
Multitarget Molecular Imaging in Metastatic Castration Resistant Adenocarcinoma Prostate Cancer with Therapy Induced Neuroendocrine Differentiation

 ,
, 
 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
- (a)
- Patients with metastatic CRPC (CRPCm) and histologically proven neuroendocrine prostate cancer.
- (b)
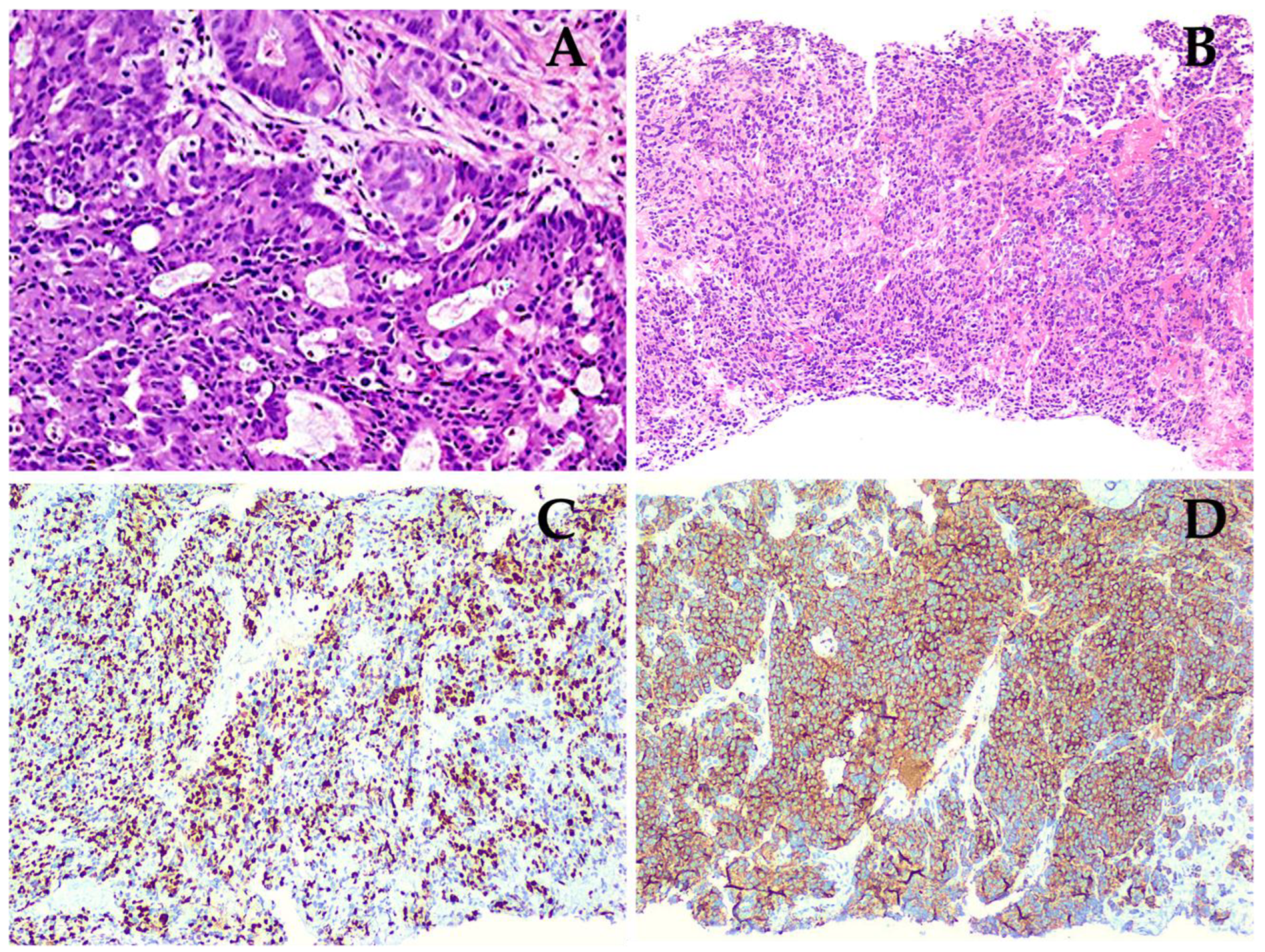
- First initial diagnosis biopsy-proven with adenocarcinoma PCa with a second biopsy that confirmed NE differentiation with immunohistochemical markers (chromogranin and synaptophysin).
