
Pediatric Low-Grade Glioma Surgery with Sodium Fluorescein: Efficient Localization for Removal and Association with Intraoperative Pathological Sampling
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
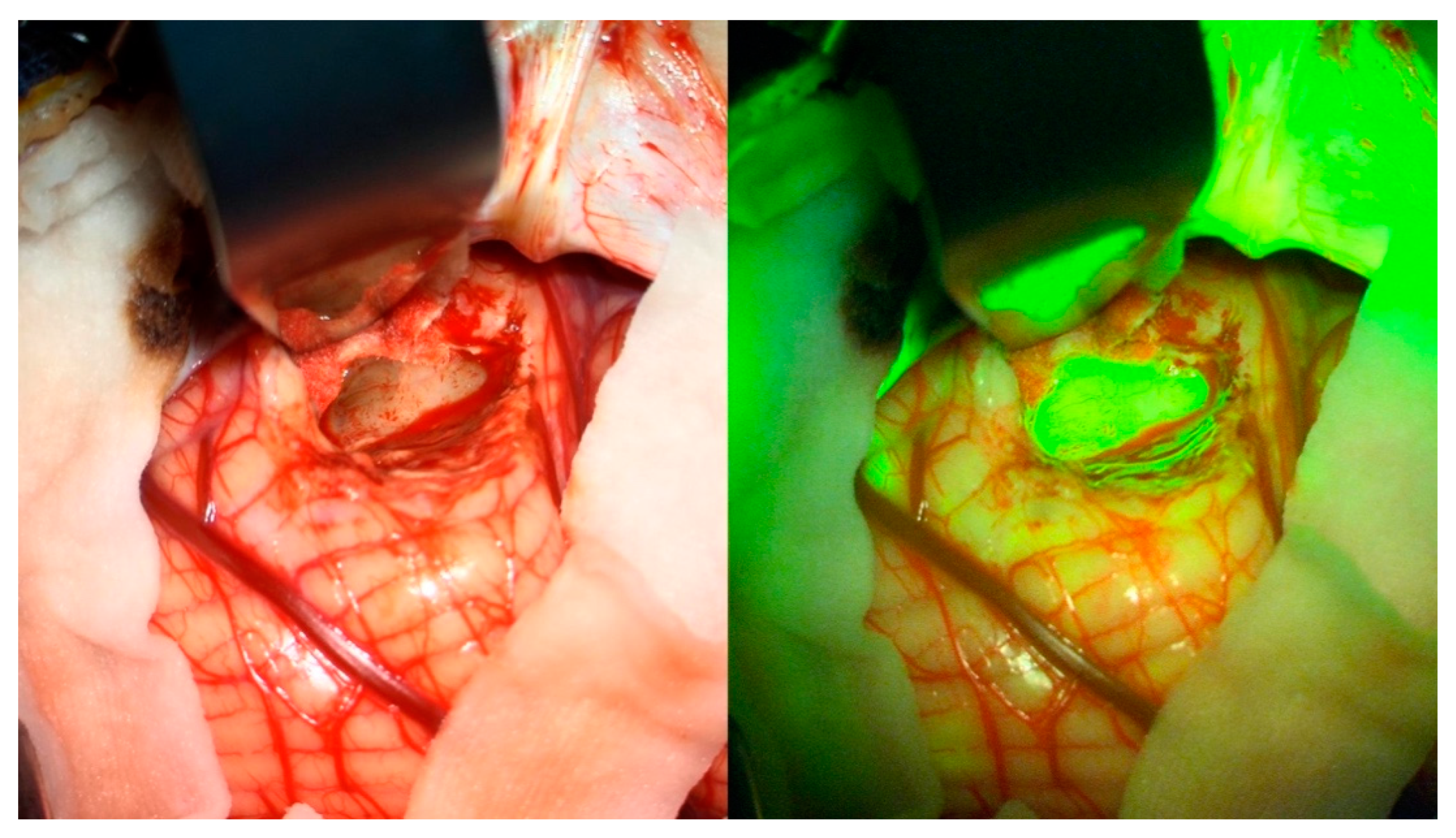
2.2. Surgical Procedure
2.3. Image Analysis
2.4. Pathological Analysis
2.5. Statistical Analysis
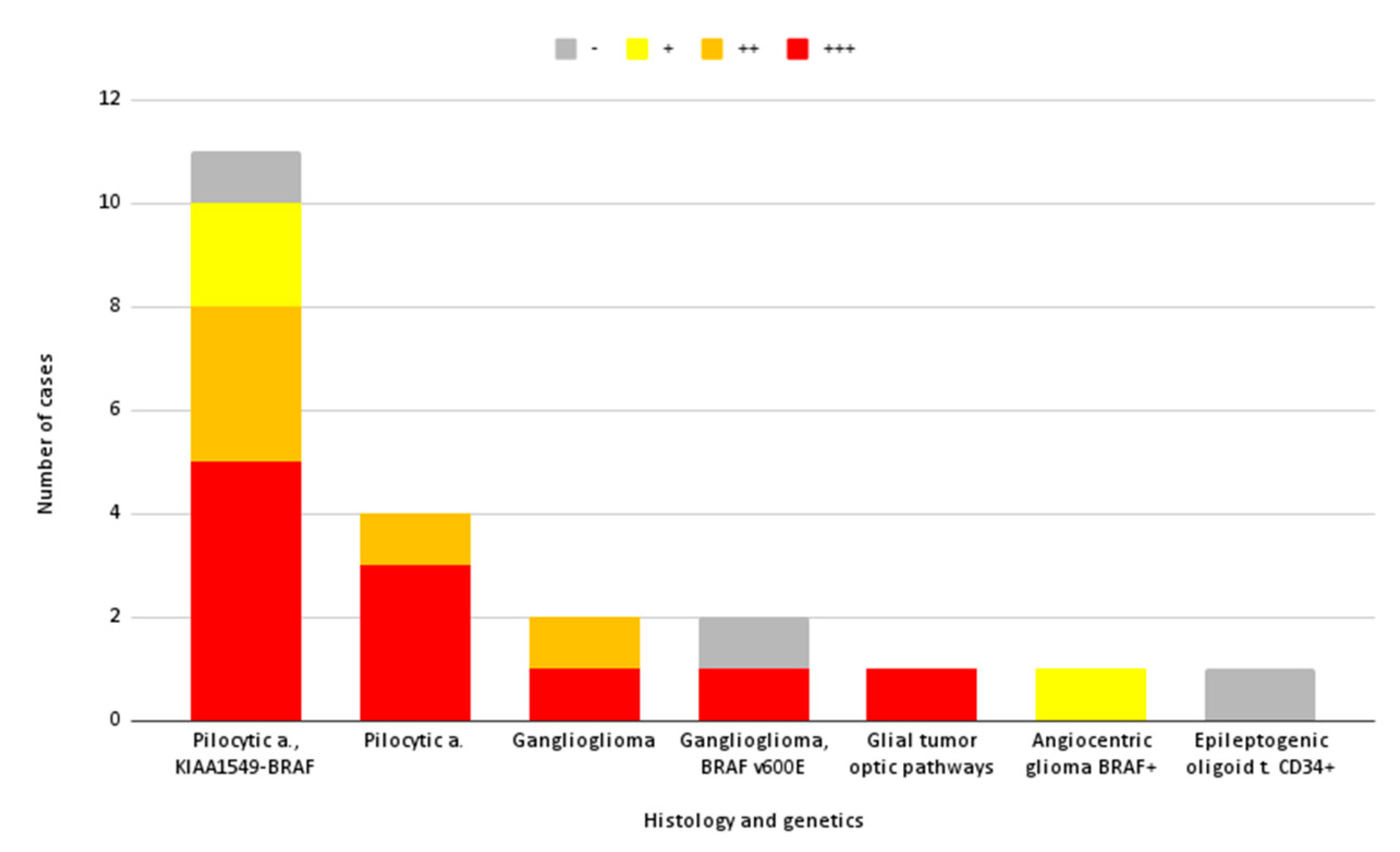
3. Results
3.1. Patient Population and Surgical Procedure
3.2. Image Analysis
3.3. Intraoperative Fluorescence Relationship with Preoperative MRI Gadolinium Enhancement Pattern and Intensity
3.4. Utility of SF in Localizing Pediatric LGGs
3.5. Extemporaneous Pathological Sampling (EPS) and SF
4. Discussion
4.1. Sodium Fluorescein in Pediatric LGG: Considerations, Feasibility, and Safety
4.2. Association between Fluorescence and Gadolinium Enhancement and Image Analysis
4.3. Utility of SF in Localizing Pediatric LGGs and Association with EPS
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bale, T.A.; Rosenblum, M.K. The 2021 WHO Classification of Tumors of the Central Nervous System: An update on pediatric low-grade gliomas and glioneuronal tumors. Brain Pathol. 2022, 32, e13060. [Google Scholar] [CrossRef] [PubMed]
- Chalil, A.; Ramaswamy, V. Low Grade Gliomas in Children. J. Child Neurol. 2016, 31, 517–522. [Google Scholar] [CrossRef] [PubMed]
- Ganz, J.C. Chapter 15—Low grade gliomas. In Progress in Brain Research; Recent Advances and Controversies in Gamma Knife Neurosurgery; Ganz, J.C., Ed.; Elsevier: Amsterdam, The Netherlands, 2022; Volume 268, pp. 271–277. [Google Scholar]
- Hong, C.S.; Ho, W.; Piazza, M.G.; Ray-Chaudhury, A.; Zhuang, Z.; Heiss, J.D. Characterization of the blood brain barrier in pediatric central nervous system neoplasms. J. Interdiscip. Histopathol. 2016, 4, 29–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sturm, D.; Pfister, S.M.; Jones, D.T.W. Pediatric Gliomas: Current Concepts on Diagnosis, Biology, and Clinical Management. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2017, 35, 2370–2377. [Google Scholar] [CrossRef] [PubMed]
