
Undifferentiated Carcinoma with Osteoclast-Like Giant Cells of the Common Bile Duct: A Case Report of a Rare Entity at an Unusual Location


Abstract
:1. Introduction
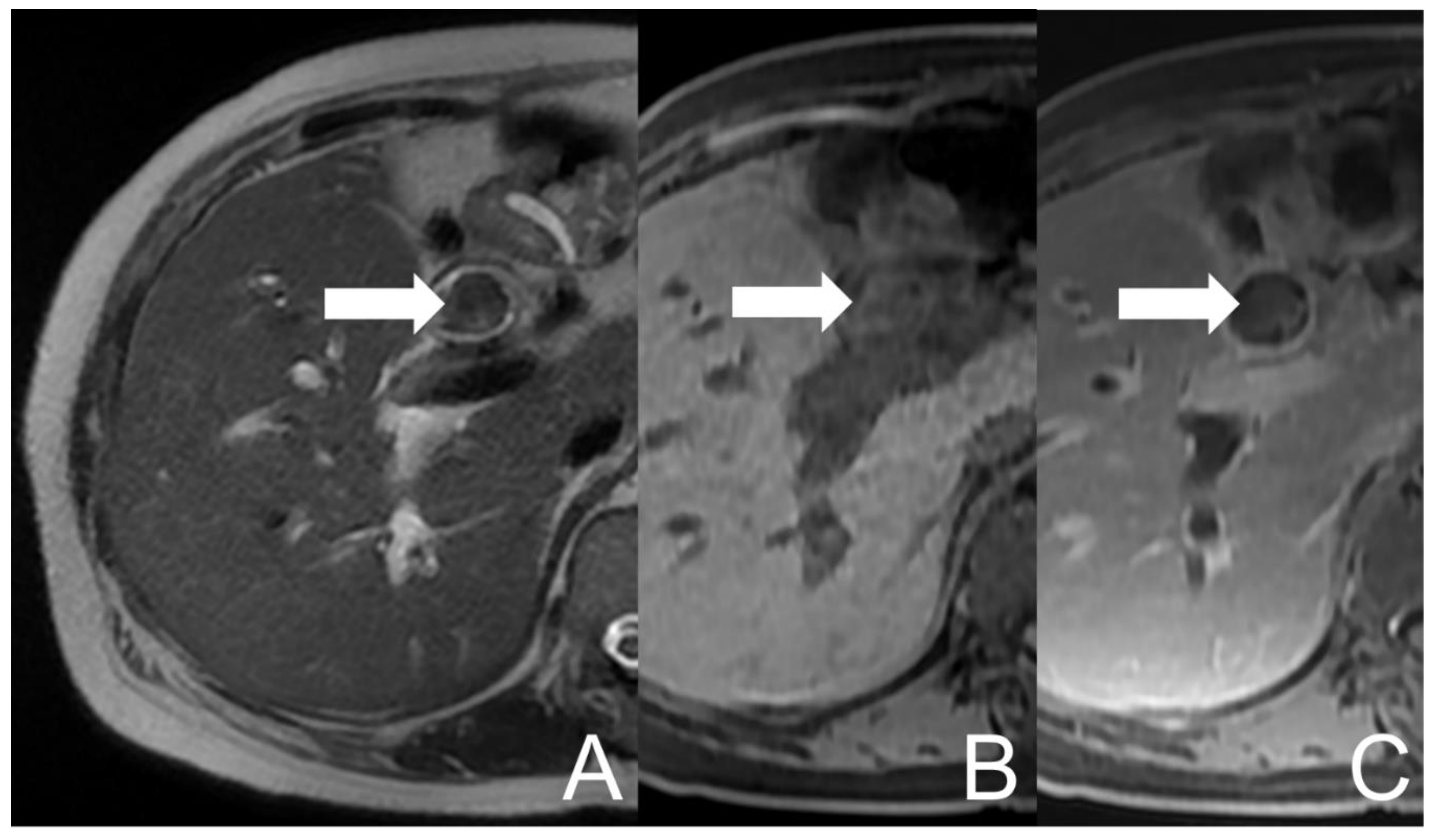
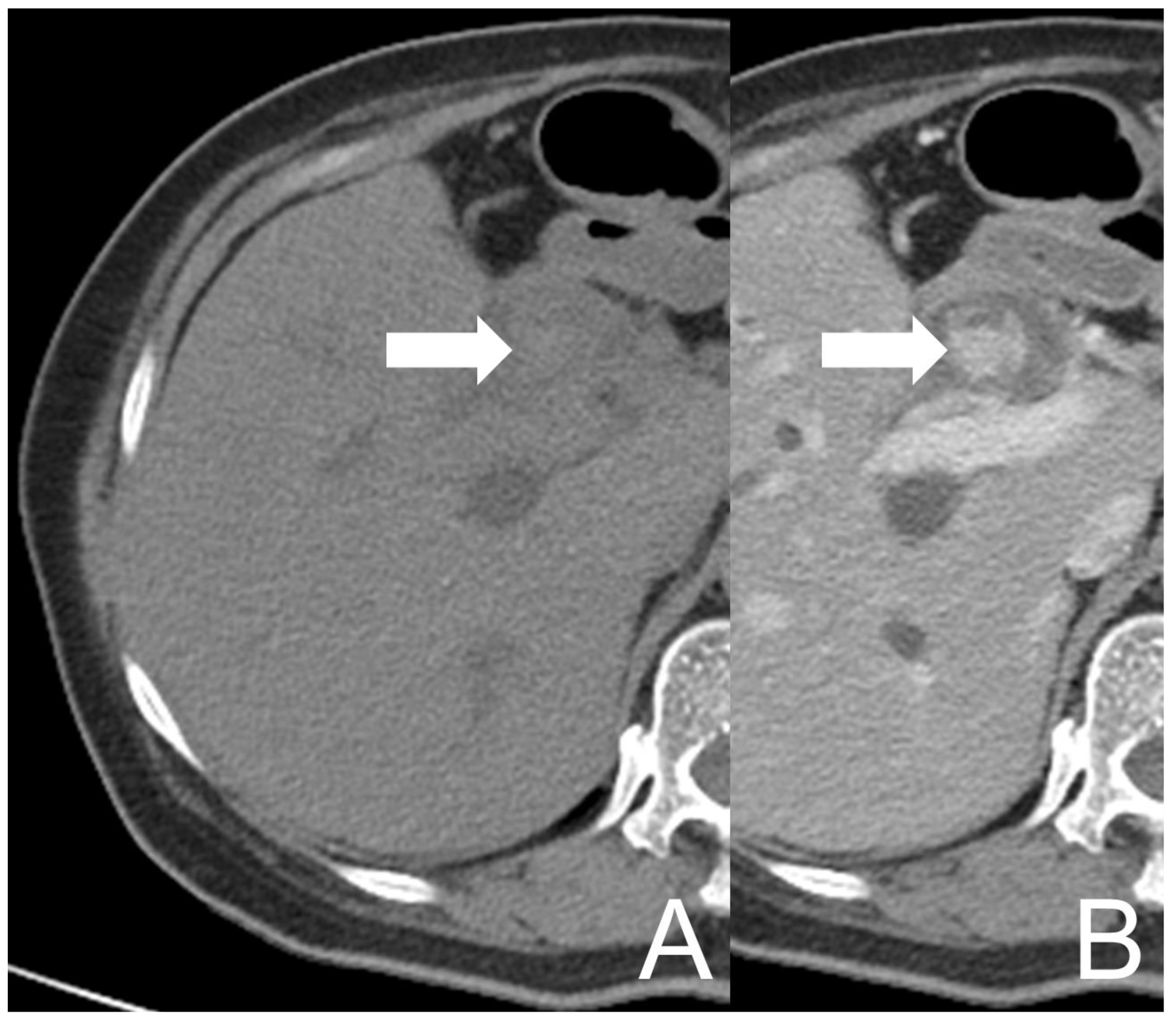
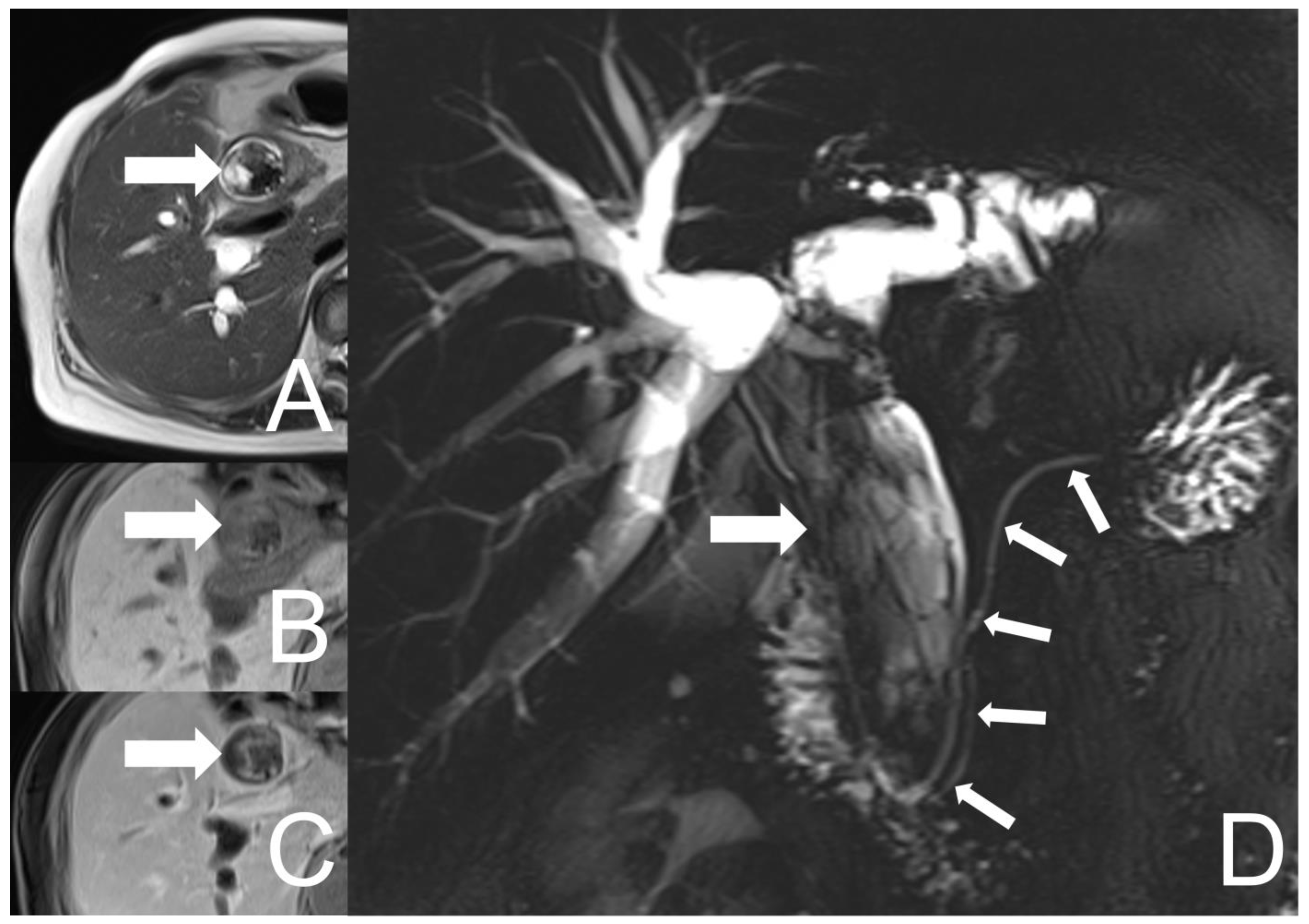
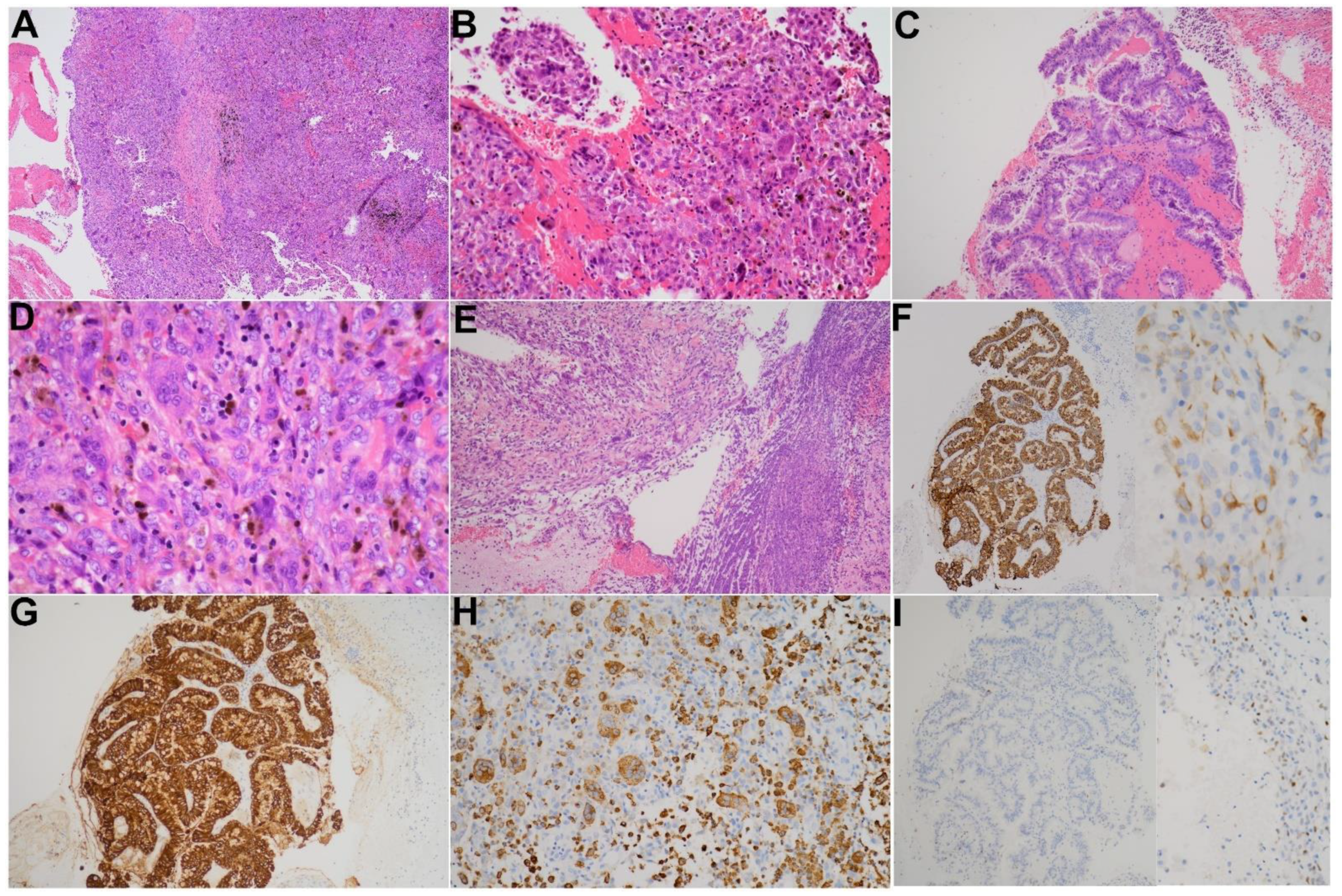
2. Case Description
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arends, M.J.; Fukayama, M.; Klimstra, D.S.; Lam, A.K.Y.; Nagtegaal, I.D.; Odze, R.D.; Paradis, V.; Park, Y.N.; Rugge, M.; Salto-Tellez, M. The WHO Classification of Tumors of the Digestive System, 5th ed.; WHO: Geneva, Switzerland, 2019.
