
The Prevalence of High- and Low-Risk Types of HPV in Patients with Squamous Cell Carcinoma of the Head and Neck, Patients with Chronic Tonsillitis, and Healthy Individuals Living in Poland

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Specimen Collection
2.2. HNSCC Group
2.3. Chronic Tonsillitis Group
2.4. Control Group
2.5. DNA Preparation
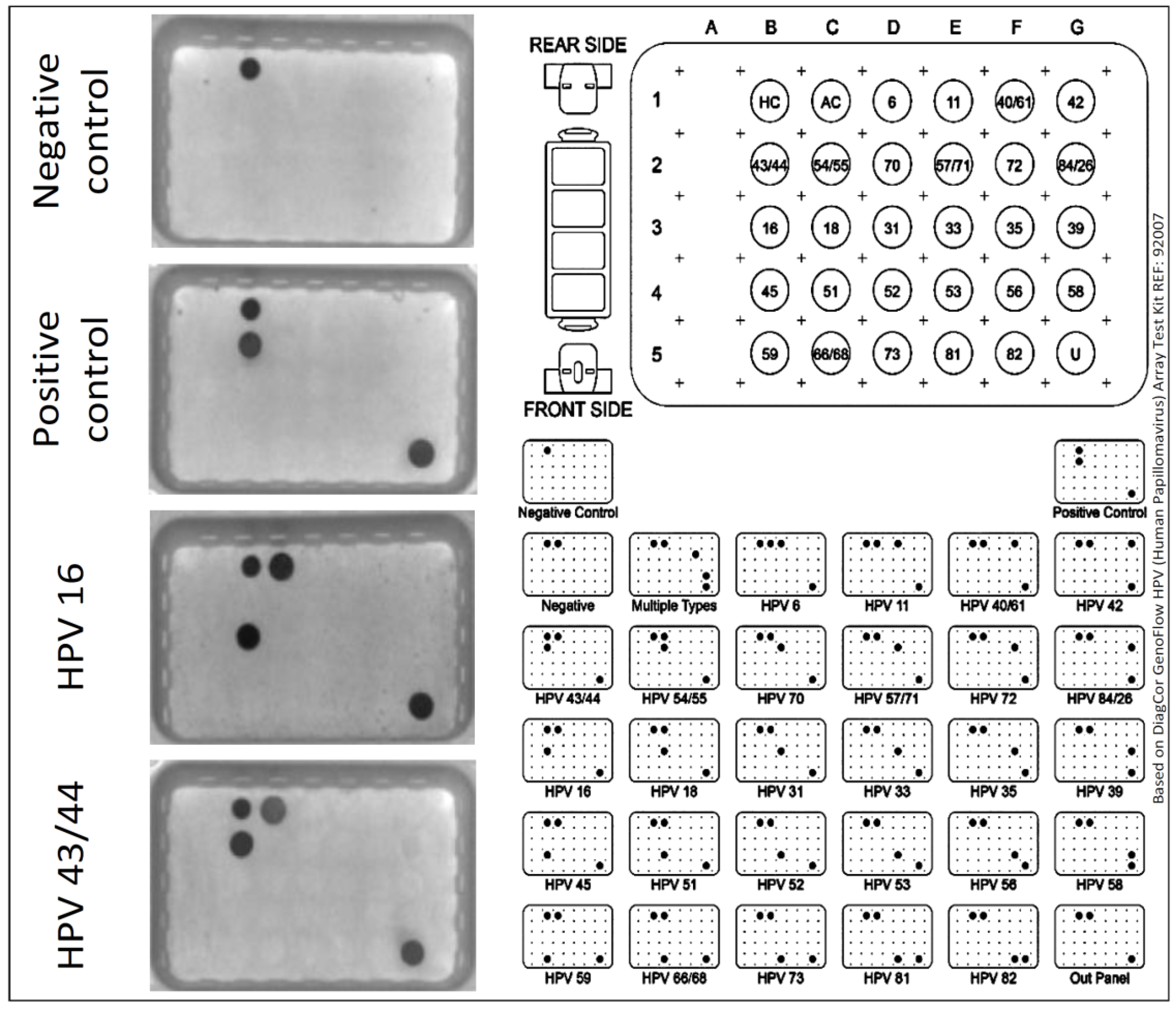
2.6. HPV Detection and Type Determination
2.7. Statistical Analysis
3. Results
3.1. HPV Prevalence and Its Genotypes in All Study Groups
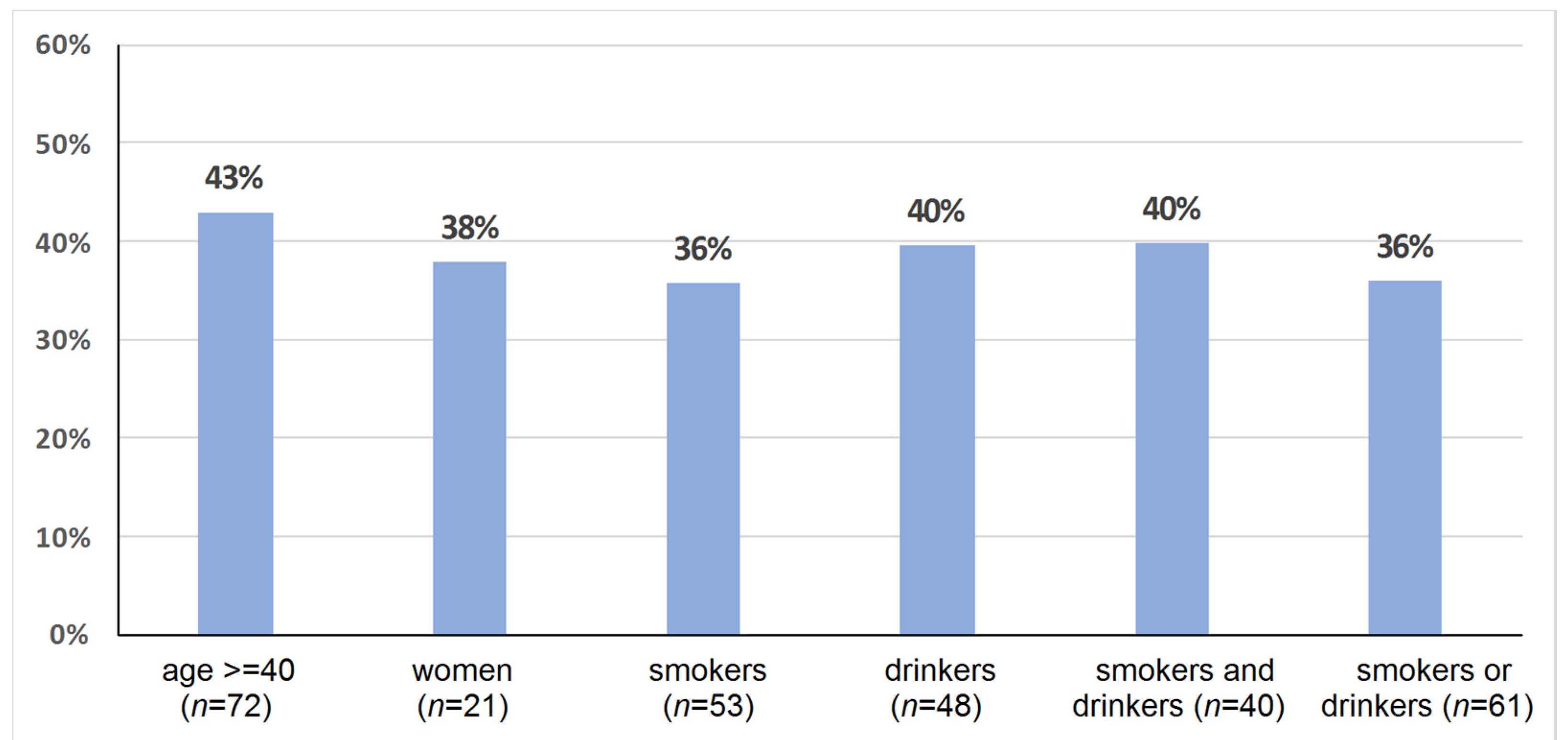
3.2. HPV Prevalence and Its Genotypes, Demographic Parameters, and Smoking and Drinking in All Study Groups
3.3. Associations of HPV Status and Its Genotype, Tumor Localization, TNM and Grading in HNSCC Cases
4. Discussion
4.1. HPV Infection in HNSCC
4.2. HPV Infection in Chronic Tonsillitis
4.3. HPV Infection in Healthy Individuals
4.4. Relevance to Vaccination Programs
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Golusiński, W.; Leemans, C.R.; Dietz, A. HPV Infection in Head and Neck Cancer, 1st ed.; Springer: Cham, Switzerland, 2017; pp. 4–18, 58, 73–78, 113–123. [Google Scholar] [CrossRef]
- Castellsagué, X. Natural history and epidemiology of HPV infection and cervical cancer. Gynecol. Oncol. 2008, 110 (Suppl. 2), S4–S7. [Google Scholar] [CrossRef] [PubMed]
- de Villiers, E.M. Cross-roads in the classification of papillomaviruses. Virology 2013, 445, 2–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gheit, T. Mucosal and Cutaneous Human Papillomavirus Infections and Cancer Biology. Front. Oncol. 2019, 9, 355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rooper, L.M.; Windon, M.J.; Hernandez, T.; Miles, B.; Ha, P.K.; Ryan, W.R.; Van Zante, A.; Eisele, D.W.; D’Souza, G.; Fakhry, C.; et al. HPV-positive Squamous Cell Carcinoma of the Larynx, Oral Cavity, and Hypopharynx: Clinicopathologic Characterization With Recognition of a Novel Warty Variant. Am. J. Surg. Pathol. 2020, 44, 691–702. [Google Scholar] [CrossRef]
- Franceschi, S.; Muñoz, N.; Snijders, P.J. How strong and how wide is the link between HPV and oropharyngeal cancer? Lancet 2000, 356, 871–872. [Google Scholar] [CrossRef]
