
Subepithelial Hyalinisation Predicts Recurrence of Unicystic Ameloblastomas

 ,
, 



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
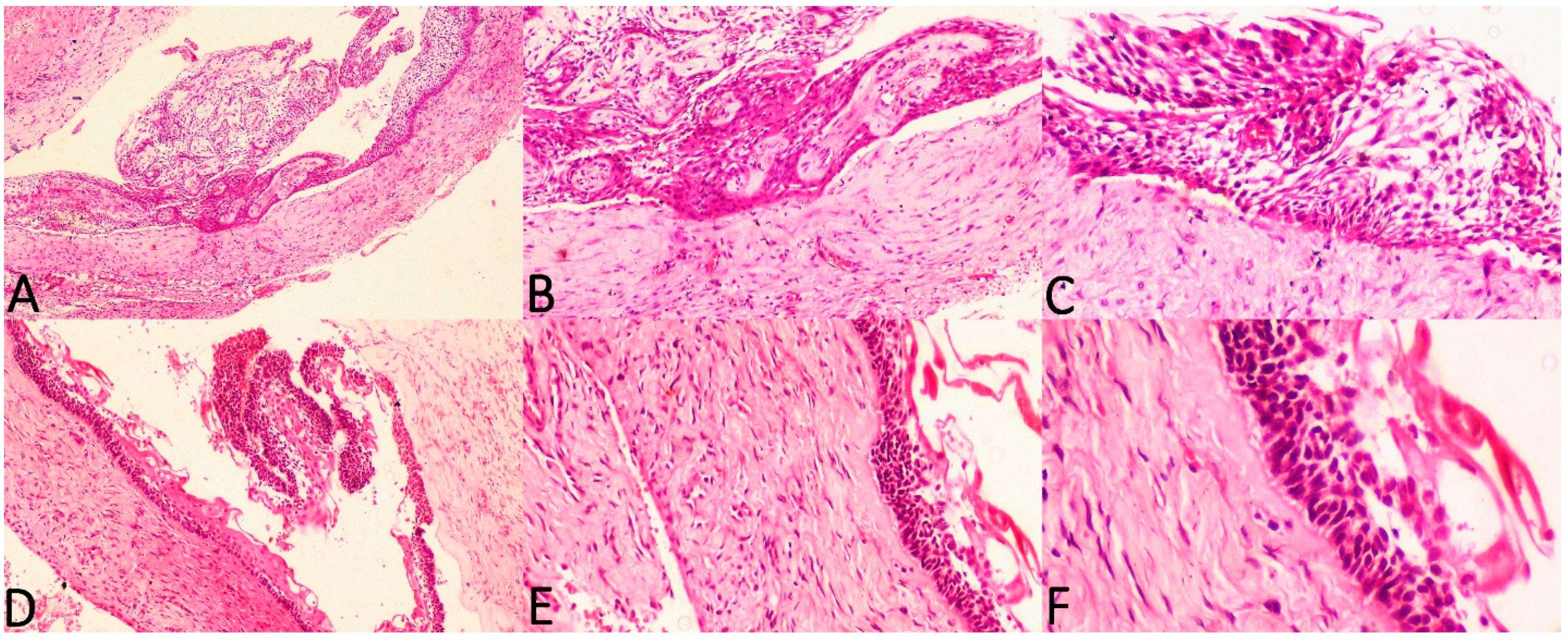
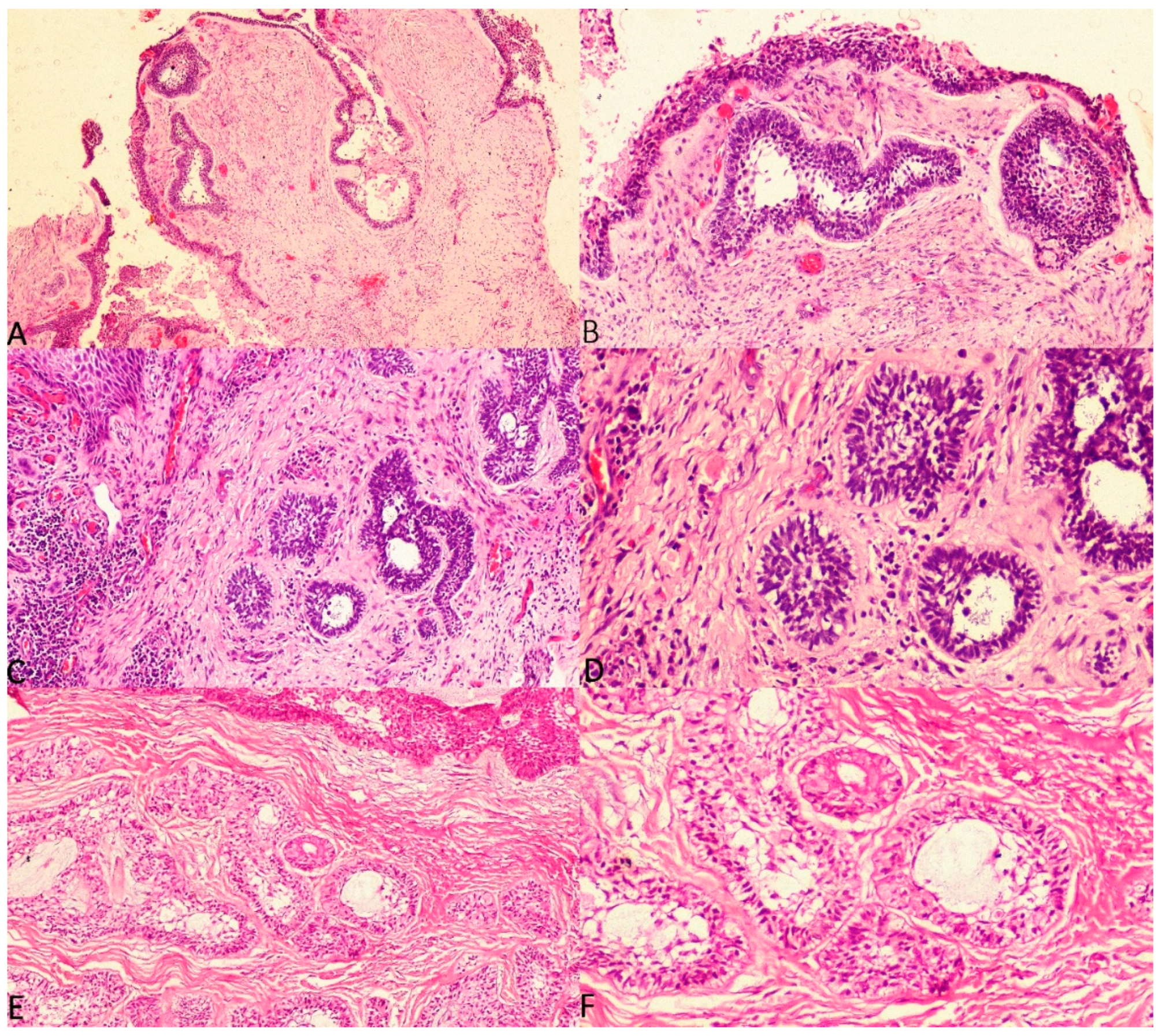
2.2. Histopathological Correlation of Hyalinisation in UA with Recurrence
2.3. Clinicopathological Correlation of UA with Recurrence
2.4. Interpretation and Analysis
3. Results
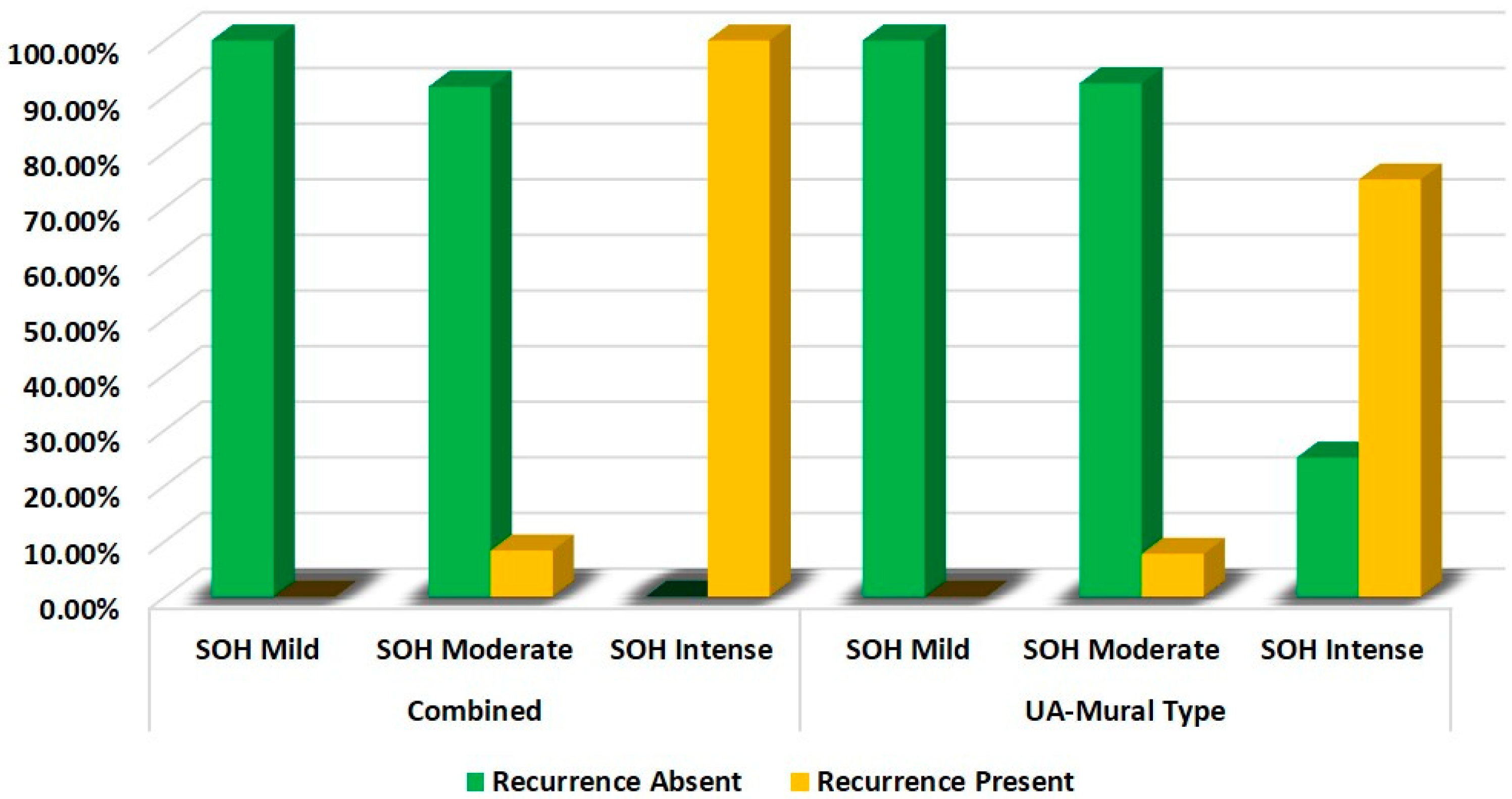
3.1. Correlation of Histological Parameter with SOH
3.2. Correlation between Clinical Parameters and Recurrence
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- von Böhl, M.; Kuijpers-Jagtman, A.M. Hyalinization during orthodontic tooth movement: A systematic review on tissue reactions. Eur. J. Orthod. 2009, 31, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.K. The wonderful colors of the hematoxylin-eosin stain in diagnostic surgical pathology. Int. J. Surg. Pathol. 2014, 22, 12–32. [Google Scholar] [CrossRef] [PubMed]
- Wright, J.M.; Soluk Tekkesin, M. Odontogenic tumours: Where are we in 2017? J. Istanb. Univ. Fac. Dent. 2017, 51 (Suppl. 1), S10–S30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masthan, K.M.; Anitha, N.; Krupaa, J.; Manikkam, S. Ameloblastoma. J. Pharm. Bioallied. Sci. 2015, 7 (Suppl. 1), S167–S170. [Google Scholar] [CrossRef] [PubMed]
- Li, T.J.; Wu, Y.T.; Yu, S.F.; Yu, G.Y. Unicystic ameloblastoma: A clinicopathologic study of 33 Chinese patients. Am. J. Surg. Pathol. 2000, 24, 1385–1392. [Google Scholar] [CrossRef]
- Kim, J.; Nam, E.; Yoon, S. Conservative management (marsupialization) of unicystic ameloblastoma: Literature review and a case report. Maxillofac. Plast. Reconstr. Surg. 2017, 39, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saluja, T.; Iyer, J. Unmasking the Grey Zone of Hyalinization with a Proposed Classification of Oral Hyalinizing Lesions. J. Interdiscip. Histopathol. 2017, 5, 18–21. [Google Scholar] [CrossRef]
