
Identifying Patients at Risk of Acute Kidney Injury among Patients Receiving Immune Checkpoint Inhibitors: A Machine Learning Approach

Abstract
:1. Introduction
2. Materials and Methods
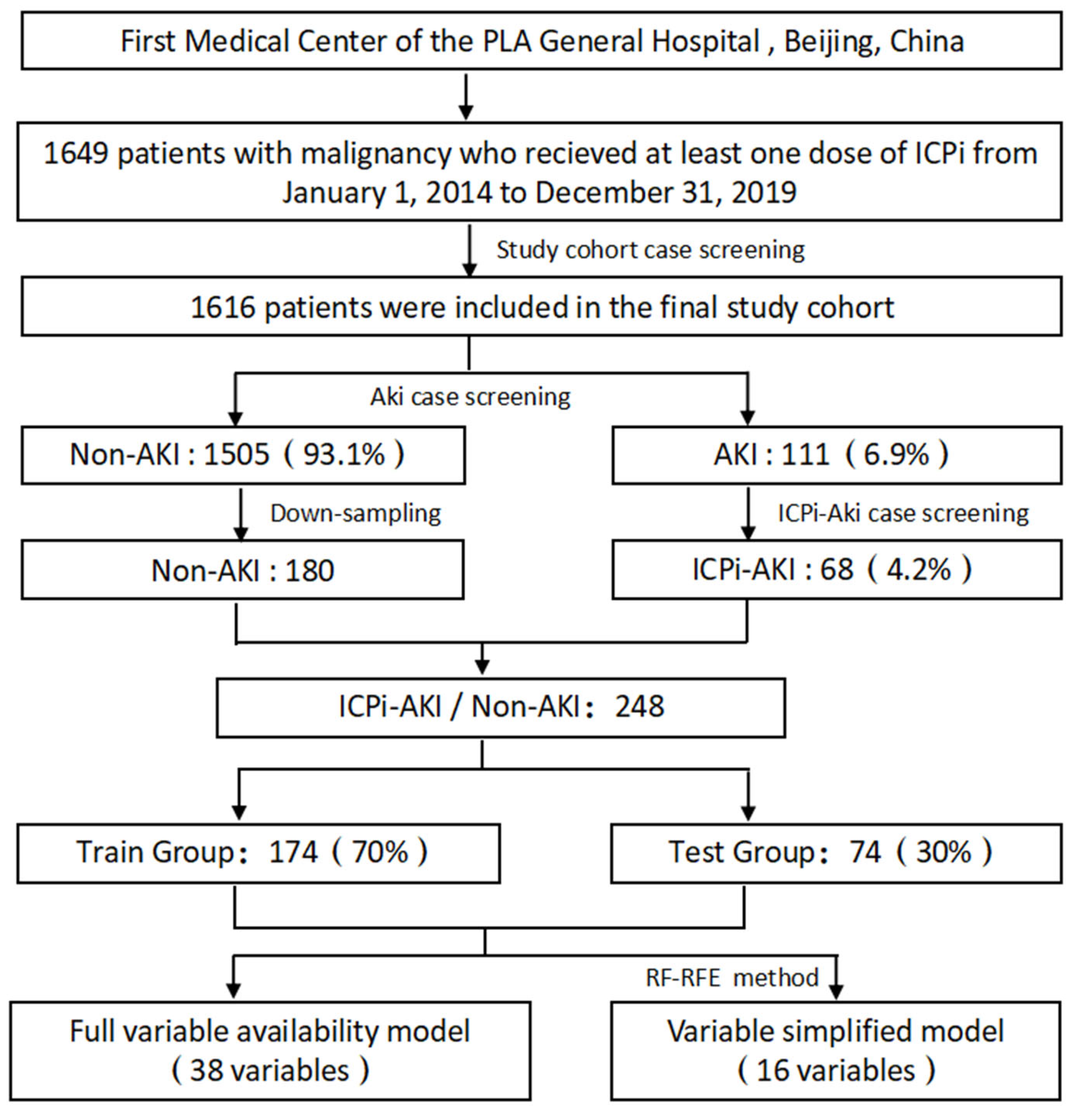
2.1. Data Sources and Study Population
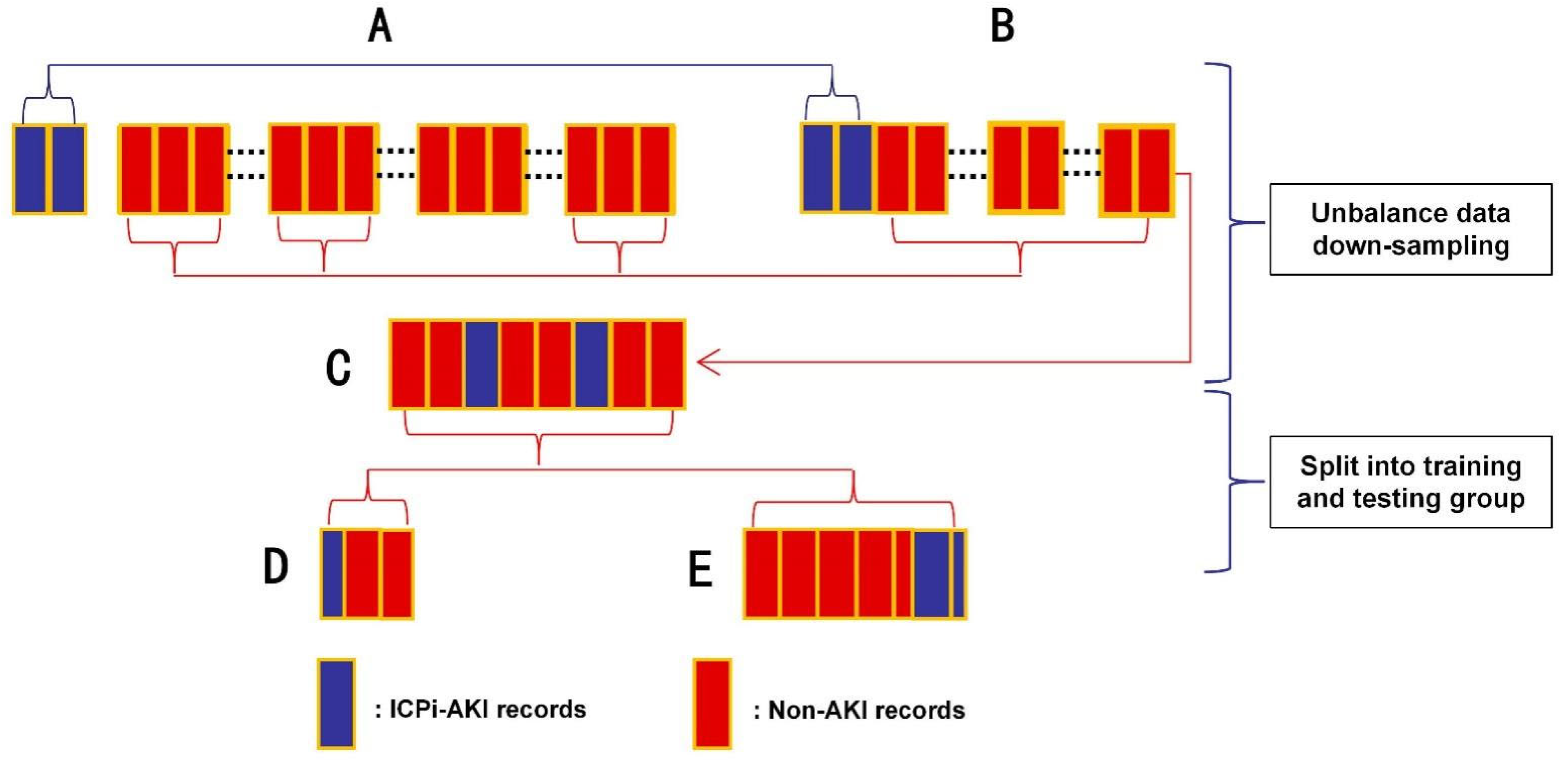
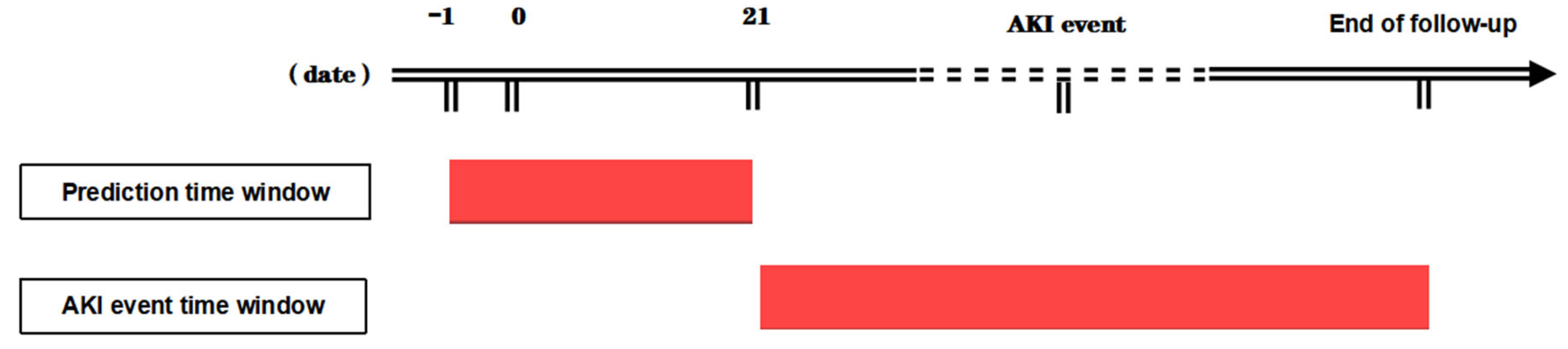
2.2. Study Design
2.3. Model Evaluation
2.4. Statistical Analysis
3. Results
3.1. Comparison of Clinical Characteristics between Groups
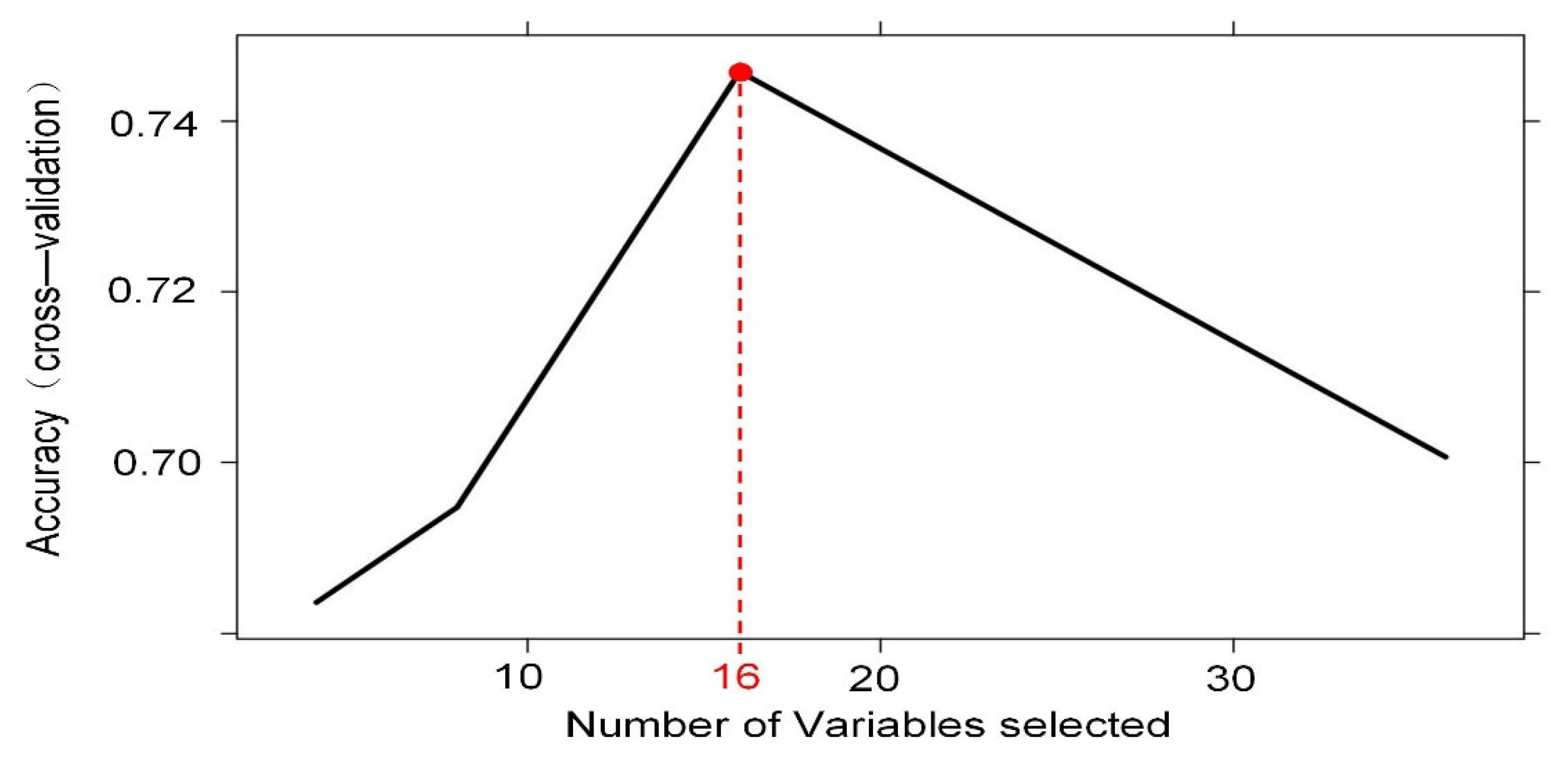
3.2. Significant Variable Screening
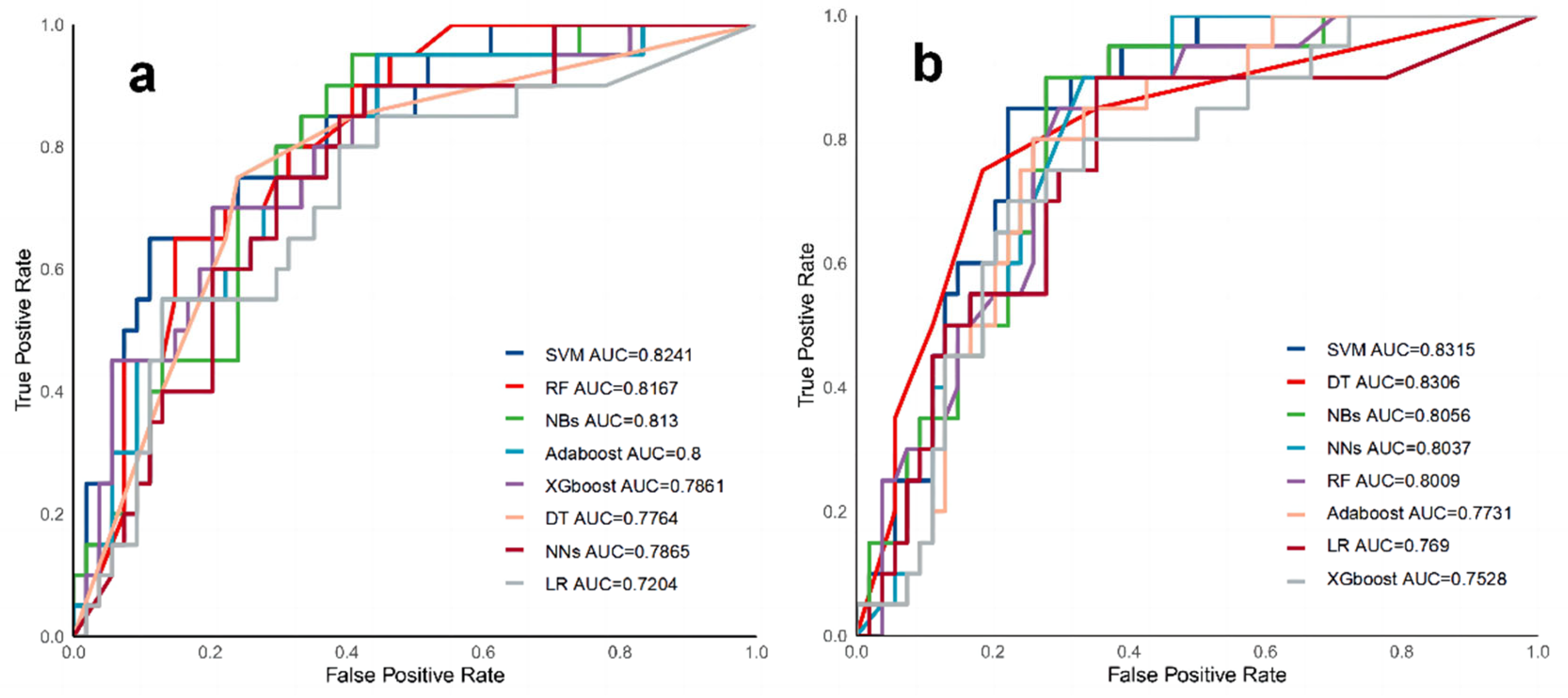
3.3. Model Performance Evaluation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gupta, S.; Short, S.A.P.; Sise, M.E.; Prosek, J.M.; Madhavan, S.M.; Soler, M.J.; Ostermann, M.; Herrmann, S.M.; Abudayyeh, A.; Anand, S.; et al. Acute kidney injury in patients treated with immune checkpoint inhibitors. J. Immunother. Cancer 2021, 9, e003467. [Google Scholar] [CrossRef] [PubMed]
- Hussaini, S.; Chehade, R.; Boldt, R.G.; Raphael, J.; Blanchette, P.; Vareki, S.M.; Fernandes, R. Association between immune-related side effects and efficacy and benefit of immune checkpoint inhibitors—A systematic review and meta-analysis. Cancer Treat. Rev. 2021, 92, 102134. [Google Scholar] [CrossRef] [PubMed]
- Seethapathy, H.; Zhao, S.; Chute, D.F.; Zubiri, L.; Oppong, Y.; Strohbehn, I.; Cortazar, F.B.; Leaf, D.E.; Mooradian, M.J.; Villani, A.-C.; et al. The incidence, causes, and risk factors of acute kidney injury in patients receiving immune checkpoint inhibitors. Clin. J. Am. Soc. Nephrol. 2019, 14, 1692–1700. [Google Scholar] [CrossRef] [PubMed]
- Cortazar, F.B.; Kibbelaar, Z.A.; Glezerman, I.G.; Abudayyeh, A.; Mamlouk, O.; Motwani, S.S.; Murakami, N.; Herrmann, S.M.; Manohar, S.; Shirali, A.C.; et al. Clinical features and outcomes of immune checkpoint inhibitor–associated AKI: A multicenter study. J. Am. Soc. Nephrol. 2020, 31, 435–446. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, S.M.; Perazella, M.A. Immune checkpoint inhibitors and immune-related adverse renal events. Kidney Int. Rep. 2020, 5, 1139–1148. [Google Scholar] [CrossRef]
- Shirali, A.C.; Perazella, M.A.; Gettinger, S. Association of acute interstitial nephritis with programmed cell death 1 inhibitor therapy in lung cancer patients. Am. J. Kidney Dis. 2016, 68, 287–291. [Google Scholar] [CrossRef]
- Gameiro, J.; Branco, T.; Lopes, J.A. Artificial intelligence in acute kidney injury risk prediction. J. Clin. Med. 2020, 9, 678. [Google Scholar] [CrossRef] [Green Version]
- Ebiaredoh-Mienye, S.A.; Swart, T.G.; Esenogho, E.; Mienye, I.D. A Machine Learning Method with Filter-Based Feature Selection for Improved Prediction of Chronic Kidney Disease. Bioengineering 2022, 9, 350. [Google Scholar] [CrossRef]
