
Dual-Energy CT for Accurate Discrimination of Intraperitoneal Hematoma and Intestinal Structures
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
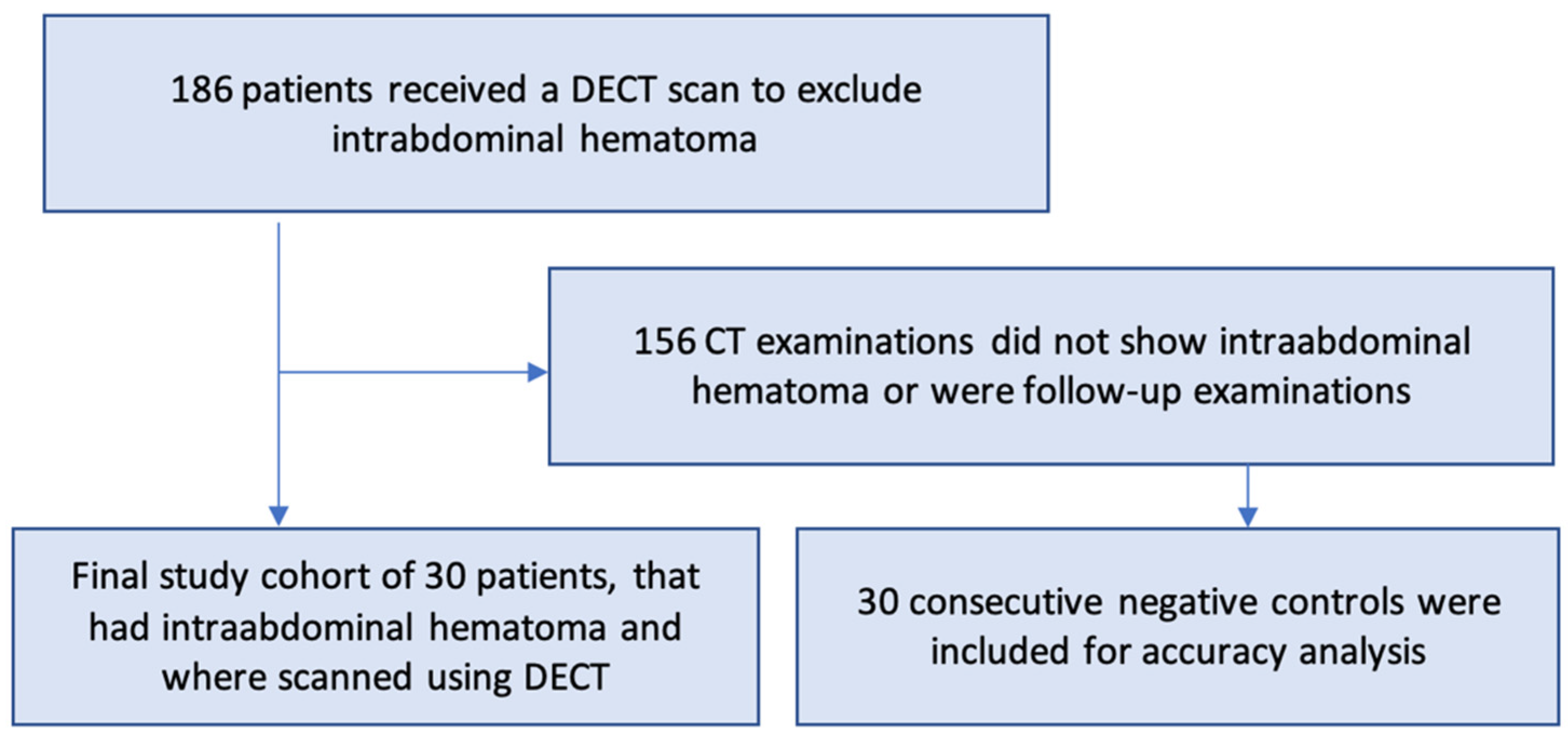
2.1. Patient Population
2.2. Reference Standard
2.3. Acquisition Parameters
2.4. Subjective Image Analysis
2.4.1. Diagnostic Performance
2.4.2. Diagnostic Confidence
2.5. Objective DECT Image Analysis
2.6. Statistics
3. Results
3.1. Subjective Image Analysis
3.1.1. Diagnostic Performance
3.1.2. Diagnostic Confidence
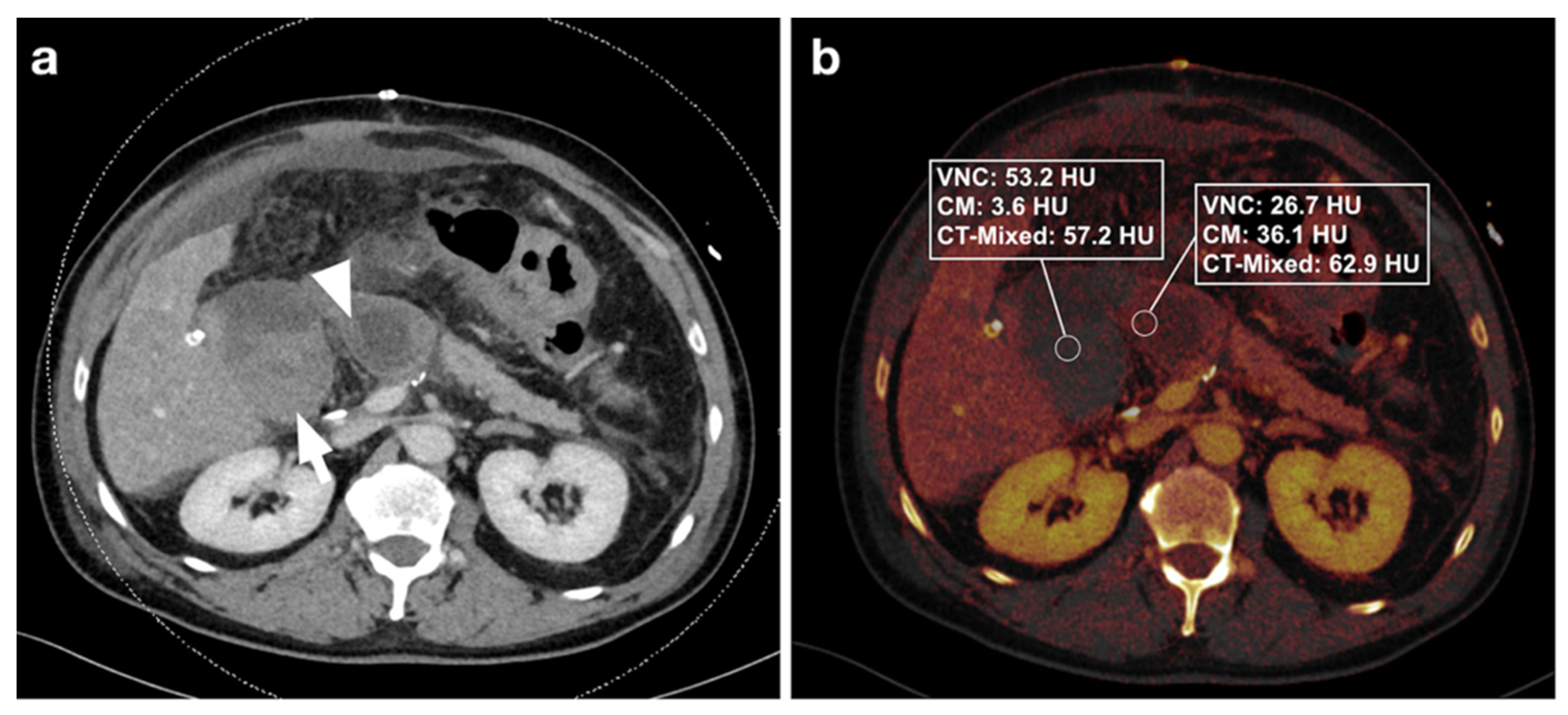
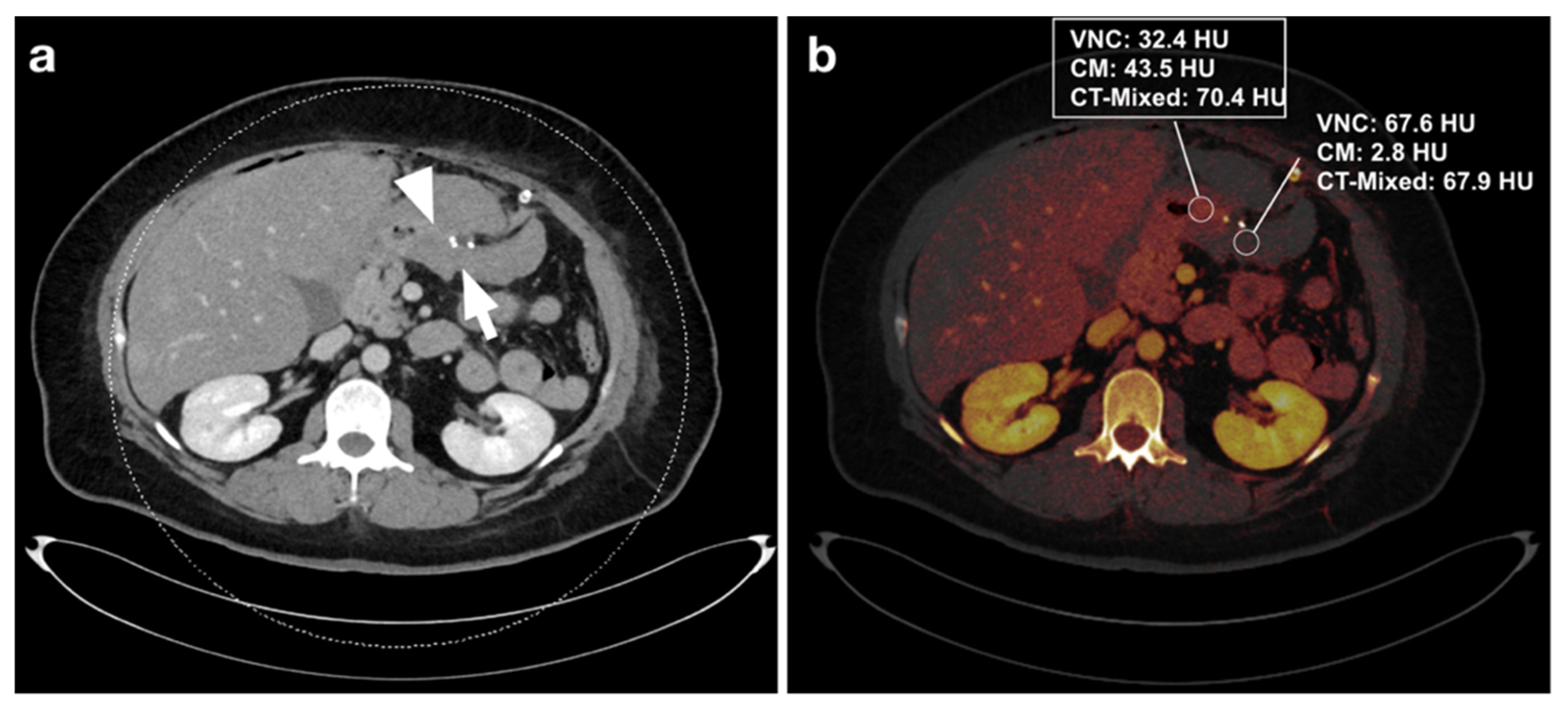
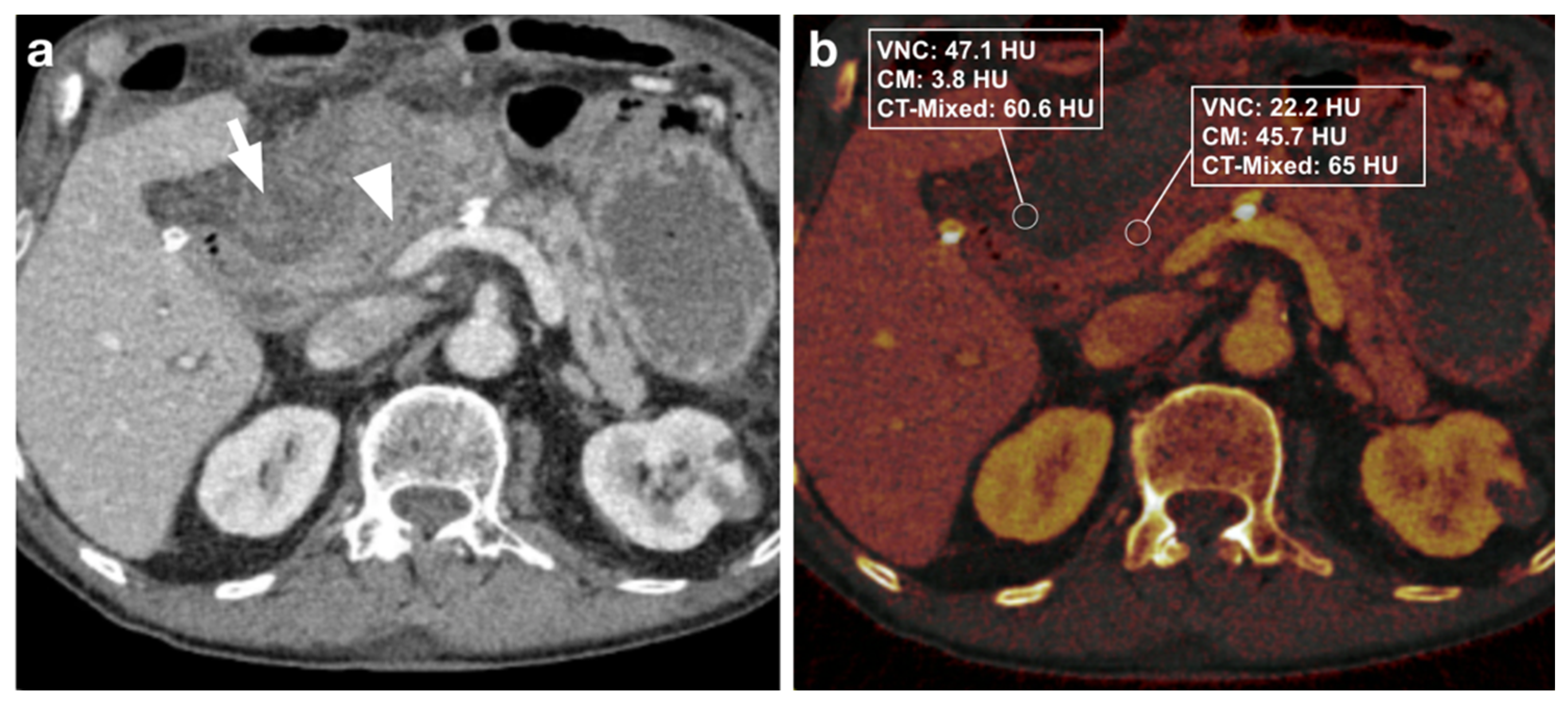
3.2. Objective Image Analysis
3.2.1. DECT Image Analysis
3.2.2. Diagnostic Performance
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lucey, B.C.; Varghese, J.C.; Soto, J.A. Spontaneous hemoperitoneum: Causes and significance. Curr. Probl. Diagn. Radiol. 2005, 34, 182–195. [Google Scholar] [CrossRef] [PubMed]
- Mondie, C.; Maguire, N.J.; Rentea, R.M. Retroperitoneal Hematoma. In StatPearls; StatPearls Publishing Copyright© 2021; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2021. [Google Scholar]
- Queiroz, R.M.; Filho, F.B. Spontaneous hematoma of the rectus sheath following percutaneous transluminal coronary angioplasty and stent placement. Pan. Afr. Med. J. 2018, 30, 88. [Google Scholar] [CrossRef] [PubMed]
