
Photoplethysmographic Measurement of Arterial Stiffness in Polish Patients with Long-COVID-19 Syndrome—The Results of a Cross-Sectional Study
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Group
2.2. Arterial Stiffness Measurement
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Study Group
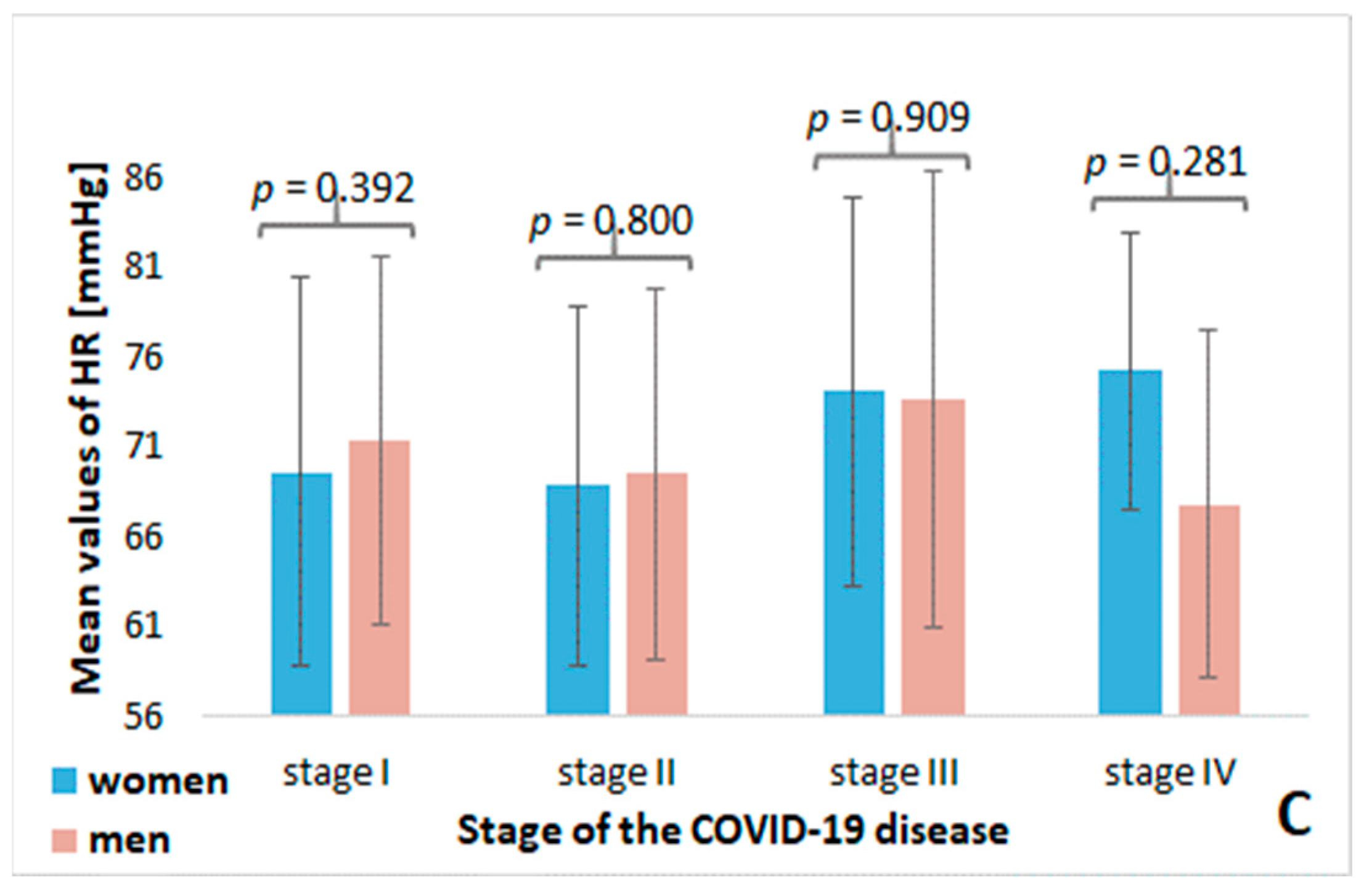
3.2. Analysis of Stiffness Parameters Depending on the Severity of COVID-19 Disease
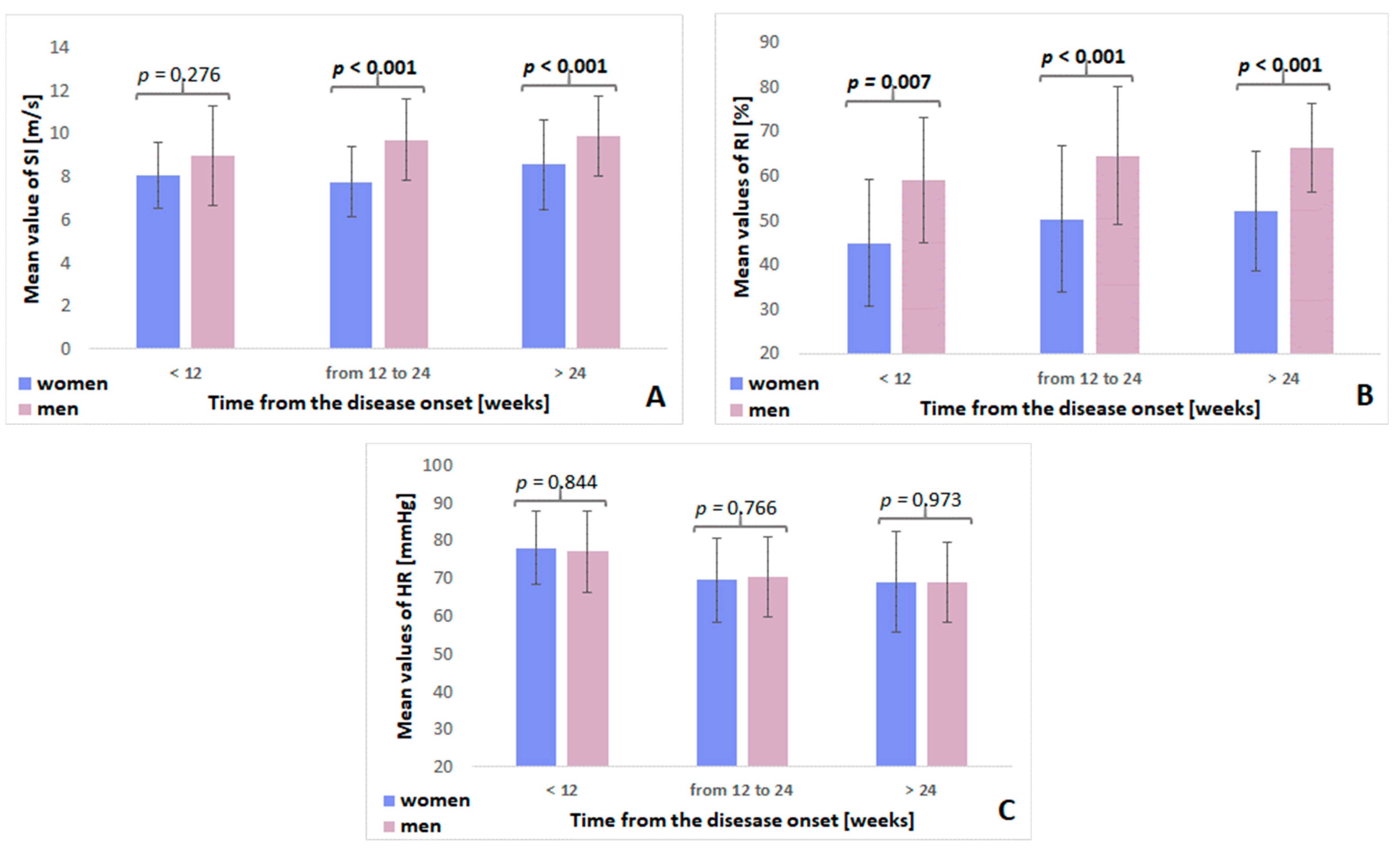
3.3. Analysis of Stiffness Parameters Depending on the Time from the Disease Onset
3.4. Multiple Linear Regression Analysis of the Influence of Selected Risk Factors for Arterial Stiffness
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 29 October 2022).
- World Health Organization. Weekly Epidemiological Update on COVID-19 as of 9 November 2022. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-COVID-19---9-november-2022 (accessed on 21 November 2022).