- Singh, A.; Shaikh, S.; Samadi, F.M.; Shrivastava, S.; Verma, R. Maxillary unicystic ameloblastoma: A review of the literature. Natl. J. Maxillofac. Surg. 2011, 2, 163–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tummers, M.; Thesleff, I. The importance of signal pathway modulation in all aspects of tooth development. J. Exp. Zool. Part B Mol. Dev. Evol. 2009, 312, 309–319. [Google Scholar] [CrossRef]
- Ueno, H.; Ishiguro, M.; Nakatani, E.; Ishikawa, T.; Uetake, H.; Murotani, K.; Matsui, S.; Teramukai, S.; Sugai, T.; Ajioka, Y.; et al. Prognostic value of desmoplastic reaction characterization in stage II colon cancer: Prospective validation in a Phase 3 study (SACURA Trial). Br. J. Cancer 2021, 124, 1088–1097. [Google Scholar] [CrossRef] [PubMed]
- Cottom, H.E.; Bshena, F.I.; Speight, P.M.; Craig, G.T.; Jones, A.V. Histopathological features that predict the recurrence of odontogenic keratocysts. J. Oral Pathol. Med. 2012, 41, 408–414. [Google Scholar] [CrossRef] [PubMed]
- Katabi, N.; Xu, B. Salivary gland neoplasms: Diagnostic approach with focus on patterns of recognition and useful ancillary tools. Diagn. Histopathol. 2018, 24, 180–188. [Google Scholar] [CrossRef]
- Satish, V.; Prabhadevi, M.C.; Sharma, R. Odontome: A Brief Overview. Int. J. Clin. Pediatr. Dent. 2011, 4, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Jahagirdar, P.B.; Kale, A.D.; Hallikerimath, S. Stromal characterization and comparison of odontogenic cysts and odontogenic tumours using picrosirius red stain and polarizing microscopy: A retrospective and histochemical study. Indian J. Cancer 2015, 52, 408–412. [Google Scholar] [CrossRef] [PubMed]
