
Conventional Ameloblastoma. A Case Report with Microarray and Bioinformatic Analysis
 ,
,
Abstract
:1. Introduction
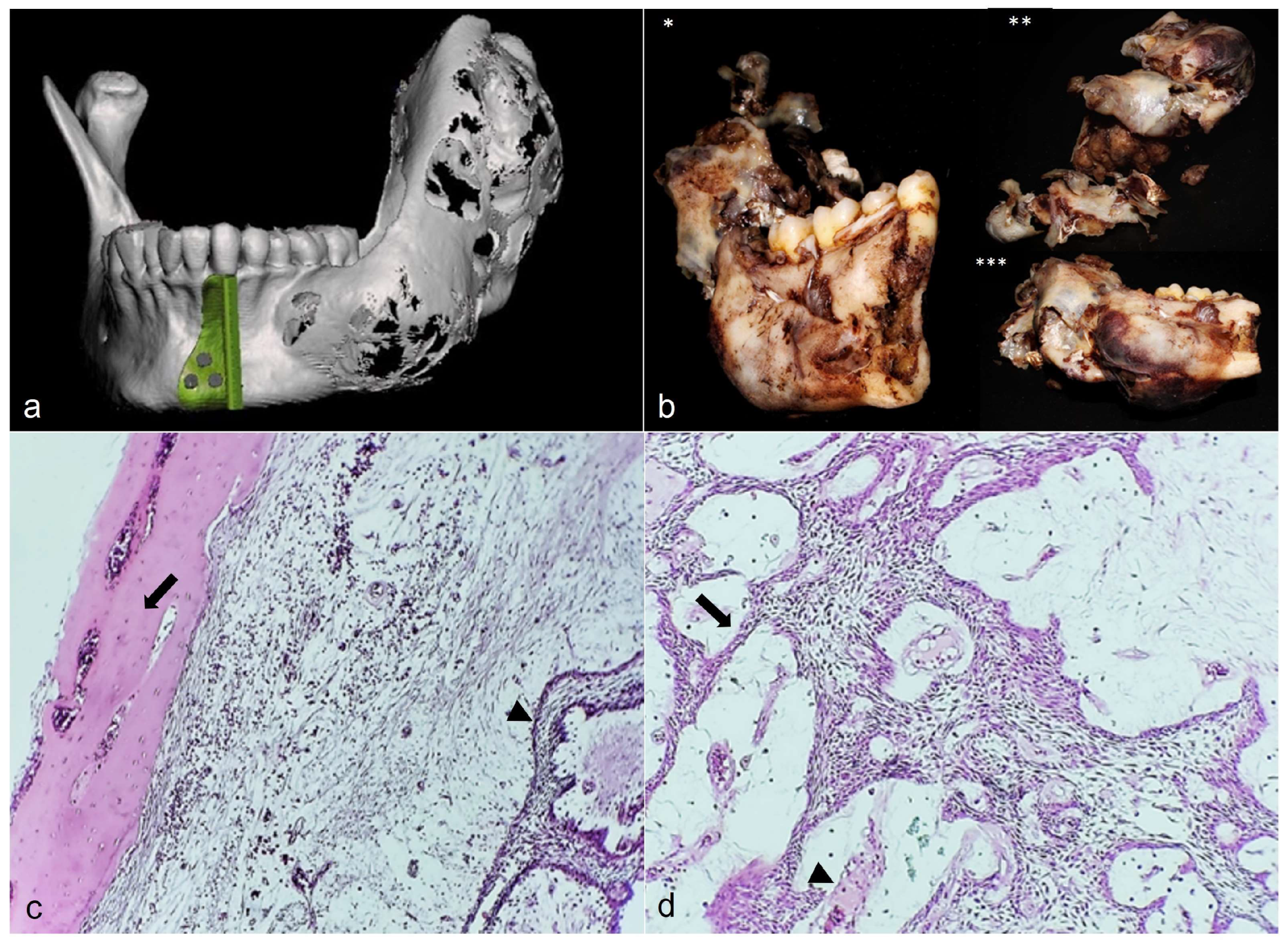
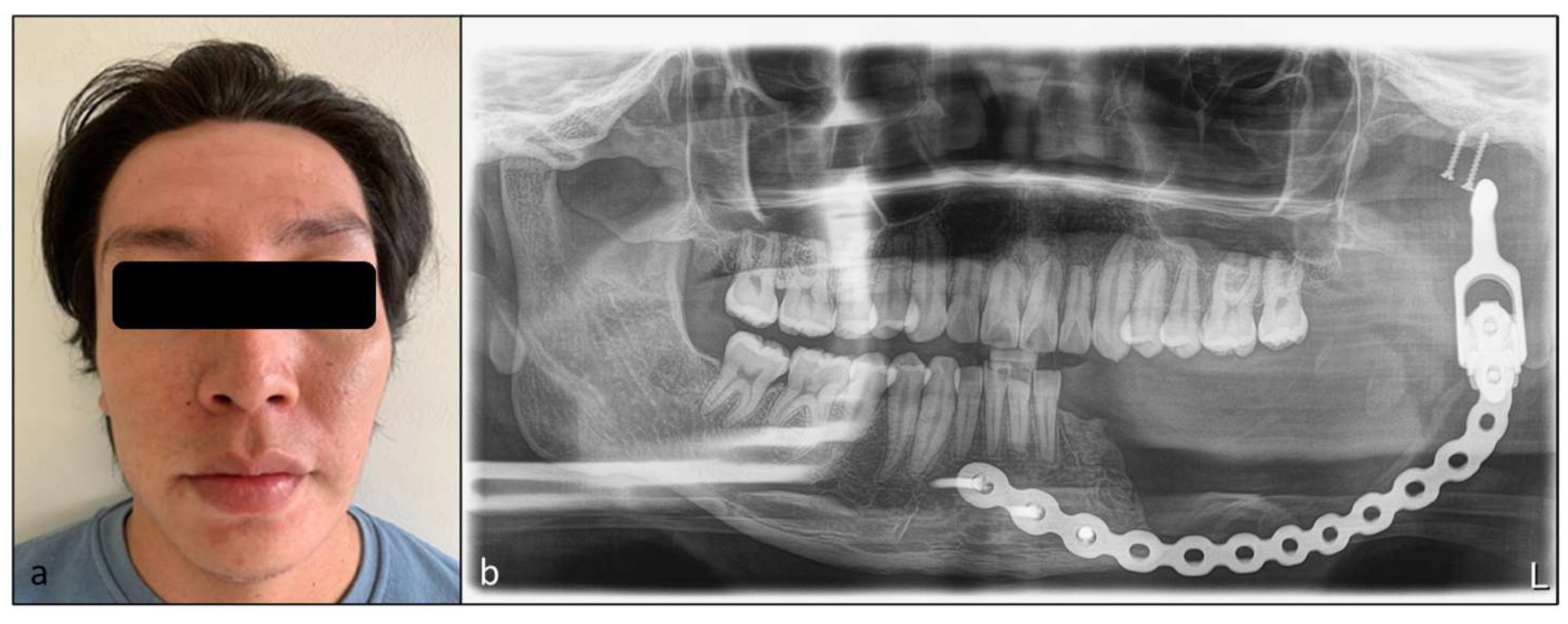
2. Case Report
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vered, M.; Muller, S.; Heikinheimo, K. Ameloblastoma. In WHO Classification of Head and Neck Tumours, 4th ed.; EI-Naggar, A.K., Chan, J.K.C., Grandis, J.R., Takata, T., Slootweg, P.J., Eds.; IARC: Lyon, France, 2017; pp. 215–219. [Google Scholar]
- You, Z.; Liu, S.P.; Du, J.; Wu, Y.H.; Zhang, S.Z. Advancements in MAPK signaling pathways and MAPK-targeted therapies for ameloblastoma: A review. J. Oral Pathol. Med. 2019, 48, 3–201. [Google Scholar] [CrossRef] [PubMed]
- Aramanadka, C.; Kamath, A.T.; Kudva, A. Recurrent Ameloblastoma: A surgical challenge. Case Rep. Dent. 2018, 2018, 8271205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, H.A.; Ng, C.W.B.; Kwa, C.T.; Sim, Q.X.C. Ameloblastoma: A succinct review of the classification, genetic understanding and novel molecular targeted therapies. Surgeon 2021, 19, 4–238. [Google Scholar] [CrossRef]
- Davanian, H.; Balasiddaiah, A.; Heymann, R.; Sundström, M.; Redenström, P.; Silfverberg, M.; Brodin, D.; Sällberg, M.; Lindskog, S.; Kruger Weiner, C.; et al. Ameloblastoma RNA profiling uncovers a distinct non-coding RNA signature. Oncotarget 2017, 8, 3–4530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adeel, M.; Rajput, M.S.A.; Arain, A.A.; Baloch, M.; Khan, M. Ameloblastoma: Management and outcome. Cureus 2018, 10, e3437. [Google Scholar] [CrossRef] [Green Version]
