
Trajectories of Cognitive Impairment in Adults Bearing Vascular Risk Factors, with or without Diagnosis of Mild Cognitive Impairment: Findings from a Longitudinal Study Assessing Executive Functions, Memory, and Social Cognition

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
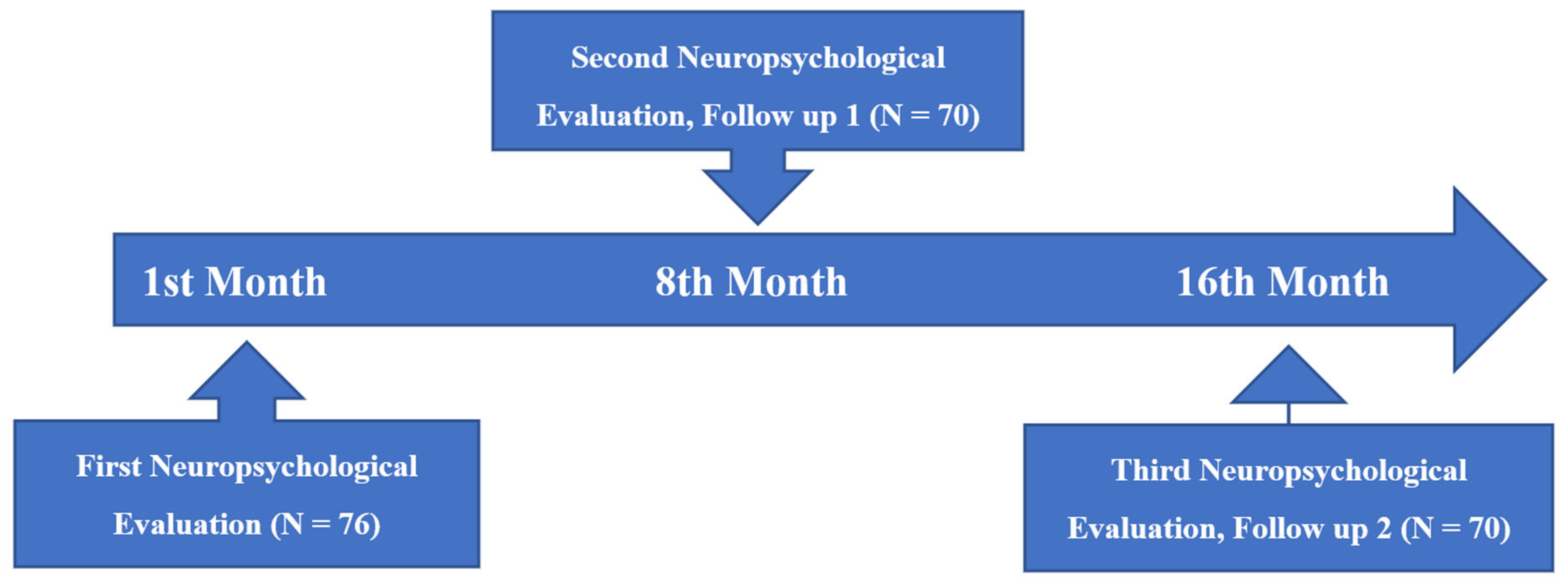
2.1. Design
2.2. Procedure
2.3. Ethics
2.4. Participants
3. Measures
3.1. Main Neuropsychological Assessment
3.1.1. Global Cognitive Status
3.1.2. Measures of Executive Functions
3.1.3. Measures of Memory
3.1.4. Measures of Theory of Mind
4. Statistical Analysis
4.1. Results
4.1.1. Global Cognitive Status
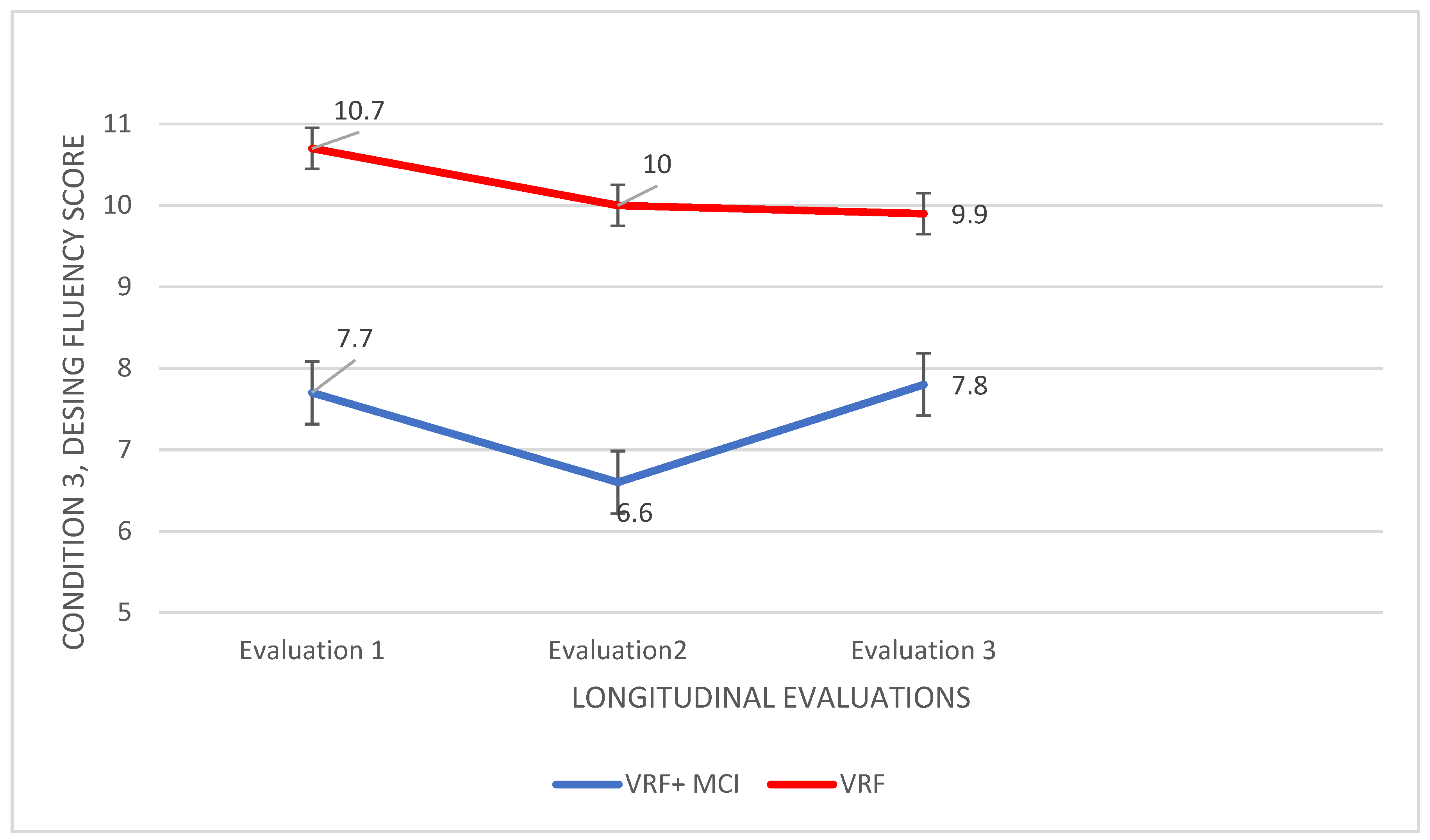
4.1.2. Executive Functions
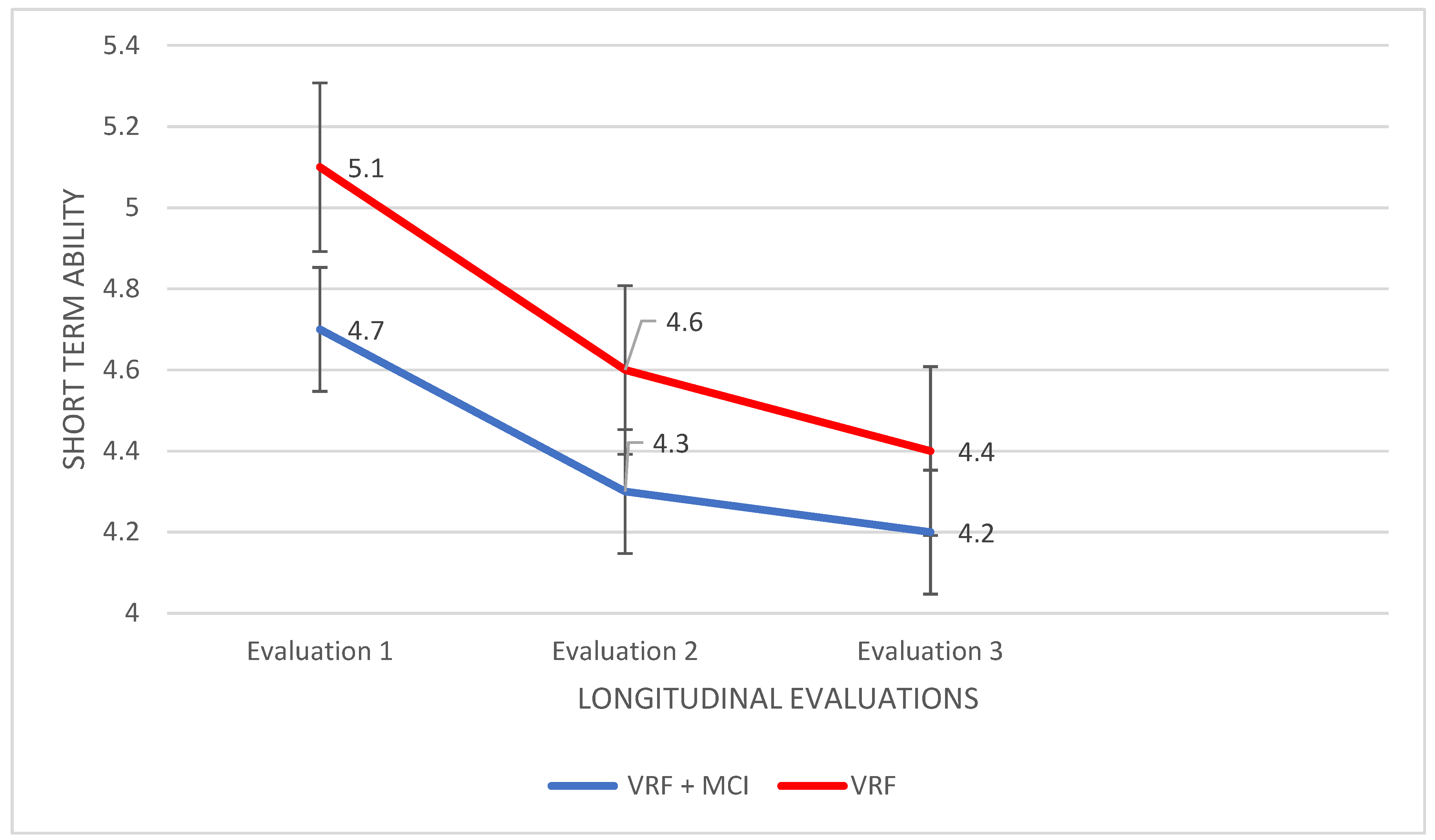
4.1.3. Memory
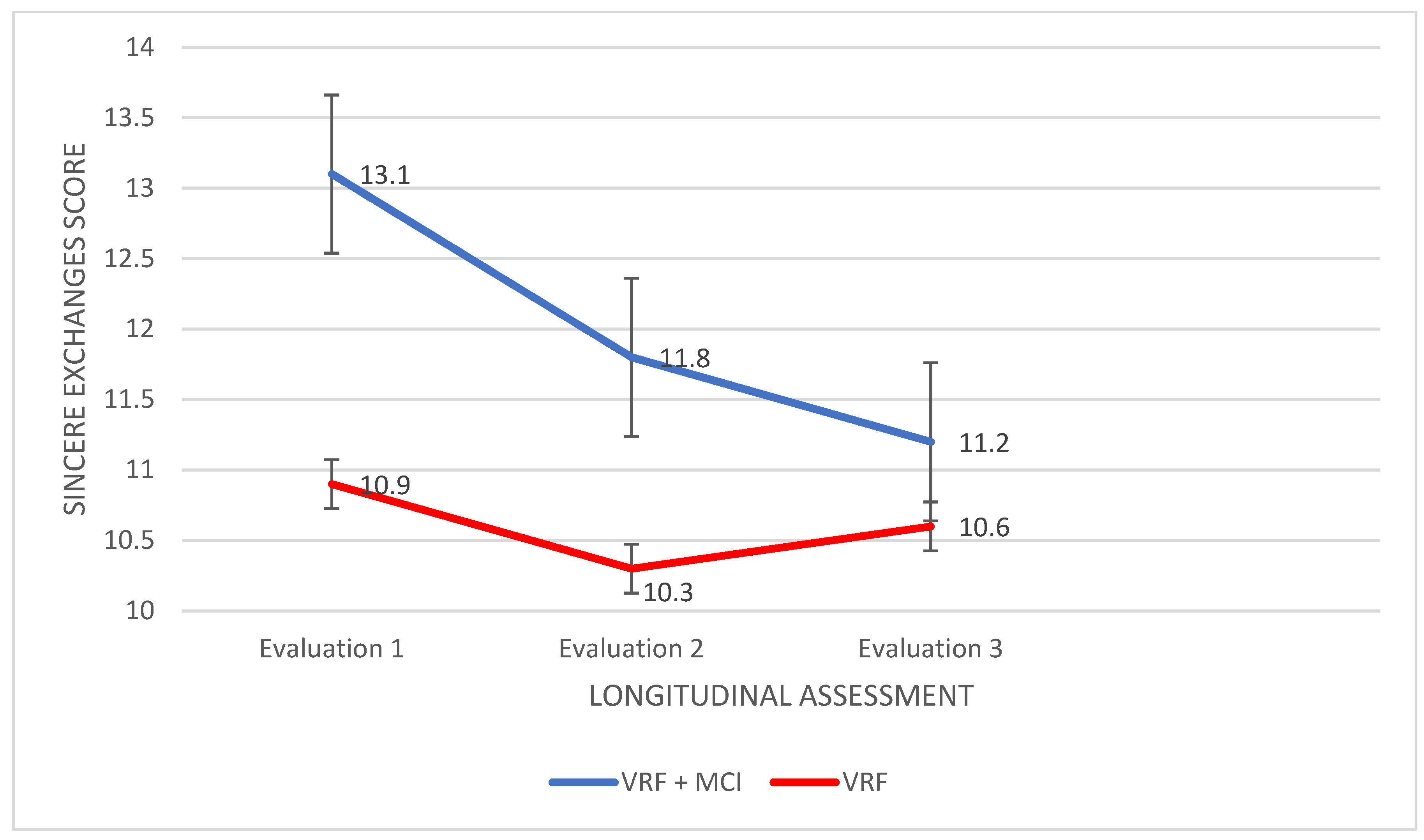
4.1.4. Theory of Mind
5. Discussion
5.1. Cognitive Abilities’ Decline in People with VRF
5.2. Social Cognition Abilities’ Decline in People with VRF + MCI
5.3. Cognitive Abilities Which Differentiate People with VRF from People with VRF + MCI
6. Conclusions
Limitations and Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zlokovic, B.V. The Blood-Brain Barrier in Health and Chronic Neurodegenerative Disorders. Neuron 2008, 57, 178–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersen, M.A.; Ryu, J.K.; Akassoglou, K. Fibrinogen in neurological diseases: Mechanisms, imaging and therapeutics. Nat. Rev. Neurosci. 2018, 19, 283–301. [Google Scholar] [CrossRef] [PubMed]
- Laurent, S.; Boutouyrie, P.; Cunha, P.G.; Lacolley, P.; Nilsson, P.M. Concept of Extremes in Vascular Aging. Hypertension 2019, 74, 218–228. [Google Scholar] [CrossRef] [PubMed]
- van Sloten, T.T.; Protogerou, A.D.; Henry, R.M.; Schram, M.T.; Launer, L.J.; Stehouwer, C.D. Association between arterial stiffness, cerebral small vessel disease and cognitive impairment: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2015, 53, 121–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merlini, M.; Rafalski, V.A.; Coronado, P.E.R.; Gill, T.M.; Ellisman, M.; Muthukumar, G.; Subramanian, K.S.; Ryu, J.K.; Syme, C.A.; Davalos, D.; et al. Fibrinogen Induces Microglia-Mediated Spine Elimination and Cognitive Impairment in an Alzheimer’s Disease Model. Neuron 2019, 101, 1099–1108.e6. [Google Scholar] [CrossRef] [Green Version]
- Cortes-Canteli, M.; Zamolodchikov, D.; Ahn, H.J.; Strickland, S.; Norris, E.H. Fibrinogen and Altered Hemostasis in Alzheimer’s Disease. J. Alzheimer’s Dis. 2012, 32, 599–608. [Google Scholar] [CrossRef] [Green Version]
- Chui, H.C.; Ramirez-Gomez, L. Clinical and imaging features of mixed Alzheimer and vascular pathologies. Alzheimer’s Res. Ther. 2015, 7, 21. [Google Scholar] [CrossRef] [Green Version]
- Qiu, C.; Winblad, B.; Fratiglioni, L. The age-dependent relation of blood pressure to cognitive function and dementia. Lancet Neurol. 2005, 4, 487–499. [Google Scholar] [CrossRef]
- Croteau, E.; Castellano, C.; Fortier, M.; Bocti, C.; Fulop, T.; Paquet, N.; Cunnane, S. A cross-sectional comparison of brain glucose and ketone metabolism in cognitively healthy older adults, mild cognitive impairment and early Alzheimer’s disease. Exp. Gerontol. 2018, 107, 18–26. [Google Scholar] [CrossRef]
- Bocti, C.; Pépin, F.; Tétreault, M.; Cossette, P.; Langlois, F.; Imbeault, H.; Duval, N.; Lacombe, G.; Fulop, T. Orthostatic hypotension associated with executive dysfunction in mild cognitive impairment. J. Neurol. Sci. 2017, 382, 79–83. [Google Scholar] [CrossRef]
- Wharton, W.; Hirshman, E.; Merritt, P.; Stangl, B.; Scanlin, K.; Krieger, L. Lower blood pressure correlates with poorer performance on visuospatial attention tasks in younger individuals. Biol. Psychol. 2006, 73, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Pyun, J.-M.; Ryoo, N.; Park, Y.H.; Kim, S. Fibrinogen Levels and Cognitive Profile Differences in Patients with Mild Cognitive Impairment. Dement. Geriatr. Cogn. Disord. 2020, 49, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Nishi, H.; Sawamoto, N.; Namiki, C.; Yoshida, H.; Thuy, D.H.D.; Ishizu, K.; Hashikawa, K.; Fukuyama, H. Correlation between Cognitive Deficits and Glucose Hypometabolism in Mild Cognitive Impairment. J. Neuroimaging 2009, 20, 29–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tampubolon, G. Repeated systemic inflammation was associated with cognitive deficits in older Britons. Alzheimer’s Dementia: Diagn. Assess. Dis. Monit. 2015, 3, 1–6. [Google Scholar] [CrossRef]