- Singh, E.; Pujari, R.K.; Murgod, S.; Girish, H.C. Odontogenic tumour patterns: An introspective analysis. Br. J. Med. Res. 2016, 11, 1–17. [Google Scholar] [CrossRef]
- Siwach, P.; Joy, T.; Tupkari, J.; Thakur, A. Controversies in Odontogenic Tumours: Review. Sultan Qaboos Univ. Med. J. 2017, 17, e268–e276. [Google Scholar] [CrossRef]
- Su, C.Y.; Li, J.Q.; Zhang, L.L.; Wang, H.; Wang, F.H.; Tao, Y.W.; Wang, Y.Q.; Guo, Q.R.; Li, J.J.; Liu, Y.; et al. The Biological Functions and Clinical Applications of Integrins in Cancers. Front. Pharmacol. 2020, 11, 579068. [Google Scholar] [CrossRef]
- Angadi, P.V. Head and neck: Odontogenic tumour: Ameloblastoma Atlas Genet. Cytogenet. Oncol. Haematol. 2011, 15, 223–229. [Google Scholar]
- Sathi, G.S.; Fujii, M.; Tamamura, R.; Borkosky, S.S.; Katase, N.; Kawakami, T.; Nagatsuka, H.; Nagai, N. Juxta-epithelial hyalinization inhibits tumour growth and invasion in ameloblastoma. J. Hard Tissue Biol. 2008, 17, 63–68. [Google Scholar] [CrossRef] [Green Version]
- Dandriyal, R.; Gupta, A.; Pant, S.; Baweja, H.H. Surgical management of ameloblastoma: Conservative or radical approach. Natl. J. Maxillofac. Surg. 2011, 2, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Wu, Y.; Yu, S.; Yu, G. Clinicopathological features of unicystic ameloblastoma with special reference to its recurrence. Chin. J. Stomatol. 2002, 37, 210–212. [Google Scholar]
- Cadavid, A.M.; Araujo, J.P.; Coutinho-Camillo, C.M.; Bologna, S.; Junior, C.A.; Lourenço, S.V. Ameloblastomas: Current aspects of the new WHO classification in an analysis of 136 cases. Surg. Exp. Pathol. 2019, 2, 17. [Google Scholar] [CrossRef]
