
Difference in Procedure-Related Risk of Miscarriage between Early and Mid-Trimester Amniocentesis: A Retrospective Cohort Study



Abstract
:1. Introduction
2. Materials and Methods
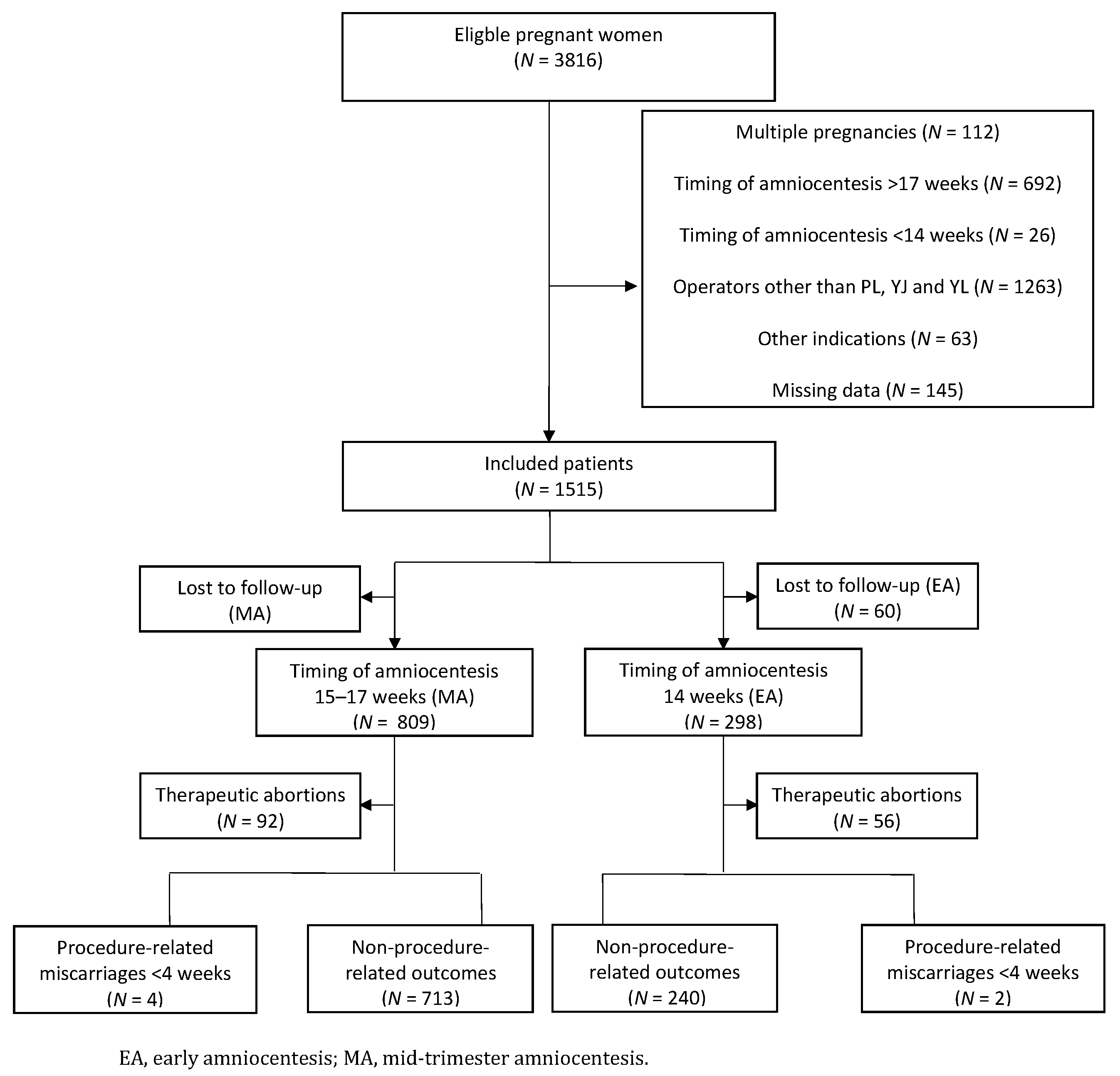
- Timing of the procedure (EA at 14 and MA at 15–17 gestational weeks)
- Final pregnancy outcome (procedure-related miscarriages <4 weeks after amniocentesis, non-procedure-related outcomes, live births and therapeutic abortions)
- Indication of amniocentesis (ultrasound abnormality, positive serum screening, abnormal first-trimester screening, genetic disorder in family history, genetic disorder in previous pregnancy, maternal age, personal request, abnormal NIPT and abnormal chorionic villus sampling)
- Genetic results (trisomy 21, 18, 13 or others)
- Maternal age
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Committee on Practice Bulletins—Obstetrics, Committee on Genetics, and Society for Maternal–Fetal Medicine. Practice Bulletin No. 162: Prenatal Diagnostic Testing for Genetic Disorders. Obstet. Gynecol. 2016, 127, e108–e122. [Google Scholar] [CrossRef] [PubMed]
- Tabor, A.; Philip, J.; Madsen, M.; Bang, J.; Obel, E.B.; Norgaard-Pedersen, B. Randomised controlled trial of genetic amniocentesis in 4606 low-risk women. Lancet 1986, 1, 1287–1293. [Google Scholar] [CrossRef]
- Alfirevic, Z.; Navaratnam, K.; Mujezinovic, F. Amniocentesis and Chorionic Villus Sampling. R. Coll. Obstet. Gynaecol. 2010, 8, 2–6. [Google Scholar]
- Akolekar, R.; Beta, J.; Picciarelli, G.; Ogilvie, C.; D’Antonio, F. Procedure-related risk of miscarriage following amniocentesis and chorionic villus sampling: A systematic review and meta-analysis. Ultrasound Obs. Gynecol 2015, 45, 16–26. [Google Scholar] [CrossRef]
- Ghi, T.; Sotiriadis, A.; Calda, P.; Da Silva Costa, F.; Raine-Fenning, N.; Alfirevic, Z.; McGillivray, G.; International Society of Ultrasound in Obstetrics and Gynecology. ISUOG Practice Guidelines: Invasive procedures for prenatal diagnosis. Ultrasound Obs. Gynecol 2016, 48, 256–268. [Google Scholar] [CrossRef]
- Jauniaux, E.; Pahal, G.S.; Rodeck, C.H. What invasive procedure to use in early pregnancy? Baillieres Best Pr. Res. Clin. Obs. Gynaecol. 2000, 14, 651–662. [Google Scholar] [CrossRef]
- Philip, J.; Silver, R.K.; Wilson, R.D.; Thom, E.A.; Zachary, J.M.; Mohide, P.; Mahoney, M.J.; Simpson, J.L.; Platt, L.D.; Pergament, E.; et al. Late first-trimester invasive prenatal diagnosis: Results of an international randomized trial. Obs. Gynecol. 2004, 103, 1164–1173. [Google Scholar] [CrossRef]
- The Canadian Early and Mid-trimester Amniocentesis Trial (CEMAT) Group. Randomised trial to assess safety and fetal outcome of early and midtrimester amniocentesis. Lancet 1998, 351, 242–247. [Google Scholar] [CrossRef]