- Balogun, J.A.; Rutka, J.T. Surgery of Intracranial Gliomas in Children. In Progress in Neurological Surgery; Chernov, M.F., Muragaki, Y., Kesari, S., McCutcheon, I.E., Eds.; S. Karger AG: Bazel, Switserland, 2018; Volume 30, pp. 204–217. ISBN 978-3-318-06056-0. [Google Scholar]
- Fernandez, C.; Figarella-Branger, D.; Girard, N.; Bouvier-Labit, C.; Gouvernet, J.; Paredes, A.P.; Lena, G. Pilocytic Astrocytomas in Children: Prognostic Factors—A Retrospective Study of 80 Cases. Neurosurgery 2003, 53, 544–555. [Google Scholar] [CrossRef] [PubMed]
- Lohkamp, L.-N.; Mottolese, C.; Szathmari, A.; Huguet, L.; Beuriat, P.-A.; Christofori, I.; Desmurget, M.; Di Rocco, F. Awake brain surgery in children-review of the literature and state-of-the-art. Childs Nerv. Syst. Off. J. Int. Soc. Pediatr. Neurosurg. 2019, 35, 2071–2077. [Google Scholar] [CrossRef] [PubMed]
- Lohkamp, L.-N.; Beuriat, P.-A.; Desmurget, M.; Cristofori, I.; Szathmari, A.; Huguet, L.; Di Rocco, F.; Mottolese, C. Awake brain surgery in children-a single-center experience. Childs Nerv. Syst. Off. J. Int. Soc. Pediatr. Neurosurg. 2020, 36, 967–974. [Google Scholar] [CrossRef]
- Navarro-Bonnet, J.; Suarez-Meade, P.; Brown, D.A.; Chaichana, K.L.; Quinones-Hinojosa, A. Following the light in glioma surgery: A comparison of sodium fluorescein and 5-aminolevulinic acid as surgical adjuncts in glioma resection. J. Neurosurg. Sci. 2020, 63, 633–647. [Google Scholar] [CrossRef]
- Suero Molina, E.; Schipmann, S.; Stummer, W. Maximizing safe resections: The roles of 5-aminolevulinic acid and intraoperative MR imaging in glioma surgery-review of the literature. Neurosurg. Rev. 2019, 42, 197–208. [Google Scholar] [CrossRef] [Green Version]
- Hendricks, B.K.; Sanai, N.; Stummer, W. Fluorescence-guided surgery with aminolevulinic acid for low-grade gliomas. J. Neurooncol. 2019, 141, 13–18. [Google Scholar] [CrossRef]
- Kiesel, B.; Freund, J.; Reichert, D.; Wadiura, L.; Erkkilae, M.T.; Woehrer, A.; Hervey-Jumper, S.; Berger, M.S.; Widhalm, G. 5-ALA in Suspected Low-Grade Gliomas: Current Role, Limitations, and New Approaches. Front. Oncol. 2021, 11, 699301. [Google Scholar] [CrossRef] [PubMed]