- Hoang, M.P.; Rogers, B.B.; Albores-Saavedra, J. Giant cell tumor of the skin: A morphologic and immunohistochemical study of five cases. Ann. Diagn. Pathol. 2002, 6, 288–293. [Google Scholar] [CrossRef] [PubMed]
- Maheswaran, P.; Addis, B.J. Osteoclastoma-like giant cell tumour of the skin. Histopathology 1990, 16, 604–607. [Google Scholar] [CrossRef] [PubMed]
- Molberg, K.H.; Heffess, C.; Delgado, R.; Albores-Saavedra, J. Undifferentiated carcinoma with osteoclast-like giant cells of the pancreas and periampullary region. Cancer 1998, 82, 1279–1287. [Google Scholar] [CrossRef]
- Cheng, C.H.; Su, B.; Ding, D.C. Rare case of undifferentiated uterine sarcoma with neuroectodermal differentiation and osteoclast-like giant cells. Taiwan J. Obstet. Gynecol. 2018, 57, 442–446. [Google Scholar] [CrossRef]
- Dahm, H.H. Non-Small Cell Carcinoma of the Lung with Osteoclast-Like Giant Cells. Int. J. Surg. Pathol. 2017, 25, 258–261. [Google Scholar] [CrossRef] [Green Version]
- Jimenez-Heffernan, J.A.; Adrados, M.; Munoz-Hernandez, P.; Fernandez-Rico, P.; Ballesteros-Garcia, A.I.; Fraga, J. Cytologic Features of Malignant Melanoma with Osteoclast-Like Giant Cells. Acta Cytol. 2018, 62, 151–154. [Google Scholar] [CrossRef]
- Katoh, M.; Shigematsu, H. Leiomyosarcoma of the heart and its pulmonary metastasis, both with prominent osteoclast-like multinucleated giant cells expressing tartrate-resistant acid phosphatase activity. Pathol. Int. 1999, 49, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Manduch, M.; Dexter, D.F.; Jalink, D.W.; Vanner, S.J.; Hurlbut, D.J. Undifferentiated pancreatic carcinoma with osteoclast-like giant cells: Report of a case with osteochondroid differentiation. Pathol. Res. Pract. 2009, 205, 353–359. [Google Scholar] [CrossRef]
- Mehdi, G.; Ansari, H.A.; Siddiqui, S.A. Cytology of anaplastic giant cell carcinoma of the thyroid with osteoclast-like giant cells—A case report. Diagn. Cytopathol. 2007, 35, 111–112. [Google Scholar] [CrossRef]
- Ohashi, R.; Yanagihara, K.; Namimatsu, S.; Sakatani, T.; Takei, H.; Naito, Z.; Shimizu, A. Osteoclast-like giant cells in invasive breast cancer predominantly possess M2-macrophage phenotype. Pathol. Res. Pract. 2018, 214, 253–258. [Google Scholar] [CrossRef]
- Paal, E.; Thompson, L.D.; Frommelt, R.A.; Przygodzki, R.M.; Heffess, C.S. A clinicopathologic and immunohistochemical study of 35 anaplastic carcinomas of the pancreas with a review of the literature. Ann. Diagn. Pathol. 2001, 5, 129–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tschang, T.P.; Garza-Garza, R.; Kissane, J.M. Pleomorphic carcinoma of the pancreas: An analysis of 15 cases. Cancer 1977, 39, 2114–2126. [Google Scholar] [CrossRef]
- Yonemasu, H.; Takashima, M.; Nishiyama, K.I.; Ueki, T.; Yao, T.; Tanaka, M.; Tsuneyoshi, M. Phenotypical characteristics of undifferentiated carcinoma of the pancreas: A comparison with pancreatic ductal adenocarcinoma and relevance of E-cadherin, alpha catenin and beta catenin expression. Oncol. Rep. 2001, 8, 745–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liao, X.; Houldsworth, J.; Luo, J.; Harpaz, N.; Zhu, H. Polypoid Undifferentiated Carcinoma With Osteoclast-like Giant Cells Arising in the Distal Common Bile Duct: A Rare Case Report. Anticancer Res. 2019, 39, 437–441. [Google Scholar] [CrossRef] [PubMed]
