
A Narrative Review on Non-Cirrohotic Portal Hypertension: Not All Portal Hypertensions Mean Cirrhosis
 , , and
, , and
Abstract
:1. Introduction
2. Epidemiology
3. Pathophysiological Differences between NCPH and Cirrhosis
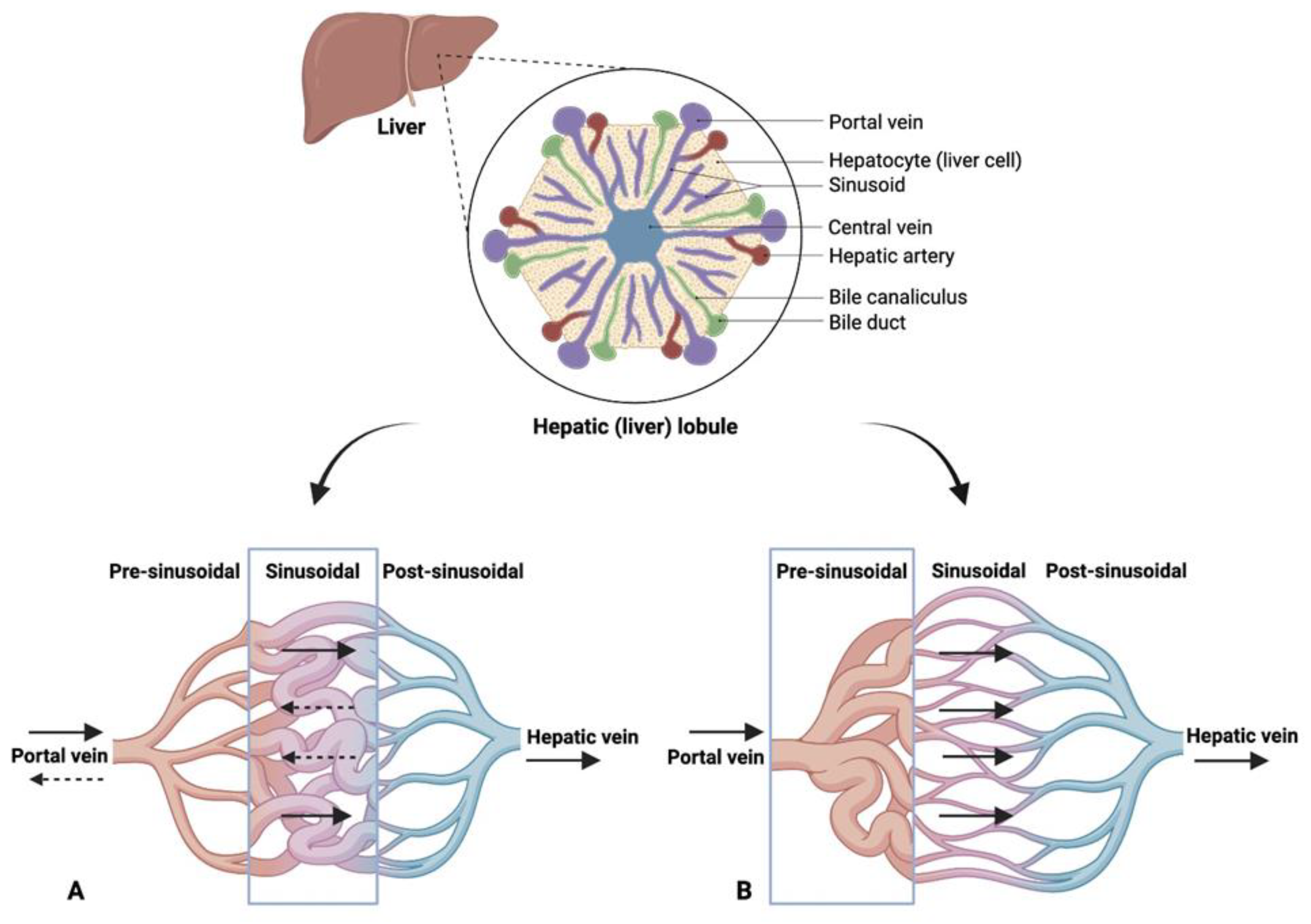
4. Pathophysiology
5. Etiology and Risk Factors
5.1. Immune-Related Factors
5.2. Coagulation Disorders
5.3. Infectious Etiology
5.4. Toxic or Chemical Agents
5.5. Genetic Predisposition
6. Natural History of NCPH
7. Diagnosis
7.1. Histological Features
- Obliterative Portal Venopathy: Previously referred to by several names like hepatoportal sclerosis, this lesion signifies the narrowing of the portal vein branch lumen to the extent of its complete disappearance and its substitution by fibrosis. As a result, portal tracts can appear fibrotic and hard to discern due to the veiled vein lumen. Various immunohistochemical methods can help identify such cases with portal vein stenosis being a significant independent predictor of NCPH.
