
Multimodality Imaging of Benign Primary Cardiac Tumor
 , and
, and
Abstract
:1. Introduction
2. Clinical Manifestations
3. Multimodality Imaging
3.1. Echocardiography
3.2. Cardiac Magnetic Resonance
3.3. Cardiac Computed Tomography
3.4. Positron Emission Tomography
4. Benign Cardiac Primary Cardiac Tumor (Table 1)
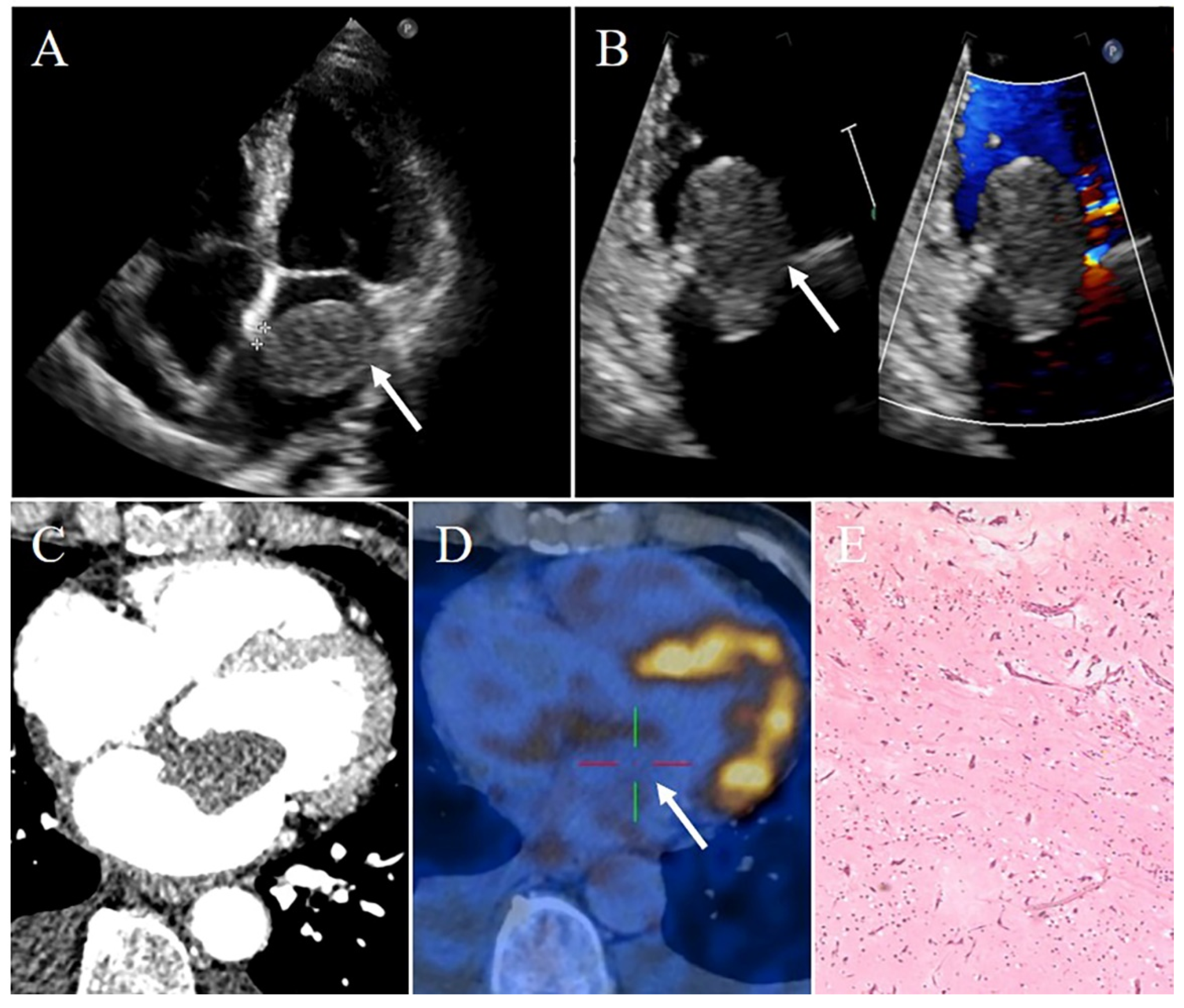
4.1. Myxoma

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Tumor | Common Age | Common Gender | Most Common Site | Echo Features | CT Features | CMR Features |
|---|---|---|---|---|---|---|
| Myxoma | Middle age (30–60 y); younger if associated with Carney complex | Females | Left atrium; attached to the fossa ovalis | Heterogeneous; narrow pedicle; regular mobile throughout the cardiac cycle | Heterogeneous; low-attenuation; calcification seen in 10–20% of patients | Smooth, well-defined, lobular or oval; heterogeneous; isointense on T1WI; hyperintense on T2WI; heterogeneous enhancement |
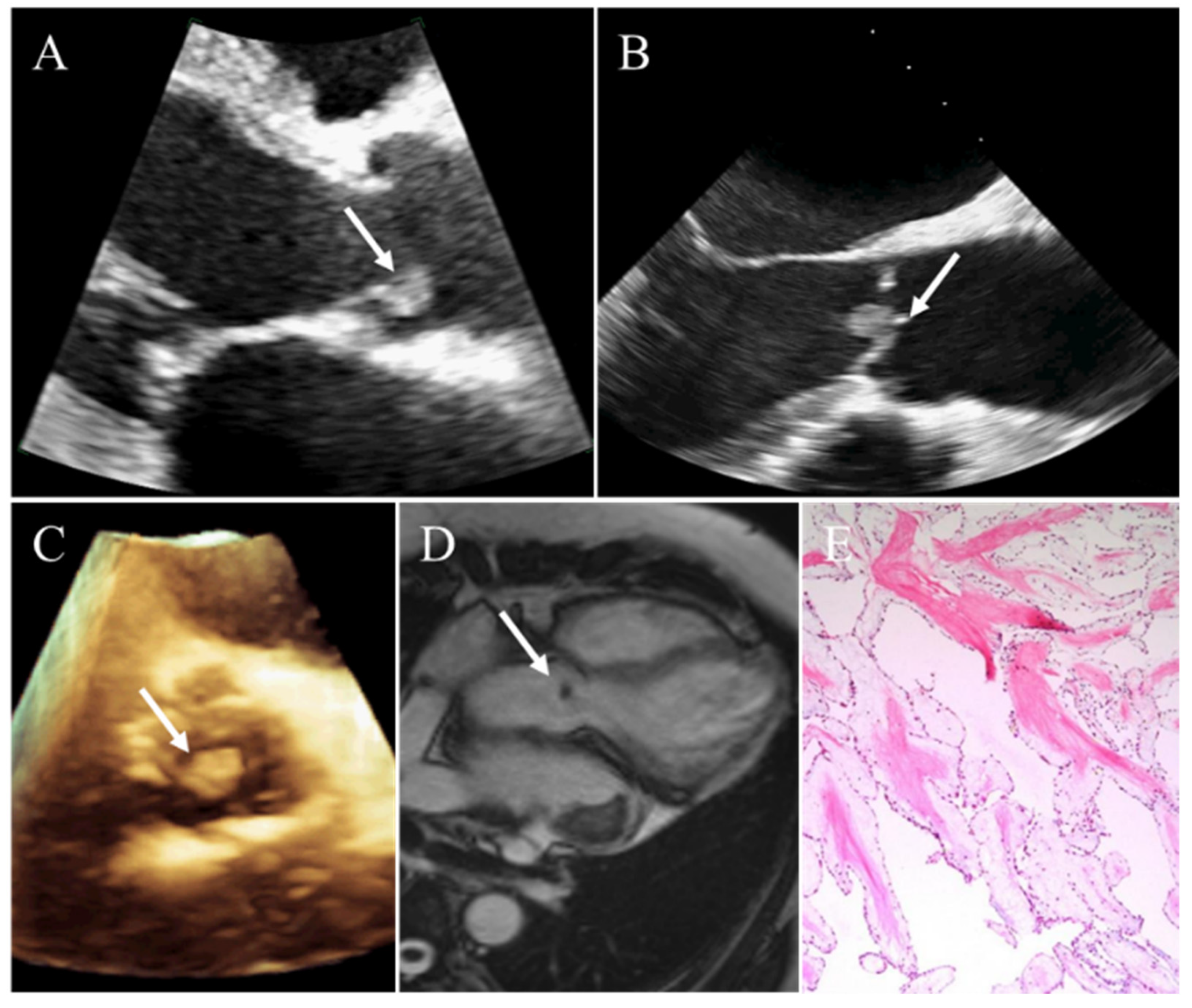
| Papillary fibroelastoma | 40–80 y | Men | Cardiac valves | Small (usually <1.5 cm); round; well-circumscribed; homogeneously textured appearance; a short pedicle; shimmering edges | Difficult to observe | Difficult to observe |
| Lipoma | No defined age distribution | No defined sex distribution | Left heart; subendocardial layer | Usually hypoechoic in the pericardial space, homogenous and hyperechoic in cardiac chambers; broad base; immobile; well-circumscribed | Homogeneous fat attenuation; well-defined; smooth; encapsulated; no contrast enhanced | Homogeneous hyperintense on T1WI and complete signal loss in fat suppression sequence; hyperintensity on T2WI; no enhancement |
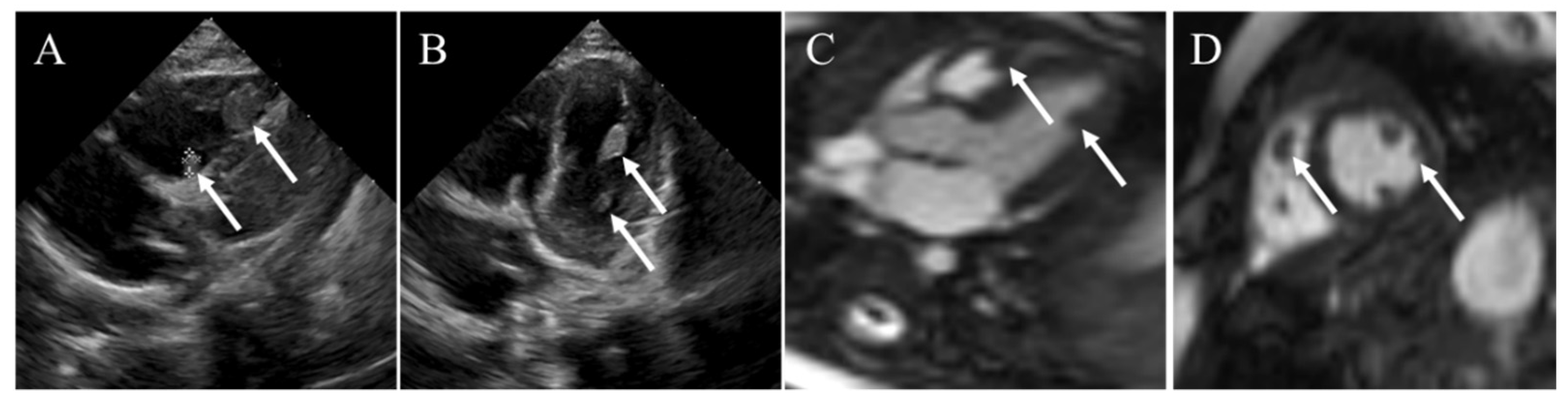
| Rhabdomyoma | Infants and children | No defined sex distribution | Usually intramyocardial or intracavitary; no difference in distribution between the left and right heart | Multiple; small; round; lobulated; well-circumscribed; homogenous hyperecho | Multiple homogeneous low attenuation; no enhancement | Isointense on T1WI; hyperintense on T2WI; no enhancement |
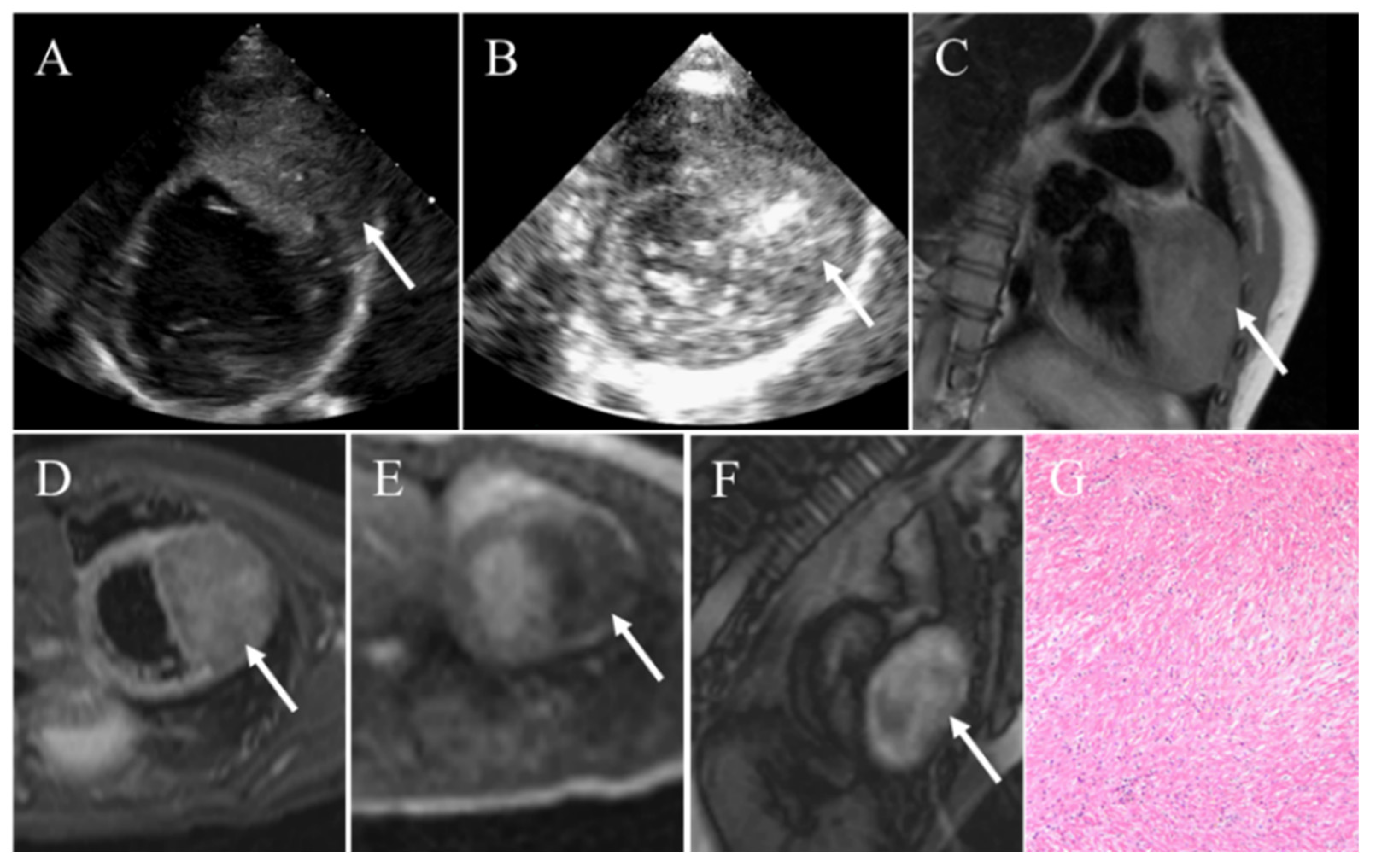
| Fibroma | Infants and children | No defined sex distribution | Ventricles | Large; intramural; well-circumscribed; noncontractile; central calcification | Homogenous; intramural; soft-tissue attenuation; central calcification; little to no enhancement | Iso-intense on T1WI; hypointense on T2WI; homogenous; no enhancement on resting first-pass perfusion imaging and EGE; hyperenhancement on LGE |
| Paraganglioma | 20–60 y (typically in young adults) | No defined sex distribution | Left atrium; interatrial septum; aortic body | Granular; oval; well-demarcated; broad base; heterogeneous | Well-circumscribed; heterogeneous; low attenuation; heterogeneous marked enhancement | Isointense or hypointense on T1WI; hyerointense on T2WI; heterogeneous and peripheral rim enhancement |
| Hemangioma | Adulthood | Females | Ventricles | Well-circumscribed; oscillated with the cardiac cycle; blood flow signals on color Doppler flow imaging; obviously enhancement | Well-defined; low density or equal density; heterogeneous intense enhancement; “vascular blush” on coronary angiography | Heterogeneous isointense or hypointense on T1WI; hyperintense on T2WI; heterogeneous enhancement |
4.2. Papillary Fibroelastoma
4.3. Lipoma
4.4. Rhabdomyoma
4.5. Fibroma
4.6. Cardiac Paraganglioma
4.7. Hemangioma
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Silverman, N.A. Primary cardiac tumors. Ann. Surg. 1980, 191, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Gu, T.; Shi, E.; Xiu, Z.; Fang, Q.; Wang, C.; Wang, X.; Cheng, Y. Primary malignant cardiac tumors. J. Cancer Res. Clin. Oncol. 2014, 140, 1047–1055. [Google Scholar] [CrossRef] [PubMed]
- Burke, A.; Tavora, F. The 2015 who classification of tumors of the heart and pericardium. J. Thorac. Oncol. 2016, 11, 441–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paraskevaidis, I.A.; Michalakeas, C.A.; Papadopoulos, C.H.; Anastasiou-Nana, M. Cardiac tumors. ISRN Oncol. 2011, 2011, 208929. [Google Scholar] [CrossRef] [Green Version]
- Burnside, N.; MacGowan, S.W. Malignant primary cardiac tumours. Interact. Cardiovasc. Thorac. Surg. 2012, 15, 1004–1006. [Google Scholar] [CrossRef] [Green Version]
- Reynen, K. Frequency of primary tumors of the heart. Am. J. Cardiol. 1996, 77, 107. [Google Scholar] [CrossRef]
