
Deep Learning Approach in Image Diagnosis of Pseudomonas Keratitis

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
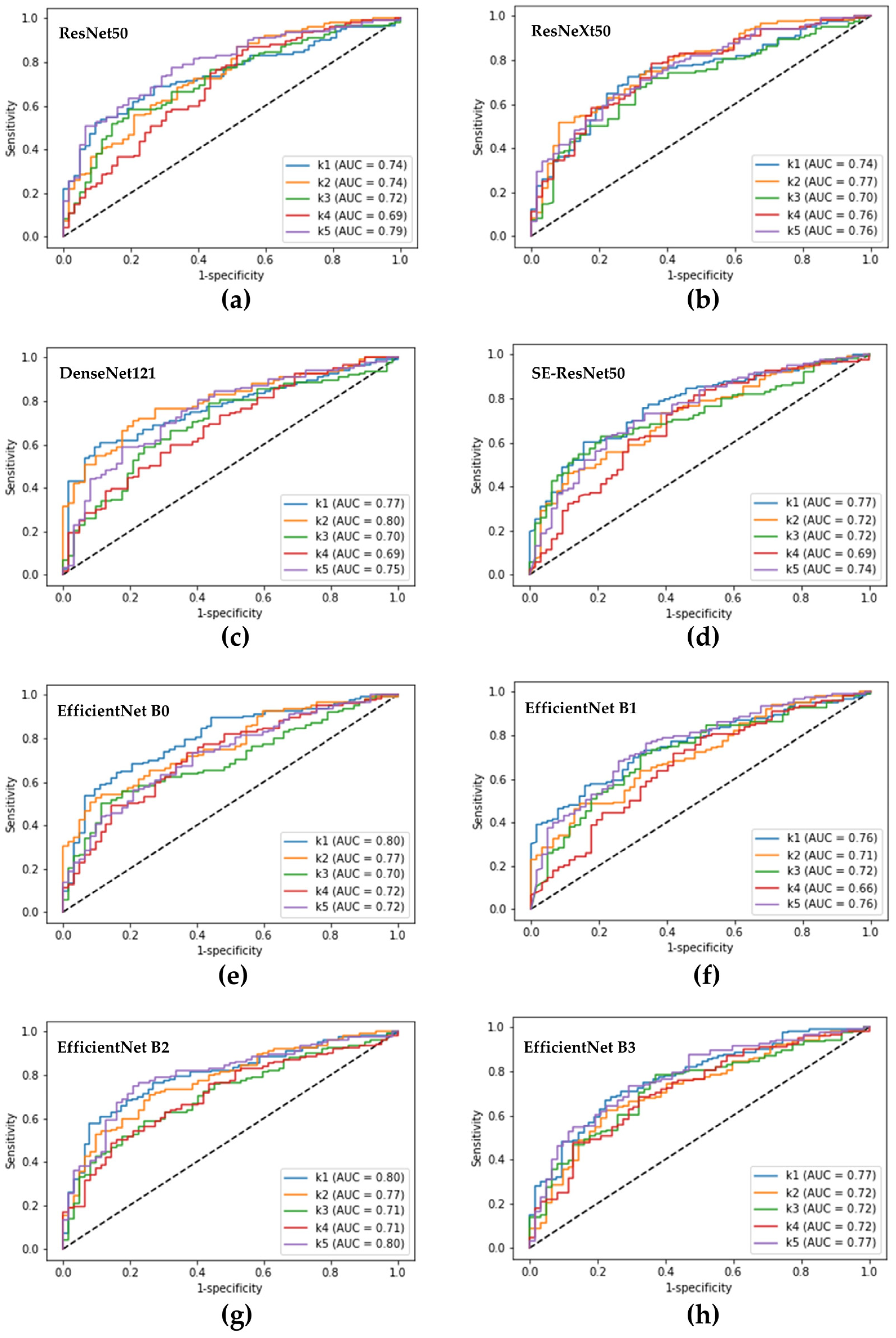
3.1. The Performance of a Single DL Model in Diagnosing Pseudomonas Keratitis
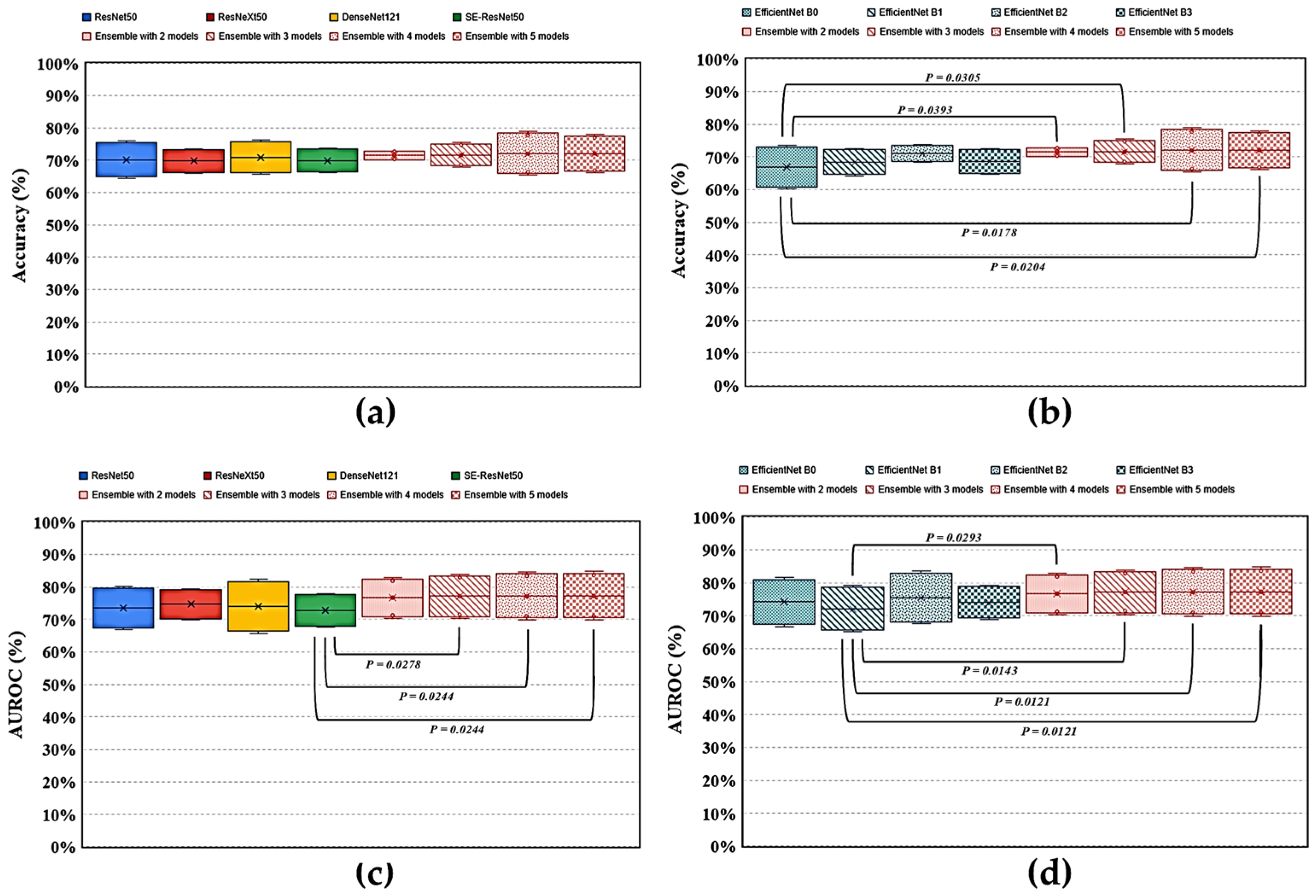
3.2. The Performance of an Ensemble Model for Recognizing Pseudomonas Keratitis
3.3. Comparing Ensemble with Single DL Models in Identifying Pseudomonas Keratitis in BK
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ung, L.; Bispo, P.J.M.; Shanbhag, S.S.; Gilmore, M.S.; Chodosh, J. The persistent dilemma of microbial keratitis: Global burden, diagnosis, and antimicrobial resistance. Surv. Ophthalmol. 2019, 64, 255–271. [Google Scholar] [CrossRef]
- Ung, L.; Chodosh, J. Foundational concepts in the biology of bacterial keratitis. Exp. Eye Res. 2021, 209, 108647. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.B.; Das, S.; Chodosh, J.; Sharma, N.; Zegans, M.E.; Kowalski, R.P.; Jhanji, V. Paradox of complex diversity: Challenges in the diagnosis and management of bacterial keratitis. Prog. Retin. Eye Res. 2021, 88, 101028. [Google Scholar] [CrossRef] [PubMed]
- Fang, P.C.; Chien, C.C.; Yu, H.J.; Ho, R.W.; Tseng, S.L.; Lai, Y.H.; Kuo, M.T. A dot hybridization assay for the diagnosis of bacterial keratitis. Mol. Vis. 2017, 23, 306–317. [Google Scholar] [PubMed]
- Hsiao, Y.T.; Fang, P.C.; Chen, J.L.; Hsu, S.L.; Chao, T.L.; Yu, H.J.; Lai, Y.H.; Huang, Y.T.; Kuo, M.T. Molecular bioburden of the lens storage case for contact lens-related keratitis. Cornea 2018, 37, 1542–1550. [Google Scholar] [CrossRef] [PubMed]
- Hilliam, Y.; Kaye, S.; Winstanley, C. Pseudomonas aeruginosa and microbial keratitis. J. Med. Microbiol. 2020, 69, 3–13. [Google Scholar] [CrossRef] [Green Version]
