
The Role of Widefield and Ultra Widefield Optical Coherence Tomography in the Diagnosis and Management of Vitreoretinal Diseases

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Examinations and Image Acquisition Protocol
2.3. Image Grading
2.4. Statistical Analysis
3. Results
3.1. Demographics
3.2. Vitreous Pathologies
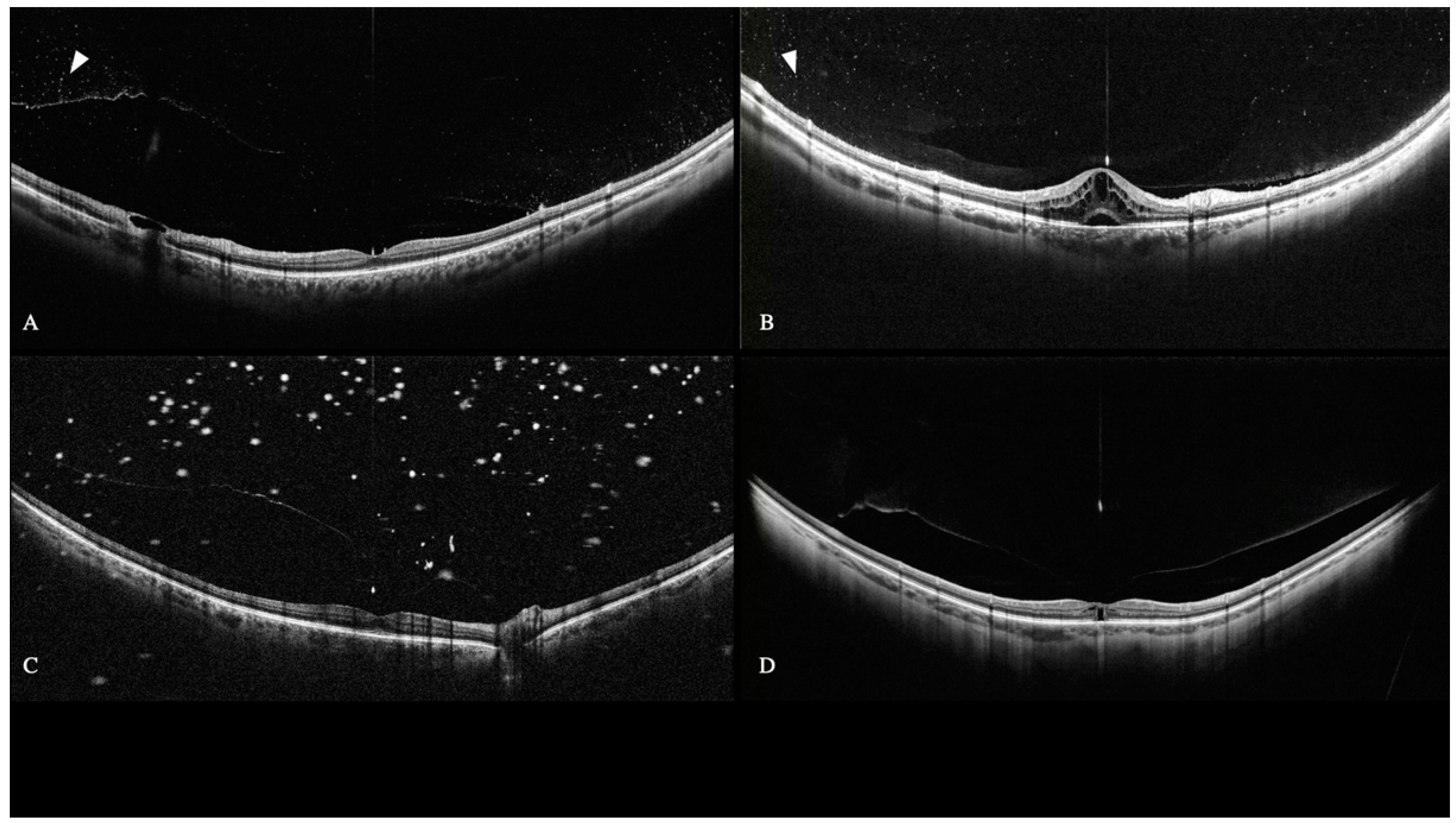
3.2.1. Floaters and Posterior Vitreous Detachment (PVD)
3.2.2. Anomalous PVD
3.2.3. Vitreous Opacities and Cellularity
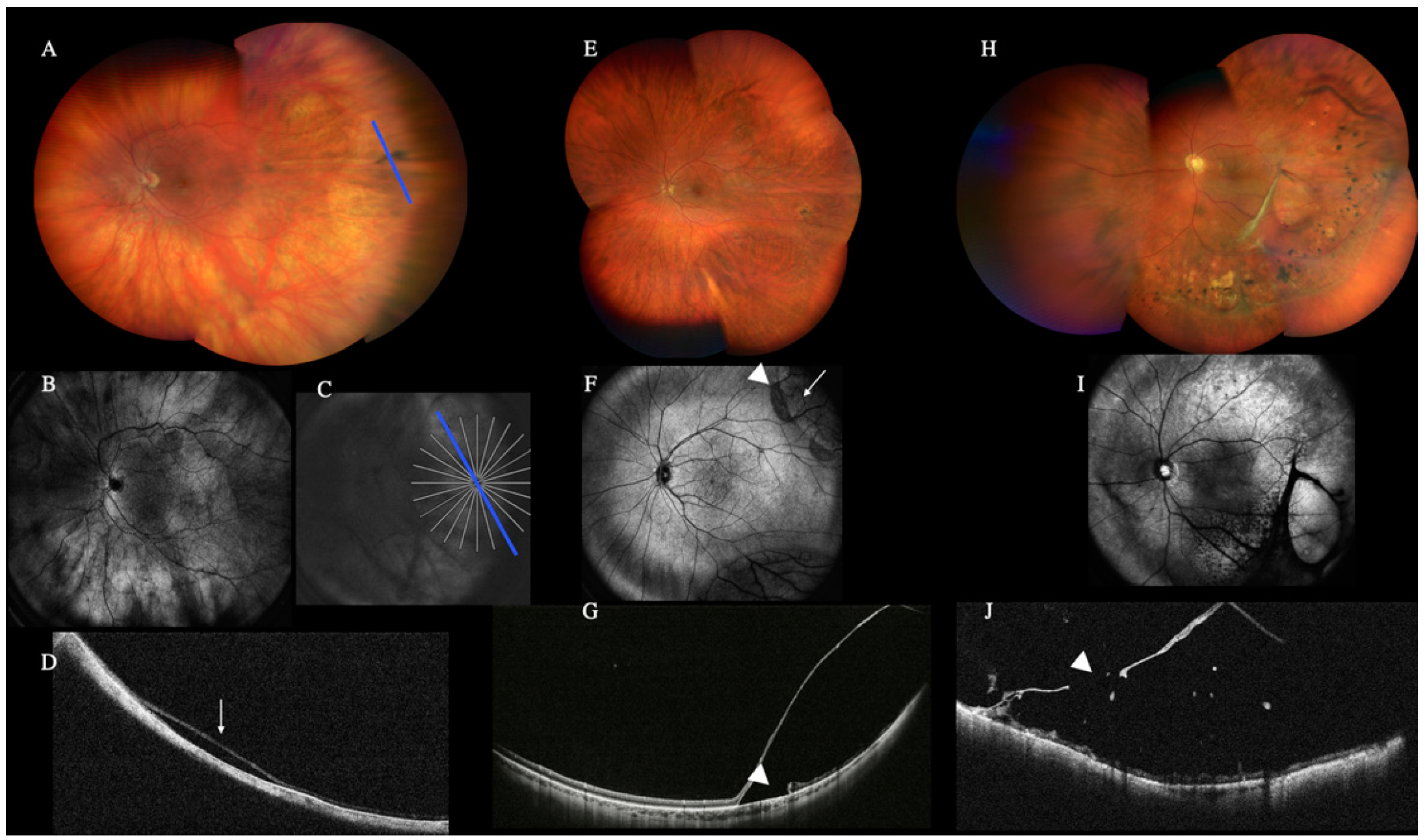
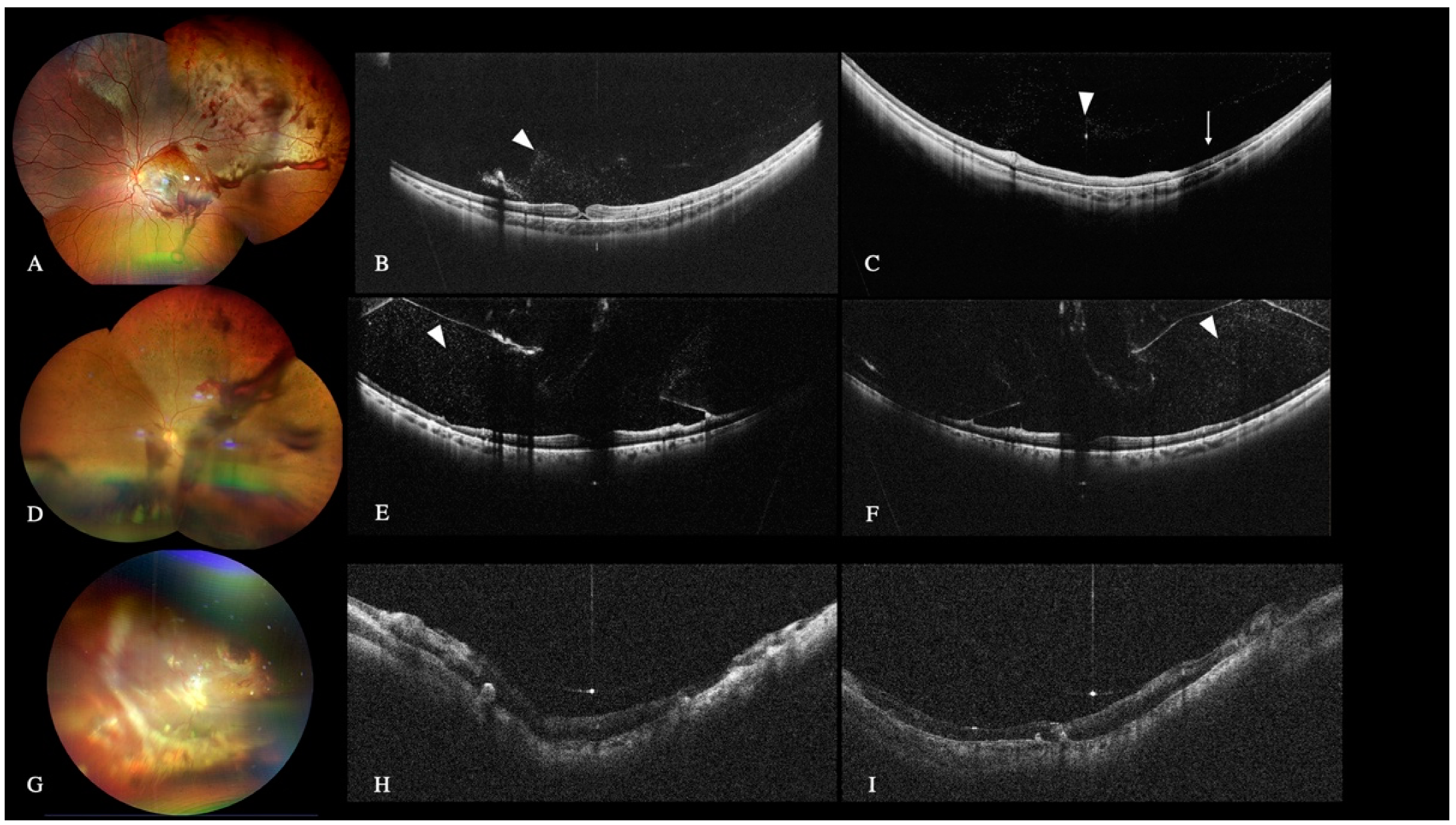
3.3. Peripheral Retinal Lesions and Retinal Detachment
3.3.1. Peripheral Lesions
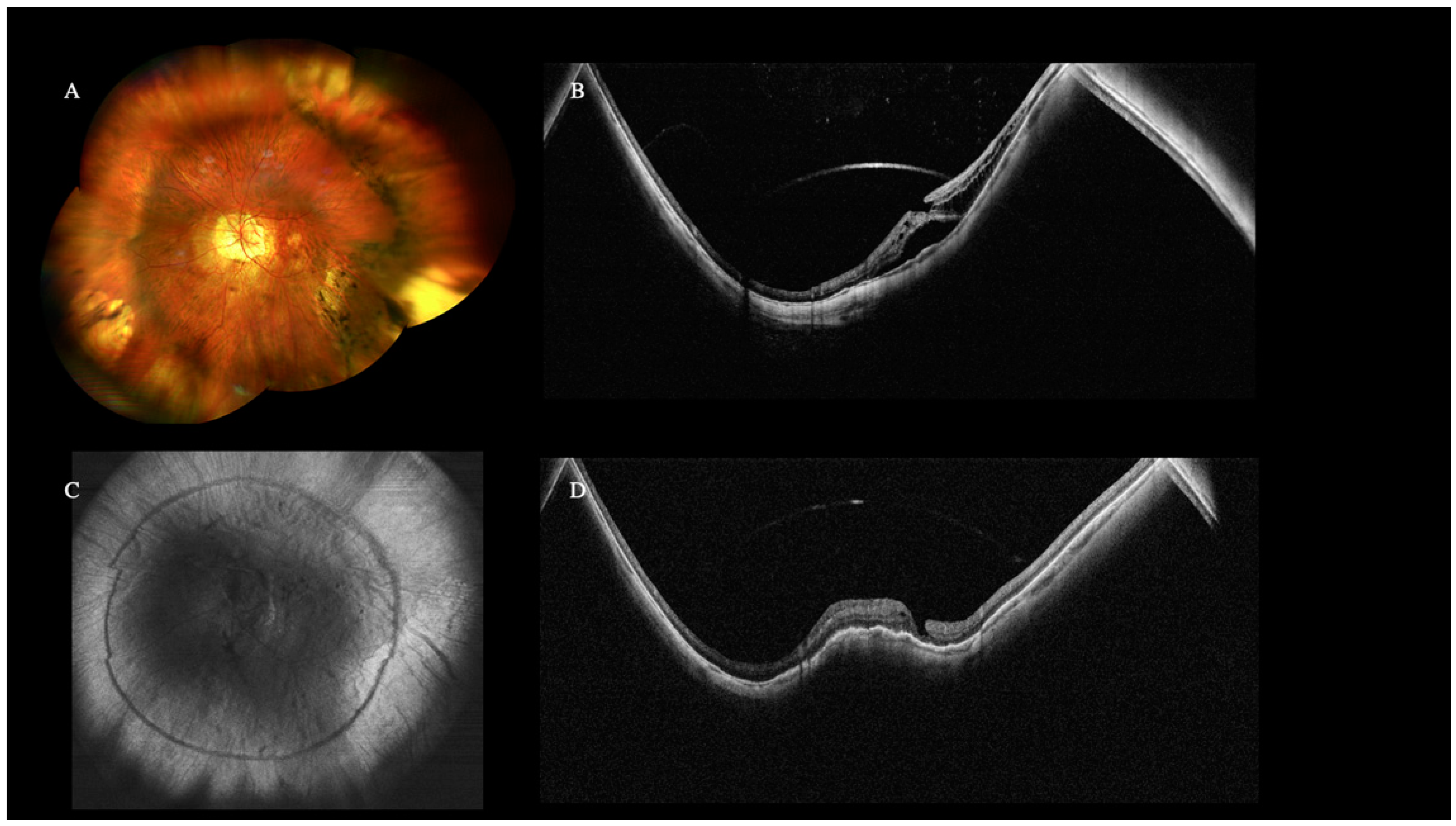
3.3.2. Retinal Detachment
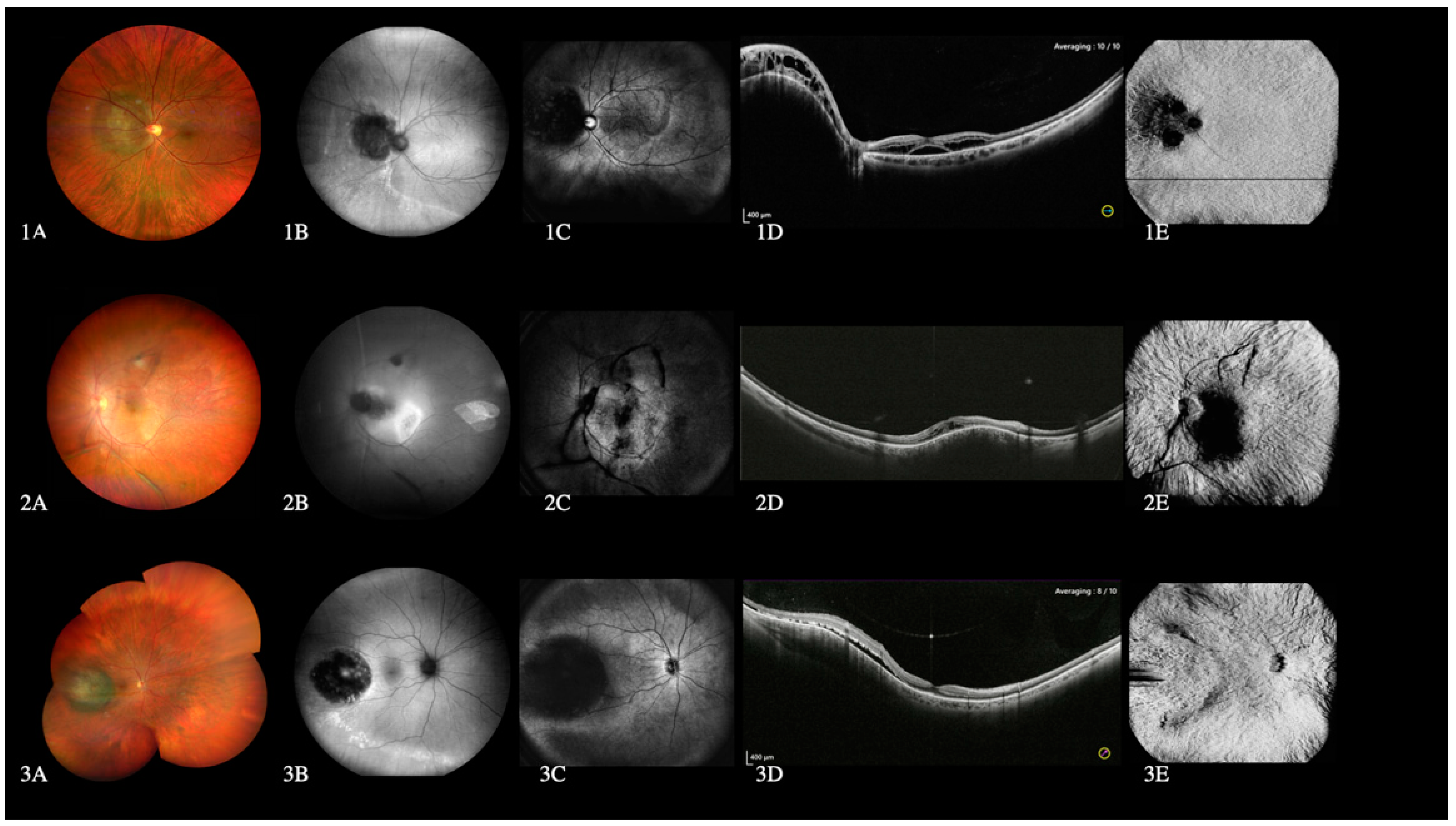
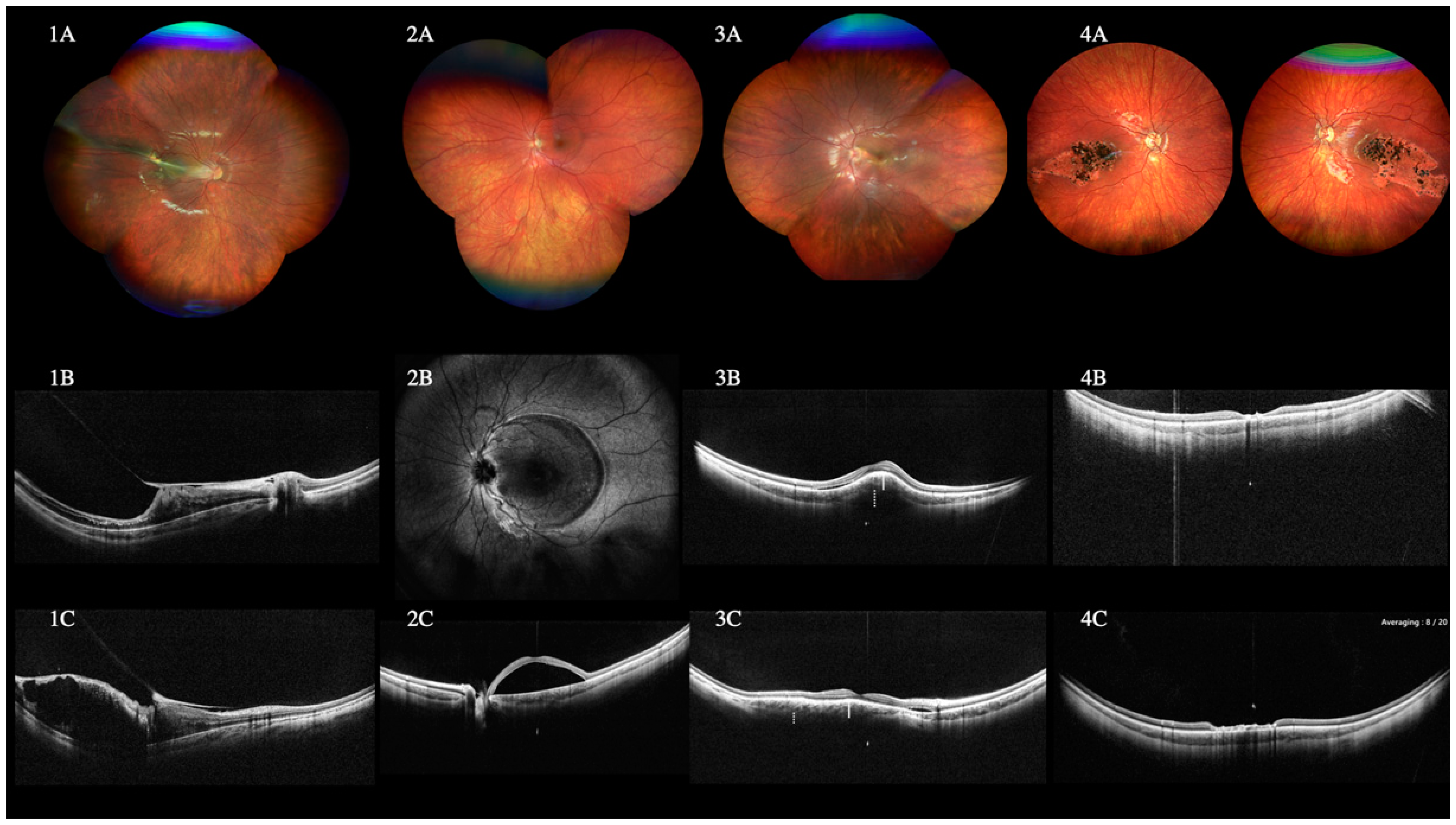
3.4. High Myopia
3.5. Choroidal Lesions
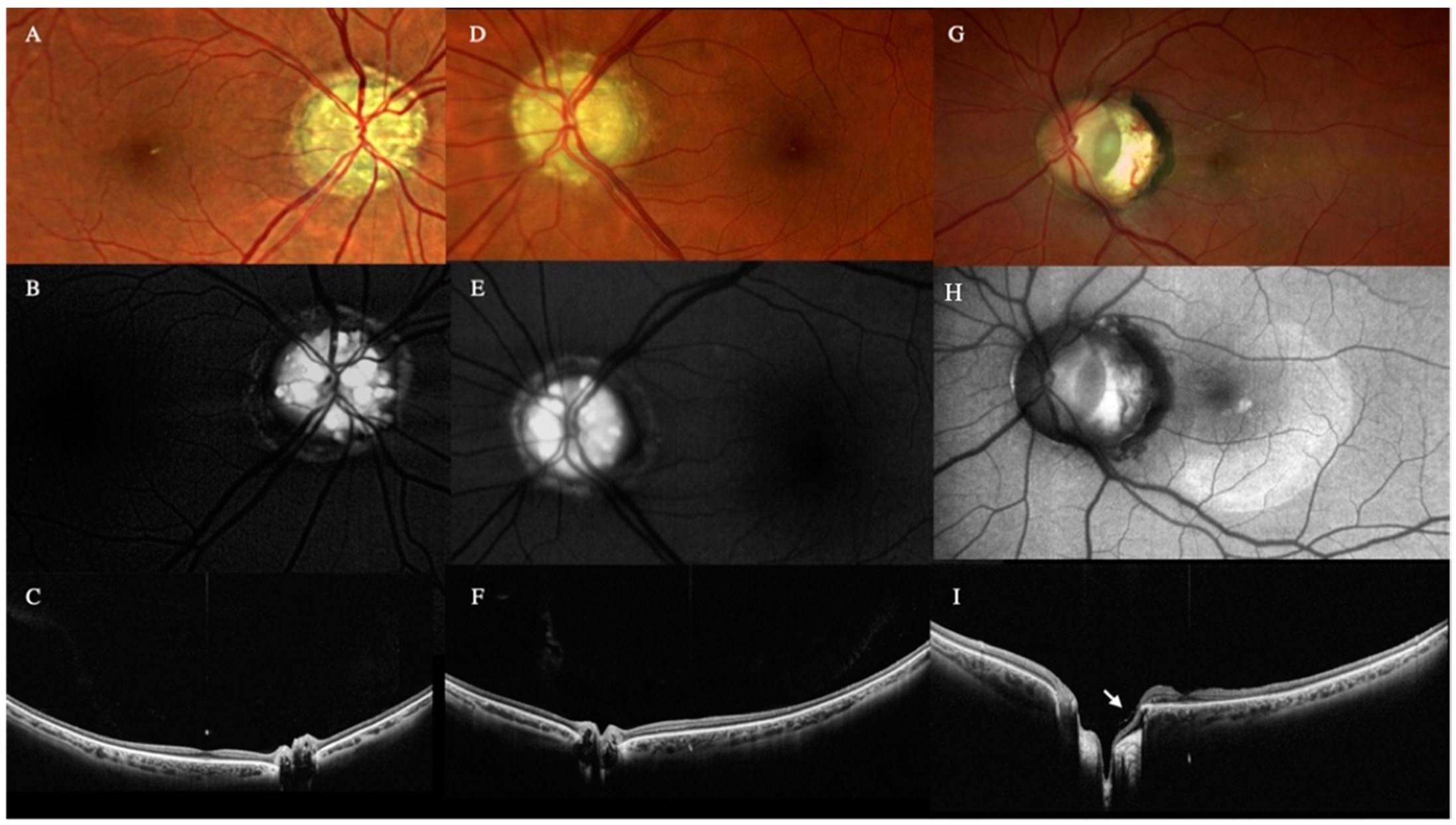
3.6. Optic Nerve Lesions
3.7. Difficult Situations
3.7.1. Miosis
3.7.2. Media Opacities
3.7.3. Pediatric Cases
3.7.4. Postoperative Follow-Up
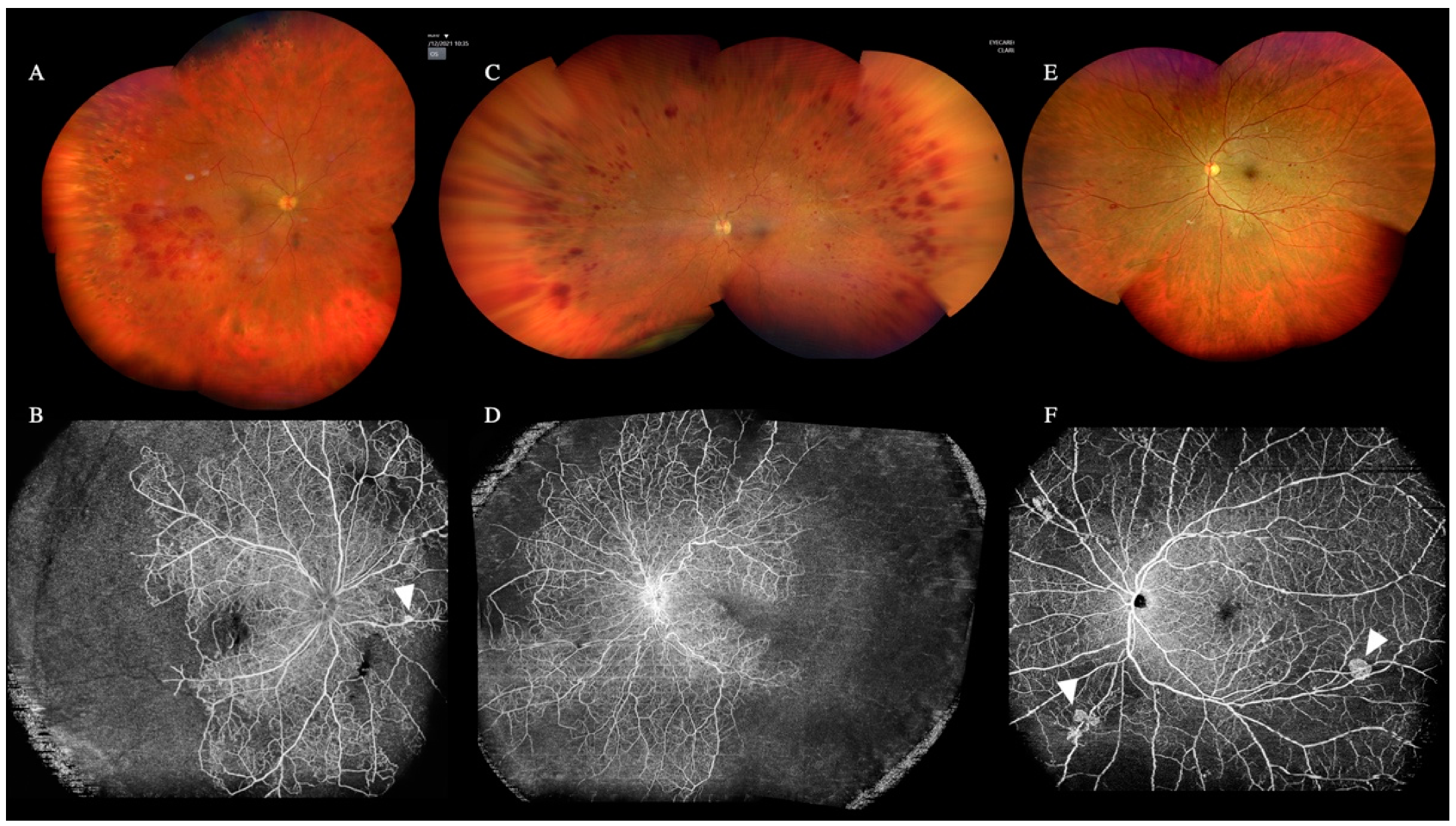
3.8. Role of WF and UWF OCTA
4. Discussion
4.1. Vitreous Pathologies
4.2. Peripheral Retinal Lesions and Retinal Detachment
4.3. High Myopia
4.4. Choroidal Lesions
4.5. Optic Nerve Lesions
4.6. Difficult Situations
4.7. WF and UWF OCTA
