
A Multi-Task Convolutional Neural Network for Lesion Region Segmentation and Classification of Non-Small Cell Lung Carcinoma

Abstract
:1. Introduction and Literature Review
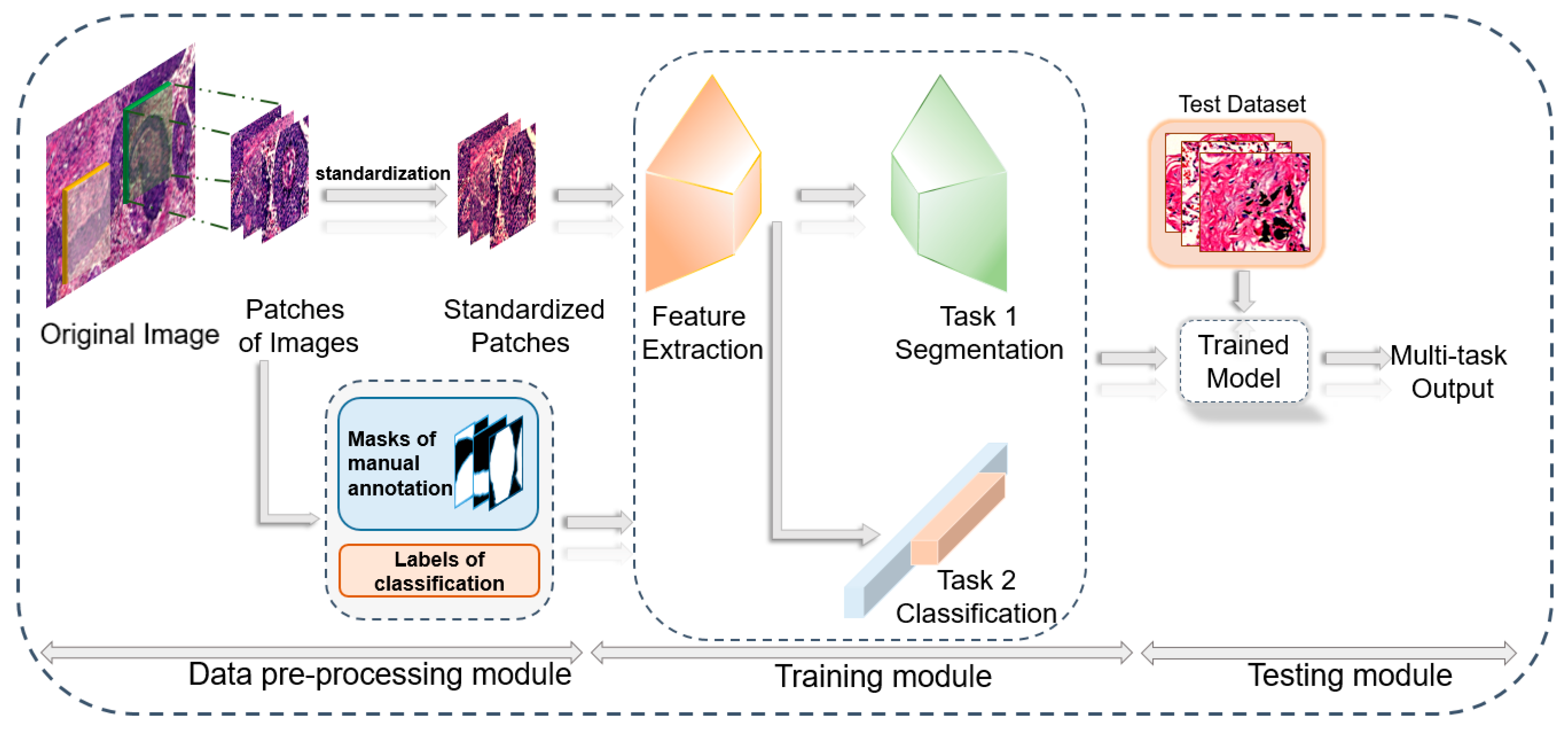
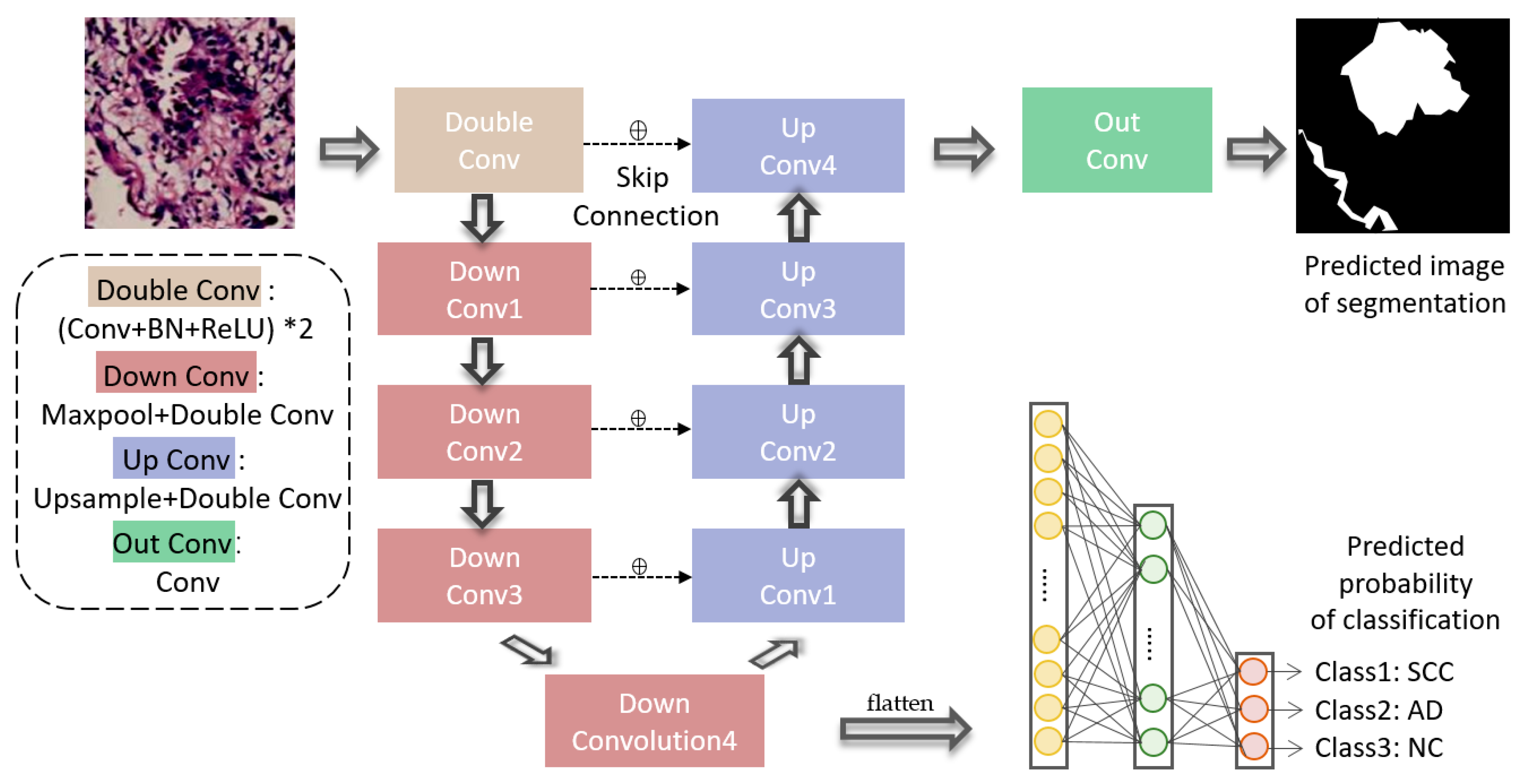
- We propose a novel end-to-end multi-task convolutional neural network (MCN) for lung cancer lesion region segmentation and tumor histological subtype classification, achieved by sharing the same extracted spatial information.
- Our model solved the complex problem of multi-class segmentation and classification, obtaining balanced loss weight ratios.