- Centofanti, P.; di Rosa, E.; Deorsola, L.; Dato, G.M.; Patanè, F.; la Torre, M.; Barbato, L.; Verzini, A.; Fortunato, G.; di Summa, M. Primary cardiac tumors: Early and late results of surgical treatment in 91 patients. Ann. Thorac. Surg. 1999, 68, 1236–1241. [Google Scholar] [CrossRef]
- Uzun, O.; Wilson, D.G.; Vujanic, G.M.; Parsons, J.M.; de Giovanni, J.V. Cardiac tumours in children. Orphanet. J. Rare Dis. 2007, 2, 11. [Google Scholar] [CrossRef] [Green Version]
- Beghetti, M.; Gow, R.M.; Haney, I.; Mawson, J.; Williams, W.G.; Freedom, R.M. Pediatric primary benign cardiac tumors: A 15-year review. Am. Heart J. 1997, 134, 1107–1114. [Google Scholar] [CrossRef]
- Oliveira, G.H.; Al-Kindi, S.G.; Hoimes, C.; Park, S.J. Characteristics and survival of malignant cardiac tumors: A 40-year analysis of >500 patients. Circulation 2015, 132, 2395–2402. [Google Scholar] [CrossRef]
- Biersmith, M.A.; Tong, M.S.; Guha, A.; Simonetti, O.P.; Addison, D. Multimodality cardiac imaging in the era of emerging cancer therapies. J. Am. Heart Assoc. 2020, 9, e013755. [Google Scholar] [CrossRef]
- Rathi, V.K.; Czajka, A.T.; Thompson, D.V.; Doyle, M.; Tewatia, T.; Yamrozik, J.; Williams, R.B.; Biederman, R.W.W. Can cardiovascular mri be used to more definitively characterize cardiac masses initially identified using echocardiography? Echocardiography 2018, 35, 735–742. [Google Scholar] [CrossRef] [PubMed]
- Dell’Aquila, M.; Carbone, A.; Pennacchia, I.; Stigliano, E.; Oliva, A.; Arena, V. Sudden death by massive systemic embolism from cardiac myxoma. Role of the clinical autopsy and review of literature. Cardiovasc. Pathol. 2020, 49, 107244. [Google Scholar] [CrossRef] [PubMed]
- Kitchin, P.L.; Benson, P. Left ventricular myxoma causing sudden death. Am. J. Forensic Med. Pathol. 2015, 36, 58–60. [Google Scholar] [CrossRef] [PubMed]
- Hermann, F.E.M.; Hagl, C.; Juchem, G. Giant left atrial myxoma and left ventricular inflow obstruction. Dtsch. Arztebl. Int. 2021, 118, 486. [Google Scholar] [CrossRef]
- Jones, J.P.; Ramcharan, T.; Chaudhari, M.; Bhole, V.; McLeod, K.; Sadagopan, S.; Uzun, O.; Parry, A.; Till, J.; McMahon, C.J.; et al. Ventricular fibromas in children, arrhythmia risk, and outcomes: A multicenter study. Heart Rhythm 2018, 15, 1507–1512. [Google Scholar] [CrossRef]
- Pinede, L.; Duhaut, P.; Loire, R. Clinical presentation of left atrial cardiac myxoma. A series of 112 consecutive cases. Medicine 2001, 80, 159–172. [Google Scholar] [CrossRef]
- Lee, P.T.; Hong, R.; Pang, P.Y.; Chua, Y.L.; Ding, Z.P. Clinical presentation of cardiac myxoma in a singapore national cardiac centre. Singap. Med. J. 2021, 62, 195–198. [Google Scholar] [CrossRef]
- Yuan, L.; Ge, L.; Zhu, Y.; Chen, C.; Zhou, Z.; Yang, Q. Cardiac myxoma and ischemic stroke. QJM 2020, 113, 674–675. [Google Scholar] [CrossRef] [Green Version]
- Lima, N.A.; Byers-Spencer, K.; Cwikla, K.; Huffman, C.; Diaz, M.; Melgar, T.A.; Helmstetter, N. Benign cardiac neoplasms in the united states: A thirteen-year review. Cardiology 2021, 146, 748–753. [Google Scholar] [CrossRef]
- Poterucha, T.J.; Kochav, J.; O’Connor, D.S.; Rosner, G.F. Cardiac tumors: Clinical presentation, diagnosis, and management. Curr. Treat. Options Oncol. 2019, 20, 66. [Google Scholar] [CrossRef] [PubMed]
- Alamri, Y.; Lau, Y.Y.; Lainchbury, J. Large right atrial myxoma presenting with heart failure. ANZ J. Surg. 2019, 89, 1341–1342. [Google Scholar] [CrossRef] [PubMed]
- Nomoto, N.; Tani, T.; Konda, T.; Kim, K.; Kitai, T.; Ota, M.; Kaji, S.; Imai, Y.; Okada, Y.; Furukawa, Y. Primary and metastatic cardiac tumors: Echocardiographic diagnosis, treatment and prognosis in a 15-years single center study. J. Cardiothorac. Surg. 2017, 12, 103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butany, J.; Nair, V.; Naseemuddin, A.; Nair, G.M.; Catton, C.; Yau, T. Cardiac tumours: Diagnosis and management. Lancet Oncol. 2005, 6, 219–228. [Google Scholar] [CrossRef]
- Asakai, H. Ventricular fibromas in children: Surgical resection can be a cure to lethal arrhythmias. Heart Rhythm 2018, 15, 1513–1514. [Google Scholar] [CrossRef] [PubMed]
- Miyake, C.Y.; del Nido, P.J.; Alexander, M.E.; Cecchin, F.; Berul, C.I.; Triedman, J.K.; Geva, T.; Walsh, E.P. Cardiac tumors and associated arrhythmias in pediatric patients, with observations on surgical therapy for ventricular tachycardia. J. Am. Coll. Cardiol. 2011, 58, 1903–1909. [Google Scholar] [CrossRef] [Green Version]