- Ebiaredoh-Mienye, S.A.; Esenogho, E.; Swart, T.G. Integrating Enhanced Sparse Autoencoder Based Artificial Neural Network Technique and Softmax Regression for Medical Diagnosis. Electronics 2020, 9, 1963. [Google Scholar] [CrossRef]
- Koyner, J.L.; Carey, K.A.; Edelson, D.P.; Churpek, M.M. The Development of a Machine Learning Inpatient Acute Kidney Injury Prediction Model. Crit. Care Med. 2018, 46, 1070–1077. [Google Scholar] [CrossRef]
- Zhang, Z.; Ho, K.M.; Hong, Y. Machine learning for the prediction of volume responsiveness in patients with oliguric acute kidney injury in critical care. Crit. Care 2019, 23, 112. [Google Scholar] [CrossRef] [Green Version]
- Tomašev, N.; Glorot, X.; Rae, J.W.; Zielinski, M.; Askham, H.; Saraiva, A.; Mottram, A.; Meyer, C.; Ravuri, S.; Protsyuk, I.; et al. A clinically applicable approach to continuous prediction of future acute kidney injury. Nature 2019, 572, 116–119. [Google Scholar] [CrossRef]
- Kellum, J.A.; Lameire, N. Diagnosis, evaluation, and management of acute kidney injury: A KDIGO summary (Part 1). Crit. Care 2013, 17, 204. [Google Scholar] [CrossRef] [Green Version]
- Gupta, S.; Cortazar, F.B.; Riella, L.V.; Leaf, D.E. Immune checkpoint inhibitor nephrotoxicity: Update 2020. Kidney360 2020, 1, 130–140. [Google Scholar] [CrossRef] [Green Version]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Koks, M.S.; Ocak, G.; Suelmann, B.B.M.; Hulsbergen-Veelken, C.A.R.; Haitjema, S.; Vianen, M.E.; Verhaar, M.C.; Kaasjager, K.A.H.; Khairoun, M. Immune checkpoint inhibitor-associated acute kidney injury and mortality: An observational study. PLoS ONE 2021, 16, e0252978. [Google Scholar] [CrossRef]
- Meraz-Muñoz, A.; Amir, E.; Ng, P.; Avila-Casado, C.; Ragobar, C.; Chan, C.; Kim, J.; Wald, R.; Kitchlu, A. Acute kidney injury associated with immune checkpoint inhibitor therapy: Incidence, risk factors and outcomes. J. ImmunoTher. Cancer 2020, 8, e000467. [Google Scholar] [CrossRef]
- Sun, M.; Baron, J.; Dighe, A.; Szolovits, P.; Wunderink, R.G.; Isakova, T.; Luo, Y. Early prediction of acute kidney injury in critical care setting using clinical notes and structured multivariate physiological measurements. Stud. Health Technol. Inform. 2019, 264, 368–372. [Google Scholar] [CrossRef]
- Qu, C.; Gao, L.; Yu, X.-Q.; Wei, M.; Fang, G.-Q.; He, J.; Cao, L.-X.; Ke, L.; Tong, Z.-H.; Li, W.-Q.; et al. Machine learning models of acute kidney injury prediction in acute pancreatitis patients. Gastroenterol. Res. Pract. 2020, 2020, 3431290. [Google Scholar] [CrossRef]