- Smith, E.M.; Ritchie, J.M.; Summersgill, K.F.; Hoffman, H.T.; Wang, D.H.; Haugen, T.H.; Turek, L.P. Human papillomavirus in oral exfoliated cells and risk of head and neck cancer. J. Natl. Cancer Inst. 2004, 96, 449–455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kreimer, A.R.; Clifford, G.M.; Boyle, P.; Franceschi, S. Human papillomavirus types in head and neck squamous cell carcinomas worldwide: A systematic review. Cancer Epidemiol. Biomark. Prev. 2005, 14, 467–475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaturvedi, A.K. Epidemiology and clinical aspects of HPV in head and neck cancers. Head Neck Pathol. 2012, 6 (Suppl. 1), S16–S24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaturvedi, A.K.; Anderson, W.F.; Lortet-Tieulent, J.; Curado, M.P.; Ferlay, J.; Franceschi, S.; Rosenberg, P.S.; Bray, F.; Gillison, M.L. Worldwide trends in incidence rates for oral cavity and oropharyngeal cancers. J. Clin. Oncol. 2013, 31, 4550–4559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Syrjänen, S. Human papillomavirus infections and oral tumors. Med. Microbiol. Immunol. 2003, 192, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, P.C.; Miguel, M.C.; Bagordakis, E.; Fonseca, F.P.; de Aquino, S.N.; Santos-Silva, A.R.; Lopes, M.A.; Graner, E.; Salo, T.; Kowalski, L.P.; et al. Clinicopathological prognostic factors of oral tongue squamous cell carcinoma: A retrospective study of 202 cases. Int. J. Oral. Maxillofac. Surg. 2014, 43, 795–801. [Google Scholar] [CrossRef] [PubMed]
- Argiris, A.; Karamouzis, M.V.; Raben, D.; Ferris, R.L. Head and neck cancer. Lancet 2008, 371, 1695–1709. [Google Scholar] [CrossRef]
- Fakhry, C.; Westra, W.H.; Li, S.; Cmelak, A.; Ridge, J.A.; Pinto, H.; Forastiere, A.; Gillison, M.L. Improved survival of patients with human papillomavirus-positive head and neck squamous cell carcinoma in a prospective clinical trial. J. Natl. Cancer Inst. 2008, 100, 261–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gillison, M.L.; Koch, W.M.; Capone, R.B.; Spafford, M.; Westra, W.H.; Wu, L.; Zahurak, M.L.; Daniel, R.W.; Viglione, M.; Symer, D.E.; et al. Evidence for a causal association between human papillomavirus and a subset of head and neck cancers. J. Natl. Cancer Inst. 2000, 92, 709–720. [Google Scholar] [CrossRef]