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef] [PubMed]
- Rass, V.; Ianosi, B.A.; Zamarian, L.; Beer, R.; Sahanic, S.; Lindner, A.; Kofler, M.; Schiefecker, A.J.; Mahlknecht, P.; Heim, B.; et al. Factors associated with impaired quality of life three months after being diagnosed with COVID-19. Qual. Life Res. 2022, 31, 1401–1414. [Google Scholar] [CrossRef] [PubMed]
- Bellan, M.; Soddu, D.; Balbo, P.E.; Baricich, A.; Zeppegno, P.; Avanzi, G.C.; Baldon, G.; Bartolomei, G.; Battaglia, M.; Battistini, S.; et al. Respiratory and Psychophysical Sequelae Among Patients With COVID-19 Four Months After Hospital Discharge. JAMA Netw. Open 2021, 4, e2036142. [Google Scholar] [CrossRef] [PubMed]
- Matsushita, K.; Ding, N.; Kou, M.; Hu, X.; Chen, M.; Gao, Y.; Honda, Y.; Zhao, D.; Dowdy, D.; Mok, Y.; et al. The Relationship of COVID-19 Severity with Cardiovascular Disease and Its Traditional Risk Factors: A Systematic Review and Meta-Analysis. Glob. Heart 2020, 15, 64. [Google Scholar] [CrossRef] [PubMed]
- Pająk, A.; Jankowski, P.; Zdrojewski, T. The burden of cardiovascular disease risk factors: A current problem. Kardiol. Pol. 2022, 80, 5–15. [Google Scholar] [CrossRef]
- Harrison, S.L.; Buckley, B.J.R.; Rivera-Caravaca, J.M.; Zhang, J.; Lip, G.Y.H. Cardiovascular risk factors, cardiovascular disease, and COVID-19: An umbrella review of systematic reviews. Eur. Heart J. Qual. Care Clin. Outcomes 2021, 7, 330–339. [Google Scholar] [CrossRef]
- Rezel-Potts, E.; Douiri, A.; Sun, X.; Chowienczyk, P.J.; Shah, A.M.; Gulliford, M.C. Cardiometabolic outcomes up to 12 months after COVID-19 infection. A matched cohort study in the UK. PLoS Med. 2022, 19, e1004052. [Google Scholar] [CrossRef]
- Xie, Y.; Xu, E.; Bowe, B.; Al-Aly, Z. Long-term cardiovascular outcomes of COVID-19. Nat. Med. 2022, 28, 583–590. [Google Scholar] [CrossRef]
- Goshua, G.; Pine, A.B.; Meizlish, M.L.; Chang, C.-H.; Zhang, H.; Bahel, P.; Baluha, A.; Bar, N.; Bona, R.D.; Burns, A.J.; et al. Endotheliopathy in COVID-19-Associated Coagulopathy: Evidence from a Single-Centre, Cross-Sectional Study. Lancet Haematol. 2020, 7, e575–e582. [Google Scholar] [CrossRef]
- Badaras, I.; Laučytė-Cibulskienė, A. Vascular Aging and COVID-19. Angiology 2022, 33197221121007. [Google Scholar] [CrossRef]
- Guzik, T.J.; Mohiddin, S.A.; Dimarco, A.; Patel, V.; Savvatis, K.; Marelli-Berg, F.M.; Madhur, M.S.; Tomaszewski, M.; Maffia, P.; D’acquisto, F.; et al. COVID-19 and the Cardiovascular System: Implications for Risk Assessment, Diagnosis, and Treatment Options. Cardiovasc. Res. 2020, 116, 1666–1687. [Google Scholar] [CrossRef]
- Saeed, S.; Mancia, G. Arterial stiffness and COVID-19: A bidirectional cause-effect relationship. J. Clin. Hypertens. 2021, 23, 1099–1103. [Google Scholar] [CrossRef]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Abassi, Z.; Higazi, A.A.R.; Kinaneh, S.; Armaly, Z.; Skorecki, K.; Heyman, S.N. ACE2, COVID-19 Infection, Inflammation, and Coagulopathy: Missing Pieces in the Puzzle. Front. Physiol. 2020, 11, 574753. [Google Scholar] [CrossRef]
- Zanoli, L.; Briet, M.; Empana, J.P.; Cunha, P.G.; Mäki-Petäjä, K.M.; Protogerou, A.D.; Tedgui, A.; Touyz, R.M.; Schiffrin, E.L.; Spronck, B.; et al. Association for research into arterial structure, physiology (ARTERY) society, the european society of hypertension (ESH) working group on vascular structure and function, and the european network for non-invasive investigation of large arteries. vascular consequences of inflammation: A position statement from the ESH working group on vascular structure and function and the ARTERY society. J. Hypertens. 2020, 38, 1682–1698. [Google Scholar]