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Aumann, S.; Donner, S.; Fischer, J.; Müller, F. Optical Coherence Tomography (OCT): Principle and Technical Realization. In High Resolution Imaging in Microscopy and Ophthalmology; Springer: Gewerbesrasse, Switzerland, 2019; pp. 59–85. [Google Scholar] [CrossRef]
- Spaide, R.F.; Fujimoto, J.G.; Waheed, N.K.; Sadda, S.R.; Staurenghi, G. Optical Coherence Tomography Angiography. Prog. Retin. Eye Res. 2018, 64, 1–55. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.; Swanson, E.A.; Lin, C.P.; Schuman, J.S.; Stinson, W.G.; Chang, W.; Hee, M.R.; Flotte, T.; Gregory, K.; Puliafito, C.A.; et al. Optical Coherence Tomography. Science 1991, 254, 1178–1181. [Google Scholar] [CrossRef] [PubMed]
- Choma, M.; Sarunic, M.; Yang, C.; Izatt, J. Sensitivity Advantage of Swept Source and Fourier Domain Optical Coherence Tomography. Opt. Express 2003, 11, 2183–2189. [Google Scholar] [CrossRef] [PubMed]
- de Boer, J.F.; Cense, B.; Park, B.H.; Pierce, M.C.; Tearney, G.J.; Bouma, B.E. Improved Signal-to-Noise Ratio in Spectral-Domain Compared with Time-Domain Optical Coherence Tomography. Opt. Lett. 2003, 28, 2067–2069. [Google Scholar] [CrossRef] [PubMed]
- Leitgeb, R.; Hitzenberger, C.; Fercher, A. Performance of Fourier Domain vs. Time Domain Optical Coherence Tomography. Opt. Express 2003, 11, 889–894. [Google Scholar] [CrossRef]
- Klein, T.; Wieser, W.; Reznicek, L.; Neubauer, A.; Kampik, A.; Huber, R. Multi-MHz Retinal OCT. Biomed. Opt. Express 2013, 4, 1890–1908. [Google Scholar] [CrossRef]