- Jin, Y.; Li, X.M.; Liu, R.; Chen, G.; Zhang, X.; Wu, Q. Surgical treatment of primary cardiac tumor associated with malignant arrhythmias. Heart Surg. Forum 2020, 23, E178–E182. [Google Scholar] [CrossRef]
- Lamba, G.; Frishman, W.H. Cardiac and pericardial tumors. Cardiol. Rev. 2012, 20, 237–252. [Google Scholar] [CrossRef]
- Lee, S.J.; Kim, J.H.; Na, C.Y.; Oh, S.S. Eleven years’ experience with korean cardiac myxoma patients: Focus on embolic complications. Cerebrovasc. Dis. 2012, 33, 471–479. [Google Scholar] [CrossRef]
- Kesav, P.; John, S.; Joshi, P.; Gaba, W.H.; Hussain, S.I. Cardiac myxoma embolization causing ischemic stroke and multiple partially thrombosed cerebral aneurysms. Stroke 2021, 52, e10–e14. [Google Scholar] [CrossRef]
- Kuon, E.; Kreplin, M.; Weiss, W.; Dahm, J.B. The challenge presented by right atrial myxoma. Herz 2004, 29, 702–709. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.G.; Wang, B.; Hu, Y.; Liu, J.H.; Liu, B.; Liu, H.; Zhao, P.; Zhang, L.; Li, Y.J. Clinicopathologic features and outcomes of primary cardiac tumors: A 16-year-experience with 212 patients at a chinese medical center. Cardiovasc. Pathol. 2018, 33, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Hong, Z.L.; Zhao, Y.C.; Chen, S.; Lin, Y.C.; Wu, S.S. Percutaneous ultrasound-guided core needle biopsy for the diagnosis of cardiac tumors: Optimizing the treatment strategy for patients with intermural and pericardial cardiac tumors. Front. Oncol. 2022, 12, 931081. [Google Scholar] [CrossRef]
- D’Angelo, E.C.; Paolisso, P.; Vitale, G.; Foà, A.; Bergamaschi, L.; Magnani, I.; Saturi, G.; Rinaldi, A.; Toniolo, S.; Renzulli, M.; et al. Diagnostic accuracy of cardiac computed tomography and 18-f fluorodeoxyglucose positron emission tomography in cardiac masses. JACC Cardiovasc. Imaging 2020, 13, 2400–2411. [Google Scholar] [CrossRef] [PubMed]
- Günther, T.; Schreiber, C.; Noebauer, C.; Eicken, A.; Lange, R. Treatment strategies for pediatric patients with primary cardiac and pericardial tumors: A 30-year review. Pediatr. Cardiol. 2008, 29, 1071–1076. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Hong, H.; Zhang, H.; Xu, Z.; Liu, J.; Qiu, L. Treatment strategies for primary tumors of the heart in children: A 10-year experience. Ann. Thorac. Surg. 2015, 100, 1744–1749. [Google Scholar] [CrossRef] [Green Version]
- Klein, A.L.; Abbara, S.; Agler, D.A.; Appleton, C.P.; Asher, C.R.; Hoit, B.; Hung, J.; Garcia, M.J.; Kronzon, I.; Oh, J.K.; et al. American society of echocardiography clinical recommendations for multimodality cardiovascular imaging of patients with pericardial disease: Endorsed by the society for cardiovascular magnetic resonance and society of cardiovascular computed tomography. J. Am. Soc. Echocardiogr. 2013, 26, 965–1012. [Google Scholar] [CrossRef]
- Xia, H.; Gan, L.; Jiang, Y.; Tang, Q.; Zhang, P.; Tang, X.; Wen, L.; Liu, Z.; Gao, Y. Use of transesophageal echocardiography and contrast echocardiography in the evaluation of cardiac masses. Int. J. Cardiol. 2017, 236, 466–472. [Google Scholar] [CrossRef]
- Tyebally, S.; Chen, D.; Bhattacharyya, S.; Mughrabi, A.; Hussain, Z.; Manisty, C.; Westwood, M.; Ghosh, A.K.; Guha, A. Cardiac tumors: Jacc cardiooncology state-of-the-art review. JACC CardioOncol. 2020, 2, 293–311. [Google Scholar] [CrossRef]
- Buckley, O.; Madan, R.; Kwong, R.; Rybicki, F.J.; Hunsaker, A. Cardiac masses, part 1: Imaging strategies and technical considerations. AJR Am. J. Roentgenol. 2011, 197, W837–W841. [Google Scholar] [CrossRef]
- Shyu, K.G.; Chen, J.J.; Cheng, J.J.; Hwang, J.J.; Kuan, P.; Lien, W.P. Comparison of transthoracic and transesophageal echocardiography in the diagnosis of intracardiac tumors in adults. J. Clin. Ultrasound 1994, 22, 381–389. [Google Scholar] [CrossRef] [PubMed]
- Engberding, R.; Daniel, W.G.; Erbel, R.; Kasper, W.; Lestuzzi, C.; Curtius, J.M.; Sutherland, G.R.; Lambertz, H.; von Hehn, A.; Lesbre, J.P.; et al. Diagnosis of heart tumours by transoesophageal echocardiography: A multicentre study in 154 patients. European cooperative study group. Eur. Heart J. 1993, 14, 1223–1228. [Google Scholar] [CrossRef] [PubMed]