- Zanoli, L.; Boutouyrie, P.; Fatuzzo, P.; Granata, A.; Lentini, P.; Oztürk, K.; Cappello, M.; Theocharidou, E.; Tuttolomondo, A.; Pinto, A.; et al. Inflammation and aortic stiffness: An individual participant data meta-analysis in patients with inflammatory bowel disease. J. Am. Heart Assoc. 2017, 6, e007003. [Google Scholar] [CrossRef] [Green Version]
- Zota, I.M.; Stătescu, C.; Sascău, R.A.; Roca, M.; Anghel, L.; Mitu, O.; Ghiciuc, C.M.; Boisteanu, D.; Anghel, R.; Cozma, S.R.; et al. Arterial Stiffness Assessment Using the Arteriograph in Patients with Moderate–Severe OSA and Metabolic Syndrome—A Pilot Study. J. Clin. Med. 2021, 10, 4238. [Google Scholar] [CrossRef]
- Rodilla, E.; López-Carmona, M.D.; Cortes, X.; Cobos-Palacios, L.; Canales, S.; Sáez, M.C.; Campos Escudero, S.; Rubio-Rivas, M.; Díez Manglano, J.; Freire Castro, S.J.; et al. Impact of Arterial Stiffness on All-Cause Mortality in Patients Hospitalized with COVID-19 in Spain. Hypertension 2021, 77, 856–867. [Google Scholar] [CrossRef]
- Clarenbach, C.F.; Stoewhas, A.C.; van Gestel, A.J.R.; Latshang, T.D.; Lo Cascio, C.M.; Bloch, K.E.; Kohler, M. Comparison of Photoplethysmographic and Arterial Tonometry-Derived Indices of Arterial Stiffness. Hypertens. Res. 2012, 35, 228–233. [Google Scholar] [CrossRef] [Green Version]
- Brillante, D.G.; O’sullivan, A.J.; Howes, L.G. Arterial Stiffness Indices in Healthy Volunteers Using Non-Invasive Digital Photoplethysmography. Blood Press. 2009, 17, 116–123. [Google Scholar] [CrossRef] [Green Version]
- Schnaubelt, S.; Oppenauer, J.; Tihanyi, D.; Mueller, M.; Maldonado-Gonzalez, E.; Zejnilovic, S.; Haslacher, H.; Perkmann, T.; Strassl, R.; Anders, S.; et al. Arterial stiffness in acute COVID-19 and potential associations with clinical outcome. J. Intern. Med. 2021, 290, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Ratchford, S.M.; Stickford, J.L.; Province, V.M.; Stute, N.; Augenreich, M.A.; Koontz, L.K.; Bobo, L.K.; Stickford, A.S.L. Vascular alterations among young adults with SARS-CoV-2. Am. J. Physiol. Heart Circ. Physiol. 2021, 320, H404–H410. [Google Scholar] [CrossRef] [PubMed]
- Ring, M.; Eriksson, M.J.; Fritz, T.; Nyberg, G.; Östenson, C.G.; Krook, A.; Zierath, J.R.; Caidahl, K. Influence of Physical Activity and Gender on Arterial Function in Type 2 Diabetes, Normal and Impaired Glucose Tolerance. Diabetes Vasc. Dis. Res. 2015, 12, 315–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noon, J.P.; Trischuk, T.C.; Gaucher, S.A.; Galante, S.; Scott, R.L. The Effect of Age and Gender on Arterial Stiffness in Healthy Caucasian Canadians. J. Clin. Nurs. 2008, 17, 2311–2317. [Google Scholar] [CrossRef] [PubMed]
- Flisiak, R.; Horban, A.; Jaroszewicz, J.; Kozielewicz, D.; Mastalerz-Migas, A.; Owczuk, R.; Parczewski, M.; Pawłowska, M.; Piekarska, A.; Simon, K.; et al. Management of SARS-CoV-2 infection: Recommendations of the Polish Association of Epidemiologists and Infectiologists as of April 26, 2021. Pol. Arch. Intern. Med. 2021, 131, 487–496. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19. 2020. Available online: https://www.nice.org.uk/guidance/ng188 (accessed on 21 November 2022).