- Nodular Regenerative Hyperplasia (NRH): This represents a diffuse micronodularity of the liver parenchyma devoid of fibrosis. A reticulin stain usually highlights NRH, revealing small hyperplastic hepatocyte nodules interspersed with atrophic plates, sometimes demonstrating signs of ischemic biliary metaplasia.
- Incomplete Septal Fibrosis/Cirrhosis: This complex entity shows liver parenchyma crisscrossed by thin, incomplete fibrotic bands. Despite being challenging to discern, this feature often correlates clinically with NCPH.
7.2. Clinical Implication
8. Management and Treatment
9. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Schouten, J.N.; Garcia-Pagan, J.C.; Valla, D.C.; Janssen, H.L. Idiopathic noncirrhotic portal hypertension. Hepatology 2011, 54, 1071–1081. [Google Scholar] [CrossRef]
- Banti, G. Splenomegalie mit Leberzirrhose Beitrage zur Pathologischen. Anat. Allg. Pathol. 1889, 24, 21–33. [Google Scholar]
- Kingham, J.G.; Levison, D.A.; Stansfeld, A.G.; Dawson, A.M. Non-cirrhotic intrahepatic portal hypertension: A long term follow-up study. QJM Int. J. Med. 1981, 50, 259–268. [Google Scholar]
- Mikkelsen, W.P.; Edmondson, H.A.; Peters, R.L.; Redeker, A.G.; Reynolds, T.B. Extra- and intrahepatic portal hypertension without cirrhosis (hepatoportal sclerosis). Ann. Surg. 1965, 162, 602–620. [Google Scholar] [CrossRef]
- Hillaire, S.; Bonte, E.; Denninger, M.H.; Casadevall, N.; Cadranel, J.F.; Lebrec, D.; Valla, D.; Degott, C. Idiopathic non-cirrhotic portal hypertension in the West: A re-evaluation in 28 patients. Gut 2002, 51, 275–280. [Google Scholar] [CrossRef]
- Madhu, K.; Avinash, B.; Ramakrishna, B.; Eapen, C.E.; Shyamkumar, N.K.; Zachariah, U.; Chandy, G.; Kurian, G. Idiopathic non-cirrhotic intrahepatic portal hypertension: Common cause of cryptogenic intrahepatic portal hypertension in a Southern Indian tertiary hospital. Indian J. Gastroenterol. 2009, 28, 83–87. [Google Scholar] [CrossRef]
- Kobayashi, Y.; Inokuchi, K.; Saku, M.; Yo, S. Epidemiology and clinical features of idiopathic portal hypertension. In 1975 Report of the Ministry of Health and Welfare Research Committee on Idiopathic Portal Hypertension; Ministry of Health and Welfare: Tokyo, Japan, 1975. [Google Scholar]
- Sarin, S.K.; Kumar, A.; Chawla, Y.K.; Baijal, S.S.; Dhiman, R.K.; Jafri, W.; Lesmana, L.A.; Guha Mazumder, D.; Omata, M.; Qureshi, H.; et al. Noncirrhotic portal fibrosis/idiopathic portal hypertension: APASL recommendations for diagnosis and treatment. Hepatol. Int. 2007, 1, 398–413. [Google Scholar] [CrossRef]
- Okudaira, M.; Ohbu, M.; Okuda, K. Idiopathic portal hypertension and its pathology. Semin. Liver Dis. 2002, 22, 59–72. [Google Scholar] [CrossRef]
- Iber, F.L. Obliterative portal venopathy of the liver and “idiopathic portal hypertension”. Ann. Intern. Med. 1969, 71, 660–661. [Google Scholar] [CrossRef]