- Obeid, A.I.; Marvasti, M.; Parker, F.; Rosenberg, J. Comparison of transthoracic and transesophageal echocardiography in diagnosis of left atrial myxoma. Am. J. Cardiol. 1989, 63, 1006–1008. [Google Scholar] [CrossRef]
- Zaragoza-Macias, E.; Chen, M.A.; Gill, E.A. Real time three-dimensional echocardiography evaluation of intracardiac masses. Echocardiography 2012, 29, 207–219. [Google Scholar] [CrossRef]
- Tang, Q.Y.; Guo, L.D.; Wang, W.X.; Zhou, W.; Liu, Y.N.; Liu, H.Y.; Li, L.; Deng, Y.B. Usefulness of contrast perfusion echocardiography for differential diagnosis of cardiac masses. Ultrasound Med. Biol. 2015, 41, 2382–2390. [Google Scholar] [CrossRef]
- Uenishi, E.K.; Caldas, M.A.; Tsutsui, J.M.; Abduch, M.C.; Sbano, J.C.; Filho, R.K.; Mathias, W., Jr. Evaluation of cardiac masses by real-time perfusion imaging echocardiography. Cardiovasc. Ultrasound 2015, 13, 23. [Google Scholar] [CrossRef] [Green Version]
- Kirkpatrick, J.N.; Wong, T.; Bednarz, J.E.; Spencer, K.T.; Sugeng, L.; Ward, R.P.; DeCara, J.M.; Weinert, L.; Krausz, T.; Lang, R.M. Differential diagnosis of cardiac masses using contrast echocardiographic perfusion imaging. J. Am. Coll. Cardiol. 2004, 43, 1412–1419. [Google Scholar] [CrossRef] [Green Version]
- Pazos-López, P.; Pozo, E.; Siqueira, M.E.; García-Lunar, I.; Cham, M.; Jacobi, A.; Macaluso, F.; Fuster, V.; Narula, J.; Sanz, J. Value of cmr for the differential diagnosis of cardiac masses. JACC Cardiovasc. Imaging 2014, 7, 896–905. [Google Scholar] [CrossRef] [Green Version]
- Tumma, R.; Dong, W.; Wang, J.; Litt, H.; Han, Y. Evaluation of cardiac masses by cmr-strengths and pitfalls: A tertiary center experience. Int. J. Cardiovasc. Imaging 2016, 32, 913–920. [Google Scholar] [CrossRef]
- Alabed, S.; Garg, P.; Johns, C.S.; Alandejani, F.; Shahin, Y.; Dwivedi, K.; Zafar, H.; Wild, J.M.; Kiely, D.G.; Swift, A.J. Cardiac magnetic resonance in pulmonary hypertension-an update. Curr. Cardiovasc. Imaging Rep. 2020, 13, 30. [Google Scholar] [CrossRef]
- Kumar, P.; Singh, A.; Deshmukh, A.; Kumar, S. Cardiac mri for the evaluation of cardiac neoplasms. Clin. Radiol. 2020, 75, 241–253. [Google Scholar] [CrossRef] [PubMed]
- Motwani, M.; Kidambi, A.; Herzog, B.A.; Uddin, A.; Greenwood, J.P.; Plein, S. Mr imaging of cardiac tumors and masses: A review of methods and clinical applications. Radiology 2013, 268, 26–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fussen, S.; de Boeck, B.W.; Zellweger, M.J.; Bremerich, J.; Goetschalckx, K.; Zuber, M.; Buser, P.T. Cardiovascular magnetic resonance imaging for diagnosis and clinical management of suspected cardiac masses and tumours. Eur. Heart J. 2011, 32, 1551–1560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dawson, D.; Mohiaddin, R. Assessment of pericardial diseases and cardiac masses with cardiovascular magnetic resonance. Prog. Cardiovasc. Dis. 2011, 54, 305–319. [Google Scholar] [CrossRef]
- Pontone, G.; di Cesare, E.; Castelletti, S.; de Cobelli, F.; de Lazzari, M.; Esposito, A.; Focardi, M.; di Renzi, P.; Indolfi, C.; Lanzillo, C.; et al. Appropriate use criteria for cardiovascular magnetic resonance imaging (cmr): Sic-sirm position paper part 1 (ischemic and congenital heart diseases, cardio-oncology, cardiac masses and heart transplant). Radiol. Med. 2021, 126, 365–379. [Google Scholar] [CrossRef]
- Mousavi, N.; Cheezum, M.K.; Aghayev, A.; Padera, R.; Vita, T.; Steigner, M.; Hulten, E.; Bittencourt, M.S.; Dorbala, S.; di Carli, M.F.; et al. Assessment of cardiac masses by cardiac magnetic resonance imaging: Histological correlation and clinical outcomes. J. Am. Heart Assoc. 2019, 8, e007829. [Google Scholar] [CrossRef] [Green Version]
- Zatorska, K.; Michalowska, I.; Duchnowski, P.; Szymanski, P.; Kusmierczyk, M.; Hryniewiecki, T. The usefulness of magnetic resonance imaging in the diagnosis of infectious endocarditis. J. Heart Valve Dis. 2015, 24, 767–775. [Google Scholar]
- Spuentrup, E.; Mahnken, A.H.; Kühl, H.P.; Krombach, G.A.; Botnar, R.M.; Wall, A.; Schaeffter, T.; Günther, R.W.; Buecker, A. Fast interactive real-time magnetic resonance imaging of cardiac masses using spiral gradient echo and radial steady-state free precession sequences. Investig. Radiol. 2003, 38, 288–292. [Google Scholar] [CrossRef]
- Hoey, E.; Ganeshan, A.; Nader, K.; Randhawa, K.; Watkin, R. Cardiac neoplasms and pseudotumors: Imaging findings on multidetector ct angiography. Diagn. Interv. Radiol. 2012, 18, 67–77. [Google Scholar] [CrossRef] [Green Version]