- (c)
- Prior treatment based on androgen deprivation therapy, chemotherapy, novel androgen receptor pathway inhibitor or a combination of each one of them.
- (a)
- Patients who had other primary malignancies at the time of examination.
- (b)
- Non-histopathological NEPC confirmation. NEPC was defined by the presence of either pure small/large-cell carcinoma (by tumour morphology) or mixed histology with both adenocarcinoma and small/large-cell neuroendocrine carcinoma along with positive neuroendocrine immunohistochemical markers [17].
2.2. Image Acquisition
2.3. Image Analysis
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Cancer Institute—Surveillance, Epidemiology, and End Results Program (SEER). Cancer Stat Facts: Prostate Cancer. Available online: https://seer.cancer.gov/statfacts/html/prost.html (accessed on 30 March 2021).
- World Health Organization. International Agency for Research on Cancer—GLOBOCAN 2020. Available online: https://gco.iarc.fr/ (accessed on 30 March 2021).
- Barron, D.A.; Rowley, D.R. The reactive stroma microenvironment and prostate cancer progression. Endocr. Relat. Cancer 2012, 19, R187–R204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- You, S.; Knudsen, B.S.; Erho, N.; Alshalalfa, M.; Takhar, M.; Al-Deen Ashab, H.; Davicioni, E.; Karnes, R.J.; Klein, E.A.; Den, R.B.; et al. Integrated Classification of Prostate Cancer Reveals a Novel Luminal Subtype wth Poor Outcome. Cancer Res. 2016, 76, 4948–4958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nuhn, P.; De Bono, J.S.; Fizazi, K.; Freedland, S.J.; Grilli, M.; Kantoff, P.W.; Sonpavde, G.; Sternberg, C.N.; Yegnasubramanian, S.; Antonarakis, E.S. Update on Systemic Prostate Cancer Therapies: Management of Metastatic Castration-resistant Prostate Cancer in the Era of Precision Oncology. Eur. Urol. 2018, 75, 88–99. [Google Scholar] [CrossRef] [PubMed]
- Hu, C.-D.; Choo, R.; Huang, J. Neuroendocrine Differentiation in Prostate Cancer: A Mechanism of Radioresistance and Treatment Failure. Front. Oncol. 2015, 5, 90. [Google Scholar] [CrossRef] [Green Version]
- Dicken, H.; Hensley, P.J.; Kyprianou, N. Prostate tumor neuroendocrine differentiation via EMT: The road less traveled. Asian J. Urol. 2019, 6, 82–90. [Google Scholar] [CrossRef]
- Patel, G.K.; Chugh, N.; Tripathi, M. Neuroendocrine Differentiation of Prostate Cancer—An Intriguing Example of Tumor Evolution at Play. Cancers 2019, 11, 1405. [Google Scholar] [CrossRef] [Green Version]
- Beltran, H.; Rickman, D.S.; Park, K.; Chae, S.S.; Sboner, A.; MacDonald, T.Y.; Wang, Y.; Sheikh, K.L.; Terry, S.; Tagawa, S.T.; et al. Molecular Characterization of Neuroendocrine Prostate Cancer and Identification of New Drug Targets. Cancer Discov. 2011, 1, 487–495. [Google Scholar] [CrossRef] [Green Version]
- Papandreou, C.N.; Daliani, D.D.; Thall, P.F.; Tu, S.-M.; Wang, X.; Reyes, A.; Troncoso, P.; Logothetis, C.J. Results of a Phase II Study with Doxorubicin, Etoposide, and Cisplatin in Patients with Fully Characterized Small-Cell Carcinoma of the Prostate. J. Clin. Oncol. 2002, 20, 3072–3080. [Google Scholar] [CrossRef]