- Tsentidou, G.; Moraitou, D.; Tsolaki, M. Cognition in Vascular Aging and Mild Cognitive Impairment. J. Alzheimer’s Dis. 2019, 72, 55–70. [Google Scholar] [CrossRef] [PubMed]
- Tsentidou, G.; Moraitou, D.; Tsolaki, M. Similar Theory of Mind Deficits in Community Dwelling Older Adults with Vascular Risk Profile and Patients with Mild Cognitive Impairment: The Case of Paradoxical Sarcasm Comprehension. Brain Sci. 2021, 11, 627. [Google Scholar] [CrossRef]
- Petersen, R.C.; Caracciolo, B.; Brayne, C.; Gauthier, S.; Jelic, V.; Fratiglioni, L. Mild cognitive impairment: A concept in evolution. J. Intern. Med. 2014, 275, 214–228. [Google Scholar] [CrossRef] [Green Version]
- Zhuang, L.; Yang, Y.; Gao, J. Cognitive assessment tools for mild cognitive impairment screening. J. Neurol. 2019, 268, 1615–1622. [Google Scholar] [CrossRef]
- Kirova, A.-M.; Bays, R.B.; Lagalwar, S. Working Memory and Executive Function Decline across Normal Aging, Mild Cognitive Impairment, and Alzheimer’s Disease. BioMed Res. Int. 2015, 2015, 748212. [Google Scholar] [CrossRef] [Green Version]
- Winblad, B.; Palmer, K.; Kivipelto, M.; Jelic, V.; Fratiglioni, L.; Wahlund, L.-O.; Nordberg, A.; Backman, L.J.; Albert, M.S.; Almkvist, O.; et al. Mild cognitive impairment—Beyond controversies, towards a consensus: Report of the International Working Group on Mild Cognitive Impairment. J. Intern. Med. 2004, 256, 240–246. [Google Scholar] [CrossRef]
- Dubois, B.; Feldman, H.H.; Jacova, C.; DeKosky, S.T.; Barberger-Gateau, P.; Cummings, J.L.; Delacourte, A.; Galasko, D.; Gauthier, S.; Jicha, G.A.; et al. Research Criteria for the Diagnosis of Alzheimer’s Disease: Revising the NINCDS–ADRDA Criteria. Lancet Neurol. 2007, 6, 734–746. [Google Scholar] [CrossRef] [PubMed]
- Attems, J.; Jellinger, K.A. Olfactory tau pathology in Alzheimer disease and mild cognitive impairment. Clin. Neuropathol. 2006, 25, 265. [Google Scholar] [PubMed]
- Mitchell, T.W.; Mufson, E.J.; Schneider, J.A. Parahippocampal tau pathology in healthy aging, mild cognitive impairment, and early Alzheimer’s disease. Ann. Neurol. 2002, 51, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Cl´ement, F.; Gauthier, S.; Belleville, S. Executive functions in mild cognitive impairment: Emergence and breakdown of neural plasticity. Cortex 2013, 49, 1268–1279. [Google Scholar] [CrossRef] [PubMed]
- Kochan, N.; Breakspear, M.; Slavin, M.; Valenzuela, M.; McCraw, S.; Brodaty, H.; Sachdev, P. Functional Alterations in Brain Activation and Deactivation in Mild Cognitive Impairment in Response to a Graded Working Memory Challenge. Dement. Geriatr. Cogn. Disord. 2010, 30, 553–568. [Google Scholar] [CrossRef] [PubMed]
- Saunders, N.L.J.; Summers, M.J. Longitudinal deficits to attention, executive, and working memory in subtypes of mild cognitive impairment. Neuropsychology 2011, 25, 237–248. [Google Scholar] [CrossRef]
- Storandt, M.; Grant, E.A.; Miller, J.P.; Morris, J.C. Longitudinal course and neuropathologic outcomes in original vs revised MCI and in pre-MCI. Neurology 2006, 67, 467–473. [Google Scholar] [CrossRef]
- Summers, M.J.; Saunders, N.L.J. Neuropsychological measures predict decline to alzheimer’s dementia from mild cognitive impairment. Neuropsychology 2012, 26, 498–508. [Google Scholar] [CrossRef]
- Junquera, A.; García-Zamora, E.; Olazarán, J.; Parra, M.A.; Fernández-Guinea, S. Role of Executive Functions in the Conversion from Mild Cognitive Impairment to Dementia. J. Alzheimer’s Dis. 2020, 77, 641–653. [Google Scholar] [CrossRef]
- Mez, J.; Cosentino, S.; Brickman, A.M.; Huey, E.D.; Manly, J.J.; Mayeux, R. Faster Cognitive and Functional Decline in Dysexecutive versus Amnestic Alzheimer’s Subgroups: A Longitudinal Analysis of the National Alzheimer’s Coordinating Center (NACC) Database. PLoS ONE 2013, 8, e65246. [Google Scholar] [CrossRef]
