
Transjugular Intrahepatic Portosystemic Shunt in Chronic Portal Vein Thrombosis—From Routine Recommendations to Demanding Scenarios

Abstract
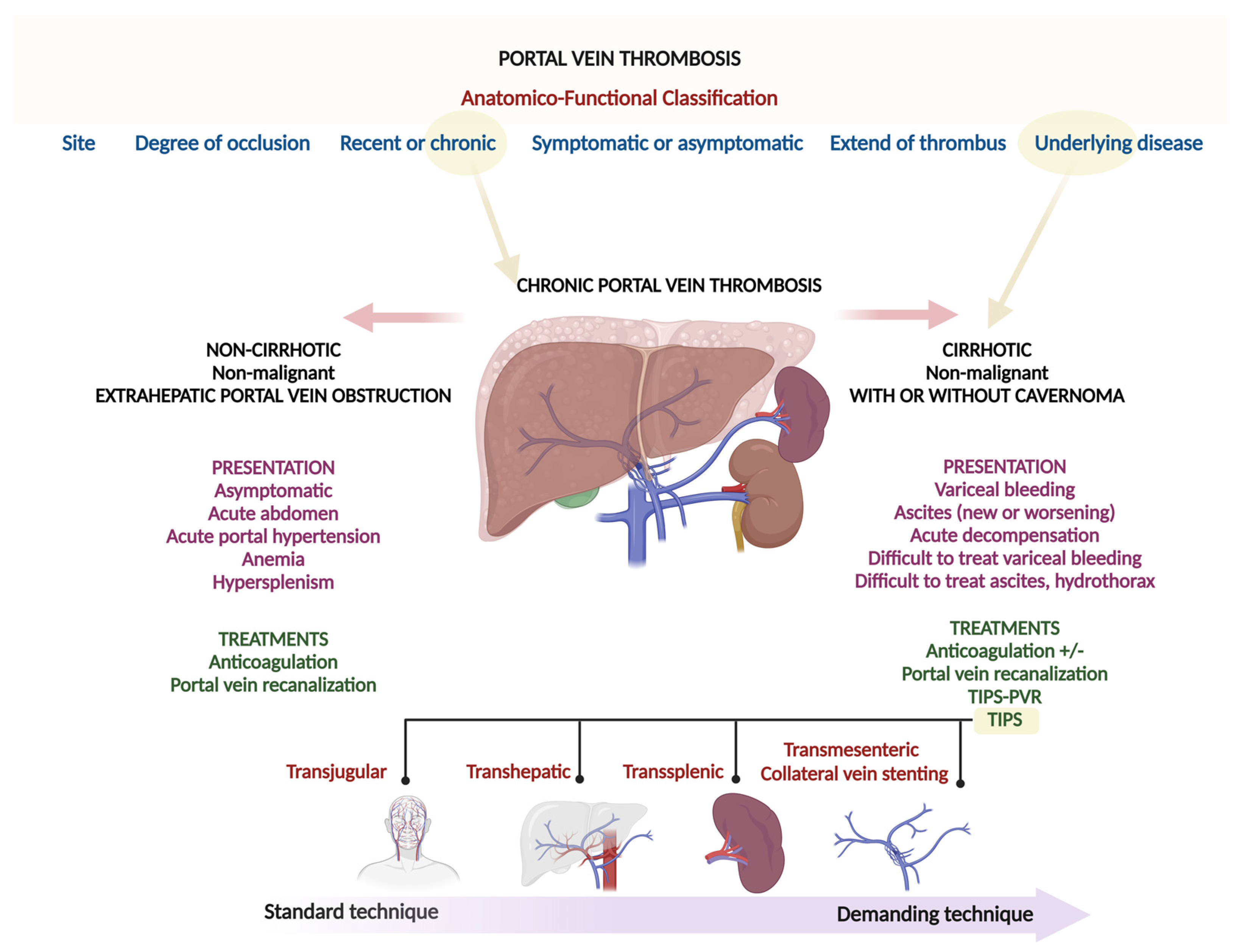
:1. Introduction
2. Interventional Strategies in Chronic PVT
3. Endovascular Therapies
4. Technical Challenges to TIPS and Modifications in Approach
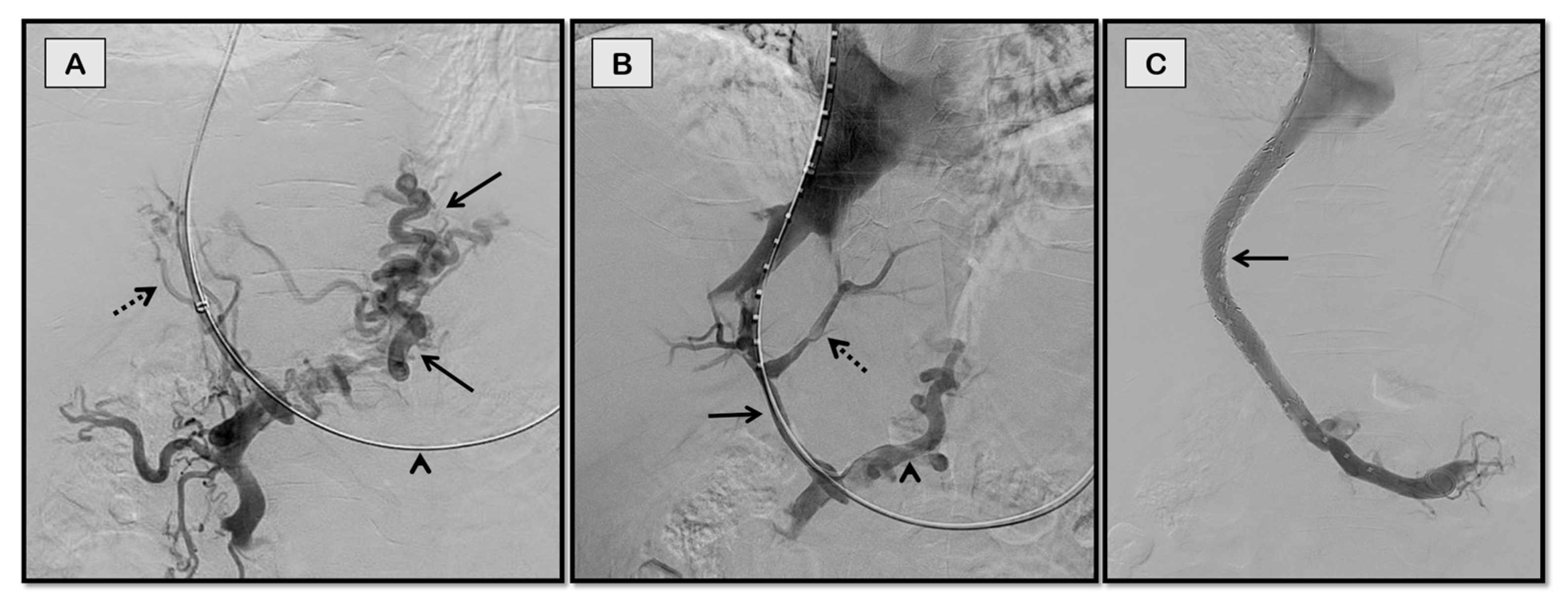
4.1. Transjugular Approach
4.2. Transhepatic Approach
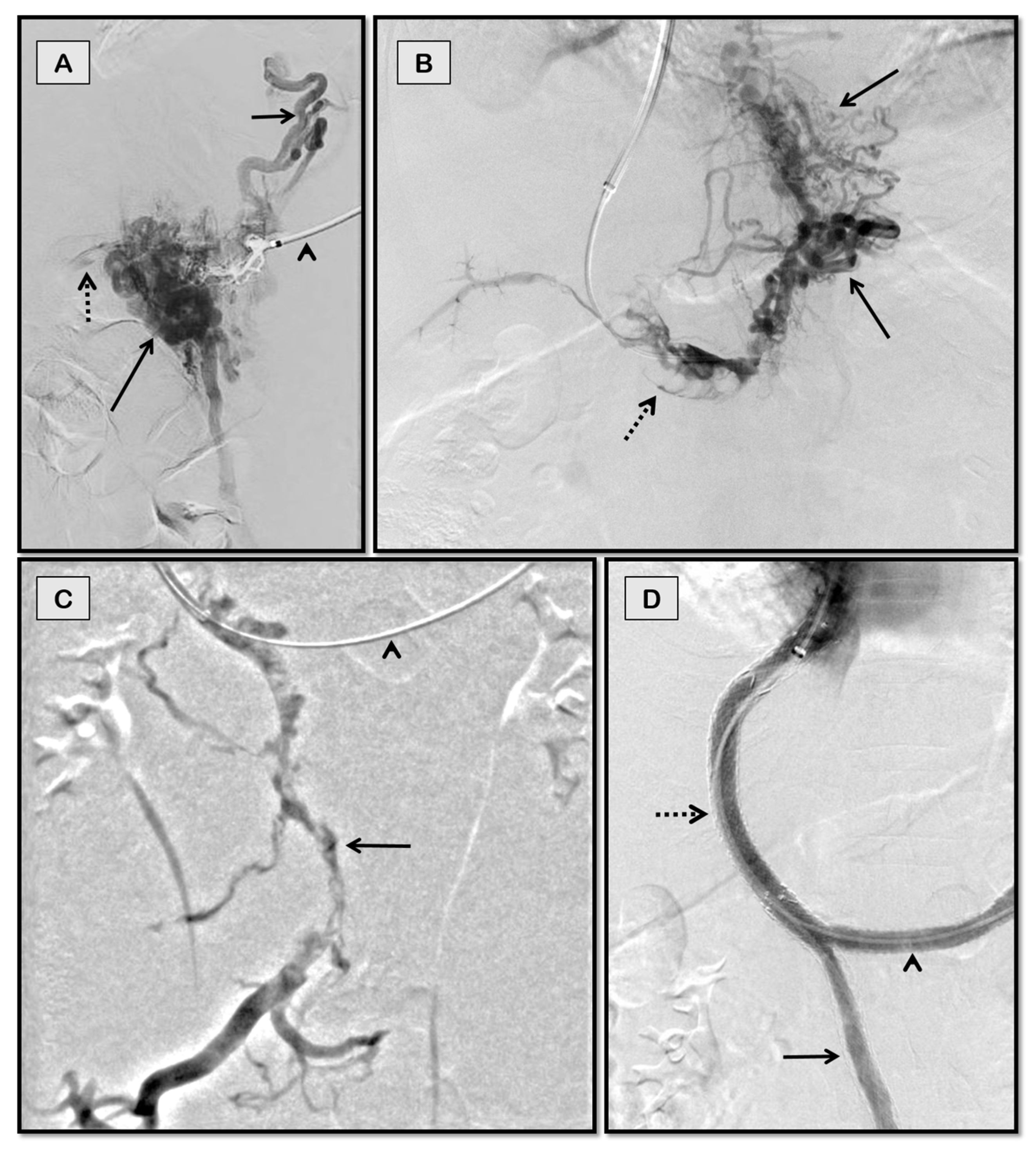
4.3. Trans-Splenic Approach
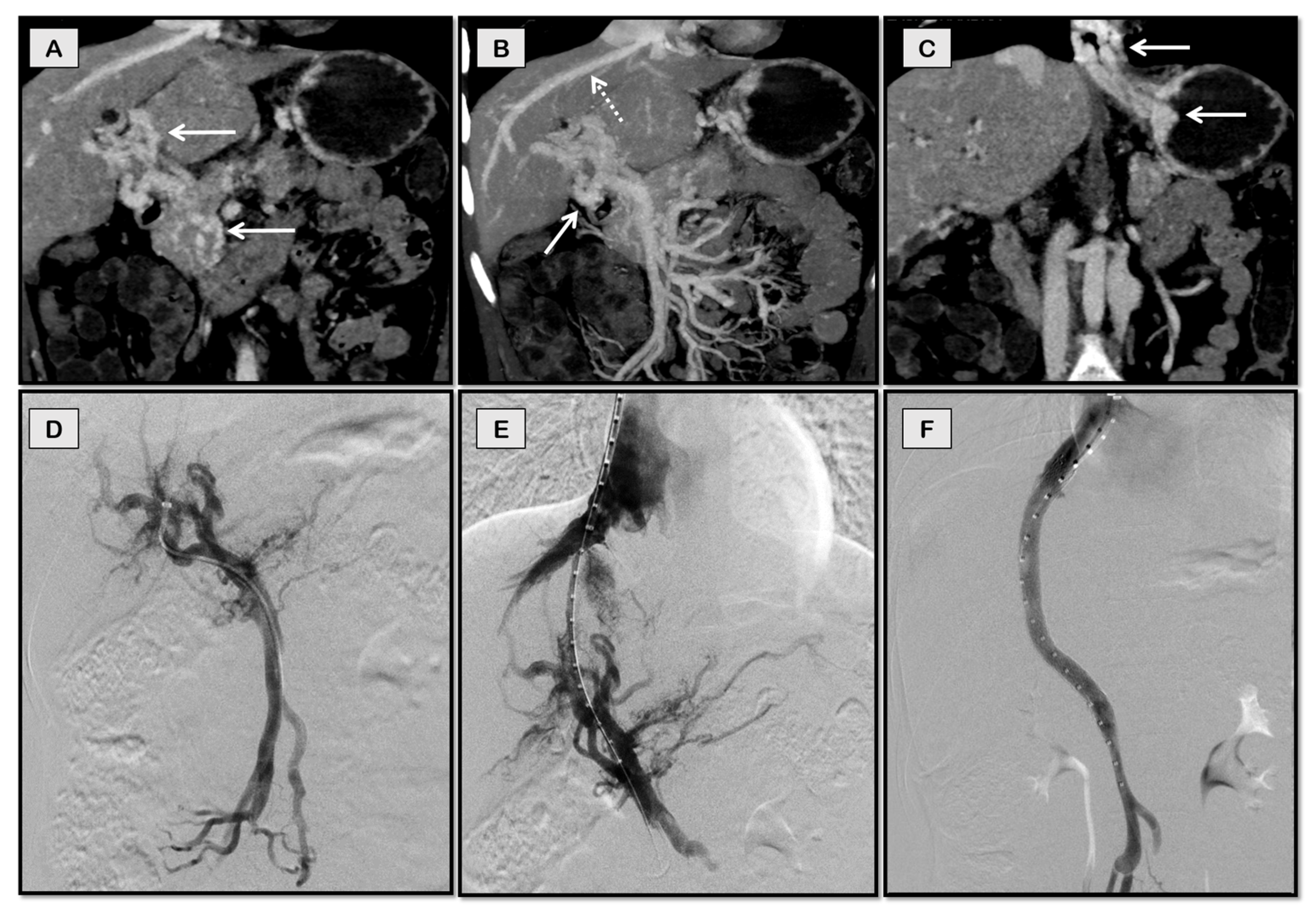
4.4. Transmesenteric Approach
4.5. Collateral Vein Stenting
5. TIPS—Technical Success, Complications, and Long-Term Patency
6. The Role of Anticoagulation
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ögren, M.; Bergqvist, D.; Björck, M.; Acosta, S.; Eriksson, H.; Sternby, N.H. Portal vein thrombosis: Prevalence, patient characteristics and lifetime risk: A population study based on 23 796 consecutive autopsies. World J. Gastroenterol. 2006, 12, 2115–2119. [Google Scholar] [CrossRef] [PubMed]
- Rajani, R.; Björnsson, E.; Bergquist, A.; Danielsson, Å.; Gustavsson, A.; Grip, O.; Melin, T.; Sangfelt, P.; Wallerstedt, S.; Almer, S. The epidemiology and clinical features of portal vein thrombosis: A multicentre study. Aliment. Pharmacol. Ther. 2010, 32, 1154–1162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khanna, R.; Sarin, S.K. Non-cirrhotic portal hypertension—Diagnosis and management. J. Hepatol. 2014, 60, 421–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Englesbe, M.J.; Schaubel, D.E.; Cai, S.; Guidinger, M.K.; Merion, R.M. Portal vein thrombosis and liver transplant survival benefit. Liver Transplant. 2010, 16, 999–1005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarin, S.K.; Agarwal, S.R. Extrahepatic Portal Vein Obstruction. Semin. Liver Dis. 2002, 22, 043–058. [Google Scholar] [CrossRef] [PubMed]