- Gibson, A.; Faulkner, L.; Lichtenfels, M.; Ogese, M.; Al-Attar, Z.; Alfirevic, A.; Esser, P.R.; Martin, S.F.; Pirmohamed, M.; Park, B.K.; et al. The effect of inhibitory signals on the priming of drug hapten–specific T cells that express distinct Vβ receptors. J. Immunol. 2017, 199, 1223–1237. [Google Scholar] [CrossRef] [Green Version]
- Perazella, M.A.; Shirali, A.C. Immune checkpoint inhibitor nephrotoxicity: What do we know and what should we do? Kidney Int. 2020, 97, 62–74. [Google Scholar] [CrossRef]
- Shimamura, Y.; Watanabe, S.; Maeda, T.; Abe, K.; Ogawa, Y.; Takizawa, H. Incidence and risk factors of acute kidney injury, and its effect on mortality among Japanese patients receiving immune check point inhibitors: A single-center observational study. Clin. Exp. Nephrol. 2021, 25, 479–487. [Google Scholar] [CrossRef] [PubMed]
- Cortellini, A.; Tucci, M.; Adamo, V.; Stucci, L.S.; Russo, A.; Tanda, E.T.; Spagnolo, F.; Rastelli, F.; Bisonni, R.; Santini, D.; et al. Integrated analysis of concomitant medications and oncological outcomes from PD-1/PD-L1 checkpoint inhibitors in clinical practice. J. ImmunoTher. Cancer 2020, 8, e001361. [Google Scholar] [CrossRef] [PubMed]
- Topalian, S.L.; Sznol, M.; McDermott, D.F.; Kluger, H.M.; Carvajal, R.D.; Sharfman, W.H.; Brahmer, J.R.; Lawrence, D.P.; Atkins, M.B.; Powderly, J.D.; et al. Survival, durable tumor remission, and long-term safety in patients with advanced melanoma receiving nivolumab. J. Clin. Oncol. 2014, 32, 1020–1030. [Google Scholar] [CrossRef] [PubMed]
- Brahmer, J.; Reckamp, K.L.; Baas, P.; Crinò, L.; Eberhardt, W.E.E.; Poddubskaya, E.; Antonia, S.; Pluzanski, A.; Vokes, E.E.; Holgado, E.; et al. Nivolumab versus docetaxel in advanced squamous-cell non–small-cell lung cancer. N. Engl. J. Med. 2015, 373, 123–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eigentler, T.K.; Hassel, J.C.; Berking, C.; Aberle, J.; Bachmann, O.; Grünwald, V.; Kähler, K.C.; Loquai, C.; Reinmuth, N.; Steins, M.; et al. Diagnosis, monitoring and management of immune-related adverse drug reactions of anti-PD-1 antibody therapy. Cancer Treat. Rev. 2016, 45, 7–18. [Google Scholar] [CrossRef]
- Gettinger, S.N.; Horn, L.; Gandhi, L.; Spigel, D.R.; Antonia, S.J.; Rizvi, N.A.; Powderly, J.D.; Heist, R.S.; Carvajal, R.D.; Jackman, D.M.; et al. Overall survival and long-term safety of nivolumab (anti–programmed death 1 antibody, BMS-936558, ONO-4538) in patients with previously treated advanced non–small-cell lung cancer. J. Clin. Oncol. 2015, 33, 2004–2012. [Google Scholar] [CrossRef]
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, D.R.; Steins, M.; Ready, N.E.; Chow, L.Q.; Vokes, E.E.; Felip, E.; Holgado, E.; et al. Nivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancer. N. Engl. J. Med. 2015, 373, 1627–1639. [Google Scholar] [CrossRef]