- Ahmed, S.P.; Gunasekaran, N.; Arunachalam, P.; Annasamy, R.K. Mural unicystic ameloblastoma with multifarious histopathological patterns: An exquisite case report. Indian J. Dent. Res. 2020, 31, 803. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Frequency | Percentage (%) |
|---|---|---|
| Age Groups | ||
| 0–20 | 9 | 15.0 |
| 21–40 | 28 | 46.7 |
| 41–60 | 18 | 30.0 |
| >61 | 5 | 8.3 |
| Gender | ||
| Male | 38 | 63.3 |
| Female | 22 | 36.7 |
| Size | ||
| 1–2 cm | 14 | 23.3 |
| 3–4 cm | 14 | 23.3 |
| >4 cm | 32 | 53.3 |
| Region | ||
| Body of Mandible | 22 | 36.7 |
| Angle of Mandible | 29 | 48.3 |
| Symphysis | 8 | 13.3 |
| Retromolar Trigone | 0 | 0.0 |
| Maxillary Sinus | 1 | 1.7 |
| Jaw | ||
| Maxilla | 1 | 1.7 |
| Mandible | 59 | 98.3 |
| Groups | SOH | Recurrence | χ2 | p-Value | |
|---|---|---|---|---|---|
| Absent | Present | ||||
| UA-Intraluminal Type | Mild | 100.0% | 0.0% | - | - |
| Moderate | 100.0% | 0.0% | |||
| Intense | - | - | |||
| UA-Luminal Type | Mild | 90.0% | 10.0% | 15.950 | 0.001 |
| Moderate | 87.5% | 12.5% | |||
| Intense | 0.0% | 100.0% | |||
| UA-Mural Type | Mild | 100.0% | 0.0% | 14.024 | 0.001 |
| Moderate | 92.3% | 7.7% | |||
| Intense | 25.0% | 75.0% | |||
| Groups | SOH | Recurrence | χ2 | p-Value | |
|---|---|---|---|---|---|
| Absent | Present | ||||
| Combined (UA-Intraluminal and UA-Luminal Type) | Mild | 100.0% | 0.0% | 22.067 | 0.001 |
| Moderate | 91.7% | 8.3% | |||
| Intense | 0.0% | 100.0% | |||
| UA-Mural Type | Mild | 100.0% | 0.0% | 14.024 | 0.001 |
| Moderate | 92.3% | 7.7% | |||
| Intense | 25.0% | 75.0% | |||
| Clinical Parameters | Recurrence | χ2 | p-Value | ||
|---|---|---|---|---|---|
| Absent | Present | ||||
| Age Groups | 0–20 | 33.3% | 66.7% | 4.072 | 0.254 |
| 21–40 | 60.0% | 40.0% | |||
| 41–60 | 70.0% | 30.0% | |||
