 26 | 16.7% | 6 | 3.5% | <0.01 |
| Urinary tract infection | 11 | 7.1% | 10 | 5.8% | 0.638 |
| P-DDIs | 10 | 6.4% | 2 | 1.2% | 0.011 |
| Blood circulation | 5 | 3.2% | 0 | 0.0% | 0.023 |
| Surgical wound | 4 | 2.6% | 0 | 0.0% | 0.050 |
| Graft site | 9 | 5.8% | 1 | 0.6% | 0.016 |
| Urinary tract | 4 | 2.6% | 0 | 0.0% | 0.050 |
| Infection Events | All | MDR (n = 179) | No MDR (n = 150) | p-Value | XDR (n = 61) | No XDR (n = 268) | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Bloodstream infection | 34 | 25 | 73.5% | 9 | 26.5% | 0.018 | 9 | 26.5% | 25 | 73.5% | 0.209 |
| Wound infection | 9 | 6 | 66.7% | 3 | 33.3% | 0.517 | 4 | 44.4% | 5 | 55.6% | 0.111 |
| Graft-site infection | 32 | 23 | 71.9% | 9 | 28.1% | 0.037 | 9 | 28.1% | 23 | 71.9% | 0.142 |
| P-DDIs | 12 | 10 | 83.3% | 2 | 16.7% | 0.040 | 7 | 58.3% | 5 | 41.7% | 0.001 |
| Infection Events | All | MDR (n = 81) | No MDR (n = 43) | p-Value | XDR (n = 38) | No XDR (n = 86) | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Bloodstream infection | 18 | 14 | 77.8% | 4 | 22.2% | 0.230 | 7 | 38.9% | 11 | 61.1% | 0.412 |
| Wound infection | 6 | 6 | 100% | 0 | 0.0% | 0.092 | 4 | 66.7% | 2 | 33.3% | 0.071 |
| Graft-site infection | 20 | 15 | 75.0% | 5 | 25.0% | 0.321 | 7 | 35.0% | 13 | 65.0% | 0.645 |
| P-DDIs | 9 | 8 | 88.9% | 1 | 11.1% | 0.238 | 6 | 66.7% | 3 | 33.7% | 0.040 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, J.; Su, X.; Li, J.; Wu, W.; Wu, C.; Guo, P.; Liao, K.; Fu, Q.; Li, J.; Liu, L.; et al. The Association of Organ Preservation Fluid Pathogens with Early Infection-Related Events after Kidney Transplantation. Diagnostics 2022, 12, 2248. https://doi.org/10.3390/diagnostics12092248
Li J, Su X, Li J, Wu W, Wu C, Guo P, Liao K, Fu Q, Li J, Liu L, et al. The Association of Organ Preservation Fluid Pathogens with Early Infection-Related Events after Kidney Transplantation. Diagnostics. 2022; 12(9):2248. https://doi.org/10.3390/diagnostics12092248
Chicago/Turabian StyleLi, Jianming, Xiaojun Su, Jianyi Li, Wenrui Wu, Chenglin Wu, Penghao Guo, Kang Liao, Qian Fu, Jun Li, Longshan Liu, and et al. 2022. "The Association of Organ Preservation Fluid Pathogens with Early Infection-Related Events after Kidney Transplantation" Diagnostics 12, no. 9: 2248. https://doi.org/10.3390/diagnostics12092248