- Schwake, M.; Schipmann, S.; Müther, M.; Köchling, M.; Brentrup, A.; Stummer, W. 5-ALA fluorescence-guided surgery in pediatric brain tumors—A systematic review. Acta Neurochir. 2019, 161, 1099–1108. [Google Scholar] [CrossRef] [PubMed]
- Beez, T.; Sarikaya-Seiwert, S.; Steiger, H.-J.; Hänggi, D. Fluorescence-guided surgery with 5-aminolevulinic acid for resection of brain tumors in children—A technical report. Acta Neurochir. 2014, 156, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Preuβ, M.; Renner, C.; Krupp, W.; Christiansen, H.; Fischer, L.; Merkenschlager, A.; Kieβ, W.; Müller, W.; Manzo, N.; Meixensberger, J.; et al. The use of 5-aminolevulinic acid fluorescence guidance in resection of pediatric brain tumors. Childs Nerv. Syst. 2013, 29, 1263–1267. [Google Scholar] [CrossRef]
- Smith, E.J.; Gohil, K.; Thompson, C.M.; Naik, A.; Hassaneen, W. Fluorescein-Guided Resection of High Grade Gliomas: A Meta-Analysis. World Neurosurg. 2021, 155, 181–188.e7. [Google Scholar] [CrossRef]
- Falco, J.; Höhne, J.; Broggi, M.; Rubiu, E.; Restelli, F.; Vetrano, I.G.; Schiariti, M.; Mazzapicchi, E.; Bonomo, G.; Ferroli, P.; et al. Fluorescein-guided surgery for the resection of pilocytic astrocytomas: A multicentric retrospective study. Front. Oncol. 2022, 12, 943085. [Google Scholar] [CrossRef]
- Zhang, J.; AL-Nahari, F.; Wang, Z.; Lin, F.; Zhao, Y.; Xiao, S.; Liu, J.; Ke, C.; Chen, Z.; Jiang, Y.; et al. Application of fluorescein sodium in the resection of vermis pilocytic astrocytomas. World J. Surg. Oncol. 2017, 15, 46. [Google Scholar] [CrossRef] [Green Version]
- Höhne, J.; Acerbi, F.; Falco, J.; Akçakaya, M.O.; Schmidt, N.O.; Kiris, T.; de Laurentis, C.; Ferroli, P.; Broggi, M.; Schebesch, K.-M. Lighting Up the Tumor—Fluorescein-Guided Resection of Gangliogliomas. J. Clin. Med. 2020, 9, 2405. [Google Scholar] [CrossRef]