- Ng, A.K.T.; Simons, R.K.; Torreggiani, W.C.; Ho, S.G.F.; Kirkpatrick, A.W.; Brown, D.R.G. Intra-abdominal Free Fluid without Solid Organ Injury in Blunt Abdominal Trauma: An Indication for Laparotomy. J. Trauma Acute Care Surg. 2002, 52, 1134–1140. [Google Scholar] [CrossRef] [PubMed]
- Kirshtein, B.; Domchik, S.; Mizrahi, S.; Lantsberg, L. Laparoscopic diagnosis and treatment of postoperative complications. Am. J. Surg. 2009, 197, 19–23. [Google Scholar] [CrossRef]
- Sierra, A.; Ecochard-Dugelay, E.; Bellaïche, M.; Tilea, B.; Cavé, H.; Viala, J. Biopsy-Induced Duodenal Hematoma Is Not an Infrequent Complication Favored by Bone Marrow Transplantation. J. Pediatric Gastroenterol. Nutr. 2016, 63, 627–632. [Google Scholar] [CrossRef]
- Niehues, S.M.; Denecke, T.; Bassir, C.; Hamm, B.; Haas, M. Intramural duodenal hematoma: Clinical course and imaging findings. Acta Radiol. Open 2019, 8, 2058460119836256. [Google Scholar] [CrossRef] [Green Version]
- Jarufe, N.; Figueroa, E.; Muñoz, C.; Moisan, F.; Varas, J.; Valbuena, J.R.; Bambs, C.; Martínez, J.; Pimentel, F. Anatomic hepatectomy as a definitive treatment for hepatolithiasis: A cohort study. HPB 2012, 14, 604–610. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, M.; Zimmermann, M.; Meyer, R.; Laubert, T.; Begum, N.; Keck, T.; Kujath, P.; Schloericke, E. Spontaneous and non-spontaneous bleeding complications in patients with oral vitamin K antagonist therapy. Langenbeck’s Arch. Surg. 2014, 399, 99–107. [Google Scholar] [CrossRef]