- Kuo, M.T.; Hsu, B.W.Y.; Yin, Y.K.; Fang, P.C.; Lai, H.Y.; Chen, A.; Yu, M.S.; Tseng, V.S. A deep learning approach in diagnosing fungal keratitis based on corneal photographs. Sci. Rep. 2020, 10, 14424. [Google Scholar] [CrossRef]
- Hung, N.; Shih, A.K.Y.; Lin, C.; Kuo, M.T.; Hwang, Y.S.; Wu, W.C.; Kuo, C.F.; Kang, E.Y.; Hsiao, C.H. Using slit-lamp images for deep learning-based identification of bacterial and fungal keratitis: Model development and validation with different convolutional neural networks. Diagnostics 2021, 11, 1246. [Google Scholar] [CrossRef]
- Ghosh, A.K.; Thammasudjarit, R.; Jongkhajornpong, P.; Attia, J.; Thakkinstian, A. Deep learning for discrimination between fungal keratitis and bacterial keratitis: DeepKeratitis. Cornea 2022, 41, 616–622. [Google Scholar] [CrossRef]
- Kuo, M.T.; Hsu, B.W.; Lin, Y.S.; Fang, P.C.; Yu, H.J.; Chen, A.; Yu, M.S.; Tseng, V.S. Comparisons of deep learning algorithms for diagnosing bacterial keratitis via external eye photographs. Sci. Rep. 2021, 11, 24227. [Google Scholar] [CrossRef]
- Ganaie, M.A.; Hu, M.; Malik, A.K.; Tanveer, M.; Suganthan, P.N. Ensemble deep learning: A review. Eng. Appl. Artif. Intell. 2022, 115, 105151. [Google Scholar] [CrossRef]
- Qummar, S.; Khan, F.G.; Shah, S.; Khan, A.; Shamshirband, S.; Rehman, Z.U.; Ahmed Khan, I.; Jadoon, W. A deep learning ensemble approach for diabetic retinopathy detection. IEEE Access 2019, 7, 150530–150539. [Google Scholar] [CrossRef]
- Cho, H.; Hwang, Y.H.; Chung, J.K.; Lee, K.B.; Park, J.S.; Kim, H.G.; Jeong, J.H. Deep learning ensemble method for classifying glaucoma stages using fundus photographs and convolutional neural networks. Curr. Eye Res. 2021, 46, 1516–1524. [Google Scholar] [CrossRef]