- Mustakim, K.R.; Sodnom-Ish, B.; Eo, M.-Y.; Yoon, H.-J.; Myoung, H.; Kim, S.-M. Conservative decompression management with functional appliance in pediatric plexiform ameloblastoma. Appl. Sci. 2021, 11, 3775. [Google Scholar] [CrossRef]
- Au, S.W.; Li, K.Y.; Choi, W.S.; Su, Y.X. Risk factors for recurrence of ameloblastoma: A long-term follow-up retrospective study. Int. J. Oral Maxillofac. Surg. 2019, 48, 10–1300. [Google Scholar] [CrossRef]
- Abdalla-Aslan, R.; Friedlander-Barenboim, S.; Aframian, D.J.; Maly, A.; Nadler, C. Ameloblastoma incidentally detected in cone-beam computed tomography sialography: A case report and review of the literature. J. Am. Dent. Assoc. 2018, 149, 12–1073. [Google Scholar] [CrossRef]
- Kang, B.C.; Lee, J.S.; Yoon, S.J.; Kim, Y. Ameloblastoma with dystrophic calcification: A case report with 3-dimensional cone-beam computed tomographic images of calcification. Imaging Sci. Dent. 2020, 50, 4–373. [Google Scholar] [CrossRef]
- Fernandes, G.S.; Girardi, D.M.; Bernardes, J.P.G.; Fonseca, F.P.; Fregnani, E.R. Clinical benefit and radiological response with BRAF inhibitor in a patient with recurrent ameloblastoma harboring V600E mutation. BMC Cancer 2018, 18, 887. [Google Scholar] [CrossRef]
- Brunet, M.; Khalifa, E.; Italiano, A. Enabling precision medicine for rare head and neck tumors: The example of BRAF/MEK targeting in patients with metastatic ameloblastoma. Front. Oncol. 2019, 9, 1204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- González-González, R.; López-Verdín, S.; Lavalle-Carrasco, J.; Molina-Frechero, N.; Isiordia-Espinoza, M.; Carreón-Burciaga, R.G.; Bologna-Molina, R. Current concepts in ameloblastoma-targeted therapies in B-raf proto-oncogene serine/threonine kinase V600E mutation: Systematic review. World J. Clin. Oncol. 2020, 11, 1–31. [Google Scholar] [CrossRef] [PubMed]