- O′Rourke, M.F.; Staessen, J.A.; Vlachopoulos, C.; Duprez, D.; Plante, G.E. Clinical Applications of Arterial Stiffness; Definitions and Reference Values. Am. J. Hypertens. 2002, 15, 426–444. [Google Scholar] [CrossRef]
- Stamatelopoulos, K.S.; Armeni, E.; Georgiopoulos, G.; Kazani, M.; Kyrkou, K.; Stellos, K.; Koliviras, A.; Alexandrou, A.; Creatsa, M.; Papamichael, C.; et al. Recently Postmenopausal Women Have the Same Prevalence of Subclinical Carotid Atherosclerosis as Age and Traditional Risk Factor Matched Men. Atherosclerosis 2012, 221, 508–513. [Google Scholar] [CrossRef]
- DuPont, J.J.; Kenney, R.M.; Patel, A.R.; Jaffe, I.Z. Sex Differences in Mechanisms of Arterial Stiffness. Br. J. Pharmacol. 2019, 176, 4208–4225. [Google Scholar] [CrossRef]
- Coutinho, T.; Borlaug, B.A.; Pellikka, P.A.; Turner, S.T.; Kullo, I.J. Sex Differences in Arterial Stiffness and Ventricular-Arterial Interactions. J. Am. Coll. Cardiol. 2013, 61, 96–103. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.-Y.; Oh, B.-H. Aging and Arterial Stiffness. Circ. J. 2010, 74, 2257–2262. [Google Scholar] [CrossRef] [Green Version]
- Grassi, G. Impact of Heart Rate on Arterial Stiffness: Virtual vs. Real Assessment. J. Hypertens. 2020, 38, 2382–2383. [Google Scholar] [CrossRef]
- Whelton, S.P.; Blankstein, R.; Al-Mallah, M.H.; Lima, J.A.C.; Bluemke, D.A.; Hundley, W.G.; Polak, J.F.; Blumenthal, R.S.; Nasir, K.; Blaha, M.J. Association of Resting Heart Rate with Carotid and Aortic Arterial Stiffness: Multi-Ethnic Study of Atherosclerosis. Hypertension 2013, 62, 477–484. [Google Scholar] [CrossRef] [Green Version]
- Scallan, C.; Doonan, R.J.; Daskalopoulou, S.S. The combined effect of hypertension and smoking on arterial stiffness. Clin. Exp. Hypertens. 2010, 32, 319–328. [Google Scholar] [CrossRef]
- Madhura, M.; Sandhya, T.A. Effect of Different Phases of Menstrual Cycle on Reflection Index, Stiffness index and Pulse wave velocity in Healthy subjects. J. Clin. Diagn. Res. 2014, 8, BC01–BC04. [Google Scholar]
- Zota, I.M.; Stătescu, C.; Sascău, R.A.; Roca, M.; Anghel, L.; Maștaleru, A.; Leon-Constantin, M.M.; Ghiciuc, C.M.; Cozma, S.R.; Dima-Cozma, L.C.; et al. Acute and Long-Term Consequences of COVID-19 on Arterial Stiffness-A Narrative Review. Life 2022, 12, 781. [Google Scholar] [CrossRef]
- Chang, R.; Mamun, A.; Dominic, A.; Le, N.-T. SARS-CoV-2 Mediated Endothelial Dysfunction: The Potential Role of Chronic Oxidative Stress. Front. Physiol. 2021, 11, 605908. [Google Scholar] [CrossRef]
- Lambadiari, V.; Mitrakou, A.; Kountouri, A.; Thymis, J.; Katogiannis, K.; Korakas, E.; Varlamos, C.; Andreadou, I.; Tsoumani, M.; Triantafyllidi, H.; et al. Association of COVID-19 with Impaired Endothelial Glycocalyx, Vascular Function and Myocardial Deformation 4 Months after Infection. Eur. J. Heart Fail. 2021, 23, 1916–1926. [Google Scholar] [CrossRef]
