
Investigation of Neutrophil Extracellular Traps as Potential Mediators in the Pathogenesis of Non-Acute Subdural Hematomas: A Pilot Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Criteria
2.2. Clinical Data
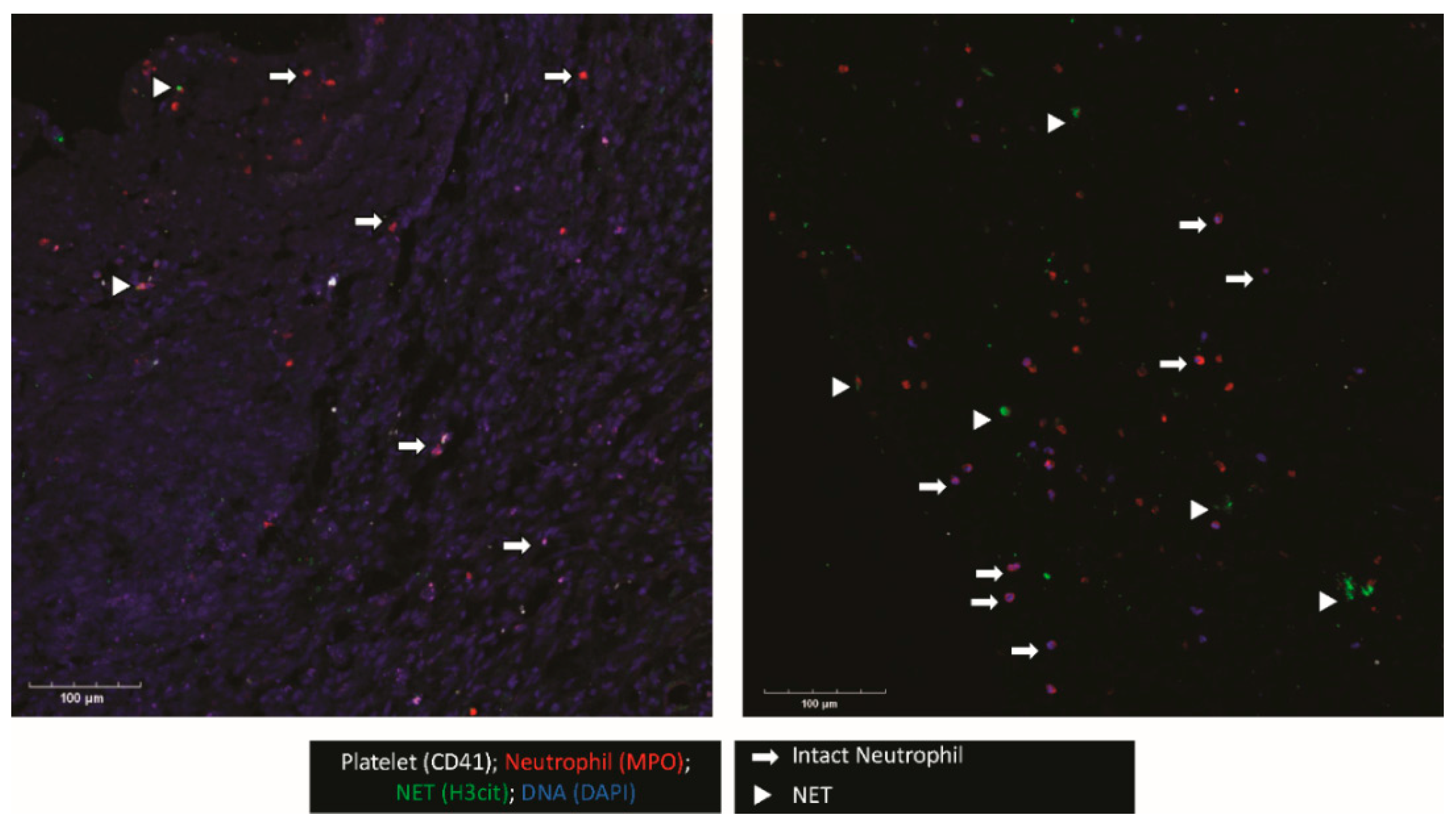
2.3. Membrane Staining
2.4. NASH Sample Collection
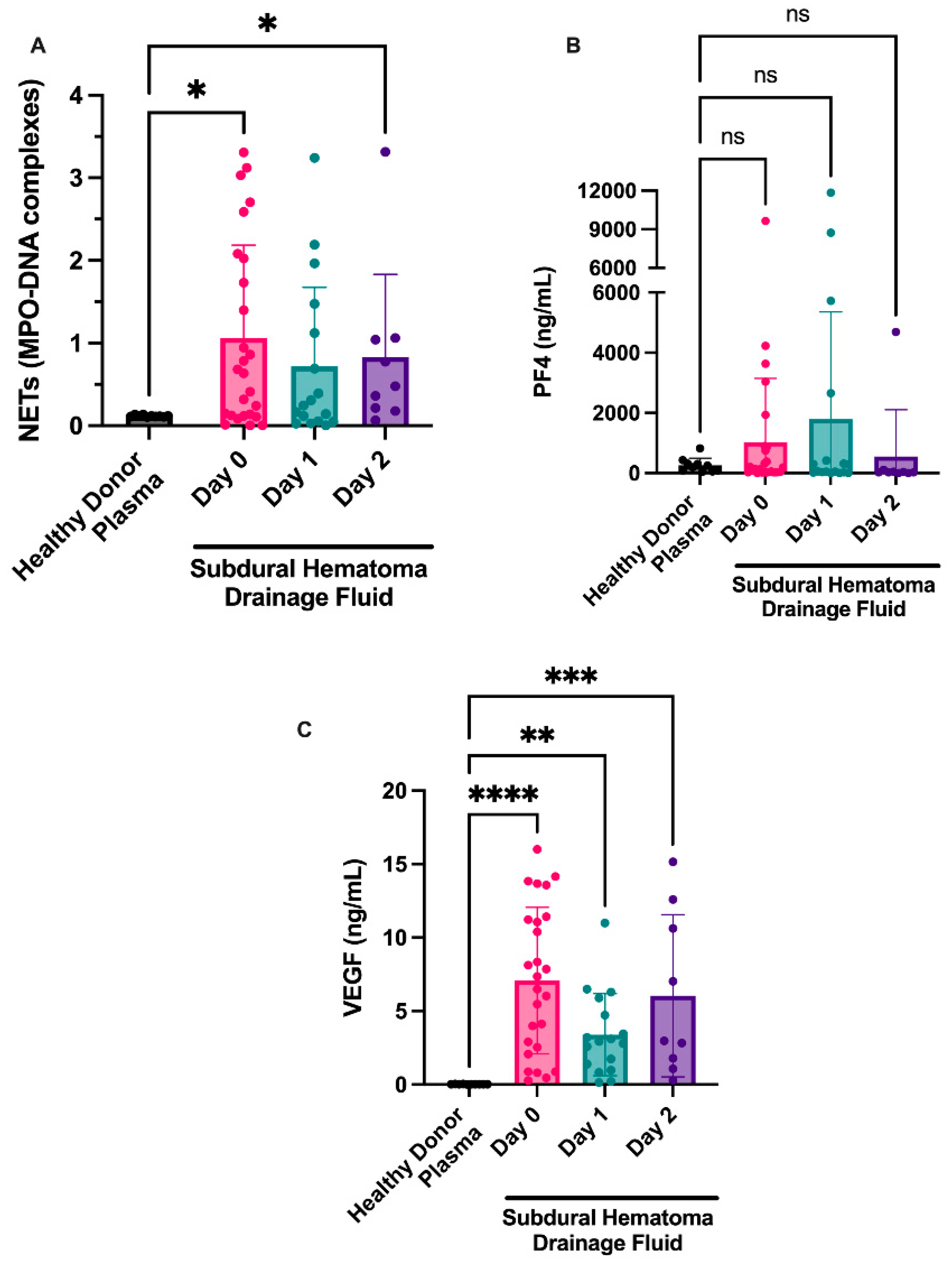
2.5. MPO-DNA Complexes
2.6. Platelet Factor 4 and VEGF ELISAs
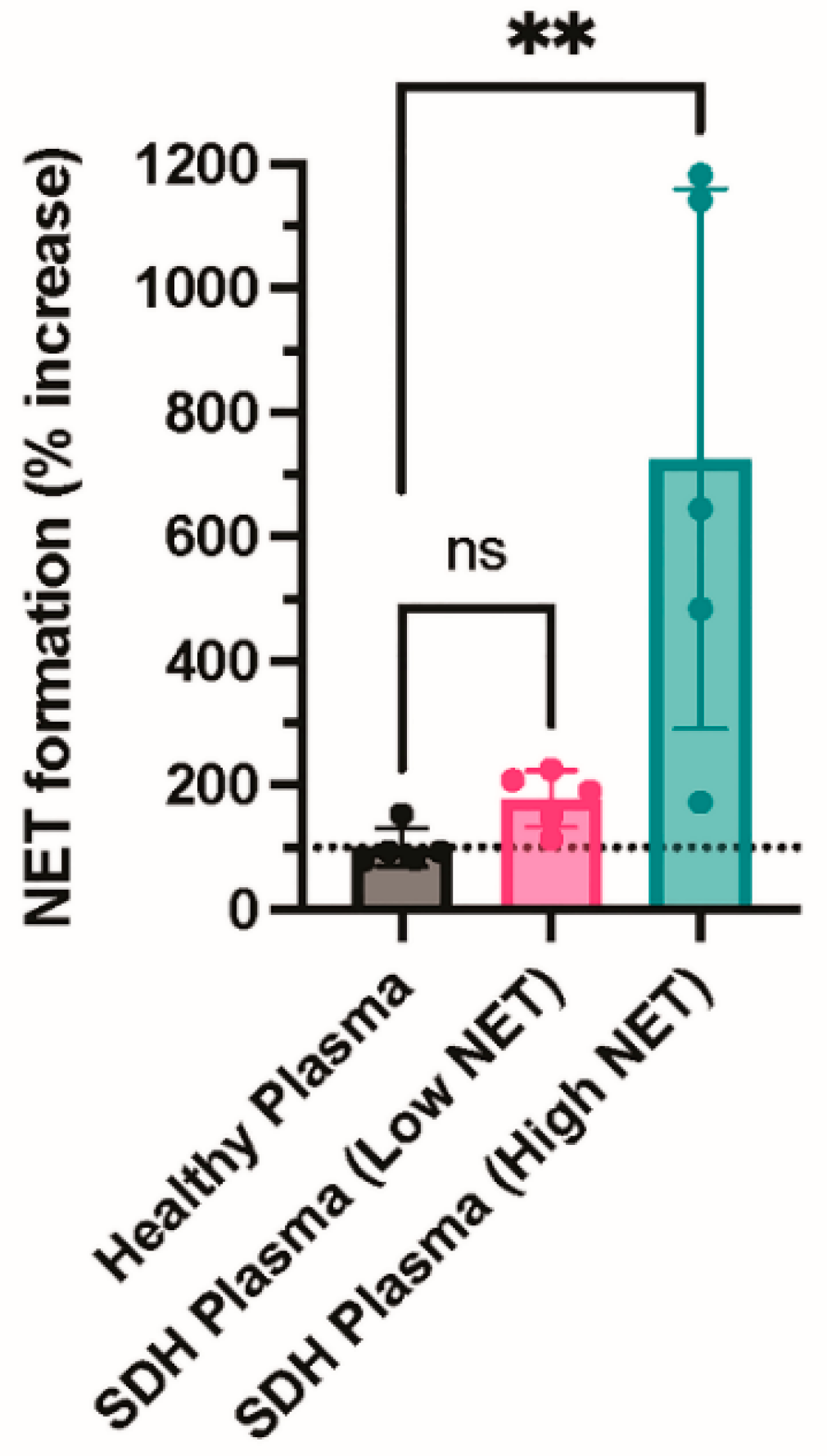
2.7. In Vitro NET Formation Using NASH Samples
2.8. Statistical Analysis
3. Results
3.1. Clinical Data
3.2. NETs Are Present in Membranes from NASHs
3.3. Markers of NET Formation Are Found in NASH Samples
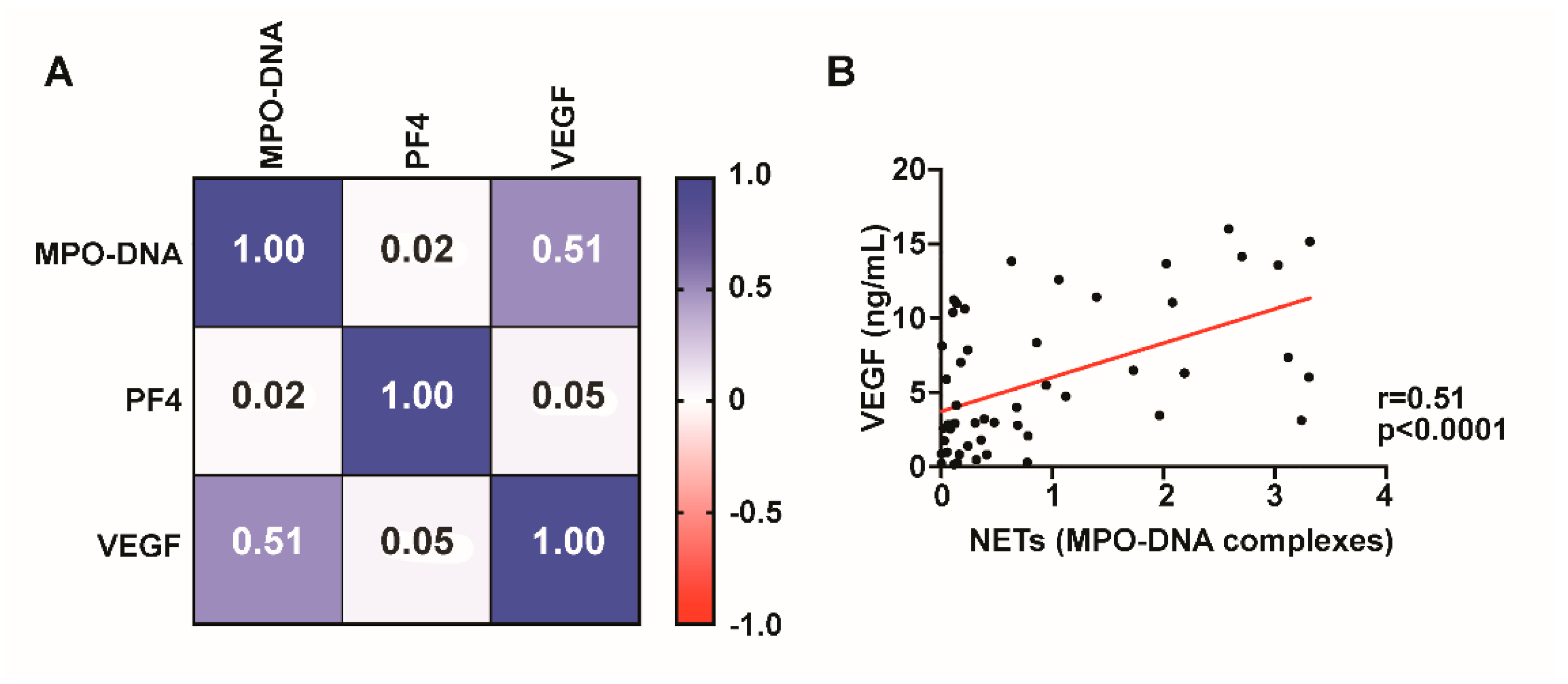
3.4. VEGF Is Present in NASHs and Correlates with NET Level
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Iantosca, M.R.; Simon, R.H. Chronic Subdural Hematoma in Adult and Elderly Patients. Neurosurg. Clin. N. Am. 2000, 11, 447–454. [Google Scholar] [CrossRef]
- Balser, D.; Farooq, S.; Mehmood, T.; Reyes, M.; Samadani, U. Actual and projected incidence rates for chronic subdural hematomas in United States Veterans Administration and civilian populations. J. Neurosurg. 2015, 123, 1209–1215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jafari, N.; Gesner, L.; Koziol, J.M.; Rotoli, G.; Hubschmann, O.R. The Pathogenesis of Chronic Subdural Hematomas: A Study on the Formation of Chronic Subdural Hematomas and Analysis of Computed Tomography Findings. World Neurosurg. 2017, 107, 376–381. [Google Scholar] [CrossRef]
- Hara, M.; Tamaki, M.; Aoyagi, M.; Ohno, K. Possible role of cyclooxygenase-2 in developing chronic subdural hematoma. J. Med. Dent. Sci. 2009, 56, 101–106. [Google Scholar]