- Albores-Saavedra, J.; Grider, D.J.; Wu, J.; Henson, D.E.; Goodman, Z.D. Giant cell tumor of the extrahepatic biliary tree: A clinicopathologic study of 4 cases and comparison with anaplastic spindle and giant cell carcinoma with osteoclast-like giant cells. Am. J. Surg. Pathol. 2006, 30, 495–500. [Google Scholar] [CrossRef]
- Griglione, N.M.; Klapproth, J.M.; Keilin, S.A. Giant cell tumor of the common bile duct. Clin. Gastroenterol. Hepatol. 2010, 8, A30. [Google Scholar] [CrossRef]
- Kolokotronis, T.; Glanemann, M.; Wagner, M.; Bohle, R.M.; Grunhage, F. Giant cell tumor of the distal common bile duct: Report of a rare, benign entity that may mimic malignant biliary obstruction. Int. J. Colorectal Dis. 2014, 29, 413–414. [Google Scholar] [CrossRef]
- Wang, D.D.; Zheng, Y.M.; Teng, L.H.; Sun, Y.N.; Gao, W.; Wang, L.M.; Wang, Y.H.; Li, F.; Lu, D.H. Benign giant-cell tumor of the common bile duct: A case report. World J. Gastroenterol. 2014, 20, 15448–15453. [Google Scholar] [CrossRef]
- Muraki, T.; Reid, M.D.; Basturk, O.; Jang, K.T.; Bedolla, G.; Bagci, P.; Mittal, P.; Memis, B.; Katabi, N.; Bandyopadhyay, S.; et al. Undifferentiated Carcinoma With Osteoclastic Giant Cells of the Pancreas: Clinicopathologic Analysis of 38 Cases Highlights a More Protracted Clinical Course Than Currently Appreciated. Am. J. Surg. Pathol. 2016, 40, 1203–1216. [Google Scholar] [CrossRef]
- Fukukura, Y.; Kumagae, Y.; Hirahara, M.; Hakamada, H.; Nagano, H.; Nakajo, M.; Kamimura, K.; Nakajo, M.; Higashi, M.; Yoshiura, T. CT and MRI features of undifferentiated carcinomas with osteoclast-like giant cells of the pancreas: A case series. Abdom. Radiol. 2019, 44, 1246–1255. [Google Scholar] [CrossRef]
- Shindoh, N.; Ozaki, Y.; Kyogoku, S.; Nakanishi, A.; Sumi, Y.; Katayama, H. Osteoclast-type giant cell tumor of the pancreas: Helical CT scans. AJR Am. J. Roentgenol. 1998, 170, 653–654. [Google Scholar] [CrossRef] [PubMed]
- Ichikawa, T.; Federle, M.P.; Ohba, S.; Ohtomo, K.; Sugiyama, A.; Fujimoto, H.; Haradome, H.; Araki, T. Atypical exocrine and endocrine pancreatic tumors (anaplastic, small cell, and giant cell types): CT and pathologic features in 14 patients. Abdom. Imaging 2000, 25, 409–419. [Google Scholar] [CrossRef]
- Togawa, Y.; Tonouchi, A.; Chiku, T.; Sano, W.; Doki, T.; Yano, K.; Uno, H.; Muronoi, T.; Kaneoya, K.; Shinagawa, T.; et al. A case report of undifferentiated carcinoma with osteoclast-like giant cells of the pancreas and literature review. Clin. J. Gastroenterol. 2010, 3, 195–203. [Google Scholar] [CrossRef]
- Demetter, P.; Marechal, R.; Puleo, F.; Delhaye, M.; Debroux, S.; Charara, F.; Gomez Galdon, M.; Van Laethem, J.L.; Verset, L. Undifferentiated Pancreatic Carcinoma With Osteoclast-Like Giant Cells: What Do We Know So Far? Front. Oncol. 2021, 11, 630086. [Google Scholar] [CrossRef] [PubMed]
- Zhan, K.; Zhang, S.; Hu, P.; Chen, J.; Liu, W.; Niu, Z. Undifferentiated carcinoma of the pancreas with osteoclast like giant cells: Literature review with CT/MR imaging findings in 3 cases. Radiol. Case Rep. 2022, 17, 2529–2533. [Google Scholar] [CrossRef] [PubMed]