- Hamidian Jahromi, A.; Johnson, L.; Youssef, A.M. Delayed small bowel perforation following blunt abdominal trauma: A case report and review of the literature. Asian J. Surg. 2016, 39, 109–112. [Google Scholar] [CrossRef] [Green Version]
- Olivier-Cabrera, S.; Tewari, V.; Gollapudi, L.; Stringel, G. Endoscopic drainage of a symptomatic intraperitoneal hematoma with a metal stent and intracavitary thrombolytics. CRSLS 2020, e2020.00055. [Google Scholar] [CrossRef]
- Kasotakis, G. Spontaneous hemoperitoneum. Surg. Clin. N. Am. 2014, 94, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Zissin, R.; Ellis, M.; Gayer, G. The CT Findings of Abdominal Anticoagulant-Related Hematomas. Semin. Ultrasound. CT MRI 2006, 27, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Lubner, M.; Menias, C.; Rucker, C.; Bhalla, S.; Peterson, C.M.; Wang, L.; Gratz, B. Blood in the Belly: CT Findings of Hemoperitoneum. RadioGraphics 2007, 27, 109–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, M.E.; Walter, J.; Obuchowski, N.A.; Achkar, J.-P.; Einstein, D.; Veniero, J.C.; Vogel, J.; Stocchi, L. Mural Attenuation in Normal Small Bowel and Active Inflammatory Crohn’s Disease on CT Enterography: Location, Absolute Attenuation, Relative Attenuation, and the Effect of Wall Thickness. Am. J. Roentgenol. 2009, 192, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Goo, H.W.; Goo, J.M. Dual-energy CT: New horizon in medical imaging. Korean J. Radiol. 2017, 18, 555–569. [Google Scholar] [CrossRef] [Green Version]