- Maurer, T.; Eiber, M.; Schwaiger, M.E.M.; Gschwend, T.M.J.E. Current use of PSMA–PET in prostate cancer management. Nat. Rev. Urol. 2016, 13, 226–235. [Google Scholar] [CrossRef]
- Hofman, M.S.; Lawrentschuk, N.; Francis, R.; Tang, C.; Vela, I.; Thomas, P.; Rutherford, N.; Martin, J.M.; Frydenberg, M.; Shakher, R.; et al. Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): A prospective, randomised, multicentre study. Lancet 2020, 395, 1208–1216. [Google Scholar] [CrossRef]
- Gofrit, O.N.; Frank, S.; Meirovitz, A.; Nechushtan, H.; Orevi, M. PET/CT With 68Ga-DOTA-TATE for Diagnosis of Neuroendocrine: Differentiation in Patients with Castrate-Resistant Prostate Cancer. Clin. Nucl. Med. 2017, 42, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zuckier, L.S.; Ghesani, N.V. Dominant uptake of fatty acid over glucose by prostate cells: A potential new diagnostic and therapeutic approach. Anticancer Res. 2010, 30, 369–374. [Google Scholar] [PubMed]
- Reinicke, K.; Sotomayor, P.; Cisterna, P.; Delgado, C.; Nualart, F.; Godoy, A. Cellular distribution of Glut-1 and Glut-5 in benign and malignant human prostate tissue. J. Cell. Biochem. 2012, 113, 553–562. [Google Scholar] [CrossRef] [PubMed]
- Spratt, D.E.; Gavane, S.; Tarlinton, L.; Fareedy, S.B.; Doran, M.G.; Zelefsky, M.J.; Osborne, J.R. Utility of FDG-PET in clinical neuroendocrine prostate cancer. Prostate 2014, 74, 1153–1159. [Google Scholar] [CrossRef] [Green Version]
- Conteduca, V.; Oromendia, C.; Eng, K.W.; Bareja, R.; Sigouros, M.; Molina, A.; Faltas, B.M.; Sboner, A.; Mosquera, J.M.; Elemento, O.; et al. Clinical features of neuroendocrine prostate cancer. Eur. J. Cancer 2019, 121, 7–18. [Google Scholar] [CrossRef]
- Mohler, J.L.; Antonarakis, E.S.; Armstrong, A.J.; D’Amico, A.V.; Davis, B.J.; Dorff, T.; Eastham, J.A.; Enke, C.A.; Farrington, T.A.; Higano, C.S.; et al. Prostate cancer, version 2.2022, NCCN clinical Practice guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2021, 17, 479–505. [Google Scholar] [CrossRef] [Green Version]
- Spetsieris, N.; Boukovala, M.; Patsakis, G.; Alafis, I.; Efstathiou, E. Neuroendocrine and Aggressive-Variant Prostate Cancer. Cancers 2020, 12, 3792. [Google Scholar] [CrossRef]
- Hope, T.A.; Goodman, J.Z.; Allen, I.E.; Calais, J.; Fendler, W.P.; Carroll, P.R. Metaanalysis of 68Ga-PSMA-11 PET Accuracy for the Detection of Prostate Cancer Validated by Histopathology. J. Nucl. Med. 2018, 60, 786–793. [Google Scholar] [CrossRef] [Green Version]
- Sartor, O.; de Bono, J.; Chi, K.N.; Fizazi, K.; Herrmann, K.; Rahbar, K.; Tagawa, S.T.; Nordquist, L.T.; Vaishampayan, N.; El-Haddad, G.; et al. Lutetium-177–PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2021, 385, 1091–1103. [Google Scholar] [CrossRef]
- Taher, A.; Jensen, C.T.; Yedururi, S.; Surasi, D.S.; Faria, S.C.; Bathala, T.K.; Mujtaba, B.; Bhosale, P.; Wagner-Bartak, N.; Morani, A.C. Imaging of Neuroendocrine Prostatic Carcinoma. Cancers 2021, 13, 5765. [Google Scholar] [CrossRef]