- Junttila, M.J.; Fishman, J.E.; Lopera, G.A.; Pattany, P.M.; Velazquez, D.L.; Williams, A.R.; Trachtenberg, B.H.; Sanina, C.; Mather, J.; Hare, J.M. Safety of serial mri in patients with implantable cardioverter defibrillators. Heart 2011, 97, 1852–1856. [Google Scholar] [CrossRef] [Green Version]
- Kakouros, N.; Giles, J.; Crundwell, N.B.; McWilliams, E.T. The utility of cardiac ct beyond the assessment of suspected coronary artery disease. Clin. Radiol. 2012, 67, 695–708. [Google Scholar] [CrossRef] [PubMed]
- Achenbach, S.; Kondo, T. Technical advances in cardiac ct. Cardiol. Clin. 2012, 30, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Young, P.M.; Foley, T.A.; Araoz, P.A.; Williamson, E.E. Computed tomography imaging of cardiac masses. Radiol. Clin. N. Am. 2019, 57, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Grebenc, M.L.; Rosado-de-Christenson, M.L.; Green, C.E.; Burke, A.P.; Galvin, J.R. Cardiac myxoma: Imaging features in 83 patients. Radiographics 2002, 22, 673–689. [Google Scholar] [CrossRef] [PubMed]
- Shin, W.; Choe, Y.H.; Kim, S.M.; Song, I.Y.; Kim, S.S. Detection of cardiac myxomas with non-contrast chest ct. Acta Radiol. 2014, 55, 273–278. [Google Scholar] [CrossRef]
- Kassop, D.; Donovan, M.S.; Cheezum, M.K.; Nguyen, B.T.; Gambill, N.B.; Blankstein, R.; Villines, T.C. Cardiac masses on cardiac ct: A review. Curr. Cardiovasc. Imaging Rep. 2014, 7, 9281. [Google Scholar] [CrossRef] [Green Version]
- Husmann, L.; Valenta, I.; Gaemperli, O.; Adda, O.; Treyer, V.; Wyss, C.A.; Veit-Haibach, P.; Tatsugami, F.; von Schulthess, G.K.; Kaufmann, P.A. Feasibility of low-dose coronary ct angiography: First experience with prospective ecg-gating. Eur. Heart J. 2008, 29, 191–197. [Google Scholar] [CrossRef] [Green Version]
- Feng, Q.; Yin, Y.; Hua, X.; Zhu, R.; Hua, J.; Xu, J. Prospective ecg triggering versus low-dose retrospective ecg-gated 128-channel ct coronary angiography: Comparison of image quality and radiation dose. Clin. Radiol. 2010, 65, 809–814. [Google Scholar] [CrossRef]
- Rahbar, K.; Seifarth, H.; Schäfers, M.; Stegger, L.; Hoffmeier, A.; Spieker, T.; Tiemann, K.; Maintz, D.; Scheld, H.H.; Schober, O.; et al. Differentiation of malignant and benign cardiac tumors using 18f-fdg pet/ct. J. Nucl. Med. 2012, 53, 856–863. [Google Scholar] [CrossRef] [Green Version]
- El-Galaly, T.C.; Villa, D.; Gormsen, L.C.; Baech, J.; Lo, A.; Cheah, C.Y. Fdg-pet/ct in the management of lymphomas: Current status and future directions. J. Intern. Med. 2018, 284, 358–376. [Google Scholar] [CrossRef] [Green Version]
- Zaucha, J.M.; Chauvie, S.; Zaucha, R.; Biggii, A.; Gallamini, A. The role of pet/ct in the modern treatment of hodgkin lymphoma. Cancer Treat. Rev. 2019, 77, 44–56. [Google Scholar] [CrossRef] [PubMed]
- Saif, M.W.; Tzannou, I.; Makrilia, N.; Syrigos, K. Role and cost effectiveness of pet/ct in management of patients with cancer. Yale J. Biol. Med. 2010, 83, 53–65. [Google Scholar]
- Shao, D.; Wang, S.X.; Liang, C.H.; Gao, Q. Differentiation of malignant from benign heart and pericardial lesions using positron emission tomography and computed tomography. J. Nucl. Cardiol. 2011, 18, 668–677. [Google Scholar] [CrossRef] [PubMed]
- Nensa, F.; Tezgah, E.; Poeppel, T.D.; Jensen, C.J.; Schelhorn, J.; Köhler, J.; Heusch, P.; Bruder, O.; Schlosser, T.; Nassenstein, K. Integrated 18f-fdg pet/mr imaging in the assessment of cardiac masses: A pilot study. J. Nucl. Med. 2015, 56, 255–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masuda, A.; Manabe, O.; Oyama-Manabe, N.; Naya, M.; Obara, M.; Sakakibara, M.; Hirata, K.; Yamada, S.; Naka, T.; Tsutsui, H.; et al. Cardiac fibroma with high (18)f-fdg uptake mimicking malignant tumor. J. Nucl. Cardiol. 2017, 24, 323–324. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Ma, X.; Tan, Y.; Lu, Q.; Wang, Y. Hamartoma of mature cardiac myocytes mimicking malignancy on 18f-fdg pet/ct images. Clin. Nucl. Med. 2019, 44, 892–894. [Google Scholar] [CrossRef]
- Martineau, P.; Dilsizian, V.; Pelletier-Galarneau, M. Incremental value of fdg-pet in the evaluation of cardiac masses. Curr. Cardiol. Rep. 2021, 23, 78. [Google Scholar] [CrossRef]
- Boursier, C.; Duval, X.; Bourdon, A.; Imbert, L.; Mahida, B.; Chevalier, E.; Claudin, M.; Hoen, B.; Goehringer, F.; Selton-Suty, C.; et al. Ecg-gated cardiac fdg pet acquisitions significantly improve detectability of infective endocarditis. JACC Cardiovasc. Imaging 2020, 13, 2691–2693. [Google Scholar] [CrossRef]