- Stamatelopoulos, K.; Georgiopoulos, G.; Baker, K.F.; Tiseo, G.; Delialis, D.; Lazaridis, C.; Barbieri, G.; Masi, S.; Vlachogiannis, N.I.; Sopova, K.; et al. Estimated Pulse Wave Velocity Improves Risk Stratification for All-Cause Mortality in Patients with COVID-19. Sci. Rep. 2021, 11, 20239. [Google Scholar] [CrossRef]
- Kumar, N.; Kumar, S.; Kumar, A.; Bhushan, D.; Kumar, A.; Kumar, A.; Singh, V.; Singh, P.K. The COSEVAST Study Outcome: Evidence of COVID-19 Severity Proportionate to Surge in Arterial Stiffness. Indian J. Crit. Care Med. 2021, 25, 1113–1119. [Google Scholar] [CrossRef]
- Ikonomidis, I.; Lambadiari, V.; Mitrakou, A.; Kountouri, A.; Katogiannis, K.; Thymis, J.; Korakas, E.; Pavlidis, G.; Kazakou, P.; Panagopoulos, G.; et al. Myocardial Work and Vascular Dysfunction Are Partially Improved at 12 Months after COVID-19 Infection. Eur. J. Heart Fail. 2022, 24, 727–729. [Google Scholar] [CrossRef]
- Raisi-Estabragh, Z.; McCracken, C.; Cooper, J.; Fung, K.; Paiva, J.M.; Khanji, M.Y.; Rauseo, E.; Biasiolli, L.; Raman, B.; Piechnik, S.K.; et al. Adverse cardiovascular magnetic resonance phenotypes are associated with greater likelihood of incident coronavirus disease 2019: Findings from the UK Biobank. Aging Clin. Exp. Res. 2021, 33, 1133–1144. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total Group n = 225 | Men n = 102 (45.33%) | Women n = 123 (54.67%) | p | |
|---|---|---|---|---|
| Age (years), M ± SD | 58.98 ± 8.57 | 59.18 ± 8.56 | 58.81 ± 8.61 | 0.475 |
| BMI (kg/m2), M ± SD | 29.35 ± 4.82 | 29.41 ± 5.09 | 29.30 ± 5.38 | 0.752 |
| Smoking status, n (%) | <0.001 | |||
| Non-smokers | 126 (56.00) | 42 (41.18) | 84 (68.29) | |
| Smokers | 17 (7.56) | 14 (13.72) | 3 (2.44) | |
| Former smokers | 81 (36.00) | 46 (45.10) | 35 (28.45) | |
| Hypertension, n (%) | 139 (61.78) | 73 (71.57) | 66 (53.66) | 0.006 |
| Diabetes, n (%) | 50 (22.73) | 27 (12.27) | 23 (10.45) | 0.163 |
| Hyperuricemia, n (%) | 15 (7.54) | 5 (2.51) | 10 (5.03) | 0.382 |
| Dyslipidemia, n (%) | 116 (52.73) | 58 (26.36) | 58 (26.36) | 0.140 |
| SI (m/s), M ± SD | 8.80 ± 1.95 | 9.54 ± 2.07 | 8.19 ± 1.62 | <0.001 |
| RI (%), M ± SD | 56.85 ± 16.28 | 64.29 ± 14.25 | 50.68 ± 15.29 | <0.001 |
| HR (beats/min.), M ± SD | 70.35 ± 10.67 | 70.87 ± 10.77 | 69.91 ± 10.62 | 0.286 |
| SP (mmHg), M ± SD | 139.93 ± 17.42 | 141.66 ± 16.96 | 136.67 ± 17.63 | 0.031 |
| DP (mmHg), M ± SD | 83.10 ± 11.02 | 86.48 ± 11.25 | 80.30 ± 10.03 | <0.001 |
| Stage I n = 112 | Stage II n = 58 | Stage III n = 35 | Stage IV n = 15 | p | |
|---|---|---|---|---|---|
| Age (years), M ± SD | 58.82 ± 7.93 | 57.64 ± 8.29 | 61.14 ± 10.49 | 59.13 ± 8.93 | 0.299 |
| Sex (M/F), n (%) | 52 (46.4) | 24 (41.4) | 17 (48.6) | 7 (46.7) | 0.902 |
| BMI (kg/m2), M ± SD | 29.60 ± 4.76 | 29.18 ± 5.41 | 29.95 ± 4.42 | 26.87 ± 3,61 | 0.187 |
| Smoking status, n (%) | 0.736 | ||||
| Non-smokers | 59 (53.2) | 35 (60.3) | 22 (62.9) | 8 (53.3) | |
| Smokers | 8 (7.2) | 6 (10.3) | 1 (2.9) | 1 (6.7) | |