- Sarin, S.K.; Sollano, J.D.; Chawla, Y.K.; Amarapurkar, D.; Hamid, S.; Hashizume, M.; Jafri, W.; Kumar, A.; Kudo, M.; A Lesmana, L.; et al. Consensus on extra-hepatic portal vein obstruction. Liver Int. 2006, 26, 512–519. [Google Scholar] [CrossRef]
- Northup, P.G.; Garcia-Pagan, J.C.; Garcia-Tsao, G.; Intagliata, N.M.; Superina, R.A.; Roberts, L.N.; Lisman, T.; Valla, D.C. Vascular Liver Disorders, Portal Vein Thrombosis, and Procedural Bleeding in Patients with Liver Disease: 2020 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2021, 73, 366–413. [Google Scholar] [CrossRef]
- Null, N. EASL Clinical Practice Guidelines: Vascular diseases of the liver. J. Hepatol. 2016, 64, 179–202. [Google Scholar] [CrossRef]
- Artru, F.; Vietti-Violi, N.; Sempoux, C.; Barbosa, J.V.; Becce, F.; Sah, N.; Marot, A.; Deltenre, P.; Moschouri, E.; Fraga, M.; et al. Portal vein recanalisation alone to treat severe portal hypertension in non-cirrhotic patients with chronic extrahepatic portal vein obstruction. JHEP Rep. 2022, 4, 100511. [Google Scholar] [CrossRef]
- Benner, K.G.; Keeffe, E.B.; Keller, F.S.; Rösch, J. Clinical Outcome after Percutaneous Transhepatic Obliteration of Esophageal Varices. Gastroenterology 1983, 85, 146–153. [Google Scholar] [CrossRef]
- Smith-Laing, G.; Scott, J.; Long, R.G.; Dick, R.; Sherlock, S. Role of percutaneous transhepatic obliteration of varices in the management of hemorrhage from gastroesophageal varices. Gastroenterology 1981, 80, 1031–1036. [Google Scholar] [CrossRef] [PubMed]
- Pargewar, S.S.; Desai, S.N.; Rajesh, S.; Singh, V.P.; Arora, A.; Mukund, A. Imaging and radiological interventions in extra-hepatic portal vein obstruction. World J. Radiol. 2016, 8, 556–570. [Google Scholar] [CrossRef] [PubMed]