- Luchini, C.; Pea, A.; Lionheart, G.; Mafficini, A.; Nottegar, A.; Veronese, N.; Chianchiano, P.; Brosens, L.A.; Noe, M. Offerhaus, G.J.A.; et al. Pancreatic undifferentiated carcinoma with osteoclast-like giant cells is genetically similar to, but clinically distinct from, conventional ductal adenocarcinoma. J. Pathol. 2017, 243, 148–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wada, T.; Itano, O.; Oshima, G.; Chiba, N.; Ishikawa, H.; Koyama, Y.; Du, W.; Kitagawa, Y. A male case of an undifferentiated carcinoma with osteoclast-like giant cells originating in an indeterminate mucin-producing cystic neoplasm of the pancreas. A case report and review of the literature. World J. Surg. Oncol. 2011, 9, 100. [Google Scholar] [CrossRef] [Green Version]
- Dhall, D.; Klimstra, D.S. The cellular composition of osteoclastlike giant cell-containing tumors of the pancreatobiliary tree. Am. J. Surg. Pathol. 2008, 32, 335–337. [Google Scholar] [CrossRef]
- Athanasou, N.A.; Wells, C.A.; Quinn, J.; Ferguson, D.P.; Heryet, A.; McGee, J.O. The origin and nature of stromal osteoclast-like multinucleated giant cells in breast carcinoma: Implications for tumour osteolysis and macrophage biology. Br. J. Cancer 1989, 59, 491–498. [Google Scholar] [CrossRef] [Green Version]
- Zhou, S.; Yu, L.; Zhou, R.; Li, X.; Yang, W. Invasive breast carcinomas of no special type with osteoclast-like giant cells frequently have a luminal phenotype. Virchows Arch. 2014, 464, 681–688. [Google Scholar] [CrossRef]
- Zhao, X.; Qu, J.; Sun, Y.; Wang, J.; Liu, X.; Wang, F.; Zhang, H.; Wang, W.; Ma, X.; Gao, X.; et al. Prognostic significance of tumor-associated macrophages in breast cancer: A meta-analysis of the literature. Oncotarget 2017, 8, 30576–30586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hahn, S.A.; Kern, S.E. Molecular genetics of exocrine pancreatic neoplasms. Surg. Clin. N. Am. 1995, 75, 857–869. [Google Scholar] [CrossRef]
- Hruban, R.H.; van Mansfeld, A.D.; Offerhaus, G.J.; van Weering, D.H.; Allison, D.C.; Goodman, S.N.; Kensler, T.W.; Bose, K.K.; Cameron, J.L.; Bos, J.L. K-ras oncogene activation in adenocarcinoma of the human pancreas. A study of 82 carcinomas using a combination of mutant-enriched polymerase chain reaction analysis and allele-specific oligonucleotide hybridization. Am. J. Pathol. 1993, 143, 545–554. [Google Scholar] [PubMed]
- Westra, W.H.; Sturm, P.; Drillenburg, P.; Choti, M.A.; Klimstra, D.S.; Albores-Saavedra, J.; Montag, A.; Offerhaus, G.J.; Hruban, R.H. K-ras oncogene mutations in osteoclast-like giant cell tumors of the pancreas and liver: Genetic evidence to support origin from the duct epithelium. Am. J. Surg. Pathol. 1998, 22, 1247–1254. [Google Scholar] [CrossRef] [PubMed]
- Bazzichetto, C.; Luchini, C.; Conciatori, F.; Vaccaro, V.; Di Cello, I.; Mattiolo, P.; Falcone, I.; Ferretti, G.; Scarpa, A.; Cognetti, F.; et al. Morphologic and Molecular Landscape of Pancreatic Cancer Variants as the Basis of New Therapeutic Strategies for Precision Oncology. Int. J. Mol. Sci. 2020, 21, 8841. [Google Scholar] [CrossRef]