- Huang, S.H.; O’Sullivan, B. Overview of the 8th Edition TNM Classification for Head and Neck Cancer. Curr. Treat. Options Oncol. 2017, 18, 40. [Google Scholar] [CrossRef] [PubMed]
- Schwentner, I.; Höfer, S.; Schmutzhard, J.; Deibl, M.; Sprinzl, G.M. Impact of tonsillectomy on quality of life in adults with chronic tonsillitis. Swiss Med. Wkly. 2007, 137, 454–461. [Google Scholar]
- Darrow, D.H.; Siemens, C. Indications for tonsillectomy and adenoidectomy. Laryngoscope 2002, 112, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Plank, L. Tonsillitis, Chronic. In Head and Neck Pathology. Encyclopedia of Pathology; Volavšek, M., Ed.; Springer: Cham, Switzerland, 2016; pp. 485–489. [Google Scholar] [CrossRef]
- Abu Bakar, M.; McKimm, J.; Haque, S.Z.; Majumder, M.A.A.; Haque, M. Chronic tonsillitis and biofilms: A brief overview of treatment modalities. J. Inflamm. Res. 2018, 11, 329–337. [Google Scholar] [CrossRef] [Green Version]
- Baumann, I.; Kucheida, H.; Blumenstock, G.; Zalaman, I.M.; Maassen, M.M.; Plinkert, P.K. Benefit from tonsillectomy in adult patients with chronic tonsillitis. Eur. Arch. Otorhinolaryngol. 2006, 263, 556–559. [Google Scholar] [CrossRef]
- TIBCO Software Inc. Tatistica (Data Analysis Software System), Version 13. 2017. Available online: http://statistica.io (accessed on 15 July 2021).
- Combes, J.D.; Clavel, C.; Dalstein, V.; Gheit, T.; Clifford, G.M.; Tommasino, M.; Franceschi, S.; Lacau, S.; Guily, J.; SPLIT Study Group. Human papillomavirus detection in gargles, tonsil brushings, and frozen tissues in cancer-free patients. Oral. Oncol. 2018, 82, 34–36. [Google Scholar] [CrossRef]
- Egawa, N.; Doorbar, J. The low-risk papillomaviruses. Virus Res. 2017, 231, 119–127. [Google Scholar] [CrossRef]
- Pannone, G.; Santoro, A.; Carinci, F.; Bufo, P.; Papagerakis, S.M.; Rubini, C.; Campisi, G.; Giovannelli, L.; Contaldo, M.; Serpico, R.; et al. Double demonstration of oncogenic high risk human papilloma virus DNA and HPV-E7 protein in oral cancers. Int. J. Immunopathol. Pharmacol. 2011, 24 (Suppl. 2), 95–101. [Google Scholar] [CrossRef] [Green Version]
- Castellsagué, X.; Alemany, L.; Quer, M.; Halec, G.; Quirós, B.; Tous, S.; Clavero, O.; Alòs, L.; Biegner, T.; Szafarowski, T.; et al. ICO International HPV in Head and Neck Cancer Study Group. HPV Involvement in Head and Neck Cancers: Comprehensive Assessment of Biomarkers in 3680 Patients. J. Natl. Cancer Inst. 2016, 108, djv403. [Google Scholar] [CrossRef] [PubMed]