- Toprani, S.M. DNA damage and repair scenario in ameloblastoma. Oral Oncol. 2020, 108, 104804. [Google Scholar] [CrossRef]
- do Canto, A.M.; Rozatto, J.R.; Schussel, J.L.; de Freitas, R.R.; Hasséus, B.; Braz-Silva, P.H. Immunohistochemical biomarkers in ameloblastomas. Acta Odontol. Scand. 2016, 74, 8–585. [Google Scholar] [CrossRef] [PubMed]
- Heikinheimo, K.; Jee, K.; Niini, T.; Aalto, Y.; Happonen, R.-P.; Leivo, I.; Knuutila, S. Gene expression profiling of ameloblastoma and human tooth germ by means of a cDNA microarray. J. Dent. Res. 2002, 81, 8–525. [Google Scholar] [CrossRef]
- Hu, S.; Parker, J.; Divaris, K.; Padilla, R.; Murrah, V.; Wright, J.T. Ameloblastoma phenotypes reflected in distinct transcriptome profiles. Sci. Rep. 2016, 6, 30867. [Google Scholar] [CrossRef] [Green Version]
- De Villiers, P.; Suggs, C.; Simmons, D.; Murrah, V.; Wright, J.T. Microgenomics of ameloblastoma. J. Dent. Res. 2011, 90, 4–463. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Peng, Y.; Dang, J.; Liu, X.; Zhu, D.; Zhang, Y.; Shi, Y.; Fan, H. Identification of key biomarkers related to epithelial-mesenchymal transition and immune infiltration in ameloblastoma using integrated bioinformatics analysis. Oral Dis. 2022. [Google Scholar] [CrossRef]
- DAVID Bioinformatics Resources 6.8. 2022. Available online: https://david.ncifcrf.gov/ (accessed on 7 November 2022).