- Wanless, I.R. Micronodular transformation (nodular regenerative hyperplasia) of the liver: A report of 64 cases among 2500 autopsies and a new classification of benign hepatocellular nodules. Hepatology 1990, 11, 787–797. [Google Scholar] [CrossRef]
- Schouten, J.N.; Nevens, F.; Hansen, B.; Laleman, W.; van den Born, M.; Komuta, M.; Roskams, T.; Verheij, J.; Janssen, H.L. Idiopathic noncirrhotic portal hypertension is associated with poor survival: Results of a long-term cohort study. Aliment. Pharmacol. Ther. 2012, 35, 1424–1433. [Google Scholar] [CrossRef] [PubMed]
- Siramolpiwat, S.; Seijo, S.; Miquel, R.; Berzigotti, A.; Garcia-Criado, A.; Darnell, A.; Turon, F.; Hernandez-Gea, V.; Bosch, J.; Garcia-Pagán, J.C. Idiopathic portal hypertension: Natural history and long-term outcome. Hepatology 2014, 59, 2276–2285. [Google Scholar] [CrossRef] [PubMed]
- Barge, S.; Grando, V.; Nault, J.C.; Broudin, C.; Beaugrand, M.; Ganne-Carrié, N.; Roulot, D.; Ziol, M. Prevalence and clinical significance of nodular regenerative hyperplasia in liver biopsies. Liver Int. 2016, 36, 1059–1066. [Google Scholar] [CrossRef] [PubMed]
- Ohnishi, K.; Chin, N.; Tanaka, H.; Iida, S.; Sato, S.; Terabayashi, H.; Nomura, F.l. Differences in portal hemodynamics in cirrhosis and idiopathic portal hypertension. Am. J. Gastroenterol. 1989, 84, 409–412. [Google Scholar]
- Guido, M.; Alves, V.A.F.; Balabaud, C.; Bathal, P.S.; Bioulac-Sage, P.; Colombari, R.; Crawford, J.M.; Dhillon, A.P.; Ferrell, L.D.; Gill, R.M.; et al. International Liver Pathology Study Group. Histology of portal vascular changes associated with idiopathic non-cirrhotic portal hypertension: Nomenclature and definition. Histopathology 2019, 74, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Futagawa, S.; Fukazawa, M.; Horisawa, M.; Musha, H.; Ito, T.; Sugiura, M.; Kameda, H.; Okuda, K. Portographic liver changes in idiopathic noncirrhotic portal hypertension. AJR Am. J. Roentgenol. 1980, 134, 917–923. [Google Scholar] [CrossRef]
- Khan, S.; Saxena, R. Regression of Hepatic Fibrosis and Evolution of Cirrhosis: A Concise Review. Adv. Anat. Pathol. 2021, 28, 408–414. [Google Scholar] [CrossRef]
- Montenovo, M.I.; Jalikis, F.G.; Yeh, M.; Reyes, J.D. Progression of Hepatic Adenoma to Carcinoma in the Setting of Hepatoportal Sclerosis in HIV Patient: Case Report and Review of the Literature. Case Rep. Hepatol. 2016, 2016, 1732069. [Google Scholar] [CrossRef]
- Nakanuma, Y.; Tsuneyama, K.; Ohbu, M.; Katayanagi, K. Pathology and pathogenesis of idiopathic portal hypertension with an emphasis on the liver. Pathol. Res. Pract. 2001, 197, 65–76. [Google Scholar] [CrossRef]
- De Gottardi, A.; Rautou, P.E.; Schouten, J.; Rubbia-Brandt, L.; Leebeek, F.; Trebicka, J.; Murad, S.D.; Vilgrain, V.; Hernandez-Gea, V.; Nery, F.; et al. Porto-sinusoidal vascular disease: Proposal and description of a novel entity. Lancet Gastroenterol. Hepatol. 2019, 4, 399–411. [Google Scholar] [CrossRef]
- Youssef, W.I.; Tavill, A.S. Connective tissue diseases and the liver. J. Clin. Gastroenterol. 2002, 35, 345–349. [Google Scholar] [CrossRef]