- Fujimoto, J.; Swanson, E. The Development, Commercialization, and Impact of Optical Coherence Tomography. Investig. Ophthalmol Vis. Sci. 2016, 57, OCT1–OCT13. [Google Scholar] [CrossRef]
- Wang, Y.; Nelson, J.; Chen, Z.; Reiser, B.; Chuck, R.; Windeler, R. Optimal Wavelength for Ultrahigh-Resolution Optical Coherence Tomography. Opt. Express 2003, 11, 1411–1417. [Google Scholar] [CrossRef]
- Grulkowski, I.; Liu, J.J.; Potsaid, B.; Jayaraman, V.; Lu, C.D.; Jiang, J.; Cable, A.E.; Duker, J.S.; Fujimoto, J.G. Retinal, Anterior Segment and Full Eye Imaging Using Ultrahigh Speed Swept Source OCT with Vertical-Cavity Surface Emitting Lasers. Biomed. Opt. Express 2012, 3, 2733–2751. [Google Scholar] [CrossRef] [Green Version]
- Potsaid, B.; Gorczynska, I.; Srinivasan, V.J.; Chen, Y.; Jiang, J.; Cable, A.; Fujimoto, J.G. Ultrahigh Speed Spectral/Fourier Domain OCT Ophthalmic Imaging at 70,000 to 312,500 Axial Scans per Second. Opt. Express 2008, 16, 15149–15169. [Google Scholar] [CrossRef]
- Baldascino, A.; Ripa, M.; Carlà, M.M.; Caporossi, T.; Grieco, G.; Gambini, G.; de Vico, U.; Raguso, G.; Kilian, R.; Rizzo, C.; et al. Optical Coherence Tomography Angiography to Estimate Early Retinal Blood Flow Changes after Uncomplicated Cataract Surgery. Vision 2022, 6, 38. [Google Scholar] [CrossRef] [PubMed]