- STRING. 2022. Available online: https://string-db.org/ (accessed on 7 November 2022).
- Nagy, A.; Munkacsy, G.; Gyorffy, B. Pancancer survival analysis of cancer hallmark genes. Sci. Rep. 2021, 11, 6047. [Google Scholar] [CrossRef]
- Metascape, A. Gene Annotation & Analysis Resource. 2022. Available online: https://metascape.org/gp/index.html#/main/step1 (accessed on 7 November 2022).
- Pandiar, D.; Anand, R.; Kamboj, M.; Narwal, A.; Shameena, P.M.; Devi, A. Metastasizing ameloblastoma: A 10 year clinicopathological review with an insight into pathogenesis. Head Neck Pathol. 2021, 15, 3–967. [Google Scholar] [CrossRef]
- Kim, J.; Nam, E.; Yoon, S. Conservative management (marsupialization) of unicystic ameloblastoma: Literature review and a case report. Maxillofac. Plast. Reconstr. Surg. 2017, 39, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morice, A.; Neiva, C.; Fabre, M.; Spina, P.; Jouenne, F.; Galliani, E.; Vazquez, M.P.; Picard, A. Conservative management is effective in unicystic ameloblastoma occurring from the neonatal period: A case report and a literature review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 129, e234–e242. [Google Scholar] [CrossRef] [PubMed]
- Trosman, S.J.; Krakovitz, P.R. Pediatric maxillary and mandibular tumors. Otolaryngol. Clin. N. Am. 2015, 48, 1–101. [Google Scholar] [CrossRef] [PubMed]
- Meshram, M.; Sagarka, L.; Dhuvad, J.; Anchlia, S.; Vyas, S.; Shah, H. Conservative management of unicystic ameloblastoma in young patients: A prospective single-center trial and review of literature. J. Maxillofac. Oral Surg. 2017, 16, 3–333. [Google Scholar] [CrossRef]
- Troiano, G.; Dioguardi, M.; Cocco, A.; Laino, L.; Cervino, G.; Cicciu, M.; Ciavarella, D.; Lo Muzio, L. Conservative vs radical approach for the treatment of solid/multicystic ameloblastoma: A systematic review and meta-analysis of the last decade. Oral Health Prev. Dent. 2017, 15, 5–421. [Google Scholar] [CrossRef]
- Yang, Y.C.; Wang, J.J.; Huang, Y.; Cai, W.X.; Tao, Q. Development and validation of a prognostic nomogram for postoperative recurrence-free survival of ameloblastoma. Cancer Manag. Res. 2021, 13, 4403–4416. [Google Scholar] [CrossRef]
- Awadalkreem, F.; Abdoun, O. Enucleation and surgical stent as a treatment strategy for a large unicystic ameloblastoma: Case report and review of literature. Int. J. Surg. Case Rep. 2020, 77, 371–377. [Google Scholar] [CrossRef]
- Qiao, X.; Shi, J.; Liu, J.; Liu, J.; Guo, Y.; Zhong, M. Recurrence rates of intraosseous ameloblastoma cases with conservative or aggressive treatment: A systematic review and meta-analysis. Front. Oncol. 2021, 11, 647200. [Google Scholar] [CrossRef]
- Wilson, G.W.; Bosack, R.C. Reconstruction after hemimandibulectomy using a costochondral rib graft and a dacron-urethane tray with autogenous iliac bone: Report of a case. J. Oral Maxillofac. Surg. 1988, 46, 2–138. [Google Scholar] [CrossRef]