- Malyszko, J.; Tesarova, P.; Capasso, G.; Capasso, A. The link between kidney disease and cancer: Complications and treatment. Lancet 2020, 396, 277–287. [Google Scholar] [CrossRef]
- Rizvi, N.A.; Mazières, J.; Planchard, D.; Stinchcombe, T.E.; Dy, G.K.; Antonia, S.J.; Horn, L.; Lena, H.; Minenza, E.; Mennecier, B.; et al. Activity and safety of nivolumab, an anti-PD-1 immune checkpoint inhibitor, for patients with advanced, refractory squamous non-small-cell lung cancer (CheckMate 063): A phase 2, single-arm trial. Lancet Oncol. 2015, 16, 257–265. [Google Scholar] [CrossRef]
- Dumenil, C.; Massiani, M.-A.; Dumoulin, J.; Giraud, V.; Labrune, S.; Chinet, T.; Leprieur, E.G. Clinical factors associated with early progression and grade 3–4 toxicity in patients with advanced non-small-cell lung cancers treated with nivolumab. PLoS ONE 2018, 13, e0195945. [Google Scholar] [CrossRef] [Green Version]
- Garon, E.B.; Rizvi, N.A.; Hui, R.; Leighl, N.; Balmanoukian, A.S.; Eder, J.P.; Patnaik, A.; Aggarwal, C.; Gubens, M.; Horn, L.; et al. Pembrolizumab for the treatment of non-small-cell lung cancer. N. Engl. J. Med. 2015, 372, 2018–2028. [Google Scholar] [CrossRef]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus chemotherapy for PD-L1–positive non–small-cell lung cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef] [Green Version]
- Zhu, A.X.; Finn, R.S.; Edeline, J.; Cattan, S.; Ogasawara, S.; Palmer, D.; Verslype, C.; Zagonel, V.; Fartoux, L.; Vogel, A.; et al. Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE-224): A non-randomised, open-label phase 2 trial. Lancet Oncol. 2018, 19, 940–952. [Google Scholar] [CrossRef]
- Ren, Z.; Qin, S.; Meng, Z.; Chen, Z.; Chai, X.; Xiong, J.; Bai, Y.; Yang, L.; Zhu, H.; Fang, W.; et al. A phase 2 study of camrelizumab for advanced hepatocellular carcinoma: Two-year outcomes and continued treatment beyond first RECIST-defined progression. Liver Cancer 2021, 10, 500–509. [Google Scholar] [CrossRef]
- Qin, S.; Finn, R.S.; Kudo, M.; Meyer, T.; Vogel, A.; Ducreux, M.; Macarulla, T.M.; Tomasello, G.; Boisserie, F.; Hou, J.; et al. RATIONALE 301 study: Tislelizumab versus sorafenib as first-line treatment for unresectable hepatocellular carcinoma. Future Oncol. 2019, 15, 1811–1822. [Google Scholar] [CrossRef] [Green Version]
- Fuchs, C.S.; Doi, T.; Jang, R.W.; Muro, K.; Satoh, T.; Machado, M.; Sun, W.; Jalal, S.I.; Shah, M.A.; Metges, J.P.; et al. Safety and efficacy of pembrolizumab monotherapy in patients with previously treated advanced gastric and gastroesophageal junction cancer: Phase 2 clinical KEYNOTE-059 trial. JAMA Oncol. 2018, 4, e180013. [Google Scholar] [CrossRef]