- Nagiel, A.; Lalane, R.A.; Sadda, S.R.; Schwartz, S.D. Ultra-Widefield Fundus Imaging: A Review of Clinical Applications and Future Trends. Retina 2016, 36, 660–678. [Google Scholar] [CrossRef]
- Choudhry, N.; Golding, J.; Manry, M.W.; Rao, R.C. Ultra-Widefield Steering-Based Spectral-Domain Optical Coherence Tomography Imaging of the Retinal Periphery. Ophthalmology 2016, 123, 1368–1374. [Google Scholar] [CrossRef] [PubMed]
- Parolini, B.; Palmieri, M.; Finzi, A.; Besozzi, G.; Lucente, A.; Nava, U.; Pinackatt, S.; Adelman, R.; Frisina, R. The New Myopic Traction Maculopathy Staging System. Eur. J. Ophthalmol. 2021, 31, 1299–1312. [Google Scholar] [CrossRef] [PubMed]
- Son, G.; Sohn, J.; Kong, M. Acute Symptomatic Vitreous Floaters Assessed with Ultra-Wide Field Scanning Laser Ophthalmoscopy and Spectral Domain Optical Coherence Tomography. Sci. Rep. 2021, 11, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Milston, R.; Madigan, M.C.; Sebag, J. Vitreous Floaters: Etiology, Diagnostics, and Management. Surv. Ophthalmol. 2016, 61, 211–227. [Google Scholar] [CrossRef]
- Lahham, S.; Ali, Q.; Palileo, B.M.; Lee, C.; Fox, J.C. Role of Point of Care Ultrasound in the Diagnosis of Retinal Detachment in the Emergency Department. Open Access Emerg. Med. OAEM 2019, 11, 265–270. [Google Scholar] [CrossRef]