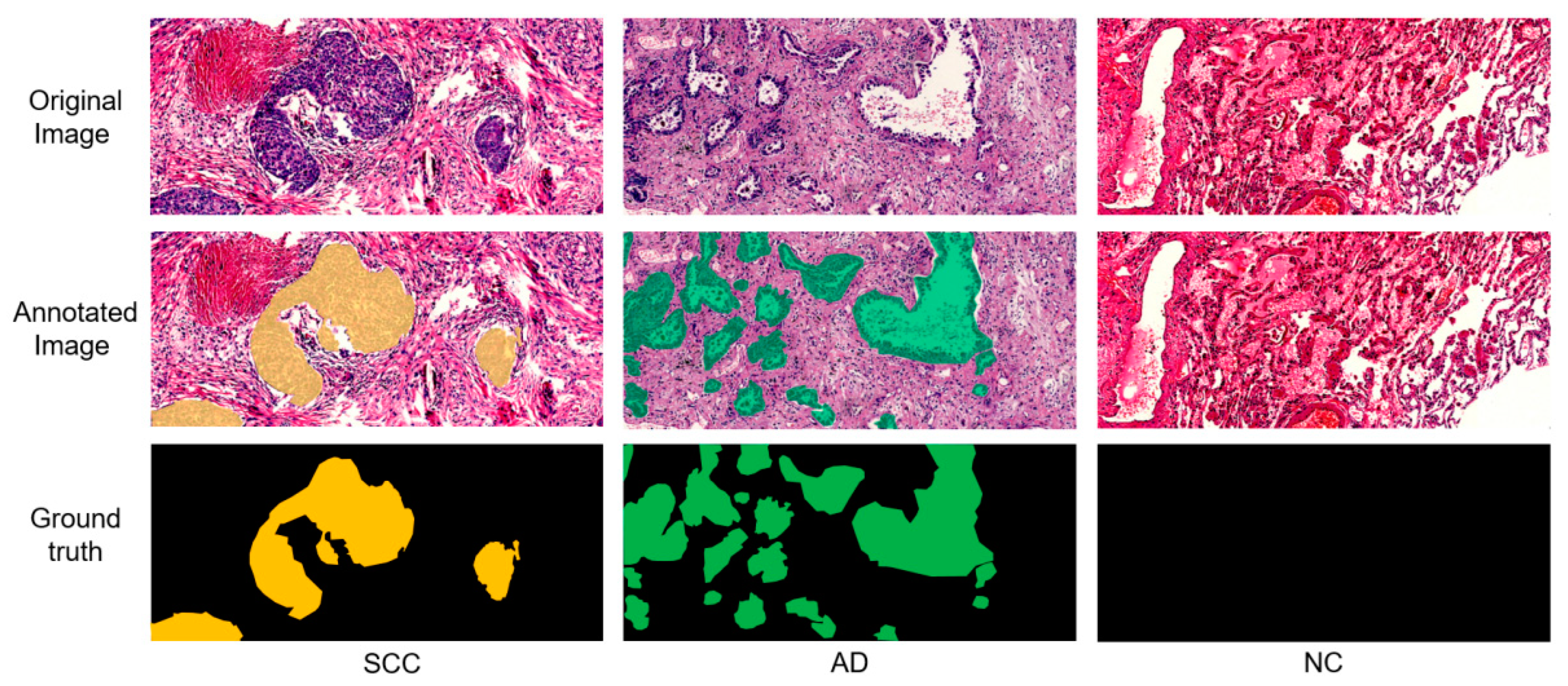
- Our model recognized and segmented cancer lesions more precisely than manually annotation, which is boundary-blurry, shape-irregular and location-random.