- Chareonthaitawee, P.; Beanlands, R.S.; Chen, W.; Dorbala, S.; Miller, E.J.; Murthy, V.L.; Birnie, D.H.; Chen, E.S.; Cooper, L.T.; Tung, R.H.; et al. Joint snmmi-asnc expert consensus document on the role of (18)f-fdg pet/ct in cardiac sarcoid detection and therapy monitoring. J. Nucl. Med. 2017, 58, 1341–1353. [Google Scholar] [CrossRef] [Green Version]
- Soussan, M.; Brillet, P.Y.; Nunes, H.; Pop, G.; Ouvrier, M.J.; Naggara, N.; Valeyre, D.; Weinmann, P. Clinical value of a high-fat and low-carbohydrate diet before fdg-pet/ct for evaluation of patients with suspected cardiac sarcoidosis. J. Nucl. Cardiol. 2013, 20, 120–127. [Google Scholar] [CrossRef]
- Osborne, M.T.; Hulten, E.A.; Murthy, V.L.; Skali, H.; Taqueti, V.R.; Dorbala, S.; DiCarli, M.F.; Blankstein, R. Patient preparation for cardiac fluorine-18 fluorodeoxyglucose positron emission tomography imaging of inflammation. J. Nucl. Cardiol. 2017, 24, 86–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffmeier, A.; Schmid, C.; Deiters, S.; Drees, G.; Rothenburger, M.; Tjan, T.D.; Schmidt, C.; Löher, A.; Maintz, D.; Spieker, T.; et al. Neoplastic heart disease—The muenster experience with 108 patients. Thorac. Cardiovasc. Surg. 2005, 53, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Freedom, R.M.; Lee, K.J.; MacDonald, C.; Taylor, G. Selected aspects of cardiac tumors in infancy and childhood. Pediatr. Cardiol. 2000, 21, 299–316. [Google Scholar] [CrossRef] [PubMed]
- Nehaj, F.; Sokol, J.; Mokan, M.; Jankovicova, V.; Kovar, F.; Kubaskova, M.; Mizera, S.; Mokan, M. Outcomes of patients with newly diagnosed cardiac myxoma: A retrospective multicentric study. BioMed Res. Int. 2018, 2018, 8320793. [Google Scholar] [CrossRef]
- Zheng, J.J.; Geng, X.G.; Wang, H.C.; Yan, Y.; Wang, H.Y. Clinical and histopathological analysis of 66 cases with cardiac myxoma. Asian Pac. J. Cancer Prev. 2013, 14, 1743–1746. [Google Scholar] [CrossRef] [Green Version]
- Türkmen, N.; Eren, B.; Fedakar, R.; Comunoglu, N. An unusual cause of sudden death: Cardiac myxoma. Adv. Ther. 2007, 24, 529–532. [Google Scholar] [CrossRef]
- Pitsava, G.; Zhu, C.; Sundaram, R.; Mills, J.L.; Stratakis, C.A. Predicting the risk of cardiac myxoma in carney complex. Genet. Med. 2021, 23, 80–85. [Google Scholar] [CrossRef]
- Boyacıoğlu, K.; Kalender, M.; Dönmez, A.A.; Çayhan, B.; Tuncer, M.A. Outcomes following embolization in patients with cardiac myxoma. J. Card. Surg. 2017, 32, 621–626. [Google Scholar] [CrossRef]
- Reynen, K. Cardiac myxomas. N. Engl. J. Med. 1995, 333, 1610–1617. [Google Scholar] [CrossRef]
- Dujardin, K.S.; Click, R.L.; Oh, J.K. The role of intraoperative transesophageal echocardiography in patients undergoing cardiac mass removal. J. Am. Soc. Echocardiogr. 2000, 13, 1080–1083. [Google Scholar] [CrossRef]
- Ji, X.; Zhang, X. Left atrial myxoma with left ventricular myxoma diagnosed by ultrasound examination: A case report. Medicine 2021, 100, e26903. [Google Scholar] [CrossRef] [PubMed]
- Lampropoulos, K.; Bogaert, J.; Voigt, J.U.; Budts, W. Left atrial myxoma. Evaluation with transoesophageal echocardiographic and real time three-dimensional imaging. Acta Clin. Belg. 2011, 66, 318–320. [Google Scholar] [CrossRef] [PubMed]
- Espinola-Zavaleta, N.; Lozoya-Del Rosal, J.J.; Colin-Lizalde, L.; Lupi-Herrera, E. Left atrial cardiac myxoma. Two unusual cases studied by 3d echocardiography. BMJ Case Rep. 2014, 2014, bcr2014205938. [Google Scholar] [CrossRef] [PubMed]
- Mansencal, N.; Revault-d’Allonnes, L.; Pelage, J.P.; Farcot, J.C.; Lacombe, P.; Dubourg, O. Usefulness of contrast echocardiography for assessment of intracardiac masses. Arch. Cardiovasc. Dis. 2009, 102, 177–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.; Li, Q.; Xue, M.; Zhao, P.; Cui, J. Cardiac myxoma: A rare case series of 3 patients and a literature review. J. Ultrasound Med. 2017, 36, 2361–2366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, E.Y.; Choe, Y.H.; Sung, K.; Park, S.W.; Kim, J.H.; Ko, Y.H. Multidetector ct and mr imaging of cardiac tumors. Korean J. Radiol. 2009, 10, 164–175. [Google Scholar] [CrossRef] [Green Version]
- Colin, G.C.; Gerber, B.L.; Amzulescu, M.; Bogaert, J. Cardiac myxoma: A contemporary multimodality imaging review. Int. J. Cardiovasc. Imaging 2018, 34, 1789–1808. [Google Scholar] [CrossRef]