- Markwalder, T.-M. Chronic subdural hematomas: A review. J. Neurosurg. 1981, 54, 637–645. [Google Scholar] [CrossRef]
- Pepper, M.; Ferrara, N.; Orci, L.; Montesano, R. Vascular endothelial growth factor (VEGF) induces plasminogen activators and plasminogen activator inhibitor-1 in microvascular endothelial cells. Biochem. Biophys. Res. Commun. 1991, 181, 902–906. [Google Scholar] [CrossRef] [PubMed]
- Yost, C.C.; Schwertz, H.; Cody, M.J.; Wallace, J.A.; Campbell, R.A.; Vieira-De-Abreu, A.; Araujo, C.V.; Schubert, S.; Harris, E.S.; Rowley, J.W.; et al. Neonatal NET-inhibitory factor and related peptides inhibit neutrophil extracellular trap formation. J. Clin. Investig. 2016, 126, 3783–3798. [Google Scholar] [CrossRef] [Green Version]
- Chen, G.; Zhang, D.; Fuchs, T.A.; Manwani, D.; Wagner, D.D.; Frenette, P.S. Heme-induced neutrophil extracellular traps contribute to the pathogenesis of sickle cell disease. Blood 2014, 123, 3818–3827. [Google Scholar] [CrossRef] [PubMed]
- Kessenbrock, K.; Krumbholz, M.; Schönermarck, U.; Back, W.; Gross, W.L.; Werb, Z.; Gröne, H.-J.; Brinkmann, V.; Jenne, D.E. Netting neutrophils in autoimmune small-vessel vasculitis. Nat. Med. 2009, 15, 623–625. [Google Scholar] [CrossRef]
- Fuchs, T.A.; Brill, A.; Duerschmied, D.; Schatzberg, D.; Monestier, M.; Myers, D.D., Jr.; Wrobleski, S.K.; Wakefield, T.W.; Hartwig, J.H.; Wagner, D.D. Extracellular DNA traps promote thrombosis. Proc. Natl. Acad. Sci. USA 2010, 107, 15880–15885. [Google Scholar] [CrossRef] [Green Version]