2. Materials and Methods
2.1. Data Source
2.2. Multi-Task CNN for Cancer Lesion Segmentation and Histological Subtype Classification
3. Results
3.1. Setting the Valuation Indexes
3.2. Compromising on the Weight of Losses
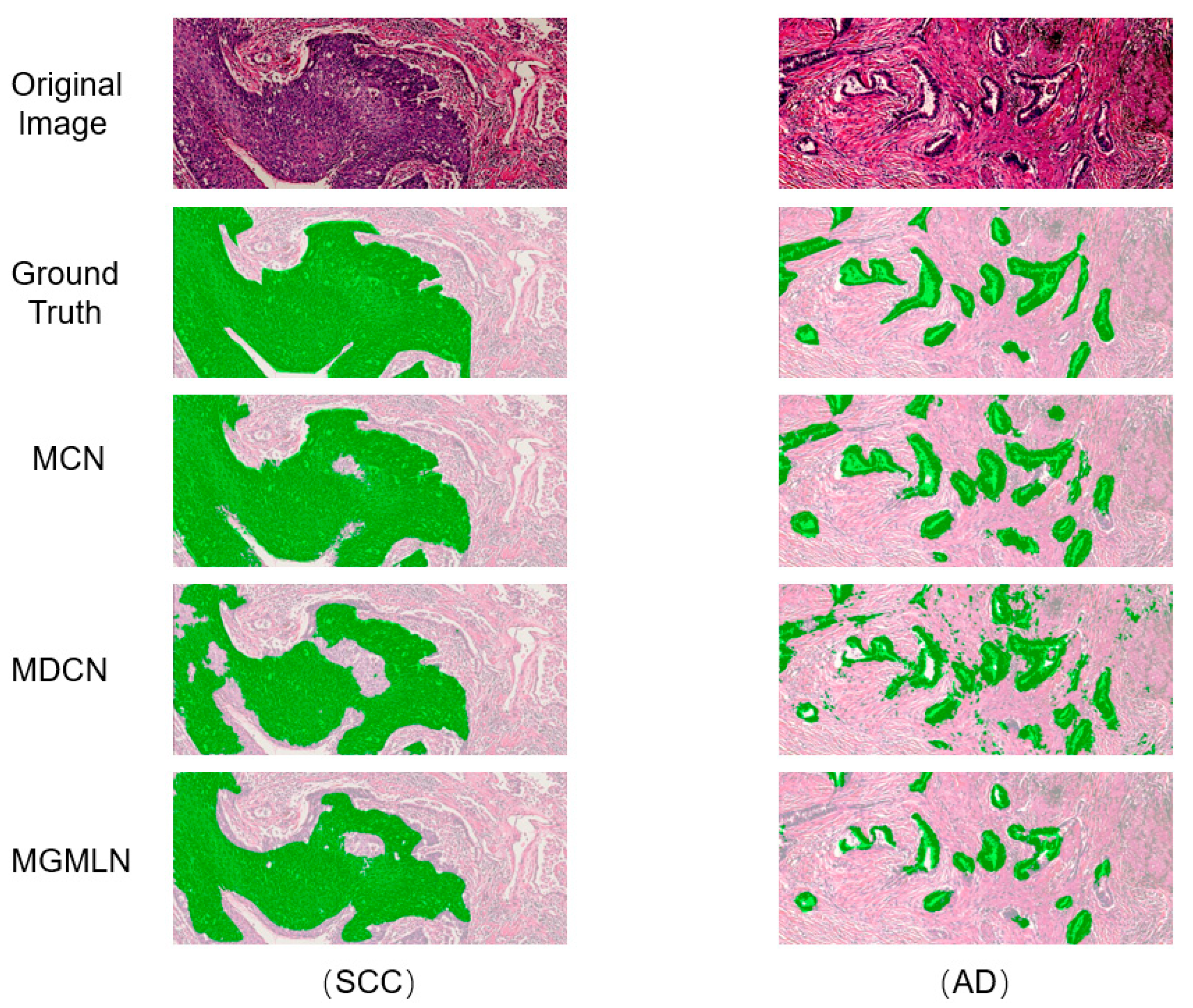
3.3. Comparison with Other Methods
3.3.1. Segmentation Evaluation
3.3.2. Classification Evaluation
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Amini, M.; Hajianfar, G.; Avval, A.H.; Nazari, M.; Deevband, M.R.; Oveisi, M.; Shiri, I.; Zaidi, H. Overall survival prognostic modelling of non-small cell lung cancer patients using positron emission tomography/computed tomography harmonised radiomics features: The quest for the optimal machine learning algorithm. Clin. Oncol. 2022, 34, 114–127. [Google Scholar] [CrossRef]
- Silva, F.; Pereira, T.; Neves, I.; Morgado, J.; Freitas, C.; Malafaia, M.; Sousa, J.; Fonseca, J.; Negrão, E.; Flor de Lima, B.; et al. Towards Machine Learning-Aided Lung Cancer Clinical Routines: Approaches and Open Challenges. J. Pers. Med. 2022, 12, 480. [Google Scholar] [CrossRef]
- Zhou, G.; Li, K.; Liu, W.; Su, Z. Grey Wolf Optimizes Mixed Parameter Multi-Classification Twin Support Vector Machine. J. Front. Comput. Sci. Technol. 2020, 14, 628. [Google Scholar] [CrossRef]
- Tkachenko, R.; Izonin, I.; Vitynskyi, P.; Lotoshynska, N.; Pavlyuk, O. Development of the non-iterative supervised learning predictor based on the ito decomposition and SGTM neural-like structure for managing medical insurance costs. Data 2018, 3, 46. [Google Scholar] [CrossRef] [Green Version]
- Karaismailoglu, E.; Karaismailoglu, S. Two novel nomograms for predicting the risk of hospitalization or mortality due to COVID-19 by the naïve Bayesian classifier method. J. Med. Virol. 2021, 93, 3194–3201. [Google Scholar] [CrossRef]
- Feng, C.; Zhao, H.; Li, Y.; Cheng, Z.; Wen, J. Improved detection of focal cortical dysplasia in normal-appearing FLAIR images using a Bayesian classifier. Med. Phys. 2021, 48, 912–925. [Google Scholar] [CrossRef]
- Izonin, I.; Tkachenko, R.; Duriagina, Z.; Shakhovska, N.; Kovtun, V.; Lotoshynska, N. Smart Web Service of Ti-Based Alloy’s Quality Evaluation for Medical Implants Manufacturing. Appl. Sci. 2022, 12, 5238. [Google Scholar] [CrossRef]
- Doroshenko, A. Piecewise-linear approach to classification based on geometrical transformation model for imbalanced dataset. In Proceedings of the 2018 IEEE Second International Conference on Data Stream Mining & Processing (DSMP), Lviv, Ukraine, 21–25 August 2018; pp. 231–235. [Google Scholar] [CrossRef]
- Izonin, I.; Tkachenko, R.; Kryvinska, N.; Gregus, M.; Tkachenko, P.; Vitynskyi, P. Committee of SGTM neural-like structures with RBF kernel for insurance cost prediction task. In Proceedings of the 2019 IEEE 2nd Ukraine Conference on Electrical and Computer Engineering (UKRCON), Lviv, Ukraine, 2–6 July 2019; pp. 1037–1040. [Google Scholar] [CrossRef]