- Brandt, J.; Aretouli, E.; Neijstrom, E.; Samek, J.; Manning, K.; Albert, M.S.; Bandeen-Roche, K. Selectivity of executive function deficits in mild cognitive impairment. Neuropsychology 2009, 23, 607–618. [Google Scholar] [CrossRef] [Green Version]
- Klekociuk, S.; Summers, J.J.; Vickers, J. Reducing false positive diagnoses in mild cognitive impairment: The importance of comprehensive neuropsychological assessment. Eur. J. Neurol. 2014, 21, 1330-e83. [Google Scholar] [CrossRef]
- Chatzikostopoulos, A.; Moraitou, D.; Tsolaki, M.; Masoura, E.; Papantoniou, G.; Sofologi, M.; Papaliagkas, V.; Kougioumtzis, G.; Papatzikis, E. Episodic Memory in Amnestic Mild Cognitive Impairment (aMCI) and Alzheimer’s Disease Dementia (ADD): Using the “Doors and People” Tool to Differentiate between Early aMCI—Late aMCI—Mild ADD Diagnostic Groups. Diagnostics 2022, 12, 1768. [Google Scholar] [CrossRef]
- Mansbach, W.E.; Mace, R.A. Predicting Functional Dependence in Mild Cognitive Impairment: Differential Contributions of Memory and Executive Functions. Gerontologist 2019, 59, 925–935. [Google Scholar] [CrossRef]
- Piccininni, C.; Quaranta, D.; Gainotti, G.; Lacidogna, G.; Guglielmi, V.; Giovannini, S.; Marra, C. The Destiny of Multiple Domain Amnesic Mild Cognitive Impairment: Effect of Alternative Neuropsychological Definitions and Their Adjunctive Role in Respect of Memory Impairment. Arch. Clin. Neuropsychol. 2021, 36, 702–710. [Google Scholar] [CrossRef]
- Chino, B.; Cuesta, P.; Pacios, J.; de Frutos-Lucas, J.; Torres-Simón, L.; Doval, S.; Marcos, A.; Bruña, R.; Maestú, F. Episodic memory dysfunction and hypersynchrony in brain functional networks in cognitively intact subjects and MCI: A study of 379 individuals. GeroScience 2022, 1–13. [Google Scholar] [CrossRef]
- Moradi, E.; Hallikainen, I.; Hänninen, T.; Tohka, J. Alzheimer’s Disease Neuroimaging Initiative. Rey’s Auditory Verbal Learning Test scores can be predicted from whole brain MRI in Alzheimer’s disease. NeuroImage Clin. 2016, 13, 415–427. [Google Scholar] [CrossRef]
- Russo, M.J.; Campos, J.; Vázquez, S.; Sevlever, G.; Allegri, R.F.; Weiner, M.W.; Aisen, P.; Petersen, R.; Weiner, M.; Jack, C.R., Jr.; et al. Adding Recognition Discriminability Index to the Delayed Recall Is Useful to Predict Conversion from Mild Cognitive Impairment to Alzheimer’s Disease in the Alzheimer’s Disease Neuroimaging Initiative. Front. Aging Neurosci. 2017, 9, 46. [Google Scholar] [CrossRef] [Green Version]
- Ihara, R.; Iwata, A.; Suzuki, K.; Ikeuchi, T.; Kuwano, R.; Iwatsubo, T.; Japanese Alzheimer’s Disease Neuroimaging Initiative. Clinical and cognitive characteristics of preclinical Alzheimer’s disease in the Japanese Alzheimer’s Disease Neuroimaging Initiative cohort. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2018, 4, 645–651. [Google Scholar] [CrossRef]
- Souto, J.J.; Silva, G.M.; Almeida, N.L.; Shoshina, I.I.; Santos, N.A.; Fernandes, T.P. Age-related episodic memory decline and the role of amyloid-β: A systematic review. Dement. Neuropsychol. 2021, 15, 299–313. [Google Scholar] [CrossRef]
- Moutoussamy, I.; Taconnat, L.; Pothier, K.; Toussaint, L.; Fay, S. Episodic memory and aging: Benefits of physical activity depend on the executive resources required for the task. PLoS ONE 2022, 17, e0263919. [Google Scholar] [CrossRef] [PubMed]
- Baddeley, A.; Eysenck, M.; Anderson, M.C. Memory; Psychology Press: New York, NY, USA, 2015. [Google Scholar]
- Schneider-Garces, N.J.; Gordon, B.A.; Brumback-Peltz, C.R.; Shin, E.; Lee, Y.; Sutton, B.P.; Maclin, E.L.; Gratton, G.; Fabiani, M. Span, CRUNCH, and Beyond: Working Memory Capacity and the Aging Brain. J. Cogn. Neurosci. 2010, 22, 655–669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rypma, B.; D’Esposito, M. Isolating the neural mechanisms of age-related changes in human working memory. Nat. Neurosci. 2000, 3, 509–515. [Google Scholar] [CrossRef]
- Belleville, S.; Chertkow, H.; Gauthier, S. Working memory and control of attention in persons with Alzheimer’s disease and mild cognitive impairment. Neuropsychology 2007, 21, 458–469. [Google Scholar] [CrossRef]