- Caudrillier, A.; Kessenbrock, K.; Gilliss, B.M.; Nguyen, J.X.; Marques, M.B.; Monestier, M.; Toy, P.; Werb, Z.; Looney, M.R. Platelets induce neutrophil extracellular traps in transfusion-related acute lung injury. J. Clin. Investig. 2012, 122, 2661–2671. [Google Scholar] [CrossRef] [PubMed]
- Kang, L.; Yu, H.; Yang, X.; Zhu, Y.; Bai, X.; Wang, R.; Cao, Y.; Xu, H.; Luo, H.; Lu, L.; et al. Neutrophil extracellular traps released by neutrophils impair revascularization and vascular remodeling after stroke. Nat. Commun. 2020, 11, 2488. [Google Scholar] [CrossRef]
- Kim, S.-W.; Lee, H.; Lee, H.-K.; Kim, I.-D.; Lee, J.-K. Neutrophil extracellular trap induced by HMGB1 exacerbates damages in the ischemic brain. Acta Neuropathol. Commun. 2019, 7, 94. [Google Scholar] [CrossRef] [Green Version]
- Laridan, E.; Denorme, F.; Desender, L.; François, O.; Andersson, T.; Deckmyn, H.; Vanhoorelbeke, K.; de Meyer, S.F. Neutrophil extracellular traps in ischemic stroke thrombi. Ann. Neurol. 2017, 82, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Manda-Handzlik, A.; Demkow, U. The Brain Entangled: The Contribution of Neutrophil Extracellular Traps to the Diseases of the Central Nervous System. Cells 2019, 8, 1477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denorme, F.; Portier, I.; Rustad, J.L.; Cody, M.J.; de Araujo, C.V.; Hoki, C.; Alexander, M.D.; Grandhi, R.; Dyer, M.R.; Neal, M.D.; et al. Neutrophil extracellular traps regulate ischemic stroke brain injury. J. Clin. Investig. 2022, 132, e154225. [Google Scholar] [CrossRef] [PubMed]
- Middleton, E.A.; He, X.-Y.; Denorme, F.; Campbell, R.A.; Ng, D.; Salvatore, S.P.; Mostyka, M.; Baxter-Stoltzfus, A.; Borczuk, A.C.; Loda, M.; et al. Neutrophil extracellular traps contribute to immunothrombosis in COVID-19 acute respiratory distress syndrome. Blood 2020, 136, 1169–1179. [Google Scholar] [CrossRef] [PubMed]