- Sodhi, S.K.; Golding, J.; Trimboli, C.; Choudhry, N. Feasibility of Peripheral OCT Imaging Using a Novel Integrated SLO Ultra-Widefield Imaging Swept-Source OCT Device. Int. Ophthalmol. 2021, 41, 2805–2815. [Google Scholar] [CrossRef]
- Shinohara, K.; Tanaka, N.; Jonas, J.B.; Shimada, N.; Moriyama, M.; Yoshida, T.; Ohno-Matsui, K. Ultrawide-Field OCT to Investigate Relationships between Myopic Macular Retinoschisis and Posterior Staphyloma. Ophthalmology 2018, 125, 1575–1586. [Google Scholar] [CrossRef]
- Li, S.; Li, T.; Wang, X.; Cai, X.; Lu, B.; Chen, Y.; Liu, C.; Wu, Q. Natural Course of Myopic Traction Maculopathy and Factors Influencing Progression and Visual Acuity. BMC Ophthalmol. 2021, 21, 1–11. [Google Scholar] [CrossRef]
- Wolff-Korman, P.G.; Kormann, B.A.; Hasenfratz, G.C.; Spengel, F.A. Duplex and Color Doppler Ultrasound in the Differential Diagnosis of Choroidal Tumors. Acta Ophthalmol. 1992, 70, 66–70. [Google Scholar] [CrossRef] [PubMed]
- Callaway, N.F.; Mruthyunjaya, P. Widefield Imaging of Retinal and Choroidal Tumors. Int. J. Retin. Vitr. 2019, 5, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.J.; Na, K.I.; Kim, Y.K.; Jeoung, J.W.; Park, K.H. Diagnostic Ability of Wide-Field Retinal Nerve Fiber Layer Maps Using Swept-Source Optical Coherence Tomography for Detection of Preperimetric and Early Perimetric Glaucoma. J. Glaucoma 2017, 26, 577–585. [Google Scholar] [CrossRef]