- Bika, E.; Moraitou, D.; Masoura, E.; Kolios, G.; Papantoniou, G.; Sofologi, M.; Papaliagkas, V.; Ntritsos, G. The Association between the Binding Processes of Working Memory and Vascular Risk Profile in Adults. Brain Sci. 2021, 11, 1140. [Google Scholar] [CrossRef]
- Raz, L.; Knoefel, J.E.; Bhaskar, K. The neuropathology and cerebrovascular mechanisms of dementia. J. Cereb. Blood Flow Metab. 2015, 36, 172–186. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, H.I.; Visser, P.J.; Van Boxtel, M.P.; Frisoni, G.B.; Tsolaki, M.; Papapostolou, P.; Nobili, F.; Wahlund, L.-O.; Minthon, L.; Frölich, L.; et al. The association between white matter hyperintensities and executive decline in mild cognitive impairment is network dependent. Neurobiol. Aging 2012, 33, 201.e1–201.e8. [Google Scholar] [CrossRef]
- Peltsch, A.; Hemraj, A.; Garcia, A.; Munoz, D.P. Saccade deficits in amnestic mild cognitive impairment resemble mild Alzheimer’s disease. Eur. J. Neurosci. 2014, 39, 2000–2013. [Google Scholar] [CrossRef]
- Pereira, M.L.G.D.F.; Camargo, M.V.Z.D.A.; Aprahamian, I.; Forlenza, O.V. Eye movement analysis and cognitive processing: Detecting indicators of conversion to Alzheimer’s disease. Neuropsychiatr. Dis. Treat. 2014, 10, 1273–1285. [Google Scholar] [CrossRef] [Green Version]
- Kling, M.A.; Trojanowski, J.Q.; Wolk, D.A.; Lee, V.M.; Arnold, S.E. Vascular disease and dementias: Paradigm shifts to drive research in new directions. Alzheimer’s Dement. 2012, 9, 76–92. [Google Scholar] [CrossRef]
- Pantsiou, K.; Sfakianaki, O.; Papaliagkas, V.; Savvoulidou, D.; Costa, V.; Papantoniou, G.; Moraitou, D. Inhibitory Control, Task/Rule Switching, and Cognitive Planning in Vascular Dementia: Are There Any Differences From Vascular Aging? Front. Aging Neurosci. 2018, 10, 330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kessels, R.P.C.; Elferink, M.W.; van Tilborg, I. Social cognition and social functioning in patients with amnestic mild cognitive impairment or Alzheimer’s dementia. J. Neuropsychol. 2020, 15, 186–203. [Google Scholar] [CrossRef] [PubMed]
- Tsentidou, G.; Moraitou, D.; Tsolaki, M. Emotion Recognition in a Health Continuum: Comparison of Healthy Adults of Advancing Age, Community Dwelling Adults Bearing Vascular Risk Factors and People Diagnosed with Mild Cognitive Impairment. Int. J. Environ. Res. Public Health 2022, 19, 13366. [Google Scholar] [CrossRef] [PubMed]
- Elamin, M.; Pender, N.; Hardiman, O.; Abrahams, S. Social cognition in neurodegenerative disorders: A systematic review. J. Neurol. Neurosurg. Psychiatry 2012, 83, 1071–1079. [Google Scholar] [CrossRef]
- Fernandez-Duque, D.; Black, S.E. Impaired recognition of negative facial emotions in patients with frontotemporal dementia. Neuropsychologia 2005, 43, 1673–1687. [Google Scholar] [CrossRef]
- Richard-Mornas, A.; Borg, C.; Klein-Koerkamp, Y.; Paignon, A.; Hot, P.; Thomas-Antérion, C. Perceived Eye Region and the Processing of Fearful Expressions in Mild Cognitive Impairment Patients. Dement. Geriatr. Cogn. Disord. 2012, 33, 43–49. [Google Scholar] [CrossRef]
- Hayashi, S.; Terada, S.; Takenoshita, S.; Kawano, Y.; Yabe, M.; Imai, N.; Horiuchi, M.; Miki, T.; Yokota, O.; Yamada, N. Facial expression recognition in mild cognitive impairment and dementia: Is the preservation of happiness recognition hypothesis true? Psychogeriatrics 2020, 21, 54–61. [Google Scholar] [CrossRef]
- Gkinopoulos, T.; Moraitou, D.; Papantoniou, G.; Nigritinou, M.; Ginos, P.; Kotselidou, D. Decoding of Basic Emotions from Dynamic Visual Displays in Dementia: A Sign of Loss of Positivity Bias in Emotional Processing in Cognitively Unhealthy Aging? Open J. Med. Psychol. 2014, 3, 325–336. [Google Scholar] [CrossRef] [Green Version]
- Cavallini, E.; Lecce, S.; Bottiroli, S.; Palladino, P.; Pagnin, A. Beyond False Belief: Theory of Mind in Young, Young-Old, and Old-Old Adults. Int. J. Aging Hum. Dev. 2013, 76, 181–198. [Google Scholar] [CrossRef]