- Kang, Y.-K.; Boku, N.; Satoh, T.; Ryu, M.-H.; Chao, Y.; Kato, K.; Chung, H.C.; Chen, J.-S.; Muro, K.; Kang, W.K.; et al. Nivolumab in patients with advanced gastric or gastro-oesophageal junction cancer refractory to, or intolerant of, at least two previous chemotherapy regimens (ONO-4538-12, ATTRACTION-2): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 390, 2461–2471. [Google Scholar] [CrossRef]
- Janjigian, Y.Y.; Bendell, J.; Calvo, E.; Kim, J.W.; Ascierto, P.A.; Sharma, P.; Ott, P.A.; Peltola, K.; Jaeger, D.; Evans, J.; et al. CheckMate-032 study: Efficacy and safety of nivolumab and nivolumab plus ipilimumab in patients with metastatic esophagogastric cancer. J. Clin. Oncol. 2018, 36, 2836–2844. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Overall (n = 248) | Non-AKI (n = 180) | ICPi-AKI (n = 68) | p Value |
|---|---|---|---|---|
| Male (%) | 181 (73.0) | 138 (76.7) | 43 (63.2) | |
| Age, median (IRQ) | 59.50 (51.00, 67.00) | 60.00 (52.75, 67.00) | 57.00 (49.00, 64.25) | 0.053 |
| BMI, median (IRQ) | 23.10 (20.38, 25.40) | 23.10 (20.50, 25.40) | 22.75 (19.90, 25.45) | 0.521 |
| Malignancy type (%) | 0.16 | |||
| Mammary cancer | 2 (0.8) | 2 (1.1) | 0 (0.0) | |
| Colorectum cancer | 15 (6.0) | 11 (6.1) | 4 (5.9) | |
| Gastrointestinal tract cancer | 42 (16.9) | 28 (15.6) | 14 (20.6) | |
| Genitourinary cancer | 17 (6.9) | 15 (8.3) | 2 (2.9) | |
| Hepatobiliary cancer | 52 (21.0) | 34 (18.9) | 18 (26.5) | |
| Lung cancer | 91 (36.7) | 73 (40.6) | 18 (26.5) | |
| Melanoma | 2 (0.8) | 1 (0.6) | 1 (1.5) | |
| Other | 27 (10.9) | 16 (8.9) | 11 (16.2) | |
| Concomitant medications | ||||
| ACEI/ARB (%) | 32 (12.9) | 30 (16.7) | 2 (2.9) | 0.008 |
| Antibiotic (%) | 9 (3.6) | 3 (1.7) | 6 (8.8) | 0.021 |
| Diuretic (%) | 75 (30.2) | 46 (25.6) | 29 (42.6) | 0.014 |
| NSAIDS (%) | 125 (50.4) | 69 (38.3) | 56 (82.4) | <0.001 |
| Chemotherapy (%) | 68 (27.4) | 46 (25.6) | 22 (32.4) | 0.362 |
| PPI (%) | 186 (75.0) | 121 (67.2) | 65 (95.6) | <0.001 |
| Comorbidity | ||||
| Diabetes (%) | 43 (17.3) | 28 (15.6) | 15 (22.1) | 0.308 |
| Hypertension (%) | 68 (27.4) | 44 (24.4) | 24 (35.3) | 0.121 |
| Coronary heart disease (%) | 22 (8.9) | 19 (10.6) | 3 (4.4) | 0.205 |
| Cerebrovascular (%) | 11 (4.4) | 9 (5.0) | 2 (2.9) | 0.721 |
| Liver disease (%) | 38 (15.3) | 26 (14.4) | 12 (17.6) | 0.669 |
| ICPi type | ||||
| Nivolumab (%) | 99 (39.9) | 61 (33.9) | 38 (55.9) | 0.003 |
| Pembrolizumab (%) | 86 (34.7) | 59 (32.8) | 27 (39.7) | 0.383 |
| Ipilimumab (%) | 9 (3.6) | 5 (2.8) | 4 (5.9) | 0.432 |
| Toripalimab (%) | 23 (9.3) | 23 (12.8) | 0 (0.0) | 0.004 |