- Erdman, C.M.; Christie, C.; Iqbal, M.O.; Mazzola, C.A.; Tomycz, L. The utilization of sodium fluorescein in pediatric brain stem gliomas: A case report and review of the literature. Childs Nerv. Syst. 2021, 37, 1753–1758. [Google Scholar] [CrossRef]
- Minkin, K.; Naydenov, E.; Gabrovski, K.; Dimova, P.; Penkov, M.; Tanova, R.; Nachev, S.; Romanski, K. Intraoperative fluorescein staining for benign brain tumors. Clin. Neurol. Neurosurg. 2016, 149, 22–26. [Google Scholar] [CrossRef]
- Pedro, M.T.; Grübel, N.; Durner, G.; Pala, A.; Wirtz, C.R.; Koenig, R.W. Intraoperative Sodium-Fluorescence Imaging in Peripheral Nerve Sheath Tumors (PNST)—A New Additional Promising Diagnostic Tool. Front. Oncol. 2021, 11, 655392. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro-Oncol. 2021, 23, 1231–1251. [Google Scholar] [CrossRef]
- Dilek, O.; Ihsan, A.; Tulay, H. Anaphylactic reaction after fluorescein sodium administration during intracranial surgery. J. Clin. Neurosci. 2011, 18, 430–431. [Google Scholar] [CrossRef] [PubMed]
- Alkan, Z.; Cakir, B.O.; Kilinç, B.M.; Turgut, S. Grand mal seizure following intrathecal fluorescein use. Kulak Burun Bogaz Ihtis. Derg. KBB J. Ear Nose Throat 2004, 13, 80–83. [Google Scholar]
- Anari, S.; Waldron, M.; Carrie, S. Delayed absence seizure: A complication of intrathecal fluorescein injection: A case report and literature review. Auris. Nasus. Larynx 2007, 34, 515–518. [Google Scholar] [CrossRef] [PubMed]
- Park, K.-Y.; Kim, Y.B. A Case of Myelopathy after Intrathecal Injection of Fluorescein. J. Korean Neurosurg. Soc. 2007, 42, 492–494. [Google Scholar] [CrossRef]
- Göker, B.; Kırış, T. Sodium fluorescein–guided brain tumor surgery under the YELLOW-560-nm surgical microscope filter in pediatric age group: Feasibility and preliminary results. Childs Nerv. Syst. 2019, 35, 429–435. [Google Scholar] [CrossRef]
- Chen, Z.; Zhang, X.; Lin, F.; Li, C.; Jin, J.; Zhou, Z.; Zhu, S.; Cheng, Z.; Zhong, S.; He, Z.; et al. The application of fluorescein sodium for the resection of medulloblastoma. J. Neurooncol. 2022, 158, 463–470. [Google Scholar] [CrossRef]