- Pearlman-Avnion, S.; Lazar, J.N.; Muschinsky, T. Can Older People See Something Apart from Themselves? Int. J. Soc. Sci. Humanit. 2016, 6, 589–593. [Google Scholar] [CrossRef]
- Duval, C.; Piolino, P.; Bejanin, A.; Eustache, F.; Desgranges, B. Age effects on different components of theory of mind. Conscious. Cogn. 2011, 20, 627–642. [Google Scholar] [CrossRef]
- Arevalo-Rodriguez, I.; Smailagic, N.; Figuls, M.R.I.; Ciapponi, A.; Sanchez-Perez, E.; Giannakou, A.; Pedraza, O.L.; Bonfill Cosp, X.; Cullum, S. Mini-Mental State Examination (MMSE) for the detection of Alzheimer’s disease and other dementias in people with mild cognitive impairment (MCI). Cochrane Database Syst. Rev. 2015, 2015, CD010783, Update in: Cochrane Database Syst. Rev. 2021, 7, CD010783. [Google Scholar]
- Di Pucchio, A.; Vanacore, N.; Marzolini, F.; Lacorte, E.; Di Fiandra, T.; Gasparini, M. Use of neuropsychological tests for the diagnosis of dementia: A survey of Italian memory clinics. BMJ Open 2018, 8, e017847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rundek, T.; Gardener, H.; Saporta, A.S.D.; Loewenstein, D.A.; Duara, R.; Wright, C.B.; Dong, C.; Levin, B.; Elkind, M.S.; Sacco, R.L. Global Vascular Risk Score and CAIDE Dementia Risk Score Predict Cognitive Function in the Northern Manhattan Study. J. Alzheimer’s Dis. 2020, 73, 1221–1231. [Google Scholar] [CrossRef]
- Hannan, M.; Collins, E.G.; Phillips, S.A.; Quinn, L.; Steffen, A.; Bronas, U.G. Cognitive and vascular function in older adults with and without CKD. Aging Clin. Exp. Res. 2020, 33, 1885–1894. [Google Scholar] [CrossRef] [PubMed]
- Koch, G.; Belli, L.; Giudice, T.; Lorenzo, F.; Sancesario, G.; Sorge, R.; Bernardini, S.; Martorana, A. Frailty Among Alzheimer’s Disease Patients. CNS Neurol. Disord. Drug Targets 2013, 12, 507–511. [Google Scholar] [CrossRef]
- Xue, Q.-L. The Frailty Syndrome: Definition and Natural History. Clin. Geriatr. Med. 2011, 27, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Yesavage, J.A.; Brink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 1983, 17, 37–49. [Google Scholar] [CrossRef]
- Fountoulakis, K.N.; Tsolaki, M.; Iacovides, A.; Yesavage, J.; O’Hara, R.; Kazis, A.; Ierodiakonou, C. The validation of the short form of the Geriatric Depression Scale (GDS) in Greece. Aging Clin. Exp. Res. 1999, 11, 367–372. [Google Scholar] [CrossRef]
- Goodglass, H.; Kaplan, E. The Assessment of Aphasia and Related Disorders; Lea and Febiger: Philadelphia, PA, USA, 1983. [Google Scholar]
- Tsolaki, M.; Gkioka, M.; Verykouki, E.; Galoutzi, N.; Kavalou, E.; Pattakou-Parasyri, V. Prevalence of Dementia, Depression, and Mild Cognitive Impairment in a Rural Area of the Island of Crete, Greece. Am. J. Alzheimer’s Dis. Other Dement. 2017, 32, 252–264. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool For Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Poptsi, E.; Moraitou, D.; Eleftheriou, M.; Kounti-Zafeiropoulou, F.; Papasozomenou, C.; Agogiatou, C.; Bakoglidou, E.; Batsila, G.; Liapi, D.; Markou, N.; et al. Normative data for the Montreal Cognitive Assessment in Greek older adults with subjective cognitive decline, mild cognitive impairment and dementia. J. Geriatr. Psychiatry Neurol. 2019, 32, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Reitan, M. Validity of the Trail Making Test as an indicator of organic brain damage. Percept. Mot. Ski. 1958, 8, 271–276. [Google Scholar] [CrossRef]
- Vlachou, E.; Kosmides, M.E. The Greek Visual-Cognitive Tracking Test: Preliminary norms for clinical and research practice. Psychologia 2002, 9, 336–352. (In Greek) [Google Scholar]
- Delis, C.; Kaplan, E.; Kramer, H. Delis-Kaplan Executive Function System (D-KEFS); The Psychological Corporation: San Antonio, TX, USA, 2001. [Google Scholar]
- Weschsler, D. Weschler Memory Scale (WMS III): Administration and Scoring Manual; The Psychological Corporation: San Antonio, TX, USA, 1997. [Google Scholar]
- Wechler, D.; Stogiannidou, A. WAIS-IVGR Administrassion and Scoring 2014; Motivo: Athens, Greece, 2014. [Google Scholar]
- Baddeley, A.D.; Emslie, H.; Nimmo-Smith, I. The Doors and People Test: A Test of Visual and Verbal Recall and Recognition; Thames Valley Test Company: Bury-St-Edmunds, UK, 1994. [Google Scholar]