- Haratake, J.; Yamada, H.; Horie, A.; Inokuma, T. Giant cell tumor-like cholangiocarcinoma associated with systemic cholelithiasis. Cancer 1992, 69, 2444–2448. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.M.; Kim, H.; Park, Y.N. Sarcomatoid cholangiocarcinoma with osteoclast-like giant cells associated with hepatolithiasis: A case report. Clin. Mol. Hepatol. 2015, 21, 309–313. [Google Scholar] [CrossRef] [Green Version]
- Gao, H.Q.; Yang, Y.M.; Zhuang, Y.; Liu, P. Locally advanced undifferentiated carcinoma with osteoclast-like giant cells of the pancreas. World J. Gastroenterol. 2015, 21, 694–698. [Google Scholar] [CrossRef]
- Hrudka, J.; Lawrie, K.; Waldauf, P.; Ciprova, V.; Moravcova, J.; Matej, R. Negative prognostic impact of PD-L1 expression in tumor cells of undifferentiated (anaplastic) carcinoma with osteoclast-like giant cells of the pancreas: Study of 13 cases comparing ductal pancreatic carcinoma and review of the literature. Virchows Arch. 2020, 477, 687–696. [Google Scholar] [CrossRef]
- Luchini, C.; Cros, J.; Pea, A.; Pilati, C.; Veronese, N.; Rusev, B.; Capelli, P.; Mafficini, A.; Nottegar, A.; Brosens, L.A.A.; et al. PD-1, PD-L1, and CD163 in pancreatic undifferentiated carcinoma with osteoclast-like giant cells: Expression patterns and clinical implications. Hum. Pathol. 2018, 81, 157–165. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case No. | Age/Sex | Clinical Presentation | Location | Gross Features | Treatment | Follow-Up | Reference |
|---|---|---|---|---|---|---|---|
| 1 | 56/M | Jaundice, abdominal pain | Distal CBD | 1.6 cm, polypoid | Whipple procedure | Free of disease 50 months after surgery | [16] |
| 2 | 60/M | Obstructive jaundice | Distal CBD | 1 cm, polypoid | Whipple procedure | No | [16] |
| 3 | 60/M | Asymptomatic | Distal CBD | 1.5 cm, polypoid | Whipple procedure | Free of disease 16 months after surgery | [17] |
| 4 | 73/F | Abdominal pain | Distal CBD | 2.5 cm × 0.7 cm | Pylorus-preserving pancreas head resection and pancreaticogastrostomy | No | [18] |
| 5 | 81/M | Jaundice | Middle CBD | 1.5 cm × 0.6 cm, polypoid | Excision of the gallbladder and extrahepatic bile duct and a Roux-en-Y cholangiojejunostomy | Free of disease 6 months after surgery | [19] |
| 6 | 66/F | Jaundice and fever | Entire CBD and CHD | 11.3 cm, lobulated | Choledocoscopic tissue removal | Free of disease 12 months after surgery | Our case |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.-H.; Li, H.-N. Undifferentiated Carcinoma with Osteoclast-Like Giant Cells of the Common Bile Duct: A Case Report of a Rare Entity at an Unusual Location. Diagnostics 2022, 12, 1517. https://doi.org/10.3390/diagnostics12071517
Chen C-H, Li H-N. Undifferentiated Carcinoma with Osteoclast-Like Giant Cells of the Common Bile Duct: A Case Report of a Rare Entity at an Unusual Location. Diagnostics. 2022; 12(7):1517. https://doi.org/10.3390/diagnostics12071517
Chicago/Turabian StyleChen, Chuan-Han, and Hsin-Ni Li. 2022. "Undifferentiated Carcinoma with Osteoclast-Like Giant Cells of the Common Bile Duct: A Case Report of a Rare Entity at an Unusual Location" Diagnostics 12, no. 7: 1517. https://doi.org/10.3390/diagnostics12071517