| >61 | 0.0% | 100.0% | |||
| Gender | Male | 55.6% | 44.4% | 0.023 | 0.880 |
| Female | 58.3% | 41.7% | |||
| Region | Body of Mandible | 50.0% | 50.0% | 3.529 | 0.171 |
| Angle of Mandible | 50.0% | 50.0% | |||
| Symphysis | 100.0% | 0.0% | |||
| Retromolar Trigone | - | - | |||
| Maxillary Sinus | - | - | |||
| Size | 1–2 cm | 57.1% | 42.9% | 3.202 | 0.202 |
| 3–4 cm | 28.6% | 71.4% | |||
| >4 cm | 68.8% | 31.2% | |||
| Jaw | Maxilla | - | - | - | - |
| Mandible | 56.7% | 43.3% | |||
| Radiographic Features | Unilocular Radiolucency | 85.0% | 15.0% | 19.615 | 0.001 |
| Multilocular Radiolucency | 0.0% | 100.0% | |||
| Cortical Expansion | Absent | 66.7% | 33.3% | 0.305 | 0.580 |
| Present | 54.2% | 45.8% | |||
| Root Resorption | Absent | 64.3% | 35.7% | 0.621 | 0.431 |
| Present | 50.0% | 50.0% | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Augustine, D.; Rao, R.S.; Surendra, L.; Gupta, B.; Yoithapprabhunath, T.R.; Yadalam, P.K.; Mushtaq, S.; Ahmed, Z.H.; Patil, S. Subepithelial Hyalinisation Predicts Recurrence of Unicystic Ameloblastomas. Diagnostics 2022, 12, 756. https://doi.org/10.3390/diagnostics12030756
Augustine D, Rao RS, Surendra L, Gupta B, Yoithapprabhunath TR, Yadalam PK, Mushtaq S, Ahmed ZH, Patil S. Subepithelial Hyalinisation Predicts Recurrence of Unicystic Ameloblastomas. Diagnostics. 2022; 12(3):756. https://doi.org/10.3390/diagnostics12030756
Chicago/Turabian StyleAugustine, Dominic, Roopa S. Rao, Lakshminarayana Surendra, Bharti Gupta, Thuckanaickenpalayam Ragunathan Yoithapprabhunath, Pradeep Kumar Yadalam, Shazia Mushtaq, Zeeshan Hera Ahmed, and Shankargouda Patil. 2022. "Subepithelial Hyalinisation Predicts Recurrence of Unicystic Ameloblastomas" Diagnostics 12, no. 3: 756. https://doi.org/10.3390/diagnostics12030756