- Arampatzi, X.; Masoura, E. Episodic Memory and the Development of Norms to the Greek Population for the Battery «Doors and People»: A Test of Visual and Verbal Recall and Recognition. Ph.D. Thesis, Department of Psychology, Aristotle University of Thessaloniki, Thessaloniki, Greece, 2012, unpublished. [Google Scholar]
- McDonald, S.; Flanagan, S.; Rollins, J.; Kinch, J. TASIT: A new clinical tool for assessing social perception after traumatic brain injury. J. Head Trauma Rehabil. 2003, 18, 219–238. [Google Scholar] [CrossRef]
- McDonald, S.; Bornhofen, C.; Shum, D.H.K.; Long, E.; Saunders, C.; Neulinger, K. Reliability and validity of The Awareness of Social Inference Test (TASIT): A clinical test of social perception. Disabil. Rehabil. 2006, 28, 1529–1542. [Google Scholar] [CrossRef]
- Moraitou, D.; Papantoniou, G.; Gkinopoulos, T.; Nigritinou, M. Older adults’ decoding of emotions: Age-related differences in interpreting dynamic emotional displays and the well-preserved ability to recognize happiness. Psychogeriatrics 2013, 13, 139–147. [Google Scholar] [CrossRef] [Green Version]
- IBM Corp. IBM SPSS Statistics for Windows, Version 24.0; IBM Corp: Armonk, NY, USA, 2016. [Google Scholar]
- Kuang, Y.; Wu, Z.; Xia, R.; Li, X.; Liu, J.; Dai, Y.; Wang, D.; Chen, S. Phase Lag Index of Resting-State EEG for Identification of Mild Cognitive Impairment Patients with Type 2 Diabetes. Brain Sci. 2022, 12, 1399. [Google Scholar] [CrossRef]
- Michailidis, M.; Moraitou, D.; Tata, D.A.; Kalinderi, K.; Papamitsou, T.; Papaliagkas, V. Alzheimer’s Disease as Type 3 Diabetes: Common Pathophysiological Mechanisms between Alzheimer’s Disease and Type 2 Diabetes. Int. J. Mol. Sci. 2022, 23, 2687. [Google Scholar] [CrossRef]
- Yang, T.; Sun, Y.; Lu, Z.; Leak, R.K.; Zhang, F. The impact of cerebrovascular aging on vascular cognitive impairment and dementia. Ageing Res. Rev. 2017, 34, 15–29. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.-A.; Gao, M.; Chen, B.; Shi, L.; Wang, Q.; Yu, X.; Xuan, Z.; Gao, L.; Du, G. Evaluation of Hippocampal Injury and Cognitive Function Induced by Embolization in the Rat Brain. Anat. Rec. 2013, 296, 1207–1214. [Google Scholar] [CrossRef] [PubMed]
- Blasiman, R.N.; Was, C.A. Why is working memory performance unstable? A review of 21 factors. Eur. J. Psychol. 2018, 14, 188–231. [Google Scholar] [CrossRef] [PubMed]
- Qin, S.; Basak, C. Comparing the Effects of Two Cardiovascular Health Factors on Working Memory Capacity in Healthy Aging: Separate and Combined Effects of Arterial Elasticity and Physical Fitness. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2021, 77, 94–103. [Google Scholar] [CrossRef]
- Gayda, M.; Gremeaux, V.; Bherer, L.; Juneau, M.; Drigny, J.; Dupuy, O.; Lapierre, G.; Labelle, V.; Fortier, A.; Nigam, A. Cognitive function in patients with stable coronary heart disease: Related cerebrovascular and cardiovascular responses. PLoS ONE 2017, 12, e0183791. [Google Scholar] [CrossRef] [Green Version]
- Das, A.S.; Regenhardt, R.W.; Vernooij, M.W.; Blacker, D.; Charidimou, A.; Viswanathan, A. Asymptomatic Cerebral Small Vessel Disease: Insights from Population-Based Studies. J. Stroke 2019, 21, 121–138. [Google Scholar] [CrossRef] [PubMed]
- Michaelian, J.C.; Mowszowski, L.; Guastella, A.J.; Henry, J.D.; Duffy, S.; McCade, D.; Naismith, S.L. Theory of Mind in Mild Cognitive Impairment—Relationship with Limbic Structures and Behavioural Change. J. Int. Neuropsychol. Soc. 2019, 25, 1023–1034. [Google Scholar] [CrossRef] [PubMed]
- Martinez, M.; Multani, N.; Anor, C.J.; Misquitta, K.; Tang-Wai, D.F.; Keren, R.; Fox, S.; Lang, A.E.; Marras, C.; Tartaglia, M.C. Emotion Detection Deficits and Decreased Empathy in Patients with Alzheimer’s Disease and Parkinson’s Disease Affect Caregiver Mood and Burden. Front. Aging Neurosci. 2018, 10, 120. [Google Scholar] [CrossRef] [Green Version]
- Markesbery, W.R. Neuropathologic Alterations in Mild Cognitive Impairment: A Review. J. Alzheimer’s Dis. 2010, 19, 221–228. [Google Scholar] [CrossRef] [Green Version]