- Tkachenko, R.; Izonin, I. Model and principles for the implementation of neural-like structures based on geometric data transformations. In Proceedings of the International Conference on Computer Science, Engineering and Education Applications, Kiev, Ukraine, 18–20 January 2018; pp. 578–587. [Google Scholar] [CrossRef]
- ElTanboly, A.; Ismail, M.; Shalaby, A.; Switala, A.; El-Baz, A.; Schaal, S.; Gimel’farb, G.; El-Azab, M. A computer-aided diagnostic system for detecting diabetic retinopathy in optical coherence tomography images. Med. Phys. 2017, 44, 914–923. [Google Scholar] [CrossRef] [PubMed]
- Singh, C.; Bala, A. A local Zernike moment-based unbiased nonlocal means fuzzy C-Means algorithm for segmentation of brain magnetic resonance images. Expert Syst. Appl. 2019, 118, 625–639. [Google Scholar] [CrossRef]
- Freitas, N.R.; Vieira, P.M.; Lima, E.; Lima, C.S. Automatic T1 bladder tumor detection by using wavelet analysis in cystoscopy images. Phys. Med. Biol. 2018, 63, 035031. [Google Scholar] [CrossRef]
- Altaf, F.; Islam, S.M.; Akhtar, N.; Janjua, N.K. Going deep in medical image analysis: Concepts, methods, challenges, and future directions. IEEE Access 2019, 7, 99540–99572. [Google Scholar] [CrossRef]
- Shah, A.; Zhou, L.; Abrámoff, M.D.; Wu, X. Multiple surface segmentation using convolution neural nets: Application to retinal layer segmentation in OCT images. Biomed. Opt. Express 2018, 9, 4509–4526. [Google Scholar] [CrossRef]
- Hu, B.; Du, J.; Zhang, Z.; Wang, Q. Tumor tissue classification based on micro-hyperspectral technology and deep learning. Biomed. Opt. Express 2019, 10, 6370–6389. [Google Scholar] [CrossRef]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. Imagenet classification with deep convolutional neural networks. Adv. Neural Inf. Processing Syst. 2017, 60, 84–90. [Google Scholar] [CrossRef]
- Chen, H.; Zhang, Y.; Kalra, M.K.; Lin, F.; Chen, Y.; Liao, P.; Zhou, J.; Wang, G. Low-dose CT with a residual encoder-decoder convolutional neural network. IEEE T. Med. Imaging 2017, 36, 2524–2535. [Google Scholar] [CrossRef]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the IEEE conference on computer vision and pattern recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar] [CrossRef] [Green Version]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE conference on computer vision and pattern recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar] [CrossRef] [Green Version]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J.; Wojna, Z. Rethinking the inception architecture for computer vision. In Proceedings of the IEEE conference on computer vision and pattern recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 818–2826. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar] [CrossRef]