- Kothari, N.; Pineles, S.; Sarraf, D.; Velez, F.; Heilweil, G.; Holland, G.; McCannel, C.A.; Onclinx, T.; McCannel, T.A.; Sadda, S.R.; et al. Clinic-Based Ultra-Wide Field Retinal Imaging in a Pediatric Population. Int. J. Retin. Vitr. 2019, 5, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Athikarisamy, S.E.; Lam, G.C.; Ross, S.; Rao, S.C.; Chiffings, D.; Simmer, K.; Bulsara, M.K.; Patole, S. Comparison of Wide Field Imaging by Nurses with Indirect Ophthalmoscopy by Ophthalmologists for Retinopathy of Prematurity: A Diagnostic Accuracy Study. BMJ Open 2020, 10, e036483. [Google Scholar] [CrossRef] [PubMed]
- Hirano, T.; Kakihara, S.; Toriyama, Y.; Nittala, M.G.; Murata, T.; Sadda, S. Wide-Field En Face Swept-Source Optical Coherence Tomography Angiography Using Extended Field Imaging in Diabetic Retinopathy. Br. J. Ophthalmol. 2018, 102, 1199–1203. [Google Scholar] [CrossRef]
- Pichi, F.; Smith, S.D.; Abboud, E.B.; Neri, P.; Woodstock, E.; Hay, S.; Levine, E.; Baumal, C.R. Wide-Field Optical Coherence Tomography Angiography for the Detection of Proliferative Diabetic Retinopathy. Graefes Arch. Clin. Exp. Ophthalmol. 2020, 258, 1901–1909. [Google Scholar] [CrossRef]
- Huemer, J.; Khalid, H.; Wagner, S.K.; Nicholson, L.; Fu, D.J.; Sim, D.A.; Patel, P.J.; Balaskas, K.; Rajendram, R.; Keane, P.A. Phenotyping of Retinal Neovascularization in Ischemic Retinal Vein Occlusion Using Wide Field OCT Angiography. Eye 2021, 35, 2812–2819. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Features | Number (%) |