- Bounajem, M.T.; Peitz, G.; Fernandez, R.; Wang, Z.; McGinity, M.; Grandhi, R. Factors Associated With Morbidity and Retreatment After Surgical Management of Nonacute Subdural Hematomas in Elderly Patients. Cureus 2022, 14, e24779. [Google Scholar] [CrossRef] [PubMed]
- Blaauw, J.; Jacobs, B.; Hertog, H.M.D.; van der Gaag, N.A.; Jellema, K.; Dammers, R.; Lingsma, H.F.; van der Naalt, J.; Kho, K.H.; Groen, R.J.M. Neurosurgical and Perioperative Management of Chronic Subdural Hematoma. Front. Neurol. 2020, 11, 550. [Google Scholar] [CrossRef]
- Camel, M.; Grubb, R.L. Treatment of chronic subdural hematoma by twist-drill craniostomy with continuous catheter drainage. J. Neurosurg. 1986, 65, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Gelabert-González, M.; Iglesias-Pais, M.; García-Allut, A.; Martínez-Rumbo, R. Chronic subdural haematoma: Surgical treatment and outcome in 1000 cases. Clin. Neurol. Neurosurg. 2005, 107, 223–229. [Google Scholar] [CrossRef]
- Javadi, A.; Amirjamshidi, A.; Aran, S.; Hosseini, S.H. A Randomized Controlled Trial Comparing the Outcome of Burr-Hole Irrigation with and without Drainage in the Treatment of Chronic Subdural Hematoma: A Preliminary Report. World Neurosurg. 2011, 75, 731–736. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, M.; Endo, S.; Inada, K.; Kudo, A.; Kitakami, A.; Kuroda, K.; Ogawa, A. Inflammatory Cytokines Locally Elevated in Chronic Subdural Haematoma. Acta Neurochir. 1998, 140, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Weigel, R.; Schilling, L.; Schmiedek, P. Specific Pattern of Growth Factor Distribution in Chronic Subdural Hematoma (CSH): Evidence for an Angiogenic Disease. Acta Neurochir. 2001, 143, 811–819. [Google Scholar] [CrossRef] [PubMed]