| Sintilimab (%) | 40 (16.1) | 34 (18.9) | 6 (8.8) | 0.084 |
| Camrelizumab (%) | 3 (1.2) | 3 (1.7) | 0 (0.0) | 0.674 |
| Atezolizumab (%) | 5 (2.0) | 4 (2.2) | 1 (1.5) | 1 |
| Laboratory test indicators | ||||
| HB, mean (SD) | 116.56 (21.87) | 120.04 (21.88) | 107.37 (19.11) | <0.001 |
| WBC, median (IQR) | 6.22 (4.50, 7.81) | 6.22 (4.48, 8.01) | 6.32 (4.59, 7.60) | 0.946 |
| PLT, median (IQR) | 199.00 (147.75, 259.50) | 206.50 (152.75, 259.50) | 183.50 (138.00, 257.25) | 0.186 |
| NE, median (IQR) | 0.70 (0.62, 0.78) | 0.69 (0.61, 0.77) | 0.74 (0.66, 0.79) | 0.038 |
| LYM, median (IQR) | 0.19 (0.14, 0.26) | 0.20 (0.14, 0.27) | 0.18 (0.13, 0.24) | 0.093 |
| ALB, mean (SD) | 37.75 (4.61) | 38.41 (4.41) | 35.99 (4.70) | <0.001 |
| SCR, median (IQR) | 68.50 (55.35, 81.85) | 70.30 (57.58, 82.78) | 60.45 (50.55, 76.42) | 0.006 |
| ALT, median (IQR) | 17.00 (11.20, 25.77) | 16.30 (11.20, 24.90) | 18.35 (11.15, 33.73) | 0.459 |
| AST, median (IQR) | 19.30 (14.88, 29.65) | 19.40 (14.45, 27.85) | 19.00 (15.33, 34.67) | 0.423 |
| eGFR, median (IQR) | 96.90 (83.23, 107.25) | 95.43 (80.63, 104.96) | 103.62 (89.14, 111.47) | 0.006 |
| LDH, median (IQR) | 181.60 (148.07, 256.58) | 180.45 (150.05, 249.10) | 183.95 (145.67, 285.07) | 0.598 |
| D-DIMER, median (IQR) | 1.04 (0.52, 2.67) | 0.93 (0.44, 2.43) | 1.36 (0.81, 3.80) | 0.003 |
| HCT, mean (SD) | 0.34 (0.06) | 0.35 (0.06) | 0.32 (0.06) | <0.001 |
| Patients with ICPi-AKI | N = 68 (4.2% of all Patients) |
|---|---|
| AKI stage (%) | |
| Stage 1 | 48 (70.5) |
| Stage 2 | 15 (22.1) |
| Stage 3 | 5 (7.4) |
| Gradations of diagnostic uncertainty | |
| Definite ICPi-AKI | 0 |
| Probable ICPi-AKI | 21 (30.9) |
| Possible ICPi-AKI | 47 (69.1) |
| Urinalysis results | 55 (80.9) |
| Leukocyturia | 11 (16.2) |
| Microscopic hematuria | 19 (27.9) |
| Albuminuria | 35 (51.5) |
| Extrarenal IRAEs | 12 (17.6) |
| Immune associated pneumonia | 5 (7.4) |
| Immune associated hepatitis | 3 (4.4) |
| Immune related pleural effusion | 2(2.9) |
| Immune associated enteritis | 1 (1.5) |
| Immune associated fever | 1 (1.5) |
| Variables | Overall (n = 248) | Training Group (n = 174) | Testing Group (n = 74) | p Value |
|---|---|---|---|---|
| ICPi-AKI (%) | 68 (27.4) | 48 (27.6) | 20 (27.0) | |
| Male (%) | 181 (73.0) | 124 (71.3) | 57 (77.0) | 0.436 |
| Age, median (IRQ) | 59.50 [51.00, 67.00] | 60.00 [52.00, 67.00] | 59.00 [51.00, 66.00] | 0.673 |
| BMI, median (IRQ) | 23.10 [20.38, 25.40] | 23.20 [20.33, 25.28] | 22.55 [20.40, 25.67] | 0.823 |
| Malignancy type (%) | 0.779 | |||
| mammary cancer | 2 (0.8) | 1 (0.6) | 1 (1.4) | |
| Colorectum cancer | 15 (6.0) | 12 (6.9) | 3 (4.1) | |