- Saxon, R.R.; Keller, F.S. Technical Aspects of Accessing the Portal Vein during the TIPS Procedure. J. Vasc. Interv. Radiol. 1997, 8, 733–744. [Google Scholar] [CrossRef] [PubMed]
- Radosevich, P.M.; Ring, E.J.; Laberge, J.M.; Peltzer, M.Y.; Haskal, Z.J.; Doherty, M.M.; Gordon, R.L. Transjugular intrahepatic portosystemic shunts in patients with portal vein occlusion. Radiology 1993, 186, 523–527. [Google Scholar] [CrossRef] [PubMed]
- Senzolo, M.; Tibbals, J.; Cholongitas, E.; Triantos, C.K.; Burroughs, A.K.; Patch, D. Transjugular intrahepatic portosystemic shunt for portal vein thrombosis with and without cavernous transformation. Aliment. Pharmacol. Ther. 2006, 23, 767–775. [Google Scholar] [CrossRef] [PubMed]
- Kallini, J.R.; Gabr, A.; Kulik, L.; Ganger, D.; Lewandowski, R.; Thornburg, B.; Salem, R. Noncirrhotic complete obliterative portal vein thrombosis: Novel management using trans-splenic transjugular intrahepatic portosystemic shunt with portal vein recanalization. Hepatology 2016, 63, 1387–1390. [Google Scholar] [CrossRef] [Green Version]
- Miraglia, R.; Maruzzelli, L.; Cannataci, C.; Gerasia, R.; Mamone, G.; Cortis, K.; Cimò, B.; Petridis, I.; Volpes, R.; Luca, A. Radiation exposure during transjugular intrahepatic portosystemic shunt creation in patients with complete portal vein thrombosis or portal cavernoma. Radiol. Med. 2020, 125, 609–617. [Google Scholar] [CrossRef]
- Zhu, K.; Meng, X.; Zhou, B.; Qian, J.; Huang, W.; Deng, M.; Shan, H. Percutaneous Transsplenic Portal Vein Catheterization: Technical Procedures, Safety, and Clinical Applications. J. Vasc. Interv. Radiol. 2013, 24, 518–527. [Google Scholar] [CrossRef]
- Haddad, M.M.; Fleming, C.J.; Thompson, S.M.; Reisenauer, C.J.; Parvinian, A.; Frey, G.; Toskich, B.; Andrews, J.C. Comparison of Bleeding Complications between Transplenic versus Transhepatic Access of the Portal Venous System. J. Vasc. Interv. Radiol. 2018, 29, 1383–1391. [Google Scholar] [CrossRef]