|---|---|
| Sex: | 768 |
| Male | 358 (46.61%) |
| Female | 410 (53.39%) |
| Age (years); (mean-range) | 59.6 (5–94) |
| Eye involved | 1472 |
| Right | 735 (49.93%) |
| Left | 737 (50.07%) |
| Diagnosis | Number, N = 1472 Eyes |
|---|---|
| High myopia | 329 |
| Myopic Tractional Maculopathy (MTM) | 91 |
| Macular buckle | 37 |
| Retinal detachment | 144 |
| Follow up | 108 |
| Primary detachment | 36 |
| Peripheral lesions | 122 |
| Retinal tears | 12 |
| Peripheral retinoschisis | 63 |
| Other peripheral lesions | 47 |
| Vascular retinal diseases | 60 |
| BRVO/CRVO | 26 |
| CRAO | 2 |
| Diabetic retinopathy | 32 |
| Pediatric cases | 37 |
| Normal | 16 |
| Best dystrophy | 4 |
| RRD associated with Peter’s anomaly | 2 |
| FEVR | 2 |
| ROP | 2 |
| Diffuse choroidal hemangioma in Sturge Weber syndrome | 2 |
| Combined hamartoma of the retina and RPE | 2 |
| Incontinentia pigmenti | 2 |
| Morning glory syndrome | 1 |
| Traumatic FTMH with VH and traumatic retinopathy | 1 |
| Traumatic retinal detachment | 1 |
| Retinal detachment associated with Marfan syndrome | 1 |
| Optic disc pit maculopathy | 1 |
| Choroidal lesions | 16 |
| Choroidal granuloma | 1 |
| Choroidal melanoma | 4 |
| Choroidal nevus | 4 |
| Circumscribed choroidal hemangioma | 3 |
| Diffuse choroidal hemangioma | 2 |
| Combined hamartoma of the retina and RPE | 2 |