- Mahamid, J.; Miselevich, I.; Attias, D.; Laor, R.; Zuckerman, E.; Shaoul, R. Nodular regenerative hyperplasia associated with idiopathic thrombocytopenic purpura in a young girl: A case report and review of the literature. J. Pediatr. Gastroenterol. Nutr. 2005, 41, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Al-Mukhaizeem, K.A.; Rosenberg, A.; Sherker, A.H. Nodular regenerative hyperplasia of the liver: An under-recognized cause of portal hypertension in hematological disorders. Am. J. Hematol. 2004, 75, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Reshamwala, P.A.; Kleiner, D.E.; Heller, T. Nodular regenerative hyperplasia: Not all nodules are created equal. Hepatology 2006, 44, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, W.J.; Wanless, I.R. Nodular regenerative hyperplasia of the liver in a patient with rheumatoid vasculitis: A morphometric study suggesting a role for hepatic arteritis in the pathogenesis. J. Rheumatol. 1984, 11, 838–842. [Google Scholar]
- Ziol, M.; Poirel, H.; Kountchou, G.N.; Boyer, O.; Mohand, D.; Mouthon, L.; Tepper, M.; Guillet, J.G.; Guettier, C.; Raphael, M.; et al. Intrasinusoidal cytotoxic CD8+ T cells in nodular regenerative hyperplasia of the liver. Hum. Pathol. 2004, 35, 1241–1251. [Google Scholar] [CrossRef]
- Chang, P.E.; Miquel, R.; Blanco, J.L.; Laguno, M.; Bruguera, M.; Abraldes, J.G.; Bosch, J.; Garcia-Pagan, J.C. Idiopathic portal hypertension in patients with HIV infection treated with highly active antiretroviral therapy. Am. J. Gastroenterol. 2009, 104, 1707–1714. [Google Scholar] [CrossRef]
- Schouten, J.N.; Van der Ende, M.E.; Koëter, T.; Rossing, H.H.; Komuta, M.; Verheij, J.; van der Valk, M.; Hansen, B.E.; Janssen, H.L. Risk factors and outcome of HIV-associated idiopathic noncirrhotic portal hypertension. Aliment. Pharmacol. Ther. 2012, 36, 875–885. [Google Scholar] [CrossRef]
- Cachay, E.R.; Peterson, M.R.; Goicoechea, M.; Mathews, W.C. Didanosine Exposure and Noncirrhotic Portal Hypertension in a HIV Clinic in North America: A Follow-up Study. Br. J. Med. Med. Res. 2011, 1, 346–355. [Google Scholar] [CrossRef]
- Saito, K.; Nakanuma, Y.; Takegoshi, K.; Ohta, G.; Obata, Y.; Okuda, K.; Kameda, H. Non-specific immunological abnormalities and association of autoimmune diseases in idiopathic portal hypertension. A study by questionnaire. Hepatogastroenterology 1993, 40, 163–166. [Google Scholar]
- Inagaki, H.; Nonami, T.; Kawagoe, T.; Miwa, T.; Hosono, J.; Kurokawa, T.; Harada, A.; Nakao, A.; Takagi, H.; Suzuki, H.; et al. Idiopathic portal hypertension associated with systemic lupus erythematosus. J. Gastroenterol. 2000, 35, 235–239. [Google Scholar] [CrossRef] [PubMed]