- Chen, C.A.; Hsu, S.L.; Hsiao, C.H.; Ma, D.H.; Sun, C.C.; Yu, H.J.; Fang, P.C.; Kuo, M.T. Comparison of fungal and bacterial keratitis between tropical and subtropical Taiwan: A prospective cohort study. Ann. Clin. Microbiol. Antimicrob. 2020, 19, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, H.; Li, L.; Wormstone, I.M.; Qiao, C.; Zhang, C.; Liu, P.; Li, S.; Wang, H.; Mou, D.; Pang, R.; et al. Development and validation of a deep learning system to detect glaucomatous optic neuropathy using fundus photographs. JAMA Ophthalmol. 2019, 137, 1353–1360. [Google Scholar] [CrossRef] [PubMed]
- Khor, W.B.; Prajna, V.N.; Garg, P.; Mehta, J.S.; Xie, L.; Liu, Z.; Padilla, M.; Joo, C.K.; Inoue, Y.; Goseyarakwong, P.; et al. The Asia Cornea Society Infectious Keratitis Study: A prospective multicenter study of infectious keratitis in Asia. Am. J. Ophthalmol. 2018, 195, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Redd, T.K.; Prajna, N.V.; Srinivasan, M.; Lalitha, P.; Krishnan, T.; Rajaraman, R.; Venugopal, A.; Acharya, N.; Seitzman, G.D.; Lietman, T.M.; et al. Image-based differentiation of bacterial and fungal keratitis using deep convolutional neural networks. Ophthalmol. Sci. 2022, 2, 100119. [Google Scholar] [CrossRef]
- Dahlgren, M.A.; Lingappan, A.; Wilhelmus, K.R. The clinical diagnosis of microbial keratitis. Am. J. Ophthalmol. 2007, 143, 940–944. [Google Scholar] [CrossRef] [Green Version]
- Xu, Y.; Kong, M.; Xie, W.; Duan, R.; Fang, Z.; Lin, Y.; Zhu, Q.; Tang, S.; Wu, F.; Yao, Y.F. Deep sequential feature learning in clinical image classification of infectious keratitis. Engineering 2021, 7, 1002–1010. [Google Scholar] [CrossRef]