| Vitreomacular Traction (VMT) syndrome | 10 |
| Optic nerve pathologies | 8 |
| Optic nerve coloboma | 1 |
| Optic nerve drusen | 4 |
| Optic disc pit | 3 |
| Uveitis | 5 |
| Toxoplasma retinitis | 3 |
| Behçet disease | 2 |
| Modality of Scan | Time of Acquisition (Seconds) |
|---|---|
| Radial 23 mm | 7 s |
| Radial HD 23 mm | 14 s |
| 3 D Cube 23 mm | 14 s |
| Choroid | 14 s |
| OCTA 23 × 20 mm | 30 s |
| NDB: | |
| Macular 3D | 3 s |
| Glaucoma 3D | 2 s |
| Disc 3D | 3 s |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ripa, M.; Motta, L.; Florit, T.; Sahyoun, J.-Y.; Matello, V.; Parolini, B. The Role of Widefield and Ultra Widefield Optical Coherence Tomography in the Diagnosis and Management of Vitreoretinal Diseases. Diagnostics 2022, 12, 2247. https://doi.org/10.3390/diagnostics12092247
Ripa M, Motta L, Florit T, Sahyoun J-Y, Matello V, Parolini B. The Role of Widefield and Ultra Widefield Optical Coherence Tomography in the Diagnosis and Management of Vitreoretinal Diseases. Diagnostics. 2022; 12(9):2247. https://doi.org/10.3390/diagnostics12092247
Chicago/Turabian StyleRipa, Matteo, Lorenzo Motta, Teresa Florit, Jean-Yves Sahyoun, Veronika Matello, and Barbara Parolini. 2022. "The Role of Widefield and Ultra Widefield Optical Coherence Tomography in the Diagnosis and Management of Vitreoretinal Diseases" Diagnostics 12, no. 9: 2247. https://doi.org/10.3390/diagnostics12092247