- Johnson, T.R.; Krauss, B.; Sedlmair, M.; Grasruck, M.; Bruder, H.; Morhard, D.; Fink, C.; Weckbach, S.; Lenhard, M.; Schmidt, B. Material differentiation by dual energy CT: Initial experience. Eur. Radiol. 2007, 17, 1510–1517. [Google Scholar] [CrossRef]
- Sofue, K.; Itoh, T.; Takahashi, S.; Schmidt, B.; Shimada, R.; Negi, N.; Sugimura, K.; Murakami, T. Quantification of cisplatin using a modified 3-material decomposition algorithm at third-generation dual-source dual-energy computed tomography: An experimental study. Investig. Radiol. 2018, 53, 673–680. [Google Scholar] [CrossRef]
- Martin, S.S.; Trapp, F.; Wichmann, J.L.; Albrecht, M.H.; Lenga, L.; Durden, J.; Booz, C.; Vogl, T.J.; D’Angelo, T. Dual-energy CT in early acute pancreatitis: Improved detection using iodine quantification. Eur. Radiol. 2019, 29, 2226–2232. [Google Scholar] [CrossRef]
- Mileto, A.; Marin, D.; Alfaro-Cordoba, M.; Ramirez-Giraldo, J.C.; Eusemann, C.D.; Scribano, E.; Blandino, A.; Mazziotti, S.; Ascenti, G. Iodine quantification to distinguish clear cell from papillary renal cell carcinoma at dual-energy multidetector CT: A multireader diagnostic performance study. Radiology 2014, 273, 813–820. [Google Scholar] [CrossRef]