- Bakht, M.K.; Derecichei, I.; Li, Y.; Ferraiuolo, R.-M.; Dunning, M.J.; Oh, S.W.; Hussein, A.; Youn, H.; Stringer, K.F.; Jeong, C.W.; et al. Neuroendocrine differentiation of prostate cancer leads to PSMA suppression. Endocr. Relat. Cancer 2019, 26, 131–146. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, R.; Huang, J.; Alumkal, J.J.; Zhang, L.; Feng, F.Y.; Thomas, G.; Weinstein, A.; Friedl, V.; Zhang, C.; Witte, O.N.; et al. Clinical and Genomic Characterization of Treatment-Emergent Small-Cell Neuroendocrine Prostate Cancer: A Multi-institutional Prospective Study. J. Clin. Oncol. 2018, 36, 2492–2503. [Google Scholar] [CrossRef]
- Shen, K.; Liu, B.; Zhou, X.; Ji, Y.; Chen, L.; Wang, Q.; Xue, W. The Evolving Role of 18F-FDG PET/CT in Diagnosis and Prognosis Prediction in Progressive Prostate Cancer. Front. Oncol. 2021, 11, 2436. [Google Scholar] [CrossRef] [PubMed]
- Perez, P.M.; Hope, T.A.; Behr, S.C.; van Zante, A.; Small, E.J.; Flavell, R.R. Intertumoral Heterogeneity of 18F-FDG and 68Ga-PSMA Uptake in Prostate Cancer Pulmonary Metastases. Clin. Nucl. Med. 2019, 44, e28–e32. [Google Scholar] [CrossRef] [PubMed]
- Thang, S.P.; Violet, J.; Sandhu, S.; Iravani, A.; Akhurst, T.; Kong, G.; Kumar, A.R.; Murphy, D.G.; Williams, S.G.; Hicks, R.J.; et al. Poor Outcomes for Patients with Metastatic Castration-resistant Prostate Cancer with Low Prostate-specific Membrane Antigen (PSMA) Expression Deemed Ineligible for 177Lu-labelled PSMA Radioligand Therapy. Eur. Urol. Oncol. 2018, 2, 670–676. [Google Scholar] [CrossRef] [PubMed]
- Parida, G.K.; Tripathy, S.; Gupta, S.D.; Singhal, A.; Kumar, R.; Bal, C.; Shamim, S.A. Adenocarcinoma Prostate with Neuroendocrine Differentiation: Potential Utility of 18F-FDG PET/CT and 68Ga-DOTANOC PET/CT Over 68Ga-PSMA PET/CT. Clin. Nucl. Med. 2018, 43, 248–249. [Google Scholar] [CrossRef]
- Bakht, M.K.; Lovnicki, J.M.; Tubman, J.; Stringer, K.F.; Chiaramonte, J.; Reynolds, M.R.; Derecichei, I.; Ferraiuolo, R.-M.; Fifield, B.-A.; Lubanska, D.; et al. Differential Expression of Glucose Transporters and Hexokinases in Prostate Cancer with a Neuroendocrine Gene Signature: A Mechanistic Perspective for 18F-FDG Imaging of PSMA-Suppressed Tumors. J. Nucl. Med. 2019, 61, 904–910. [Google Scholar] [CrossRef]
- Graham, M.M.; Gu, X.; Ginader, T.; Breheny, P.; Sunderland, J. 68Ga-DOTATOC Imaging of Neuroendocrine Tumors: A Systematic Review and Metaanalysis. J. Nucl. Med. 2017, 58, 1452–1458. [Google Scholar] [CrossRef] [Green Version]
- Usmani, S.; Ahmed, N.; Marafi, F.; Rasheed, R.; Amanguno, H.G.; al Kandari, F. Molecular Imaging in Neuroendocrine Differentiation of Prostate Cancer: 68Ga-PSMA versus 68Ga-DOTA NOC PET-CT. Clin. Nucl. Med. 2017, 42, 410–413. [Google Scholar] [CrossRef]
- Bilen, M.A.; Akintayo, A.A.; Abiodun-Ojo, O.A.; Kucuk, O.; Carthon, B.C.; Schuster, D.M.; Parent, E.E. The role of 68Ga-DOTATATE for evaluation of patients with metastatic castration-resistant prostate cancer (mCRPC). J. Clin. Oncol. 2020, 38, 217. [Google Scholar] [CrossRef]