- Quan, W.; Zhang, Z.; Tian, Q.; Wen, X.; Yu, P.; Wang, D.; Cui, W.; Zhou, L.; Park, E.; Baker, A.J.; et al. A rat model of chronic subdural hematoma: Insight into mechanisms of revascularization and inflammation. Brain Res. 2015, 1625, 84–96. [Google Scholar] [CrossRef] [PubMed]
- Hua, C.; Zhao, G.; Feng, Y.; Yuan, H.; Song, H.; Bie, L. Role of Matrix Metalloproteinase-2, Matrix Metalloproteinase-9, and Vascular Endothelial Growth Factor in the Development of Chronic Subdural Hematoma. J. Neurotrauma 2016, 33, 65–70. [Google Scholar] [CrossRef] [Green Version]
- Tazzyman, S.; Niaz, H.; Murdoch, C. Neutrophil-mediated tumour angiogenesis: Subversion of immune responses to promote tumour growth. Semin. Cancer Biol. 2013, 23, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Cheng, X.W.; Kuzuya, M.; Nakamura, K.; Maeda, K.; Tsuzuki, M.; Kim, W.; Sasaki, T.; Liu, Z.; Inoue, N.; Kondo, T.; et al. Mechanisms Underlying the Impairment of Ischemia-Induced Neovascularization in Matrix Metalloproteinase 2–Deficient Mice. Circ. Res. 2007, 100, 904–913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nanko, N.; Tanikawa, M.; Mase, M.; Fujita, M.; Tateyama, H.; Miyati, T.; Yamada, K. Involvement of Hypoxia-Inducible Factor-1.ALPHA. and Vascular Endothelial Growth Factor in the Mechanism of Development of Chronic Subdural Hematoma. Neurol. Medico-Chirurgica 2009, 49, 379–385. [Google Scholar] [CrossRef] [Green Version]