- Tsuneyama, K.; Harada, K.; Katayanagi, K.; Watanabe, K.; Kurumaya, H.; Minato, H.; Nakanuma, Y. Overlap of idiopathic portal hypertension and scleroderma: Report of two autopsy cases and a review of literature. J. Gastroenterol. Hepatol. 2002, 17, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Rai, T.; Ohira, H.; Fukaya, E.; Abe, K.; Yokokawa, J.; Takiguchi, J.; Shishido, S.; Sato, Y. A case of merged idiopathic portal hypertension in course of mixed connective tissue disease. Hepatol. Res. 2004, 30, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Takagi, K.; Nishio, S.; Akimoto, K.; Yoshino, T.; Kawai, S. A case of systemic sclerosis complicated by idiopathic portal hypertension: Case report and literature review. Mod. Rheumatol. 2006, 16, 183–187. [Google Scholar] [CrossRef]
- Eapen, C.E.; Nightingale, P.; Hubscher, S.G.; Lane, P.J.; Plant, T.; Velissaris, D.; Elias, E. Non-cirrhotic intrahepatic portal hypertension: Associated gut diseases and prognostic factors. Dig. Dis. Sci. 2011, 56, 227–235. [Google Scholar] [CrossRef]
- Yamaguchi, N.; Tokushige, K.; Haruta, I.; Yamauchi, K.; Hayashi, N. Analysis of adhesion molecules in patients with idiopathic portal hypertension. J. Gastroenterol. Hepatol. 1999, 14, 364–369. [Google Scholar] [CrossRef]
- Köksal, A.S.; Köklü, S.; Ibiş, M.; Balci, M.; Ciçek, B.; Saşmaz, N.; Sahin, B. Clinical features, serum interleukin-6, and interferon-gamma levels of 34 turkish patients with hepatoportal sclerosis. Dig. Dis. Sci. 2007, 52, 3493–3498. [Google Scholar] [CrossRef]
- Kline, K.; Al Hanayneh, M.; Bilal, M.; Stevenson-Lerner, H. Portal vein thrombosis leading to pre-sinusoidal non-cirrhotic portal hypertension resulting in decreased synthetic function of the liver. Gastroenterol. Hepatol. Bed Bench 2019, 12, 174–177. [Google Scholar]
- Sarin, S.K.; Aggarwal, S.R. Idiopathic portal hypertension. Digestion 1998, 59, 420–423. [Google Scholar] [CrossRef]
- Kono, K.; Ohnishi, K.; Omata, M.; Saito, M.; Nakayama, T.; Hatano, H.; Nakajima, Y.; Sugita, S.; Okuda, K. Experimental portal fibrosis produced by intraportal injection of killed nonpathogenic Escherichia coli in rabbits. Gastroenterology 1988, 94, 787–796. [Google Scholar] [CrossRef]
- Austin, A.; Campbell, E.; Lane, P.; Elias, E. Nodular regenerative hyperplasia of the liver and coeliac disease: Potential role of IgA anticardiolipin antibody. Gut 2004, 53, 1032–1034. [Google Scholar] [CrossRef] [PubMed]
- Schiano, T.D.; Kotler, D.P.; Ferran, E.; Fiel, M.I. Hepatoportal sclerosis as a cause of noncirrhotic portal hypertension in patients with HIV. Am. J. Gastroenterol. 2007, 102, 2536–2540. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.W.; Kim, E.S.; Han, M.H.; Kweon, Y.O. Non-cirrhotic portal hypertension related to azathioprine therapy in a patient with Crohn’s disease. Intest. Res. 2021, 19, 247–251. [Google Scholar] [CrossRef] [PubMed]
- Fuentes-Lacouture, M.C.; Barrera-Garavito, E.C.; Gomez, A.; Mantilla, W. Non-Cirrhotic Portal Hypertension in a Patient with Colonic Carcinoma Treated with Oxaliplatin. J. Med. Cases 2021, 12, 99–101. [Google Scholar] [CrossRef] [PubMed]