- Kaltenbach, B.; Wichmann, J.L.; Pfeifer, S.; Albrecht, M.H.; Booz, C.; Lenga, L.; Hammerstingl, R.; D’Angelo, T.; Vogl, T.J.; Martin, S.S. Iodine quantification to distinguish hepatic neuroendocrine tumor metastasis from hepatocellular carcinoma at dual-source dual-energy liver CT. Eur. J. Radiol. 2018, 105, 20–24. [Google Scholar] [CrossRef]
- Winkelmann, M.T.; Gassenmaier, S.; Walter, S.S.; Artzner, C.; Lades, F.; Faby, S.; Nikolaou, K.; Bongers, M.N. Differentiation of adrenal adenomas from adrenal metastases in single-phased staging dual-energy CT and radiomics. Diagn. Interv. Radiol. 2022, 28, 208–216. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.; Shin, N.Y.; Jang, J.; Ahn, K.J.; Kim, B.S. Dual-energy CT for differentiating acute intracranial hemorrhage from contrast staining or calcification: A meta-analysis. Neuroradiology 2020, 62, 1617–1626. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.Y.; Zhang, S.H.; Xie, Q.Z.; Yin, Z.J.; Liu, Q.Y.; Zhao, M.D.; Li, X.L.; Mao, X.J. Evaluation of Virtual Noncontrast Images Obtained from Dual-Energy CTA for Diagnosing Subarachnoid Hemorrhage. AJNR Am. J. Neuroradiol. 2015, 36, 855–860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trabzonlu, T.A.; Mozaffary, A.; Kim, D.; Yaghmai, V. Dual-energy CT evaluation of gastrointestinal bleeding. Abdom. Radiol. 2020, 45, 1–14. [Google Scholar] [CrossRef]
- Hamid, S.; Nicolaou, S.; Khosa, F.; Andrews, G.; Murray, N.; Abdellatif, W.; Qamar, S.R. Dual-Energy CT: A Paradigm Shift in Acute Traumatic Abdomen. Can. Assoc. Radiol. J. 2020, 71, 371–387. [Google Scholar] [CrossRef] [Green Version]