- Zhou, P.; Li, T.; Jin, J.; Liu, Y.; Li, B.; Sun, Q.; Tian, J.; Zhao, H.; Liu, Z.; Ma, S.; et al. Interactions between neutrophil extracellular traps and activated platelets enhance procoagulant activity in acute stroke patients with ICA occlusion. eBioMedicine 2020, 53, 102671. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Cao, Y.; Du, J.; Liu, H.; Chen, X.; Li, M.; Xiang, M.; Wang, C.; Wu, X.; Liu, L.; et al. Neutrophil extracellular traps contribute to tissue plasminogen activator resistance in acute ischemic stroke. FASEB J. 2021, 35, e21835. [Google Scholar] [CrossRef]
- Vallés, J.; Santos, M.T.; Latorre, A.M.; Tembl, J.I.; Salom, J.B.; Nieves, C.; Lago, A.; Moscardó, A. Neutrophil extracellular traps are increased in patients with acute ischemic stroke: Prognostic significance. Thromb. Haemost. 2017, 117, 1919–1929. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhou, X.; Yin, Y.; Mai, Y.; Wang, D.; Zhang, X. Hyperglycemia Induces Neutrophil Extracellular Traps Formation Through an NADPH Oxidase-Dependent Pathway in Diabetic Retinopathy. Front. Immunol. 2018, 9, 3076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Das, S.K.; Yuan, Y.F.; Li, M.Q. Specific PKC βII inhibitor: One stone two birds in the treatment of diabetic foot ulcers. Biosci. Rep. 2018, 38, BSR20171459. [Google Scholar] [CrossRef] [Green Version]
- Dekay, J.T.; Emery, I.F.; Rud, J.; Eldridge, A.; Lord, C.; Gagnon, D.J.; May, T.L.; Herrera, V.L.M.; Ruiz-Opazo, N.; Riker, R.R.; et al. DEspRhigh neutrophils are associated with critical illness in COVID-19. Sci. Rep. 2021, 11, 22463. [Google Scholar] [CrossRef]
- Bounajem, M.T.; Campbell, R.A.; Denorme, F.; Grandhi, R. Paradigms in chronic subdural hematoma pathophysiology: Current treatments and new directions. J. Trauma Acute Care Surg. 2021, 91, e134–e141. [Google Scholar] [CrossRef]