- Habib, A.; Desai, K.; Hickey, R.; Thornburg, B.; Vouche, M.; Vogelzang, R.L.; Salem, R. Portal Vein Recanalization–Transjugular Intrahepatic Portosystemic Shunt Using the Transsplenic Approach to Achieve Transplant Candidacy in Patients with Chronic Portal Vein Thrombosis. J. Vasc. Interv. Radiol. 2015, 26, 499–506. [Google Scholar] [CrossRef]
- Entezari, P.; Riaz, A.; Thornburg, B.; Salem, R. Percutaneous Ultrasound-Guided Superior and Inferior Mesenteric Vein Access for Portal Vein Recanalization–Transjugular Intrahepatic Portosystemic Shunt: A Case Series. Cardiovasc. Interv. Radiol. 2021, 44, 496–499. [Google Scholar] [CrossRef] [PubMed]
- Knight, G.M.; Clark, J.; Boike, J.R.; Maddur, H.; Ganger, D.R.; Talwar, A.; Riaz, A.; Desai, K.; Mouli, S.; Hohlastos, E.; et al. TIPS for Adults without Cirrhosis with Chronic Mesenteric Venous Thrombosis and EHPVO Refractory to Standard-of-Care Therapy. Hepatology 2021, 74, 2735–2744. [Google Scholar] [CrossRef] [PubMed]
- Klinger, C.; Riecken, B.; Schmidt, A.; De Gottardi, A.; Meier, B.; Bosch, J.; Caca, K. Transjugular portal vein recanalization with creation of intrahepatic portosystemic shunt (PVR-TIPS) in patients with chronic non-cirrhotic, non-malignant portal vein thrombosis. Z. Gastroenterol. 2018, 56, 221–237. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Ye, P.; Li, Y.; Ma, S.; Zhao, J.; Zeng, Q. Percutaneous transhepatic balloon-assisted transjugular intrahepatic portosystemic shunt for chronic, totally occluded, portal vein thrombosis with symptomatic portal hypertension: Procedure technique, safety, and clinical applications. Eur. Radiol. 2015, 25, 3431–3437. [Google Scholar] [CrossRef]