- Castro, T.P.; Bussoloti Filho, I. Prevalence of human papillomavirus (HPV) in oral cavity and oropharynx. Braz. J. Otorhinolaryngol. 2006, 72, 272–282. [Google Scholar] [CrossRef] [Green Version]
- Rusan, M.; Klug, T.E.; Henriksen, J.J.; Bonde, J.H.; Fuursted, K.; Ovesen, T. Prevalence of tonsillar human papillomavirus infections in Denmark. Eur. Arch. Otorhinolaryngol. 2015, 272, 2505–2512. [Google Scholar] [CrossRef]
- Chandrani, P.; Kulkarni, V.; Iyer, P.; Upadhyay, P.; Chaubal, R.; Das, P.; Mulherkar, R.; Singh, R.; Dutt, A. NGS-based approach to determine the presence of HPV and their sites of integration in human cancer genome. Br. J. Cancer. 2015, 112, 1958–1965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernandez, B.Y.; Lynch, C.F.; Chan, O.T.M.; Goodman, M.T.; Unger, E.R.; Steinau, M.; Thompson, T.D.; Gillison, M.; Lyu, C.; Saraiya, M. HPV Typing of Cancer Workgroup. Human papillomavirus DNA detection, p16INK4a, and oral cavity cancer in a U.S. population. Oral. Oncol. 2019, 91, 92–96. [Google Scholar] [CrossRef] [PubMed]
- Mashiana, S.S.; Navale, P.; Khandakar, B.; Sobotka, S.; Posner, M.R.; Miles, B.A.; Zhang, W.; Gitman, M.; Bakst, R.L.; Genden, E.M.; et al. Human papillomavirus genotype distribution in head and neck cancer: Informing developing strategies for cancer prevention, diagnosis, treatment and surveillance. Oral. Oncol. 2021, 113, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Koo, B.S.; Kang, S.; Park, K.; Kim, H.; Lee, K.R.; Lee, M.J.; Kim, J.M.; Choi, E.C.; Cho, N.H. HPV integration begins in the tonsillar crypt and leads to the alteration of p16, EGFR and c-myc during tumor formation. Int. J. Cancer 2007, 120, 1418–1425. [Google Scholar] [CrossRef] [PubMed]
- Mazurek, A.M.; Rutkowski, T.; Fiszer-Kierzkowska, A.; Małusecka, E.; Składowski, K. Assessment of the total cfDNA and HPV16/18 detection in plasma samples of head and neck squamous cell carcinoma patients. Oral. Oncol. 2016, 54, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Janecka-Widła, A.; Mucha-Małecka, A.; Majchrzyk, K.; Halaszka, K.; Przewoźnik, M.; Słonina, D.; Biesaga, B. Active HPV infection and its influence on survival in head and neck squamous-cell cancer. J. Cancer Res. Clin. Oncol. 2020, 146, 1677–1692. [Google Scholar] [CrossRef] [PubMed]