- Carmeliet, P.; Moons, L.; Luttun, A.; Vincenti, V.; Compernolle, V.; de Mol, M.; Wu, Y.; Bono, F.; Devy, L.; Beck, H.; et al. Synergism between vascular endothelial growth factor and placental growth factor contributes to angiogenesis and plasma extravasation in pathological conditions. Nat. Med. 2001, 7, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Yamashima, T.; Yamamoto, S.; Friede, R.L. The role of endothelial gap junctions in the enlargement of chronic subdural hematomas. J. Neurosurg. 1983, 59, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Pan, P.; Fu, H.; Zhang, L.; Huang, H.; Luo, F.; Wu, W.; Guo, Y.; Liu, X. Angiotensin II upregulates the expression of placental growth factor in human vascular endothelial cells and smooth muscle cells. BMC Cell Biol. 2010, 11, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagahori, T.; Nishijima, M.; Takaku, A. [Histological study of the outer membrane of chronic subdural hematoma: Possible mechanism for expansion of hematoma cavity]. No Shinkei Geka 1993, 21, 697–701. [Google Scholar] [PubMed]
- Fujisawa, H.; Ito, H.; Saito, K.; Ikeda, K.; Nitta, H.; Yamashita, J. Immunohistochemical localization of tissue-type plasminogen activator in the lining wall of chronic subdural hematoma. Surg. Neurol. 1991, 35, 441–445. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient No. | Age (Years)/Sex | GCS Score | Anticoagulation | Aspirin | Preoperative | Laterality | Recurrence Requiring Reoperation | Mortality 1 | Follow-Up (Months) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Statin | Steroid | |||||||||