- Luo, J.; Li, M.; Zhang, Y.; Wang, H.; Huang, M.; Li, Z.; Chen, J.; Wu, C.; Qian, J.; Guan, S.; et al. Percutaneous transhepatic intrahepatic portosystemic shunt for variceal bleeding with chronic portal vein occlusion after splenectomy. Eur. Radiol. 2018, 28, 3661–3668. [Google Scholar] [CrossRef]
- Jourabchi, N.; McWilliams, J.P.; Lee, E.W.; Sauk, S.; Kee, S.T. TIPS Placement via Combined Transjugular and Transhepatic Approach for Cavernous Portal Vein Occlusion: Targeted Approach. Case Rep. Radiol. 2013, 2013, 635391. [Google Scholar] [CrossRef]
- Salem, R.; Vouche, M.; Baker, T.; Herrero, J.I.; Caicedo, J.C.; Fryer, J.; Hickey, R.; Habib, A.; Abecassis, M.; Koller, F.; et al. Pretransplant Portal Vein Recanalization—Transjugular Intrahepatic Portosystemic Shunt in Patients with Complete Obliterative Portal Vein Thrombosis. Transplantation 2015, 99, 2347–2355. [Google Scholar] [CrossRef]
- Talwar, A.; Varghese, J.; Knight, G.M.; Katariya, N.; Caicedo, J.; Dietch, Z.; Borja-Cacho, D.; Ladner, D.; Christopher, D.; Baker, T.; et al. Preoperative portal vein recanalization–transjugular intrahepatic portosystemic shunt for chronic obliterative portal vein thrombosis: Outcomes following liver transplantation. Hepatol. Commun. 2022, 6, 1803–1812. [Google Scholar] [CrossRef]
- Alani, M.; Rowley, M.; Kang, P.; Chen, S.; Hirsch, K.; Seetharam, A. Utility of Transjugular Intrahepatic Portosystemic Shunt Placement for Maintaining Portal Vein Patency in Candidates on Wait Lists Who Develop Thrombus. Exp. Clin. Transplant. 2020, 18, 808–813. [Google Scholar] [CrossRef]
- Valentin, N.; Korrapati, P.; Constantino, J.; Young, A.; Weisberg, I. The role of transjugular intrahepatic portosystemic shunt in the management of portal vein thrombosis: A systematic review and meta-analysis. Eur. J. Gastroenterol. Hepatol. 2018, 30, 1187–1193. [Google Scholar] [CrossRef]