- Koyama, A.; Miyazaki, D.; Nakagawa, Y.; Ayatsuka, Y.; Miyake, H.; Ehara, F.; Sasaki, S.I.; Shimizu, Y.; Inoue, Y. Determination of probability of causative pathogen in infectious keratitis using deep learning algorithm of slit-lamp images. Sci. Rep. 2021, 11, 22642. [Google Scholar] [CrossRef]
- Gulshan, V.; Peng, L.; Coram, M.; Stumpe, M.C.; Wu, D.; Narayanaswamy, A.; Venugopalan, S.; Widner, K.; Madams, T.; Cuadros, J.; et al. Development and validation of a deep learning algorithm for detection of diabetic retinopathy in retinal fundus photographs. JAMA 2016, 316, 2402–2410. [Google Scholar] [CrossRef] [PubMed]
- Tan, Z.; Simkin, S.; Lai, C.; Dai, S. Deep learning algorithm for automated diagnosis of retinopathy of prematurity plus disease. Transl. Vis. Sci. Technol. 2019, 8, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayya, V.; Kamath Shevgoor, S.; Kulkarni, U.; Hazarika, M.; Barua, P.D.; Acharya, U.R. Multi-scale convolutional neural network for accurate corneal segmentation in early detection of fungal keratitis. J. Fungi 2021, 7, 850. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Model | Diagnostic Performance (95% Confidence Interval) | ||||
|---|---|---|---|---|---|
| Sensitivity | Specificity | PPV | NPV | Accuracy | |
| ResNet50 | 80.4 | 49.9 | 76.1 | 56.4 | 70.2 |
| (73.5~87.3) | (39.0~60.7) | (71.8~80.5) | (46.6~66.1) | (64.4~75.9) | |
| ResNext50 | 81.2 | 46.9 | 75.4 | 55.8 | 69.8 |
| (74.6~87.9) | (32.2~61.7) | (70.8~79.9) | (48.1~63.5) | (65.8~73.7) | |
| DenseNet121 | 82.5 | 47.9 | 75.9 | 57.9 | 70.9 |
| (78.5~86.6) | (37.0~58.8) | (71.7~80.1) | (49.0~66.9) | (65.7~76.1) | |
| SE-ResNet50 | 82.4 | 45.3 | 75.2 | 57.6 | 70.0 |
| (68.7~96.1) | (20.54~70.1) | (70.0~80.5) | (47.9~67.4) | (66.2~73.7) | |
| EfficientNet B0 | 66.5 | 67.9 | 80.4 | 50.8 | 67.0 |
| (55.7~77.4) | (62.2~73.5) | (77.6~83.2) | (42.4~59.2) | (60.3~73.6) | |