- Iravani, A.; Mitchell, C.; Akhurst, T.; Sandhu, S.; Hofman, M.S.; Hicks, R.J. Molecular Imaging of Neuroendocrine Differentiation of Prostate Cancer: A Case Series. Clin. Genitourin. Cancer 2021, 19, e200–e205. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Age (Years) | Initial HPE 1 | Gleason | Treatment | Type of Treatment | Second HPE 1 | Site of 2° Biopsy | Time to NED 2 | PSA 3 (ng/dL) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 75 | Pac 4 | 9 (4 + 5) | Sx 6 RP 7 + ADT 9+ ChT 10 | Enzalutamide, Gosereline, Docetaxel, Cabazitaxel, Carboplatin | NEC 11 | Bone | 108 | 13.5 |
| 2 | 59 | PMAc 5 | 8 (4 + 4) | ADT + ChT | Bicalutamide, Leuprorelin, Docetaxel, Abiraterone, Etoposide, Carboplatin | LCNEC 12 | Lung | 14 | 0.2 |
| 3 | 77 | PAc | 9 (4 + 5) | ADT + ChT | Goserelin, Docetaxel, Etoposide, Carboplatin | NEC | Bone | 48 | 0.003 |
| 4 | 54 | PAc | 9 (4 + 5) | Sx TURP 8 + ADT + ChT | Degarelix, Abiraterone, Docetaxel, Carboplatin, Etoposide, Irinotecan | NEC | Post Sx Bed/Prostate | 15 | 137.3 |
| 5 | 66 | PAc | 9 (4 + 5) | ADT + ChT | Goserelin, Docetaxel, Abiraterone, Enzalutamide, Cabazitaxel | NEC | Prostate | 24 | 157 |
| 6 | 86 | PAc | 9 (5 + 4) | Sx TURP + ADT + ChT | Leuprorelin, Bicalutamide, Etoposide, Docetaxel, Carboplatin | LCNEC | Post Sx Bed/Prostate | 13 | 5.3 |
| 7 | 67 | PAc | 8 (4 + 4) | ADT + ChT | Degarelix, Goserelin, Abiraterone, Docetaxel, Enzalutamide, Cabazitaxel | NEC | Liver | 48 | 19.8 |
| 8 | 86 | PAc | 9 (5 + 4) | ADT + ChT | Bicalutamide, Goserelin, Abiraterone | NEC | Prostate | 36 | 140 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vargas Ahumada, J.; González Rueda, S.D.; Sinisterra Solís, F.A.; Pitalúa Cortés, Q.; Torres Agredo, L.P.; Miguel, J.R.; Scavuzzo, A.; Soldevilla-Gallardo, I.; Álvarez Avitia, M.A.; Sobrevilla, N.; et al. Multitarget Molecular Imaging in Metastatic Castration Resistant Adenocarcinoma Prostate Cancer with Therapy Induced Neuroendocrine Differentiation. Diagnostics 2022, 12, 1387. https://doi.org/10.3390/diagnostics12061387
Vargas Ahumada J, González Rueda SD, Sinisterra Solís FA, Pitalúa Cortés Q, Torres Agredo LP, Miguel JR, Scavuzzo A, Soldevilla-Gallardo I, Álvarez Avitia MA, Sobrevilla N, et al. Multitarget Molecular Imaging in Metastatic Castration Resistant Adenocarcinoma Prostate Cancer with Therapy Induced Neuroendocrine Differentiation. Diagnostics. 2022; 12(6):1387. https://doi.org/10.3390/diagnostics12061387
Chicago/Turabian StyleVargas Ahumada, Joel, Sofía D. González Rueda, Fabio A. Sinisterra Solís, Quetzali Pitalúa Cortés, Liliana P. Torres Agredo, Jimenez Ríos Miguel, Anna Scavuzzo, Irma Soldevilla-Gallardo, Miguel A. Álvarez Avitia, Nora Sobrevilla, and et al. 2022. "Multitarget Molecular Imaging in Metastatic Castration Resistant Adenocarcinoma Prostate Cancer with Therapy Induced Neuroendocrine Differentiation" Diagnostics 12, no. 6: 1387. https://doi.org/10.3390/diagnostics12061387