- Vilarinho, S.; Sari, S.; Yilmaz, G.; Stiegler, A.L.; Boggon, T.J.; Jain, D.; Akyol, G.; Dalgic, B.; Günel, M.; Lifton, R.P. Recurrent recessive mutation in deoxyguanosine kinase causes idiopathic noncirrhotic portal hypertension. Hepatology 2016, 63, 1977–1986. [Google Scholar] [CrossRef] [PubMed]
- Calado, R.T.; Regal, J.A.; Kleiner, D.E.; Schrump, D.S.; Peterson, N.R.; Pons, V.; Chanock, S.J.; Lansdorp, P.M.; Young, N.S. A spectrum of severe familial liver disorders associate with telomerase mutations. PLoS ONE 2009, 4, e7926. [Google Scholar] [CrossRef]
- Sarin, S.K.; Kapoor, D. Non-cirrhotic portal fibrosis: Current concepts and management. J. Gastroenterol. Hepatol. 2002, 17, 526–534. [Google Scholar] [CrossRef]
- Schouten, J.N.; Verheij, J.; Seijo, S. Idiopathic non-cirrhotic portal hypertension: A review. Orphanet J. Rare Dis. 2015, 10, 67. [Google Scholar] [CrossRef]
- Gioia, S.; Nardelli, S.; Pasquale, C.; Pentassuglio, I.; Nicoletti, V.; Aprile, F.; Merli, M.; Riggio, O. Natural history of patients with non cirrhotic portal hypertension: Comparison with patients with compensated cirrhosis. Dig. Liver Dis. 2018, 50, 839–844. [Google Scholar] [CrossRef]
- Nicoletti, V.; Gioia, S.; Lucatelli, P.; Nardelli, S.; Pasquale, C.; Nogas Sobrinho, S.; Pentassuglio, I.; Greco, F.; De Santis, A.; Merli, M.; et al. Hepatic encephalopathy in patients with non-cirrhotic portal hypertension: Description, prevalence and risk factors. Dig. Liver Dis. 2016, 48, 1072–1077. [Google Scholar] [CrossRef]
- Bissonnette, J.; Garcia-Pagán, J.C.; Albillos, A.; Turon, F.; Ferreira, C.; Tellez, L.; Nault, J.C.; Carbonell, N.; Cervoni, J.P.; Abdel Rehim, M.; et al. Role of the transjugular intrahepatic portosystemic shunt in the management of severe complications of portal hypertension in idiopathic noncirrhotic portal hypertension. Hepatology 2016, 64, 224–231. [Google Scholar] [CrossRef]
- Maruyama, H.; Okugawa, H.; Kobayashi, S.; Yoshizumi, H.; Takahashi, M.; Ishibashi, H.; Yokosuka, O. Non-invasive portography: A microbubble-induced three-dimensional sonogram for discriminating idiopathic portal hypertension from cirrhosis. Br. J. Radiol. 2012, 85, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Palli, G.; Drake, B.B.; Garcia-Pagan, J.C.; Barbera, J.A.; Arguedas, M.R.; Rodriguez-Roisin, R.; Bosch, J.; Fallon, M.B. Effect of transjugular intrahepatic portosystemic shunt on pulmonary gas exchange in patients with portal hypertension and hepatopulmonary syndrome. World J. Gastroenterol. 2005, 11, 6858–6862. [Google Scholar] [CrossRef]
- Dhiman, R.K.; Chawla, Y.; Vasishta, R.K.; Kakkar, N.; Dilawari, J.B.; Trehan, M.S.; Puri, P.; Mitra, S.K.; Suri, S. Non-cirrhotic portal fibrosis (idiopathic portal hypertension): Experience with 151 patients and a review of the literature. J. Gastroenterol. Hepatol. 2002, 17, 6–16. [Google Scholar] [CrossRef]