| Gastrointestinal tract cancer | 42 (16.9) | 30 (17.2) | 12 (16.2) | |
| Genitourinary cancer | 17 (6.9) | 11 (6.3) | 6 (8.1) | |
| Hepatobiliary cancer | 52 (21.0) | 36 (20.7) | 16 (21.6) | |
| Lung cancer | 91 (36.7) | 66 (37.9) | 25 (33.8) | |
| Melanoma | 2 (0.8) | 2 (1.1) | 0 (0.0) | |
| Other | 27 (10.9) | 16 (9.2) | 11 (14.9) | |
| Medication (%) | ||||
| ACEI/ARB | 32 (12.9) | 18 (10.3) | 14 (18.9) | 0.102 |
| Antibiotic | 9 (3.6) | 6 (3.4) | 3 (4.1) | 1 |
| Diuretic | 75 (30.2) | 51 (29.3) | 24 (32.4) | 0.735 |
| NSAIDS | 125 (50.4) | 86 (49.4) | 39 (52.7) | 0.739 |
| Chemotherapy | 68 (27.4) | 53 (30.5) | 15 (20.3) | 0.136 |
| PPI | 186 (75.0) | 136 (78.2) | 50 (67.6) | 0.109 |
| Comorbidity (%) | ||||
| Diabetes | 43 (17.3) | 30 (17.2) | 13 (17.6) | 1 |
| Hypertension | 68 (27.4) | 47 (27.0) | 21 (28.4) | 0.948 |
| Coronary heart disease | 22 (8.9) | 16 (9.2) | 6 (8.1) | 0.975 |
| Cerebrovascular | 11 (4.4) | 7 (4.0) | 4 (5.4) | 0.883 |
| Liver disease | 38 (15.3) | 27 (15.5) | 11 (14.9) | 1 |
| Checkpoint inhibitor type | ||||
| Nivolumab | 99 (39.9) | 70 (40.2) | 29 (39.2) | 0.991 |
| Pembrolizumab | 86 (34.7) | 58 (33.3) | 28 (37.8) | 0.592 |
| Ipilimumab | 9 (3.6) | 6 (3.4) | 3 (4.1) | 1 |
| Toripalimab | 23 (9.3) | 14 (8.0) | 9 (12.2) | 0.433 |
| Sintilimab | 40 (16.1) | 34 (19.5) | 6 (8.1) | 0.04 |
| Camrelizumab | 3 (1.2) | 2 (1.1) | 1 (1.4) | 1 |
| Atezolizumab | 5 (2.0) | 2 (1.1) | 3 (4.1) | 0.32 |
| Laboratory test indicators | ||||
| HB, mean (SD) | 116.56 (21.87) | 117.33 (22.16) | 114.76 (21.20) | 0.397 |
| WBC, median (IQR) | 6.22 [4.50, 7.81] | 6.08 [4.42, 7.79] | 6.74 [4.79, 7.87] | 0.145 |
| PLT, median (IQR) | 199.00 [147.75, 259.50] | 188.00 [147.25, 248.75] | 218.00 [149.50, 277.75] | 0.097 |
| NE, median (IQR) | 0.70 [0.62, 0.78] | 0.70 [0.62, 0.77] | 0.71 [0.64, 0.78] | 0.478 |
| LYM, median (IQR) | 0.19 [0.14, 0.26] | 0.20 [0.14, 0.27] | 0.17 [0.13, 0.23] | 0.067 |
| ALB, mean (SD) | 37.75 (4.61) | 37.94 (4.71) | 37.29 (4.36) | 0.309 |
| SCr, median (IQR) | 68.50 [55.35, 81.85] | 67.15 [55.12, 81.15] | 71.70 [56.90, 82.38] | 0.241 |
| ALT, median (IQR) | 17.00 [11.20, 25.77] | 17.30 [11.35, 26.10] | 16.00 [11.20, 24.77] | 0.407 |
| AST, median (IQR) | 19.30 [14.88, 29.65] | 18.80 [14.30, 29.20] | 20.55 [15.53, 30.50] | 0.504 |
| eGFR, median (IQR) | 96.90 [83.23, 107.25] | 97.90 [84.88, 108.09] | 93.86 [83.16, 104.74] | 0.174 |
| LDH, median (IQR) | 181.60 [148.07, 256.58] | 179.60 [147.55, 246.17] | 190.70 [151.12, 278.98] | 0.295 |
| D-DIMER, median (IQR) | 1.04 [0.52, 2.67] | 0.98 [0.44, 2.46] | 1.15 [0.68, 3.66] | 0.041 |
| HCT, mean (SD) | 0.34 (0.06) | 0.35 (0.06) | 0.34 (0.06) | 0.677 |