- Sundberg, K.; Bang, J.; Smidt-Jensen, S.; Brocks, V.; Lundsteen, C.; Parner, J.; Keiding, N.; Philip, J. Randomised study of risk of fetal loss related to early amniocentesis versus chorionic villus sampling. Lancet 1997, 350, 697–703. [Google Scholar] [CrossRef]
- Tabor, A.; Alfirevic, Z. Update on procedure-related risks for prenatal diagnosis techniques. Fetal Diagn. Ther. 2010, 27, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Mujezinovic, F.; Alfirevic, Z. Procedure-related complications of amniocentesis and chorionic villous sampling: A systematic review. Obs. Gynecol. 2007, 110, 687–694. [Google Scholar] [CrossRef] [PubMed]
- Loquet, P.F.A.; Hauspy, J.; Kollen, M.; Vegter, M.; Dirks, M. The Psychological Advantages of Advancing the Gestational age for Amniocentesis. In Proceedings of the 1st World Congress on Ultrasound in Obstetrics and Gynecology, London, UK, 6–10 January 1991. [Google Scholar]
- Wilson, R.D.; Gagnon, A.; Audibert, F.; Campagnolo, C.; Carroll, J.; Genetics, C. Prenatal Diagnosis Procedures and Techniques to Obtain a Diagnostic Fetal Specimen or Tissue: Maternal and Fetal Risks and Benefits. J. Obs. Gynaecol. Can. 2015, 37, 656–668. [Google Scholar] [CrossRef]
- Wilson, R.D.; Johnson, J.; Windrim, R.; Dansereau, J.; Singer, J.; Winsor, E.J.; Kalousek, D. The early amniocentesis study: A randomized clinical trial of early amniocentesis and midtrimester amniocentesis. II. Evaluation of procedure details and neonatal congenital anomalies. Fetal Diagn. Ther. 1997, 12, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.D.; Langlois, S.; Johnson, J.A.; Sogc Genetics, C.; SOGC Genetics Committee; CCMG Prenatal Diagnosis Committee. Mid-trimester amniocentesis fetal loss rate. J. Obs. Gynaecol. Can. 2007, 29, 586–590. [Google Scholar] [CrossRef]
- Johnson, J.M.; Wilson, R.D.; Singer, J.; Winsor, E.; Harman, C.; Armson, B.A.; Benzie, R.; Dansereau, J.; Ho, M.F.; Mohide, P.; et al. Technical factors in early amniocentesis predict adverse outcome. Results of the Canadian Early (EA) versus Mid-trimester (MA) Amniocentesis Trial. Prenat. Diagn. 1999, 19, 732–738. [Google Scholar] [CrossRef]
- Vanakker, O.; Vilain, C.; Janssens, K.; Van der Aa, N.; Smits, G.; Bandelier, C.; Blaumeiser, B.; Bulk, S.; Caberg, J.H.; De Leener, A.; et al. Implementation of genomic arrays in prenatal diagnosis: The Belgian approach to meet the challenges. Eur. J. Med. Genet. 2014, 57, 151–156. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| MA (n = 809) (%) | EA (n = 298) (%) | |
|---|---|---|
| 14 + 0 | 32 (10.74) | |
| 14 + 1 | 25 (8.39) | |
| 14 + 2 | 34 (11.40) | |
| 14 + 3 | 35 (11.74) | |
| 14 + 4 | 53 (17.79) | |
| 14 + 5 | 60 (20.13) | |
| 14 + 6 | 59 (19.80) | |
| 150–156 | 490 (60.57) | |
| 160–166 | 228 (28.18) | |
| 170–176 | 91 (11.25) | |
| Mean gestational age | 15 + 6 | 14 + 4 |
| MA (%) | EA (%) | ||
|---|---|---|---|