| Former smokers | 44 (39.6) | 17 (29.3) | 12 (34.3) | 6 (40.0) | |
| Hypertension, n (%) | 69 (61.6) | 32 (55.2) | 23 (65.7) | 13 (86.7) | 0.155 |
| Diabetes, n (%) | 24 (24.1) | 12 (20.7) | 9 (25.7) | 2 (13.3) | 0.755 |
| Hyperuricemia, n (%) | 9 (9.7) | 5 (8.9) | 1 (2.9) | 0 (0.0) | 0.378 |
| Dyslipidemia, n (%) | 67 (59.8) | 30 (51.7) | 12 (34.3) | 6 (40.0) | 0.045 |
| SI (m/s), M ± SD | 8.77 ± 2.01 | 8.88 ± 2.07 | 8.84 ± 1.77 | 9.08 ± 1.36 | 0.940 |
| RI (%), M ± SD | 56.48 ± 16.98 | 56.59 ± 15.64 | 56.77 ± 16.18 | 56.62 ± 15.40 | 0.999 |
| HR (beats/min.), M ± SD | 70.23 ± 10.64 | 69.12 ± 10.09 | 73.78 ± 11.87 | 71.21 ± 9.35 | 0.221 |
| SP (mmHg), M ± SD | 137.33 ± 17.00 | 139.55 ± 18.58 | 139.91 ± 14.25 | 145.13 ± 20.82 | 0.384 |
| DP (mmHg), M ± SD | 82,52 ± 10.60 | 83.50 ± 11.06 | 82.29 ± 11.11 | 86.20 ± 14.50 | 0.633 |
| <12 Weeks n = 24 | 12–24 Weeks n = 83 | >24 Weeks n = 95 | p | |
|---|---|---|---|---|
| Age (years), M ± SD | 60.79 ± 11.36 | 58.86 ± 8.31 | 57.73 ± 7.61 | 0.258 |
| Sex (M/F), n (%) | 12 (50.0) | 42 (50.6) | 38 (40.0) | 0.329 |
| BMI (kg/m2), M ± SD | 28.06 ± 4.77 | 29.46 ± 4.48 | 29.39 ± 4.97 | 0.418 |
| Smoking status, n (%) | 0.651 | |||
| Non-smokers | 15 (62.5) | 41 (50.0) | 57 (60.0) | |
| Smokers | 8 (33.3) | 34 (41.5) | 31 (32.6) | |
| Former smokers | 1 (4.2) | 7 (8.5) | 7 (7.4) | |
| Hypertension, n (%) | 13 (54.2) | 54 (65.1) | 56 (58.9) | 0.546 |
| Diabetes, n (%) | 4 (16.7) | 23 (27.7) | 20 (21.1) | 0.414 |
| Hyperuricemia, n (%) | 2 (8.3) | 7 (11.1) | 5 (5.3) | 0.409 |
| Dyslipidemia, n (%) | 5 (20.8) | 55 (66.3) | 47 (49.5) | <0.001 |
| SI (m/s), M ± SD | 8.52 ± 1.98 | 8.83 ± 2.02 | 9.05 ± 1.95 | 0.321 |
| RI (%), M ± SD | 52.48 ± 13.49 | 58.07 ± 17.30 | 57.35 ± 15.67 | 0.472 |
| HR (beats/min.), M ± SD | 77.52 ± 11.73 | 69.94 ± 10.77 | 68.97 ± 10.05 | 0.002 |
| SP (mmHg), M ± SD | 138.71 ± 19.75 | 137.30 ± 16.61 | 140,35 ± 17.81 | 0.514 |
| DP (mmHg), M ± SD | 88.04 ± 12.32 | 81.64 ± 11.50 | 83.52 ± 10.31 | 0.045 |
| Predictors | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| Coefficient | Std. Error | p | Coefficient | Std. Error | p | |
| SI | SI (R2 = 0.155; p < 0.001) | |||||
| Age (years) | 0.050 | 0.015 | 0.003 | 0.043 | 0.014 | 0.002 |
| Sex women vs. men | −0.675 | 0.123 | <0.001 | −0.667 | 0.121 | <0.001 |
| BMI (kg/m2) | −0.026 | 0.027 | 0.335 | NS | ||
| Time from disease onset | NS | |||||
| <12 weeks vs. >24 weeks | −0.276 | 0.288 | 0.338 | |||
| 12–24 weeks vs. >24 weeks | 0.027 | 0.210 | 0.897 | |||
| COVID−19 severity | NS | |||||
| Stage I vs. stage IV | −0.124 | 0.215 | 0.565 | |||
| Stage II vs. stage IV | −0.008 | 0.249 | 0.973 | |||
| Stage III vs. stage IV | −0.056 | 0.289 | 0.847 | |||
| Diabetes no vs. yes | −0.094 | 0.157 | 0.547 | NS | ||
| Hypertension no vs. yes | −0.241 | 0.133 | 0.072 | NS | ||
| Smoking status | NS | |||||
| Nonsmoker vs. smoker | −0.477 | 0.207 | 0.022 | |||