- Patel, A.; Maisel, R. Condylar prostheses in head and neck cancer reconstruction. Arch. Otolaryngol. Head Neck Surg. 2001, 127, 7–842. [Google Scholar]
- Chen, J.; Zhang, R.; Liang, Y.; Ma, Y.; Song, S.; Jiang, C. Deviation Analyses of Computer-Assisted, Template-Guided Mandibular Reconstruction With Combined Osteotomy and Reconstruction Pre-Shaped Plate Position Technology: A Comparative Study. Front. Oncol. 2021, 11, 719466. [Google Scholar] [CrossRef] [PubMed]
- Elledge, R.; Mercuri, L.G.; Attard, A.; Green, J.; Speculand, B. Review of emerging temporomandibular joint total joint replacement systems. Br. J. Oral Maxillofac. Surg. 2019, 57, 8–722. [Google Scholar] [CrossRef] [PubMed]
- Hendra, F.N.; Van Cann, E.M.; Helder, M.N.; Ruslin, M.; de Visscher, J.G.; Forouzanfar, T.; de Vet, H.C.W. Global incidence and profile of ameloblastoma: A systematic review and meta-analysis. Oral Dis. 2020, 26, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.W.; Jee, Y.J.; Lee, D.W.; Kim, H.K. Conservative surgical treatment for ameloblastoma: A report of three cases. J. Korean Assoc. Oral Maxillofac. Surg. 2018, 44, 5–242. [Google Scholar] [CrossRef] [Green Version]
- Slusarenko da Silva, Y.; Tartaroti, N.A.; Sendyk, D.I.; Deboni, M.C.Z.; Naclério-Homem, M.D.G. Is conservative surgery a better choice for the solid/multicystic ameloblastoma than radical surgery regarding recurrence? A systematic review. Oral Maxillofac. Surg. 2018, 22, 349–356. [Google Scholar] [CrossRef]
- Ringer, E.; Kolokythas, A. Bone margin analysis for benign odontogenic tumors. Oral Maxillofac. Surg. Clin. N. Am. 2017, 29, 3–293. [Google Scholar] [CrossRef]
- Kumamoto, H.; Yoshida, M.; Ooya, K. Immunohistochemical detection of amelogenin and cytokeratin 19 in epithelial odontogenic tumors. Oral Dis. 2001, 7, 3–171. [Google Scholar] [CrossRef]
- Crivelini, M.M.; Felipini, R.C.; Miyahara, G.I.; de Sousa, S.C. Expression of odontogenic ameloblast-associated protein, amelotin, ameloblastin, and amelogenin in odontogenic tumors: Immunohistochemical analysis and pathogenetic considerations. J. Oral Pathol. Med. 2012, 41, 3–272. [Google Scholar] [CrossRef]
- Aviel-Ronen, S.; Liokumovich, P.; Rahima, D.; Polak-Charcon, S.; Goldberg, I.; Horowitz, A. The amyloid deposit in calcifying epithelial odontogenic tumor is immunoreactive for cytokeratins. Arch. Pathol. Lab. Med. 2000, 124, 6–872. [Google Scholar] [CrossRef]
- Murphy, C.L.; Kestler, D.P.; Foster, J.S.; Wang, S.; Macy, S.D.; Kennel, S.J.; Carlson, E.R.; Hudson, J.; Weiss, D.T.; Solomon, A. Odontogenic ameloblast-associated protein nature of the amyloid found in calcifying epithelial odontogenic tumors and unerupted tooth follicles. Amyloid 2008, 15, 2–89. [Google Scholar] [CrossRef]
- Hendarmin, L.; Sandra, F.; Nakao, Y.; Ohishi, M.; Nakamura, N. TNFalpha played a role in induction of Akt and MAPK signals in ameloblastoma. Oral Oncol. 2005, 41, 4–375. [Google Scholar] [CrossRef] [PubMed]