| Model | Accuracy | AUROC | F1-Score | Recall | Precision | MCC |
|---|---|---|---|---|---|---|
| Support Vector Machine (SVM) with radial kernel | 0.7297 | 0.8093 | NA | 0 | NA | - |
| Support Vector Machine (SVM) with sigmoid kernel | 0.7568 | 0.7787 | 0.5 | 0.45 | 0.5625 | 0.3456 |
| Support Vector Machine (SVM) with polynomial kernel | 0.7297 | 0.813 | NA | 0 | NA | - |
| Decision Tree (DT) | 0.7568 | 0.7764 | 0.625 | 0.75 | 0.5357 | 0.4663 |
| Random Forest (RF) | 0.7432 | 0.8241 | 0.2963 | 0.2 | 0.5714 | 0.2192 |
| logistic Regression (LR) | 0.7703 | 0.7204 | 0.5405 | 0.5 | 0.5882 | 0.3910 |
| Neural Networks (NNs) | 0.7703 | 0.8167 | 0.6222 | 0.7 | 0.56 | 0.4660 |
| Adaptive Boosting (Adaboost) | 0.7568 | 0.8 | 0.5714 | 0.6 | 0.5455 | 0.4030 |
| Extreme Gradient Boosting (XGboost) | 0.6892 | 0.7685 | 0.4651 | 0.5 | 0.4348 | 0.2488 |
| Naïve Bayes (NBs) | 0.7297 | 0.7861 | 0.5833 | 0.7 | 0.5 | 0.4036 |
| Model | Accuracy | AUROC | F1-Score | Recall | Precision | MCC |
|---|---|---|---|---|---|---|
| Support Vector Machine (SVM) with radial kernel | 0.7568 | 0.8315 | 0.60769 | 0.6 | 0.66667 | 0.2651 |
| Support Vector Machine (SVM) with sigmoid kernel | 0.7432 | 0.8287 | 0.42424 | 0.35 | 0.53846 | 0.2788 |
| Support Vector Machine (SVM) with polynomial kernel | 0.7297 | 0.8213 | NA | 0 | NA | - |
| Decision Tree (DT) | 0.7973 | 0.8056 | 0.6341 | 0.65 | 0.619 | 0.4944 |
| Random Forest (RF) | 0.7297 | 0.8306 | 0.375 | 0.3 | 0.5 | 0.2276 |
| logistic Regression (LR) | 0.7568 | 0.7528 | 0.5263 | 0.5 | 0.5556 | 0.3642 |
| Neural Networks (NNs) | 0.6622 | 0.769 | 0.5098 | 0.65 | 0.4194 | 0.2850 |
| Adaptive Boosting (Adaboost) | 0.7162 | 0.8009 | 0.4324 | 0.4 | 0.4706 | 0.2463 |
| Extreme Gradient Boosting (XGboost) | 0.7297 | 0.7713 | 0.4737 | 0.45 | 0.5 | 0.2933 |
| Naïve Bayes (NBs) | 0.7432 | 0.8037 | 0.5778 | 0.65 | 0.52 | 0.4017 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, X.; Wu, R.; Ji, Y.; Huang, M.; Feng, Z. Identifying Patients at Risk of Acute Kidney Injury among Patients Receiving Immune Checkpoint Inhibitors: A Machine Learning Approach. Diagnostics 2022, 12, 3157. https://doi.org/10.3390/diagnostics12123157
Yu X, Wu R, Ji Y, Huang M, Feng Z. Identifying Patients at Risk of Acute Kidney Injury among Patients Receiving Immune Checkpoint Inhibitors: A Machine Learning Approach. Diagnostics. 2022; 12(12):3157. https://doi.org/10.3390/diagnostics12123157
Chicago/Turabian StyleYu, Xiang, Rilige Wu, Yuwei Ji, Mengjie Huang, and Zhe Feng. 2022. "Identifying Patients at Risk of Acute Kidney Injury among Patients Receiving Immune Checkpoint Inhibitors: A Machine Learning Approach" Diagnostics 12, no. 12: 3157. https://doi.org/10.3390/diagnostics12123157