- Friedrich-Rust, M.; Ong, M.F.; Martens, S.; Sarrazin, C.; Bojunga, J.; Zeuzem, S.; Herrmann, E. Performance of transient elastography for the staging of liver fibrosis: A meta-analysis. Gastroenterology 2008, 134, 960–974. [Google Scholar] [CrossRef] [PubMed]
- Elkrief, L.; Lazareth, M.; Chevret, S.; Paradis, V.; Magaz, M.; Blaise, L.; Rubbia-Brandt, L.; Moga, L.; Durand, F.; Payancé, A.; et al. Liver stiffness by transient elastography to detect porto-sinusoidal vascular liver disease with portal hypertension. Hepatology 2021, 74, 364–378. [Google Scholar] [CrossRef] [PubMed]
- Ferreira-Silva, J.; Gaspar, R.; Liberal, R.; Cardoso, H.; Macedo, G. Splenic-hepatic elastography index is useful in differentiating between porto-sinusoidal vascular disease and cirrhosis in patients with portal hypertension. Dig. Liver Dis. 2023, 55, 75–80. [Google Scholar] [CrossRef]
- Ferreira-Silva, J.; Gaspar, R.; Liberal, R.; Cardoso, H.; Macedo, G. Transient splenic elastography predicts high-risk esophageal varices in patients with non-cirrhotic portal hypertension. Scand. J. Gastroenterol. 2021, 56, 1462–1466. [Google Scholar] [CrossRef]
- Cerda Reyes, E.; González-Navarro, E.A.; Magaz, M.; Muñoz-Sánchez, G.; Diaz, A.; Silva-Junior, G.; Triguero, A.; Lafoz, E.; Campreciós, G.; Orts, L.; et al. Autoimmune biomarkers in porto-sinusoidal vascular disease: Potential role in its diagnosis and pathophysiology. Liver Int. 2021, 41, 2171–2178. [Google Scholar] [CrossRef]
- Goel, A.; Ramakrishna, B.; Muliyil, J.; Madhu, K.; Sajith, K.G.; Zachariah, U.; Ramachandran, J.; Keshava, S.N.; Selvakumar, R.; Chandy, G.M.; et al. Use of serum vitamin B12 level as a marker to differentiate idiopathic noncirrhotic intrahepatic portal hypertension from cryptogenic cirrhosis. Dig. Dis. Sci. 2013, 58, 179–187. [Google Scholar] [CrossRef]
- Sharma, M.; Padaki, N.R.; Reddy, D.N. Non-Cirrhotic Portal Hypertension in Myeloproliferative Disease: Left and Right-Sided Component of Portal Hypertension: 2970. Am. J. Gastroenterol. 2019, 114, S1613. [Google Scholar] [CrossRef]
- Noronha Ferreira, C.; Seijo, S.; Plessier, A.; Silva-Junior, G.; Turon, F.; Rautou, P.E.; Baiges, A.; Bureau, C.; Bosch, J.; Hernández-Gea, V.; et al. Natural history and management of esophagogastric varices in chronic noncirrhotic, nontumoral portal vein thrombosis. Hepatology 2016, 63, 1640–1650. [Google Scholar] [CrossRef] [PubMed]
- Gane, E.; Portmann, B.; Saxena, R.; Wong, P.; Ramage, J.; Williams, R. Nodular regenerative hyperplasia of the liver graft after liver transplantation. Hepatology 1994, 20, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Lv, Y.; Li, K.; He, C.; Luo, B.; Zhang, B.; Liu, H.; Wang, Z.; Guo, W.; Wang, Q.; Chen, H.; et al. TIPSS for variceal bleeding in patients with idiopathic non-cirrhotic portal hypertension: Comparison with patients who have cirrhosis. Aliment. Pharmacol. Ther. 2019, 49, 926–939. [Google Scholar] [CrossRef]
- Romano, M.; Giojelli, A.; Capuano, G.; Pomponi, D.; Salvatore, M. Partial splenic embolization in patients with idiopathic portal hypertension. Eur. J. Radiol. 2004, 49, 268–273. [Google Scholar] [CrossRef]