- Sandra, F.; Hendarmin, L.; Nakao, Y.; Nakamura, N.; Nakamura, S. Inhibition of Akt and MAPK pathways elevated potential of TNFalpha in inducing apoptosis in ameloblastoma. Oral Oncol. 2006, 42, 1–39. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Fan, H.; Du, W.; Li, J.; Hu, J.; Luo, E. Overgrowth of costochondral grafts in craniomaxillofacial reconstruction: Rare complication and literature review. J. Craniomaxillofac. Surg. 2015, 43, 6–803. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| DEG | Clustered Genes | Poor Survival-Related Genes |
|---|---|---|
| ACE, ACTA1, ACTA2, ACTC1, ACTG2, ACTN4, ACVR1, ACVRL1, ADA, ADAM10, ADAM8, ADARB1, ADCYAP1, ADM, ADORA1, ADORA2A, ADORA3, ADRA1A, ADRA1D, ADRA2A, AGER, AGT, AGTR1, AGTR2, AHSG, AIF1, AIRE, AKR1B1, AKT1, AKT2, ALDH3A1, ALK, ALOX12, ALOX15, ALOX15B, ALOX5, ALOX5AP, AMELX, ANG, ANGPT1, ANXA1, APC, APLNR, APOA1, APOA2, APOBEC1, APOE, APP, AQP1, AREG, ARG1, ARNT, ASPH, ATF3, ATM, AVP, AVPR1B, AZGP1, BAK1, BCHE, BCL6, BDKRB2, BIRC5, BNC1, BRAF, C1QBP, C1QC, C4B, C5AR1, C8B, CAPNS1, CASR, CCL25, CD34, CDH2, CHRNB2, CHUK, CNR2, CRP, CSF1, CTSC, CTSH, CTSS, CTSV, CXCR5, CYP27B1, DAB2, DDR1, DPP4, DPT, EDA, ETV5, FANCA, FAS, FASLG, GBA, IGFBP3, ITGB1, JAG1, KITLG, MAP2K1, NFKBIA, PARP4, PRKCH, PSTPIP1, RHOA, RUNX1, RUNX2, SLC25A5, STAT4, TLR4, TNFRSF8, TSPAN31, TSPO, VIPR2, XIAP | ACE, APOA1, APOE, CRP, BCHE, APP, AGER, ACTA2, TLR4, AKT1, AGTR1, RHOA, AGT, ACTN4, CDH2, ACTC1, ACTG2, JAG1, ADA, ADORA1, ADORA3, ADAM10, C1QC, APOA2, AHSG, C4B, CTSS, ATM, FAS, FASLG, CHUK, XIAP, ALOX5, BCL6, ALOX15, ALOX12, ALOX5AP, ALOX15B, C5AR1 | ACTC1, ADAM10, AGT, AKT1, APOA2, APP, BCHE, CRP |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jurado-Castañeda, E.; Ramírez-Martínez, C.M.; Alonso-Moctezuma, A.; Páramo-Sánchez, J.T.; Rivera-Reza, D.I.; Chanes-Cuevas, O.A.; Ortiz-Solís, C.L.; Téliz-Meneses, M.A.; Hernández-Ortega, O.R.; Vizzuete-Bolaños, M.X.; et al. Conventional Ameloblastoma. A Case Report with Microarray and Bioinformatic Analysis. Diagnostics 2022, 12, 3190. https://doi.org/10.3390/diagnostics12123190
Jurado-Castañeda E, Ramírez-Martínez CM, Alonso-Moctezuma A, Páramo-Sánchez JT, Rivera-Reza DI, Chanes-Cuevas OA, Ortiz-Solís CL, Téliz-Meneses MA, Hernández-Ortega OR, Vizzuete-Bolaños MX, et al. Conventional Ameloblastoma. A Case Report with Microarray and Bioinformatic Analysis. Diagnostics. 2022; 12(12):3190. https://doi.org/10.3390/diagnostics12123190
Chicago/Turabian StyleJurado-Castañeda, Emiliano, Carla Monserrat Ramírez-Martínez, Alejandro Alonso-Moctezuma, Jessica Tamara Páramo-Sánchez, Diana Ivette Rivera-Reza, Osmar Alejandro Chanes-Cuevas, César Luis Ortiz-Solís, Mario Alberto Téliz-Meneses, Oscar Rohel Hernández-Ortega, Marco Xavier Vizzuete-Bolaños, and et al. 2022. "Conventional Ameloblastoma. A Case Report with Microarray and Bioinformatic Analysis" Diagnostics 12, no. 12: 3190. https://doi.org/10.3390/diagnostics12123190