- Walter, S.S.; Schneeweiß, S.; Maurer, M.; Kraus, M.S.; Wichmann, J.L.; Bongers, M.N.; Lescan, M.; Bamberg, F.; Othman, A.E. Virtual non-enhanced dual-energy CT reconstruction may replace true non-enhanced CT scans in the setting of suspected active hemorrhage. Eur. J. Radiol. 2018, 109, 218–222. [Google Scholar] [CrossRef]
- Rizzo, S.; Radice, D.; Femia, M.; De Marco, P.; Origgi, D.; Preda, L.; Barberis, M.; Vigorito, R.; Mauri, G.; Mauro, A.; et al. Metastatic and non-metastatic lymph nodes: Quantification and different distribution of iodine uptake assessed by dual-energy CT. Eur. Radiol. 2018, 28, 760–769. [Google Scholar] [CrossRef]
- Shaqdan, K.W.; Parakh, A.; Kambadakone, A.R.; Sahani, D.V. Role of dual energy CT to improve diagnosis of non-traumatic abdominal vascular emergencies. Abdom. Radiol. 2019, 44, 406–421. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | N | % | N | % |
|---|---|---|---|---|
| Study cohort | Negative control group | |||
| No. of patients | 30 | 30 * | ||
| Age, years, mean ± SD | 64.5 ± 15.1 years | 62.3 ± 13.2 years * | ||
| Gender | ||||
| Male | 19 | 63 | 18 | 60 * |
| Female | 11 | 37 | 12 | 40 * |
| Causes of intra-abdominal hematoma | ||||
| Post-surgical | 19 | 63 | ||
| Infection/tumor disease | 5 | 17 | ||
| Traumatic Spontaneous development | 3 3 | 10 10 | ||