| EfficientNet B1 | 74.6 | 56.3 | 77.3 | 53.2 | 68.5 |
| (64.4~84.8) | (47.0~65.6) | (75.3~79.2) | (46.4~59.9) | (64.3~72.6) | |
| EfficientNet B2 | 81.1 | 51.5 | 76.9 | 57.9 | 71.2 |
| (76.3~85.8) | (47.1~55.8) | (75.4~78.3) | (52.6~63.2) | (68.5~73.8) | |
| EfficientNet B3 | 68.8 | 68.2 | 81.1 | 52.5 | 68.6 |
| (62.0~75.5) | (65.0~71.3) | (79.8~82.4) | (47.2~57.8) | (64.6~72.5) | |
| Model | Diagnostic Performance (95% Confidence Interval) | ||||
|---|---|---|---|---|---|
| Sensitivity | Specificity | PPV | NPV | Accuracy | |
| BE2 | 83.3 | 47.9 | 76.1 | 59.3 | 71.5 |
| (77.7–89.0) | (36.8–59.1) | (73.2–79.1) | (55.7–62.9) | (70.0–72.9) | |
| BE3 | 83.7 | 47.9 | 76.2 | 60.1 | 71.7 |
| (76.7–90.6) | (40.3–55.5) | (73.9–78.4) | (50.0–70.2) | (68.0–75.4) | |
| BE4 | 79.6 | 57.2 | 78.7 | 59.2 | 72.1 |
| (69.0–90.3) | (48.6–65.9) | (75.4–82.0) | (47.4–70.9) | (65.4–78.9) | |
| BE5 | 79.1 | 57.9 | 78.9 | 58.6 | 72.0 |
| (70.6–87.7) | (47.5–68.3) | (74.9–82.9) | (48.5–68.6) | (66.1–78.0) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuo, M.-T.; Hsu, B.W.-Y.; Lin, Y.S.; Fang, P.-C.; Yu, H.-J.; Hsiao, Y.-T.; Tseng, V.S. Deep Learning Approach in Image Diagnosis of Pseudomonas Keratitis. Diagnostics 2022, 12, 2948. https://doi.org/10.3390/diagnostics12122948
Kuo M-T, Hsu BW-Y, Lin YS, Fang P-C, Yu H-J, Hsiao Y-T, Tseng VS. Deep Learning Approach in Image Diagnosis of Pseudomonas Keratitis. Diagnostics. 2022; 12(12):2948. https://doi.org/10.3390/diagnostics12122948
Chicago/Turabian StyleKuo, Ming-Tse, Benny Wei-Yun Hsu, Yi Sheng Lin, Po-Chiung Fang, Hun-Ju Yu, Yu-Ting Hsiao, and Vincent S. Tseng. 2022. "Deep Learning Approach in Image Diagnosis of Pseudomonas Keratitis" Diagnostics 12, no. 12: 2948. https://doi.org/10.3390/diagnostics12122948