- Ozturk, O.; Eldem, G.; Peynircioglu, B.; Kav, T.; Görmez, A.; Cil, B.E.; Balkancı, F.; Sokmensuer, C.; Bayraktar, Y. Outcomes of partial splenic embolization in patients with massive splenomegaly due to idiopathic portal hypertension. World J. Gastroenterol. 2016, 22, 9623–9630. [Google Scholar] [CrossRef]
- Karagul, S.; Yagci, M.A.; Tardu, A.; Ertugrul, I.; Kirmizi, S.; Sumer, F.; Isik, B.; Kayaalp, C.; Yilmaz, S. Portosystemic shunt surgery in patients with idiopathic noncirrhotic portal hypertension. Ann. Transplant. 2016, 21, 317–320. [Google Scholar] [CrossRef]
- Rosemurgy, A.S.; Frohman, H.A.; Teta, A.F.; Luberice, K.; Ross, S.B. Prosthetic H-graft portacaval shunts vs transjugular intrahepatic portasystemic stent shunts: 18-year follow-up of a randomized trial. J. Am. Coll. Surg. 2012, 214, 445–453. [Google Scholar] [CrossRef]
- Rikkers, L.F. Operations for management of esophageal variceal hemorrhage. West. J. Med. 1982, 136, 107–121. [Google Scholar]
- Spina, G.P.; Galeotti, F.; Opocher, E.; Santambrogio, R.; Cucchiaro, G.; Lopez, C.; Pezzuoli, G. Selective distal splenorenal shunt versus side-to-side portacaval shunt. Clinical results of a prospective, controlled study. Am. J. Surg. 1988, 155, 564–571. [Google Scholar] [CrossRef]
- Doki, N.; Irisawa, H.; Takada, S.; Sakura, T.; Miyawaki, S. Transjugular intrahepatic portosystemic shunt for the treatment of portal hypertension due to idiopathic myelofibrosis. Intern. Med. 2007, 46, 187–190. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NCPH | Liver Cirrhosis | |
|---|---|---|
| Portal venous blood flow | increased | normal |
| Intrahepatic vascular resistance at the sinusoidal level | decreased | increased |
| Intrahepatic vascular resistance at the presinusoidal level | increased | decreased |
| Hepatic arterial blood flow | decreased | increased |
| Arterioportal shunts | negligible | many |
| Hepatic vein-to-hepatic vein anastomoses | frequently | rare |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fiordaliso, M.; Marincola, G.; Pala, B.; Muraro, R.; Mazzone, M.; Di Marcantonio, M.C.; Mincione, G. A Narrative Review on Non-Cirrohotic Portal Hypertension: Not All Portal Hypertensions Mean Cirrhosis. Diagnostics 2023, 13, 3263. https://doi.org/10.3390/diagnostics13203263
Fiordaliso M, Marincola G, Pala B, Muraro R, Mazzone M, Di Marcantonio MC, Mincione G. A Narrative Review on Non-Cirrohotic Portal Hypertension: Not All Portal Hypertensions Mean Cirrhosis. Diagnostics. 2023; 13(20):3263. https://doi.org/10.3390/diagnostics13203263
Chicago/Turabian StyleFiordaliso, Michele, Giuseppe Marincola, Barbara Pala, Raffaella Muraro, Mariangela Mazzone, Maria Carmela Di Marcantonio, and Gabriella Mincione. 2023. "A Narrative Review on Non-Cirrohotic Portal Hypertension: Not All Portal Hypertensions Mean Cirrhosis" Diagnostics 13, no. 20: 3263. https://doi.org/10.3390/diagnostics13203263