| 1 | 64/F | 14 | Prophylactic heparin | No | No | No | Right | Hx prior operation | - | 2 |
| 2 | 85/M | 9 | None | Yes | Yes | No | Right | No | Leukemia | 2 |
| 3 | 66/M | 15 | None | Yes | Yes | Yes | Bilateral | No | - | 5 |
| 4 | 77/M | 13 | Warfarin | No | No | No | Left | No | - | 16 |
| 5 | 43/M | 15 | None | No | Yes | Yes | Right | No | - | 18 |
| 6 | 89/M | 15 | Apixaban | No | Yes | No | Right | No | - | 12 |
| 7 | 62/M | 14 | None | No | No | No | Right | No | Pneumatosis intestinalis | 0.5 |
| 8 | 55/F | 15 | None | No | No | No | Right | No | - | 19 |
| 9 | 91/M | 15 | None | No | No | No | Left | No | - | 18 |
| 10 | 95/F | 11 | None | No | No | No | Left | No | Urinary infection | 7 |
| 11 | 63/M | 15 | Warfarin | No | Yes | Yes | Left | No | - | 5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bounajem, M.T.; Denorme, F.; Rustad, J.L.; Campbell, R.A.; Grandhi, R. Investigation of Neutrophil Extracellular Traps as Potential Mediators in the Pathogenesis of Non-Acute Subdural Hematomas: A Pilot Study. Diagnostics 2022, 12, 2934. https://doi.org/10.3390/diagnostics12122934
Bounajem MT, Denorme F, Rustad JL, Campbell RA, Grandhi R. Investigation of Neutrophil Extracellular Traps as Potential Mediators in the Pathogenesis of Non-Acute Subdural Hematomas: A Pilot Study. Diagnostics. 2022; 12(12):2934. https://doi.org/10.3390/diagnostics12122934
Chicago/Turabian StyleBounajem, Michael T., Frederik Denorme, John L. Rustad, Robert A. Campbell, and Ramesh Grandhi. 2022. "Investigation of Neutrophil Extracellular Traps as Potential Mediators in the Pathogenesis of Non-Acute Subdural Hematomas: A Pilot Study" Diagnostics 12, no. 12: 2934. https://doi.org/10.3390/diagnostics12122934