- Nazlidou, E.-I.; Moraitou, D.; Natsopoulos, D.; Papantoniou, G. Social cognition in adults: The role of cognitive control. Hell. J. Nucl. Med. 2015, 18 (Suppl. 1), 109–121. [Google Scholar]
- Rivas-Fernández, M.; Lindín, M.; Zurrón, M.; Díaz, F.; Aldrey-Vázquez, J.M.; Pías-Peleteiro, J.M.; Vázquez-Vázquez, L.; Pereiro, A.X.; Lojo-Seoane, C.; Nieto-Vieites, A.; et al. Brain Atrophy and Clinical Characterization of Adults With Mild Cognitive Impairment and Different Cerebrospinal Fluid Biomarker Profiles According to the AT(N) Research Framework of Alzheimer’s Disease. Front. Hum. Neurosci. 2022, 16, 799347. [Google Scholar] [CrossRef]
- Vogel, J.W.; Initiative, T.A.D.N.; Young, A.L.; Oxtoby, N.P.; Smith, R.; Ossenkoppele, R.; Strandberg, O.T.; La Joie, R.; Aksman, L.M.; Grothe, M.J.; et al. Four distinct trajectories of tau deposition identified in Alzheimer’s disease. Nat. Med. 2021, 27, 871–881. [Google Scholar] [CrossRef] [PubMed]
- Bayram, E.; Caldwell, J.Z.; Banks, S. Current understanding of magnetic resonance imaging biomarkers and memory in Alzheimer’s disease. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2018, 4, 395–413. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhang, X.; Zhang, J.; Liu, C.; Yuan, Q.; Yin, X.; Wei, L.; Cui, J.; Tao, R.; Wei, P.; et al. Gray matter volume abnormalities in type 2 diabetes mellitus with and without mild cognitive impairment. Neurosci. Lett. 2014, 562, 1–6. [Google Scholar] [CrossRef]
- Groeneveld, O.N.; Berg, E.V.D.; Rutten, G.E.; Koekkoek, P.S.; Kappelle, L.J.; Biessels, G.J. Applicability of diagnostic constructs for cognitive impairment in patients with type 2 diabetes mellitus. Diabetes Res. Clin. Pract. 2018, 142, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Gocmeza, S.; Şahina, T.; Yazirb, Y.; Duruksuc, G.; Eraldemird, F.; Polatc, S.; Utkan, T. Resveratrol prevents cognitive deficits by attenuating oxidative damage and inflammation in rat model of streptozotocin diabetes induced vascular dementia. Physiol. Behav. 2019, 201, 198–207. [Google Scholar] [CrossRef] [PubMed]
- Rosenberga, J.; Lecheaa, N.; Pentanga, G.; Shaha, N. What magnetic resonance imaging reveals—A systematic review of the relationship between type II diabetes and associated brain distortions of structure and cognitive functioning. Front. Neuroendocrinol. 2019, 52, 79–112. [Google Scholar] [CrossRef]
- Kivipelto, M.; Helkala, E.-L.; Soininen, H.; Laakso, M.P.; Hänninen, T.; Hallikainen, M.; Alhainen, K.; Iivonen, S.; Mannermaa, A.; Tuomilehto, J.; et al. Apolipoprotein E ϵ4 Allele, Elevated Midlife Total Cholesterol Level, and High Midlife Systolic Blood Pressure Are Independent Risk Factors for Late-Life Alzheimer Disease. Ann. Intern. Med. 2002, 137, 149–155. [Google Scholar] [CrossRef]
- Sweeney, M.D.; Montagne, A.; Sagare, A.P.; Nation, D.A.; Schneider, L.S.; Chui, H.C.; Harrington, M.G.; Pa, J.; Law, M.; Wang, D.J.J.; et al. Vascular dysfunction—The disregarded partner of Alzheimer’s disease. Alzheimer’s Dement. 2019, 15, 158–167. [Google Scholar] [CrossRef] [Green Version]
- Rajtar-Zembaty, A.; Rajtar-Zembaty, J.; Sałakowski, A.; Starowicz-Filip, A.; Skalska, A. Executive functions and working memory in motor control: Does the type of MCI matter? Appl. Neuropsychol. Adult 2019, 27, 580–588. [Google Scholar] [CrossRef]
- Friedman, N.P.; Miyake, A. Unity and diversity of executive functions: Individual differences as a window on cognitive structure. Cortex 2017, 86, 186–204. [Google Scholar] [CrossRef] [Green Version]
- Grambaite, R.; Selnes, P.; Reinvang, I.; Aarsland, D.; Hessen, E.; Gjerstad, L.; Fladby, T. Executive Dysfunction in Mild Cognitive Impairment is Associated with Changes in Frontal and Cingulate White Matter Tracts. J. Alzheimer’s Dis. 2011, 27, 453–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aurtenetxe, S.; García-Pacios, J.; del Río, D.; López, M.E.; Pineda-Pardo, J.A.; Marcos, A.; Losada, M.L.D.; López-Frutos, J.M.; Maestú, F. Interference Impacts Working Memory in Mild Cognitive Impairment. Front. Neurosci. 2016, 10, 443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, Y.; Wang, Z.; Chen, P.; Cheng, P.; Zhao, K.; Zhang, H.; Shu, H.; Gu, L.; Gao, L.; Wang, Q.; et al. Episodic Memory–Related Imaging Features as Valuable Biomarkers for the Diagnosis of Alzheimer’s Disease: A Multicenter Study Based on Machine Learning. Biol. Psychiatry Cogn. Neurosci. Neuroimaging, 2020; epub ahead of print. [Google Scholar] [CrossRef]