- Falco, J.; Cavallo, C.; Vetrano, I.G.; de Laurentis, C.; Siozos, L.; Schiariti, M.; Broggi, M.; Ferroli, P.; Acerbi, F. Fluorescein Application in Cranial and Spinal Tumors Enhancing at Preoperative MRI and Operated With a Dedicated Filter on the Surgical Microscope: Preliminary Results in 279 Patients Enrolled in the FLUOCERTUM Prospective Study. Front. Surg. 2019, 6, 49. [Google Scholar] [CrossRef] [Green Version]
- Folaron, M.; Strawbridge, R.; Samkoe, K.S.; Filan, C.; Roberts, D.W.; Davis, S.C. Elucidating the kinetics of sodium fluorescein for fluorescence guided surgery of glioma. J. Neurosurg. 2018, 131, 724–734. [Google Scholar] [CrossRef] [Green Version]
- Neira, J.A.; Ung, T.H.; Sims, J.S.; Malone, H.R.; Chow, D.S.; Samanamud, J.L.; Zanazzi, G.J.; Guo, X.; Bowden, S.G.; Zhao, B.; et al. Aggressive resection at the infiltrative margins of glioblastoma facilitated by intraoperative fluorescein guidance. J. Neurosurg. 2017, 127, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Bowden, S.G.; Neira, J.A.; Gill, B.J.A.; Ung, T.H.; Englander, Z.K.; Zanazzi, G.; Chang, P.D.; Samanamud, J.; Grinband, J.; Sheth, S.A.; et al. Sodium Fluorescein Facilitates Guided Sampling of Diagnostic Tumor Tissue in Nonenhancing Gliomas. Neurosurgery 2018, 82, 719–727. [Google Scholar] [CrossRef]
- Kato, N.; Prinz, V.; Dengler, J.; Vajkoczy, P. Blood Flow Assessment of Arteriovenous Malformations Using Intraoperative Indocyanine Green Videoangiography. Stroke Res. Treat. 2019, 2019, 7292304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Della Pepa, G.M.; Ius, T.; Menna, G.; La Rocca, G.; Battistella, C.; Rapisarda, A.; Mazzucchi, E.; Pignotti, F.; Alexandre, A.; Marchese, E.; et al. “Dark corridors” in 5-ALA resection of high-grade gliomas: Combining fluorescence-guided surgery and contrast-enhanced ultrasonography to better explore the surgical field. J. Neurosurg. Sci. 2019, 63, 688–696. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Subjective | ∆ Tumor | ∆ Tumor − ∆ Healthy | ∆ Tumor − ∆ Healthy/∆ Healthy |
|---|---|---|---|
| +++, homog | 1.569 | −32.517 | −0.954 |
| +++, homog | 5.889 | −12.949 | −0.687 |