- Alom, M.Z.; Yakopcic, C.; Nasrin, M.; Taha, T.M.; Asari, V.K. Breast cancer classification from histopathological images with inception recurrent residual convolutional neural network. J. Digit. Imaging 2019, 32, 605–617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coudray, N.; Ocampo, P.S.; Sakellaropoulos, T.; Narula, N.; Snuderl, M.; Fenyö, D.; Moreira, A.L.; Razavian, N.; Tsirigos, A. Classification and mutation prediction from non–small cell lung cancer histopathology images using deep learning. Nat. Med. 2018, 24, 1559–1567. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Zhu, Y.; Yu, L.; Chen, H.; Lin, H.; Wan, X.; Fan, X.; Heng, P.A. RMDL: Recalibrated multi-instance deep learning for whole slide gastric image classification. Med. Image Anal. 2019, 58, 101549. [Google Scholar] [CrossRef]
- Boumaraf, S.; Liu, X.; Wan, Y.; Zheng, Z.; Ferkous, C.; Ma, X.; Li, Z.; Bardou, D. Conventional machine learning versus deep learning for magnification dependent histopathological breast cancer image classification: A comparative study with visual explanation. Diagnostics 2021, 11, 528. [Google Scholar] [CrossRef]
- Ukwuoma, C.C.; Hossain, M.A.; Jackson, J.K.; Nneji, G.U.; Monday, H.N.; Qin, Z. Multi-Classification of Breast Cancer Lesions in Histopathological Images Using DEEP_Pachi: Multiple Self-Attention Head. Diagnostics 2022, 12, 1152. [Google Scholar] [CrossRef]
- Tokunaga, H.; Iwana, B.K.; Teramoto, Y.; Yoshizawa, A.; Bise, R. Negative pseudo labeling using class proportion for semantic segmentation in pathology. In Proceedings of the European Conference on Computer Vision, Glasgow, UK, 23–28 August 2020; pp. 430–446. [Google Scholar] [CrossRef]
- Selvaraju, R.R.; Das, A.; Vedantam, R.; Cogswell, M.; Parikh, D.; Batra, D. Grad-CAM: Why did you say that? arXiv 2016, arXiv:1611.07450. [Google Scholar] [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-net: Convolutional networks for biomedical image segmentation. In Proceedings of the International Conference on Medical image computing and computer-assisted intervention, Munich, Germany, 5–9 October 2015; pp. 234–241. [Google Scholar] [CrossRef]
- Ibtehaz, N.; Rahman, M.S. MultiResUNet: Rethinking the U-Net architecture for multimodal biomedical image segmentation. Neural Netw. 2020, 121, 74–87. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Chan, S.; Park, V.Y.; Chang, K.T.; Mehta, S.; Kim, M.J.; Combs, F.J.; Chang, P.; Chow, D.; Parajuli, R.; et al. Automatic detection and segmentation of breast cancer on MRI using mask R-CNN trained on non–fat-sat images and tested on fat-sat images. Acad. Radiol. 2020, 29, S135–S144. [Google Scholar] [CrossRef] [PubMed]