- Li, X.; Chen, Y.; Liu, J.; Xu, L.; Li, Y.; Liu, D.; Sun, Z.; Wen, Z. Cardiac magnetic resonance imaging of primary cardiac tumors. Quant. Imaging Med. Surg. 2020, 10, 294–313. [Google Scholar] [CrossRef]
- Sparrow, P.J.; Kurian, J.B.; Jones, T.R.; Sivananthan, M.U. Mr imaging of cardiac tumors. Radiographics 2005, 25, 1255–1276. [Google Scholar] [CrossRef]
- Abbas, A.; Garfath-Cox, K.A.; Brown, I.W.; Shambrook, J.S.; Peebles, C.R.; Harden, S.P. Cardiac mr assessment of cardiac myxomas. Br. J. Radiol. 2015, 88, 20140599. [Google Scholar] [CrossRef]
- Gheysens, O.; Cornillie, J.; Voigt, J.U.; Bogaert, J.; Westhovens, R. Left atrial myxoma on fdg-pet/ct. Clin. Nucl. Med. 2013, 38, e421–e422. [Google Scholar] [CrossRef] [PubMed]
- Ngaage, D.L.; Mullany, C.J.; Daly, R.C.; Dearani, J.A.; Edwards, W.D.; Tazelaar, H.D.; McGregor, C.G.; Orszulak, T.A.; Puga, F.J.; Schaff, H.V.; et al. Surgical treatment of cardiac papillary fibroelastoma: A single center experience with eighty-eight patients. Ann. Thorac. Surg. 2005, 80, 1712–1718. [Google Scholar] [CrossRef]
- Gowda, R.M.; Khan, I.A.; Nair, C.K.; Mehta, N.J.; Vasavada, B.C.; Sacchi, T.J. Cardiac papillary fibroelastoma: A comprehensive analysis of 725 cases. Am. Heart J. 2003, 146, 404–410. [Google Scholar] [CrossRef]
- Tamin, S.S.; Maleszewski, J.J.; Scott, C.G.; Khan, S.K.; Edwards, W.D.; Bruce, C.J.; Oh, J.K.; Pellikka, P.A.; Klarich, K.W. Prognostic and bioepidemiologic implications of papillary fibroelastomas. J. Am. Coll. Cardiol. 2015, 65, 2420–2429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zoltowska, D.M.; Sadic, E.; Becoats, K.; Ghetiya, S.; Ali, A.A.; Sattiraju, S.; Missov, E. Cardiac papillary fibroelastoma. J. Geriatr. Cardiol. 2021, 18, 346–351. [Google Scholar] [CrossRef]
- Strecker, T.; Scheuermann, S.; Nooh, E.; Weyand, M.; Agaimy, A. Incidental papillary fibroelastoma of the tricuspid valve. J. Cardiothorac. Surg. 2014, 9, 123. [Google Scholar] [CrossRef] [Green Version]
- Kurmann, R.D.; El-Am, E.A.; Sorour, A.A.; Ahmad, A.; Lee, A.T.; Scott, C.G.; Bois, M.C.; Maleszewski, J.J.; Klarich, K.W. Papillary fibroelastoma growth: A retrospective follow-up study of patients with pathology-proven papillary fibroelastoma. J. Am. Coll. Cardiol. 2021, 77, 2154–2155. [Google Scholar] [CrossRef]
- Klarich, K.W.; Enriquez-Sarano, M.; Gura, G.M.; Edwards, W.D.; Tajik, A.J.; Seward, J.B. Papillary fibroelastoma: Echocardiographic characteristics for diagnosis and pathologic correlation. J. Am. Coll. Cardiol. 1997, 30, 784–790. [Google Scholar] [CrossRef]
- Sun, J.P.; Asher, C.R.; Yang, X.S.; Cheng, G.G.; Scalia, G.M.; Massed, A.G.; Griffin, B.P.; Ratliff, N.B.; Stewart, W.J.; Thomas, J.D. Clinical and echocardiographic characteristics of papillary fibroelastomas: A retrospective and prospective study in 162 patients. Circulation 2001, 103, 2687–2693. [Google Scholar] [CrossRef] [Green Version]
- Singh, A.; Miller, A.P.; Nanda, N.C.; Rajdev, S.; Mehmood, F.; Duncan, K. Papillary fibroelastoma of the pulmonary valve: Assessment by live/real time three-dimensional transthoracic echocardiography. Echocardiography 2006, 23, 880–883. [Google Scholar] [CrossRef]
- Wintersperger, B.J.; Becker, C.R.; Gulbins, H.; Knez, A.; Bruening, R.; Heuck, A.; Reiser, M.F. Tumors of the cardiac valves: Imaging findings in magnetic resonance imaging, electron beam computed tomography, and echocardiography. Eur. Radiol. 2000, 10, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Hoey, E.T.; Shahid, M.; Ganeshan, A.; Baijal, S.; Simpson, H.; Watkin, R.W. Mri assessment of cardiac tumours: Part 1, multiparametric imaging protocols and spectrum of appearances of histologically benign lesions. Quant. Imaging Med. Surg. 2014, 4, 478–488. [Google Scholar] [CrossRef] [PubMed]
- Fang, L.; He, L.; Chen, Y.; Xie, M.; Wang, J. Infiltrating lipoma of the right ventricle involving the interventricular septum and tricuspid valve: Report of a rare case and literature review. Medicine 2016, 95, e2561. [Google Scholar] [CrossRef] [PubMed]
- D’Souza, J.; Shah, R.; Abbass, A.; Burt, J.R.; Goud, A.; Dahagam, C. Invasive cardiac lipoma: A case report and review of literature. BMC Cardiovasc. Disord. 2017, 17, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajiah, P.; Kanne, J.P.; Kalahasti, V.; Schoenhagen, P. Computed tomography of cardiac and pericardiac masses. J. Cardiovasc. Comput. Tomogr. 2011, 5, 16–29. [Google Scholar] [CrossRef]