| +++, homog | 10.354 | 14.377 | −3.574 |
| +++, homog | 68.188 | 34.958 | 1.052 |
| +++, homog | 69.271 | 95.757 | −3.615 |
| +++, homog | 92.411 | 93.253 | −110.752 |
| +++, homog | 124.392 | 125.336 | −132.771 |
| +++, homog | 170.356 | 181.507 | −16.277 |
| +++, homog | 181.021 | 184.872 | −48.006 |
| +++, homog | 202.001 | 158.957 | 3.693 |
| +++, homog | 210.597 | −7.739 | −0.035 |
| ++, homog | −1.514 | −11.415 | −1.153 |
| ++, homog | 98.78 | 108.856 | −10.803 |
| ++, heterog | 129.525 | 98.389 | 3.160 |
| ++, homog | 164.757 | 142.636 | 6.448 |
| ++, homog | 183.429 | 89.185 | 0.946 |
| +, homog | 46.275 | 7.413 | 0.191 |
| - | 22.654 | −37.171 | −0.621 |
| - | 48.519 | 5.938 | 0.139 |
| SF Uptake Pattern MRI | +++ | ++ | + | - |
|---|---|---|---|---|
| A | 4 | 2 | ||
| B | 1 | 3 | 1 | 1 |
| C | 4 | 1 | ||
| D | 1 | 2 | 2 |
| MRI\SF | +++ | ++ | + | - |
|---|---|---|---|---|
| +++ | 7 | 2 | ||
| ++ | 3 | 3 | ||
| + | 1 | 1 | 1 | |
| - | 1 | 1 | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Laurentis, C.; Beuriat, P.A.; Bteich, F.; Mottolese, C.; Szathmari, A.; Vinchon, M.; Di Rocco, F. Pediatric Low-Grade Glioma Surgery with Sodium Fluorescein: Efficient Localization for Removal and Association with Intraoperative Pathological Sampling. Diagnostics 2022, 12, 2927. https://doi.org/10.3390/diagnostics12122927
de Laurentis C, Beuriat PA, Bteich F, Mottolese C, Szathmari A, Vinchon M, Di Rocco F. Pediatric Low-Grade Glioma Surgery with Sodium Fluorescein: Efficient Localization for Removal and Association with Intraoperative Pathological Sampling. Diagnostics. 2022; 12(12):2927. https://doi.org/10.3390/diagnostics12122927
Chicago/Turabian Stylede Laurentis, Camilla, Pierre Aurélien Beuriat, Fred Bteich, Carmine Mottolese, Alexandru Szathmari, Matthieu Vinchon, and Federico Di Rocco. 2022. "Pediatric Low-Grade Glioma Surgery with Sodium Fluorescein: Efficient Localization for Removal and Association with Intraoperative Pathological Sampling" Diagnostics 12, no. 12: 2927. https://doi.org/10.3390/diagnostics12122927