| Sensitivity (95% CI) | Specificity (95% CI) | PPV (95% CI) | NPV (95% CI) | ||
|---|---|---|---|---|---|
| Reader 1 | DE-LB | 90.9% (74.5–97.6) | 100% (85.9–100) | 100% (0.85–1) | 90.1 (74.5–97.6) |
| IM | 100% (85.9–100) | 100% (85.9–100) | 100% (85.9–100) | 100% (85.9–100) | |
| Reader 2 | DE-LB | 88.2% (71.6–96.2) | 96.7% (82.5–99.8) | 96.7% (0.82–0.99) | 88.2% (71.6–96.2) |
| IM | 96.7 (81.5–99.8) | 100% (85.9–100) | 100% (85.9–100) | 96.7 (81.5–99.8) | |
| Reader 3 | DE-LB | 96.7 (81.5–99.8) | 100% (85.9–100) | 100% (85.9–100) | 96.7 (81.5–99.8) |
| IM | 100% (85.9–100) | 100% (85.9–100) | 100% (85.9–100) | 100 (85.9–100) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Winkelmann, M.T.; Hagen, F.; Artzner, K.; Bongers, M.N.; Artzner, C. Dual-Energy CT for Accurate Discrimination of Intraperitoneal Hematoma and Intestinal Structures. Diagnostics 2022, 12, 2542. https://doi.org/10.3390/diagnostics12102542
Winkelmann MT, Hagen F, Artzner K, Bongers MN, Artzner C. Dual-Energy CT for Accurate Discrimination of Intraperitoneal Hematoma and Intestinal Structures. Diagnostics. 2022; 12(10):2542. https://doi.org/10.3390/diagnostics12102542
Chicago/Turabian StyleWinkelmann, Moritz T., Florian Hagen, Kerstin Artzner, Malte N. Bongers, and Christoph Artzner. 2022. "Dual-Energy CT for Accurate Discrimination of Intraperitoneal Hematoma and Intestinal Structures" Diagnostics 12, no. 10: 2542. https://doi.org/10.3390/diagnostics12102542