- Dubois, B.; Feldman, H.H.; Jacova, C.; Hampel, H.; Molinuevo, J.L.; Blennow, K.; DeKosky, S.T.; Gauthier, S.; Selkoe, D.; Bateman, R.; et al. Advancing research diagnostic criteria for Alzheimer’s disease: The IWG-2 criteria. Lancet Neurol. 2014, 13, 614–629, Erratum in: Lancet Neurol. 2014, 13, 757. [Google Scholar] [CrossRef]
- Liang, X.; Yuan, Q.; Xue, C.; Qi, W.; Ge, H.; Yan, Z.; Chen, S.; Song, Y.; Wu, H.; Xiao, C.; et al. Convergent functional changes of the episodic memory impairment in mild cognitive impairment: An ALE meta-analysis. Front. Aging Neurosci. 2022, 14, 919859. [Google Scholar] [CrossRef] [PubMed]
- Nakhla, M.Z.; Banuelos, D.; Pagán, C.; Olvera, A.G.; Razani, J. Differences between episodic and semantic memory in predicting observation-based activities of daily living in mild cognitive impairment and Alzheimer’s disease. Appl. Neuropsychol. Adult 2021, 29, 1499–1510. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| EVALUATION 1 | EVALUATION 2 | EVALUATION 3 | ||
|---|---|---|---|---|
| MOCA | ||||
| MCI | 24.7 (SD 1.3) | 24.5 (SD 1.4) | 24.3 (SD 1.7) | |
| VRF | 26.4 (SD 1.0) | 26.1 (SD 1.0) | 25.8 (SD 1.1) | |
| TRAIL TEST B | ||||
| MCI | 88.9 (SD 16.8) | 116.3 (SD 137.9) | 102.9 (SD 22.3) | |
| VRF | 87.2 (SD 11.8) | 90.2 (SD 11.8) | 90.7 (SD 7.6) | |
| DESIGN FLUENCY 1 | ||||
| MCI | 9.6 (SD 1.8) | 9.5 (SD 1.8) | 8.1 (SD 2.1) | |
| VRF | 10.4 (SD 1.8) | 11.1 (SD 1.4) | 10.1 (SD 1.6) | |
| DESIGN FLUENCY 2 | ||||
| MCI | 10.6 (SD 1.8) | 9.0 (SD 1.9) | 8.1 (SD 1.9) | |
| VRF | 10.5 (SD 2.0) | 11.6 (SD 1.4) | 10.4 (SD 1.4) | |
| DESIGN FLUENCY 3 | ||||
| MCI | 7.7 (SD 1.7) | 6.6 (SD 1.8) | 7.8 (SD 1.9) | |
| VRF | 10.7 (SD 1.6) | 10.0 (1.4) | 9.9 (SD 1.7) | |
| SHORT-TERM MEMORY | ||||
| MCI | 4.7 (SD 0.89) | 4.3 (SD 0.86) | 4.2 (SD 0.83) | |
| VRF | 5.1 (SD 1.1) | 4.6 (1.8) | 4.4 (SD 0.81) | |
| WORKING MEMORY | ||||
| MCI | 3.4 (SD.0.50) | 3.3 (SD 0.49) | 3.5 (SD 0.50) | |
| VRF | 4.0 (SD 0.78) | 4.1 (SD 0.71) | 3.6 (SD 0.68) | |
| LONG-TERM MEMORY | ||||
| MCI | 3.2 (SD 0.71) | 3.7 (SD 0.91) | 4.0 (SD 0.70) | |
| VRF | 5.6 (SD 2.1) | 5.9 (SD 1.6) | 5.6 (SD 1.6) | |
| SINCERE EXCHANGE | ||||
| MCI | 8.5 (SD 1.8) | 8.9 (SD 1.4) | 7.0 (SD 2.1) | |
| VRF | 9.6 (SD 1.7) | 9.4 (SD 1.7) | 10 (SD 1.7) | |
| SIMPLE SARCASM | ||||
| MCI | 13.1(SD 2.0) | 11.8 (SD 1.6) | 11.2 (SD 2.4) | |
| VRF | 10.9 (SD 2.6) | 10.3 (SD 1.9) | 10.6 (SD 1.6) | |
| PARADOXICAL SARCASM | ||||
| MCI | 10.0 (SD 1.9) | 9.2 (SD 1.7) | 8.9 (SD1.9) | |
| VFE | 10.6 (SD 2.2) | 10.2 (SD 1.7) | 10.4 (SD 1.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsentidou, G.; Moraitou, D.; Tsolaki, M.; Masoura, E.; Papaliagkas, V. Trajectories of Cognitive Impairment in Adults Bearing Vascular Risk Factors, with or without Diagnosis of Mild Cognitive Impairment: Findings from a Longitudinal Study Assessing Executive Functions, Memory, and Social Cognition. Diagnostics 2022, 12, 3017. https://doi.org/10.3390/diagnostics12123017
Tsentidou G, Moraitou D, Tsolaki M, Masoura E, Papaliagkas V. Trajectories of Cognitive Impairment in Adults Bearing Vascular Risk Factors, with or without Diagnosis of Mild Cognitive Impairment: Findings from a Longitudinal Study Assessing Executive Functions, Memory, and Social Cognition. Diagnostics. 2022; 12(12):3017. https://doi.org/10.3390/diagnostics12123017
Chicago/Turabian StyleTsentidou, Glykeria, Despina Moraitou, Magdalini Tsolaki, Elvira Masoura, and Vasileios Papaliagkas. 2022. "Trajectories of Cognitive Impairment in Adults Bearing Vascular Risk Factors, with or without Diagnosis of Mild Cognitive Impairment: Findings from a Longitudinal Study Assessing Executive Functions, Memory, and Social Cognition" Diagnostics 12, no. 12: 3017. https://doi.org/10.3390/diagnostics12123017