- Mankad, R.; Herrmann, J. Cardiac tumors: Echo assessment. Echo Res. Pract. 2016, 3, R65–R77. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Zuo, Y.; Huang, Y.; Cao, L. Echocardiographical findings of giant cardiac lipoma: A case report. Medicine 2019, 98, e14456. [Google Scholar] [CrossRef]
- Shu, S.; Yuan, H.; Kong, X.; Wang, J.; Wang, J.; Zheng, C. The value of multimodality imaging in diagnosis and treatment of cardiac lipoma. BMC Med. Imaging 2021, 21, 71. [Google Scholar] [CrossRef]
- Silva-Sánchez, M.P.; Alvarado-Socarras, J.L.; Castro-Monsalve, J.; Meneses, K.M.; Santiago, J.; Prada, C.E. Everolimus for severe arrhythmias in tuberous sclerosis complex related cardiac rhabdomyomas. Am. J. Med. Genet. A 2021, 185, 1525–1531. [Google Scholar] [CrossRef]
- Ganame, J.; D’Hooge, J.; Mertens, L. Different deformation patterns in intracardiac tumors. Eur. J. Echocardiogr. 2005, 6, 461–464. [Google Scholar] [CrossRef]
- Torimitsu, S.; Nemoto, T.; Wakayama, M.; Okubo, Y.; Yokose, T.; Kitahara, K.; Ozawa, T.; Nakayama, H.; Shinozaki, M.; Sasai, D.; et al. Literature survey on epidemiology and pathology of cardiac fibroma. Eur. J. Med. Res. 2012, 17, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anwar, A.S.; Salem, M.I.; Beltagy, R.; Madi, K.; Elwatidy, A.M.F. Large left ventricular fibroma: Case report and literature review. Innovations 2020, 15, 283–285. [Google Scholar] [CrossRef] [PubMed]
- Lo Muzio, L. Nevoid basal cell carcinoma syndrome (gorlin syndrome). Orphanet. J. Rare Dis. 2008, 3, 32. [Google Scholar] [CrossRef] [Green Version]
- Araoz, P.A.; Mulvagh, S.L.; Tazelaar, H.D.; Julsrud, P.R.; Breen, J.F. Ct and mr imaging of benign primary cardiac neoplasms with echocardiographic correlation. Radiographics 2000, 20, 1303–1319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nwachukwu, H.; Li, A.; Nair, V.; Nguyen, E.; David, T.E.; Butany, J. Cardiac fibroma in adults. Cardiovasc. Pathol. 2011, 20, e146–e152. [Google Scholar] [CrossRef] [PubMed]
- Tao, T.Y.; Yahyavi-Firouz-Abadi, N.; Singh, G.K.; Bhalla, S. Pediatric cardiac tumors: Clinical and imaging features. Radiographics 2014, 34, 1031–1046. [Google Scholar] [CrossRef]
- Tella, S.H.; Jha, A.; Taïeb, D.; Horvath, K.A.; Pacak, K. Comprehensive review of evaluation and management of cardiac paragangliomas. Heart 2020, 106, 1202–1210. [Google Scholar] [CrossRef]
- Wan, J.; Li, W.; Zhou, Z.; Shang, J.; Chen, D. Primary cardiac paraganglioma with intratumoral coronary artery aneurysm. Ann. Thorac. Surg. 2014, 97, e75–e77. [Google Scholar] [CrossRef]
- Tomasian, A.; Lai, C.; Ruehm, S.; Krishnam, M.S. Cardiovascular magnetic resonance and pet-ct of left atrial paraganglioma. J. Cardiovasc. Magn. Reson. 2010, 12, 1. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Teng, P.; Xu, H.; Ma, L.; Ni, Y. Cardiac hemangioma: A comprehensive analysis of 200 cases. Ann. Thorac. Surg. 2015, 99, 2246–2252. [Google Scholar] [CrossRef]
- Miao, H.; Yang, W.; Zhou, M.; Zhu, Q.; Jiang, Z. Atrial hemangioma: A case report and review of the literature. Ann. Thorac. Cardiovasc. Surg. 2019, 25, 71–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tourmousoglou, C.; Nikoloudakis, N.; Kelpis, T.; Tsotsolis, N.; Ninios, V.; Kallifatidis, A.; Ninios, E.; Theofilogiannakos, E.K.; Thoma, M.; Asimaki, A.; et al. Left ventricular cardiac hemangioma. Am. J. Med. 2017, 130, e337–e339. [Google Scholar] [CrossRef] [PubMed]
- Brizard, C.; Latremouille, C.; Jebara, V.A.; Acar, C.; Fabiani, J.N.; Deloche, A.; Carpentier, A.F. Cardiac hemangiomas. Ann. Thorac. Surg. 1993, 56, 390–394. [Google Scholar] [CrossRef]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, Y.; Wu, W.; Gao, L.; Ji, M.; Xie, M.; Li, Y. Multimodality Imaging of Benign Primary Cardiac Tumor. Diagnostics 2022, 12, 2543. https://doi.org/10.3390/diagnostics12102543
Lin Y, Wu W, Gao L, Ji M, Xie M, Li Y. Multimodality Imaging of Benign Primary Cardiac Tumor. Diagnostics. 2022; 12(10):2543. https://doi.org/10.3390/diagnostics12102543
Chicago/Turabian StyleLin, Yixia, Wenqian Wu, Lang Gao, Mengmeng Ji, Mingxing Xie, and Yuman Li. 2022. "Multimodality Imaging of Benign Primary Cardiac Tumor" Diagnostics 12, no. 10: 2543. https://doi.org/10.3390/diagnostics12102543