- Zhang, J.-B.; Chen, J.; Zhou, J.; Wang, X.-M.; Chen, S.; Chu, J.-G.; Liu, P.; Ye, Z.-D. Systematic review and meta-analysis of trans-jugular intrahepatic portosystemic shunt for cirrhotic patients with portal vein thrombosis. World J. Clin. Cases 2021, 9, 5179–5190. [Google Scholar] [CrossRef]
- Young, K.; Wong, R. Evaluation and management of acute and chronic portal vein thrombosis in patients with cirrhosis. Clin. Liver Dis. 2017, 10, 152–156. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Guo, X.; Xu, X.; De Stefano, V.; Plessier, A.; Ferreira, C.N.; Qi, X. Anticoagulation Favors Thrombus Recanalization and Survival in Patients with Liver Cirrhosis and Portal Vein Thrombosis: Results of a Meta-Analysis. Adv. Ther. 2021, 38, 495–520. [Google Scholar] [CrossRef]
- Intagliata, N.M.; Ferreira, C.N.; Caldwell, S.H. Anticoagulation for portal vein thrombosis in cirrhosis. Clin. Liver Dis. 2016, 7, 126–131. [Google Scholar] [CrossRef]
- Wu, M.; Schuster, M.; Tadros, M. Update on Management of Portal Vein Thrombosis and the Role of Novel Anticoagulants. J. Clin. Transl. Hepatol. 2019, 7, 154. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Patients | Cirrhotic Non-cirrhotic | Cavernoma | Technical Success (%) | Mean Follow-Up (Months) | Patency (%) | Major Complication | Comments |
|---|---|---|---|---|---|---|---|---|
| Senzolo 2006 [15] | 28 | Both | 9/28 | 73 | 18.1 | 74 | 1/28 | The first large cohort study to show cavernoma is not a contraindication for TIPS Technically difficult Capsular and biliary punctures Extrahepatic portal vein laceration No fatal adverse events |
| Klinger 2018 [23] | 17 | Non-cirrhotic | 15/17 | 76.5 | 22.8 | 44.7 | 2/17 | Capsule rupture, intraperitoneal bleeding Liver hematoma Complex and difficult procedures, which only specialized centers with high experience should attempt |
| Chen 2015 [24] | 18 | Cirrhotic | 18/18 | 78 | 16 | 92.8 | 0/18 | The technical difficulty leading to open portosystemic shunt placement in four Two deaths reported were not related to the procedure |