- Long, J.; Shelhamer, E.; Darrell, T. Fully convolutional networks for semantic segmentation. In Proceedings of the IEEE conference on computer vision and pattern recognition, Boston, MA, USA, 7–12 June 2015; pp. 3431–3440. [Google Scholar] [CrossRef]
- Zhou, X.; Takayama, R.; Wang, S.; Hara, T.; Fujita, H. Deep learning of the sectional appearances of 3D CT images for anatomical structure segmentation based on an FCN voting method. Med. Phys. 2017, 44, 5221–5233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Pi, J.; Lou, M.; Qi, Y.; Li, S.; Meng, J.; Ma, Y. Multi-level feature fusion network for nuclei segmentation in digital histopathological images. Vis. Comput. 2022, 1–16. [Google Scholar] [CrossRef]
- Wang, D.; Khosla, A.; Gargeya, R.; Irshad, H.; Beck, A.H. Deep learning for identifying metastatic breast cancer. arXiv 2016, arXiv:1606.05718. [Google Scholar] [CrossRef]
- Kumar, N.; Verma, R.; Arora, A.; Kumar, A.; Gupta, S.; Sethi, A.; Gann, P.H. Convolutional neural networks for prostate cancer recurrence prediction. In Proceedings of the Medical Imaging 2017: Digital Pathology, Orlando, FL, USA, 12–13 February 2017; Volume 10140, pp. 106–117. [Google Scholar] [CrossRef]
- Liu, M.; Li, F.; Yan, H.; Wang, K.; Ma, Y.; Shen, L.; Xu, M.; Alzheimer’s Disease Neuroimaging Initiative. A multi-model deep convolutional neural network for automatic hippocampus segmentation and classification in Alzheimer’s disease. Neuroimage 2020, 208, 116459. [Google Scholar] [CrossRef]
- Zhang, Y.; Li, H.; Du, J.; Qin, J.; Wang, T.; Chen, Y.; Liu, B.; Gao, W.; Ma, G.; Lei, B. 3D multi-attention guided multi-task learning network for automatic gastric tumor segmentation and lymph node classification. IEEE Trans. Med. Imaging 2021, 40, 1618–1631. [Google Scholar] [CrossRef]
- Peykani, P.; Mohammadi, E.; Seyed Esmaeili, F.S. Measuring performance, estimating most productive scale size, and benchmarking of hospitals using DEA approach: A case study in Iran. Int. J. Hosp. Res. 2018, 7, 21–41. [Google Scholar]
- Xie, Y.; Meng, W.; Li, R.; Wang, Y.; Qian, X.; Chan, C.; Yu, Z.; Fan, X.; Pan, H.; Xie, C.; et al. Early lung cancer diagnostic biomarker discovery by machine learning methods. Transl. Oncol. 2021, 14, 100907. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diagnosis | Age | Gender (M/F) 1 | Cancer Staging (I/II/III) 2 | Tumor Volume (cm2) |
|---|---|---|---|---|
| SCC | 64.4 ± 7.8 | 14/1 | 10/4/1 | 10.74 ± 9.5 |
| AD | 53.8 ± 12.6 | 5/6 | 9/2/0 | 2.91 ± 2.1 |
| NC | 61.1 ± 9.1 | 8/2 | - | - |
| Performance in Different Γ | Classification Performance (%) | Segmentation Performance (%) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| ACC | SEN | SPE | DSC | SEN | PRE | IoU | |||
| Γ1:Γ2 = 0:1 | SCC vs. NC | 97.8 | 95.2 | 100 | Mean | — | — | — | — |
| SCC | — | — | — | — | |||||
| AD vs. NC | 90.2 | 86.1 | 100 | AD | — | — | — | — | |