| Former smoker vs. smoker | 0.062 | 0.219 | 0.778 | |||
| RI | RI (R2 = 0.218; p < 0.001) | |||||
| Age (years) | 0.060 | 0.127 | 0.638 | NS | ||
| Sex women vs. men | −6.807 | 0.993 | <0.001 | −7.285 | 1.038 | <0.001 |
| BMI (kg/m2) | −0.086 | 0.226 | 0.703 | NS | ||
| Time from disease onset | ||||||
| <12 weeks vs. >24 weeks | −3.485 | 2.340 | 0.138 | −4.670 | 2.103 | 0.027 |
| 12–24 weeks vs. > 24 weeks | 2.101 | 1.704 | 0.219 | NS | NS | NS |
| COVID−19 severity | NS | |||||
| Stage I vs. stage IV | −0.134 | 1.802 | 0.940 | |||
| Stage II vs. stage IV | −0.020 | 2.090 | 0.992 | |||
| Stage III vs. stage IV | −0.150 | 2.427 | 0.951 | |||
| Diabetes no vs. yes | 2.012 | 1.301 | 0.123 | 2.722 | 1.228 | 0.028 |
| Hypertension no vs. yes | −1.048 | 1.117 | 0.349 | NS | ||
| Smoking status | NS | |||||
| Nonsmoker vs. smoker | −5.494 | 1.702 | 0.001 | |||
| Former smoker vs. smoker | −0.528 | 1.808 | 0.771 | |||
| HR | HR (R2 = 0.086; p < 0.001) | |||||
| Age (years) | −0.016 | 0.083 | 0.846 | NS | ||
| Sex women vs. men | 0.477 | 0.716 | 0.505 | NS | ||
| BMI (kg/m2) | −0.072 | 0.148 | 0.627 | NS | ||
| Time from disease onset | s | |||||
| <12 weeks vs. >24 weeks | 5.380 | 1.530 | <0.001 | 5.686 | 1.519 | <0.001 |
| 12–24 weeks vs. >24 weeks | −2.206 | 1.115 | 0.049 | −2.378 | 1.105 | 0.033 |
| COVID−19 severity | NS | |||||
| Stage I vs. stage IV | −0.856 | 1.167 | 0.464 | |||
| Stage II vs. stage IV | −1.965 | 1.353 | 0.148 | |||
| Stage III vs. stage IV | 2.693 | 1.572 | 0.088 | |||
| Diabetes no vs. yes | −1.727 | 0.850 | 0.043 | −2.064 | 0.886 | 0.021 |
| Hypertension no vs. yes | −0.782 | 0.732 | 0.286 | NS | ||
| Smoking status | NS | |||||
| Nonsmoker vs. smoker | −1.150 | 1.146 | 0.317 | |||
| Former smoker vs. smoker | 0.084 | 1.218 | 0.945 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szoltysek-Boldys, I.; Zielinska-Danch, W.; Loboda, D.; Wilczek, J.; Gibinski, M.; Paradowska-Nowakowska, E.; Golba, K.S.; Sarecka-Hujar, B. Photoplethysmographic Measurement of Arterial Stiffness in Polish Patients with Long-COVID-19 Syndrome—The Results of a Cross-Sectional Study. Diagnostics 2022, 12, 3189. https://doi.org/10.3390/diagnostics12123189
Szoltysek-Boldys I, Zielinska-Danch W, Loboda D, Wilczek J, Gibinski M, Paradowska-Nowakowska E, Golba KS, Sarecka-Hujar B. Photoplethysmographic Measurement of Arterial Stiffness in Polish Patients with Long-COVID-19 Syndrome—The Results of a Cross-Sectional Study. Diagnostics. 2022; 12(12):3189. https://doi.org/10.3390/diagnostics12123189
Chicago/Turabian StyleSzoltysek-Boldys, Izabela, Wioleta Zielinska-Danch, Danuta Loboda, Jacek Wilczek, Michal Gibinski, Elzbieta Paradowska-Nowakowska, Krzysztof S. Golba, and Beata Sarecka-Hujar. 2022. "Photoplethysmographic Measurement of Arterial Stiffness in Polish Patients with Long-COVID-19 Syndrome—The Results of a Cross-Sectional Study" Diagnostics 12, no. 12: 3189. https://doi.org/10.3390/diagnostics12123189