- Syrjänen, S. HPV infections and tonsillar carcinoma. J. Clin. Pathol. 2004, 57, 449–455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, H.; Kishikawa, T.; Tokita, Y.; Suzuki, M.; Takemoto, N.; Hanamoto, A.; Fukusumi, T.; Yamamoto, M.; Fujii, M.; Ohno, Y.; et al. Prevalence of human papillomavirus in oral gargles and tonsillar washings. Oral. Oncol. 2020, 105, 104669. [Google Scholar] [CrossRef]
- Durzyńska, J.; Pacholska-Bogalska, J.; Kaczmarek, M.; Hanć, T.; Durda, M.; Skrzypczak, M.; Goździcka-Józefiak, A. HPV genotypes in the oral cavity/oropharynx of children and adolescents: Cross-sectional survey in Poland. Eur. J. Pediatr. 2011, 170, 757–761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Combes, J.D.; Dalstein, V.; Gheit, T.; Clifford, G.M.; Tommasino, M.; Clavel, C.; Lacau St Guily, J.; Franceschi, S.; SPLIT Study Group. Prevalence of human papillomavirus in tonsil brushings and gargles in cancer-free patients: The SPLIT study. Oral. Oncol. 2017, 66, 52–57. [Google Scholar] [CrossRef]
- Kim, Y.; Joo, Y.H.; Kim, M.S.; Lee, Y.S. Prevalence of high-risk human papillomavirus and its genotype distribution in head and neck squamous cell carcinomas. J. Pathol. Transl. Med. 2020, 54, 411–418. [Google Scholar] [CrossRef]
- Herberhold, S.; Hellmich, M.; Panning, M.; Bartok, E.; Silling, S.; Akgül, B.; Wieland, U. Human polyomavirus and human papillomavirus prevalence and viral load in non-malignant tonsillar tissue and tonsillar carcinoma. Med. Microbiol. Immunol. 2017, 206, 93–103. [Google Scholar] [CrossRef]
- Veitía, D.; Liuzzi, J.; Ávila, M.; Rodriguez, I.; Toro, F.; Correnti, M. Association of viral load and physical status of HPV-16 with survival of patients with head and neck cancer. Ecancermedicalscience 2020, 14, 1082. [Google Scholar] [CrossRef]
- Polz-Gruszka, D.; Morshed, K.; Stec, A.; Polz-Dacewicz, M. Prevalence of Human papillomavirus (HPV) and Epstein-Barr virus (EBV) in oral and oropharyngeal squamous cell carcinoma in south-eastern Poland. Infect. Agent Cancer 2015, 10, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, K.; Ni, G.; Ma, B.; Chen, S.; Luan, Y.; Wang, T.; Walton, S.; Frazer, I.; Liu, X.; Pan, X. Importance of human papillomavirus infection in squamous cell carcinomas of the tongue in Guangdong Province, China. J. Int. Med. Res. 2020, 48, 300060519897187. [Google Scholar] [CrossRef]