| NC | — | — | — | — | |||||
| Γ1:Γ2 = 0.5:1 | SCC vs. NC | 92.7 | 90.5 | 95 | Mean | 79.4 | 84.5 | 78.7 | 77.9 |
| SCC | 94.0 | 91.6 | 96.8 | 88.9 | |||||
| AD vs. NC | 98.1 | 100 | 100 | AD | 68.7 | 63.3 | 75.4 | 52.4 | |
| NC | 93.8 | 96.6 | 91.1 | 88.2 | |||||
| Γ1:Γ2 = 1:1 | SCC vs. NC | 95.1 | 95 | 95.2 | Mean | 92.3 | 92.2 | 91.9 | 85.2 |
| SCC | 93.5 | 90.1 | 97.3 | 87.9 | |||||
| AD vs. NC | 100 | 100 | 100 | AD | 89.0 | 89.4 | 88.6 | 80.2 | |
| NC | 94.5 | 97.2 | 89.7 | 87.5 | |||||
| Γ1:Γ2 = 1:0.5 | SCC vs. NC | 92.7 | 94.7 | 90.9 | Mean | 84.4 | 80.5 | 88.0 | 73.0 |
| SCC | 89.3 | 82.7 | 97.2 | 80.8 | |||||
| AD vs. NC | 95.7 | 100 | 90.9 | AD | 73.6 | 61.4 | 83.5 | 56.6 | |
| NC | 90.3 | 97.3 | 83.3 | 81.5 | |||||
| Γ1:Γ2 = 1:0 | SCC vs. NC | — | — | — | Mean | 89.4 | 88.6 | 90.5 | 82.1 |
| SCC | 95.6 | 94.2 | 97.8 | 92.3 | |||||
| AD vs. NC | — | — | — | AD | 76.8 | 73.9 | 80.1 | 62.4 | |
| NC | 95.9 | 97.6 | 93.7 | 91.7 | |||||
| Method | Tumor Type | Segmentation Performance (%) | Tumor Type | Classification Performance (%) | |||||
|---|---|---|---|---|---|---|---|---|---|
| DSC | SEN | Pre | IoU | ACC | SEN | SPE | |||
| MGMLN | Mean | 84.1 | 79.6 | 91.5 | 74.6 | SCC vs. NC | 64.1 | 100.0 | 30.0 |
| SCC | 92.0 | 88.1 | 96.4 | 85.3 | |||||
| AD | 65.1 | 52.2 | 86.9 | 48.4 | AD vs. NC | 96.6 | 100.0 | 85.7 | |
| NC | 95.1 | 98.5 | 91.3 | 90.0 | |||||
| MDCN | Mean | 81.4 | 81.7 | 85.3 | 71.1 | SCC vs. NC | 92.7 | 90.0 | 95.2 |
| SCC | 85.2 | 74.6 | 99.6 | 74.4 | |||||
| AD | 69.4 | 80.9 | 60.2 | 52.7 | AD vs. NC | 100.0 | 100.0 | 100.0 | |
| NC | 89.7 | 89.5 | 96.0 | 86.3 | |||||
| MCN | Mean | 92.3 | 92.2 | 91.9 | 85.2 | SCC vs. NC | 95.1 | 95.0 | 95.2 |
| SCC | 93.5 | 90.1 | 97.3 | 87.9 | |||||
| AD | 89.0 | 89.4 | 88.6 | 80.2 | AD vs. NC | 100.0 | 100.0 | 100.0 | |
| NC | 94.5 | 97.2 | 89.7 | 87.5 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Z.; Xu, Y.; Tian, L.; Chi, Q.; Zhao, F.; Xu, R.; Jin, G.; Liu, Y.; Zhen, J.; Zhang, S. A Multi-Task Convolutional Neural Network for Lesion Region Segmentation and Classification of Non-Small Cell Lung Carcinoma. Diagnostics 2022, 12, 1849. https://doi.org/10.3390/diagnostics12081849
Wang Z, Xu Y, Tian L, Chi Q, Zhao F, Xu R, Jin G, Liu Y, Zhen J, Zhang S. A Multi-Task Convolutional Neural Network for Lesion Region Segmentation and Classification of Non-Small Cell Lung Carcinoma. Diagnostics. 2022; 12(8):1849. https://doi.org/10.3390/diagnostics12081849
Chicago/Turabian StyleWang, Zhao, Yuxin Xu, Linbo Tian, Qingjin Chi, Fengrong Zhao, Rongqi Xu, Guilei Jin, Yansong Liu, Junhui Zhen, and Sasa Zhang. 2022. "A Multi-Task Convolutional Neural Network for Lesion Region Segmentation and Classification of Non-Small Cell Lung Carcinoma" Diagnostics 12, no. 8: 1849. https://doi.org/10.3390/diagnostics12081849