| Genetic results | Normal | 720 (89.00) | 238 (79.87) |
| Trisomy 21 | 46 (5.69) | 38 (12.75) | |
| Trisomy 13 | 1 (0.14) | 1 (0.34) | |
| Trisomy 18 | 5 (0.62) | 2 (0.67) | |
| Others | 37 (4.57) | 19 (6.36) | |
| Indication of amniocentesis | Ultrasound abnormality | 134 (16.56) | 58 (19.46) |
| Positive serum screening | 247 (30.53) | 67 (22.48) | |
| Abnormal first-trimester screening | 48 (5.93) | 23 (7.72) | |
| Genetic disorder in family history | 36 (4.45) | 13 (4.36) | |
| Genetic disorder in previous pregnancies | 52 (6.43) | 16 (5.37) | |
| Maternal age | 212 (26.21) | 76 (25.50) | |
| Personal request | 40 (4.94) | 7 (2.35) | |
| Abnormal NIPT | 34 (4.20) | 34 (11.41) | |
| Inconclusive NIPT | 5 (0.62) | 2 (0.67) | |
| Abnormal CVS | 1 (0.14) | 2 (0.67) | |
| Age (years) | <35 | 414 (51.17) | 151 (50.67) |
| ≥35 | 395 (48.83) | 147 (49.33) |
| MA (%) | EA (%) | ||
|---|---|---|---|
| Procedure-related risk of miscarriage (<4 weeks) | Yes | 4 (0.36) | 2 (0.82) |
| No | 713 (99.44) | 240 (99.17) | |
| Non-procedure-related risk of outcome | Live births | 705 (98.33) | 239 (98.76) |
| Miscarriage >4 weeks after the procedure | 8 (0.11) | 1 (0.41) | |
| Total | 717 | 242 | |
| Therapeutic abortions | 92 | 56 |
| Gestational Age | Indication AC | Result AC | Subjective Procedure Information | Miscarriage | |
|---|---|---|---|---|---|
| MA1 | 17w1d | Ultrasound abnormality | Normal | Easy Procedure | MUI not further specified |
| MA2 | 15w2d | Abnormal first trimester screening | Normal | Not described | MUI not further specified |
| MA3 | 15w5d | Ultrasound abnormality | Normal | Uncomplicated procedure | MUI not further specified |
| MA4 | 15w0d | Abnormal First trimester screening | Normal | Easy procedure | Chorioamnionitis with premature labor |
| EA1 | 14w3d | Maternal Age | Normal | Not described | PPROM—Anhydramnion |
| EA2 | 14w1d | Maternal Age | Normal | Not described | Vaginal blood loss—PPROM |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steinfort, K.; Van Houtven, E.; Jacquemyn, Y.; Blaumeiser, B.; Loquet, P. Difference in Procedure-Related Risk of Miscarriage between Early and Mid-Trimester Amniocentesis: A Retrospective Cohort Study. Diagnostics 2021, 11, 1098. https://doi.org/10.3390/diagnostics11061098
Steinfort K, Van Houtven E, Jacquemyn Y, Blaumeiser B, Loquet P. Difference in Procedure-Related Risk of Miscarriage between Early and Mid-Trimester Amniocentesis: A Retrospective Cohort Study. Diagnostics. 2021; 11(6):1098. https://doi.org/10.3390/diagnostics11061098
Chicago/Turabian StyleSteinfort, Kelly, Ellen Van Houtven, Yves Jacquemyn, Bettina Blaumeiser, and Philip Loquet. 2021. "Difference in Procedure-Related Risk of Miscarriage between Early and Mid-Trimester Amniocentesis: A Retrospective Cohort Study" Diagnostics 11, no. 6: 1098. https://doi.org/10.3390/diagnostics11061098