| Salem 2015 [27] | 44 | Cirrhotic | 13/44 | 98 | 60 | 89 | 0/44 | TIPS-assisted recanalization led to the complete resolution of portal vein thrombus in 76% without anticoagulation Transplant-free survival was 82% at five years |
| Talwar 2021 [28] | 35 | Cirrhotic | 17/35 | 100 | - | 69 | 7/35 | TIPS-assisted recanalization is effective in resolving portal vein thrombosis Allowed for end-to-end portal vein anastomoses TIPS-assisted recanalization is a viable treatment option for chronic obliterative portal vein thrombosis with or without cavernoma that eases technical aspects during liver transplantation |
| Knight 2021 [22] | 39 | Non-cirrhotic | 39/39 | 100 | 36 | 63 | 3/39 | TIPS in chronic, non-cirrhotic extrahepatic portal vein obstruction with cavernomas and mesenteric venous thrombosis is technically feasible TIPS does not adversely affect liver function in this technically difficult-to-intervene group of patients |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rajesh, S.; Singh, S.; Philips, C.A. Transjugular Intrahepatic Portosystemic Shunt in Chronic Portal Vein Thrombosis—From Routine Recommendations to Demanding Scenarios. Diagnostics 2022, 12, 3100. https://doi.org/10.3390/diagnostics12123100
Rajesh S, Singh S, Philips CA. Transjugular Intrahepatic Portosystemic Shunt in Chronic Portal Vein Thrombosis—From Routine Recommendations to Demanding Scenarios. Diagnostics. 2022; 12(12):3100. https://doi.org/10.3390/diagnostics12123100
Chicago/Turabian StyleRajesh, Sasidharan, Shobhit Singh, and Cyriac Abby Philips. 2022. "Transjugular Intrahepatic Portosystemic Shunt in Chronic Portal Vein Thrombosis—From Routine Recommendations to Demanding Scenarios" Diagnostics 12, no. 12: 3100. https://doi.org/10.3390/diagnostics12123100