- Chaturvedi, A.K.; Graubard, B.I.; Broutian, T.; Pickard, R.K.; Tong, Z.Y.; Xiao, W.; Kahle, L.; Gillison, M.L. NHANES 2009-2012 Findings: Association of Sexual Behaviors with Higher Prevalence of Oral Oncogenic Human Papillomavirus Infections in U.S. Men. Cancer Res. 2015, 75, 2468–2477. [Google Scholar] [CrossRef] [Green Version]
- Kreimer, A.R.; Villa, A.; Nyitray, A.G.; Abrahamsen, M.; Papenfuss, M.; Smith, D.; Hildesheim, A.; Villa, L.L.; Lazcano-Ponce, E.; Giuliano, A.R. The epidemiology of oral HPV infection among a multinational sample of healthy men. Cancer Epidemiol. Biomark. Prev. 2011, 20, 172–182. [Google Scholar] [CrossRef] [Green Version]
- Kiwerska, K.; Jozefiak, A.; Markowska, J.; Kedzia, W.; Jackowska, J.; Wierzbicka, M. Oral-genital human papillomavirus infection in Polish couples: Frequent detection of HPV 42. BMC Infect. Dis. 2019, 19, 122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Louvanto, K.; Rautava, J.; Willberg, J.; Wideman, L.; Syrjänen, K.; Grénman, S.; Syrjänen, S. Genotype-specific incidence and clearance of human papillomavirus in oral mucosa of women: A six-year follow-up study. PLoS ONE 2013, 8, e53413. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.M.; Kwon, I.J.; Myoung, H.; Lee, J.H.; Lee, S.K. Identification of human papillomavirus (HPV) subtype in oral cancer patients through microarray technology. Eur. Arch. Otorhinolaryngol. 2018, 275, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Al-Dabbagh, R.; Al-Hazmi, N.; Alhazzazi, T.Y.; Barrett, A.W.; Speight, P.M. Human papillomavirus and head and neck squamous cell carcinoma in a UK population: Is there an association? Indian J. Cancer 2021. [Google Scholar] [CrossRef]
- Sugiyama, M.; Bhawal, U.K.; Dohmen, T.; Ono, S.; Miyauchi, M.; Ishikawa, T. Detection of human papillomavirus-16 and HPV-18 DNA in normal, dysplastic, and malignant oral epithelium. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2003, 95, 594–600. [Google Scholar] [CrossRef] [PubMed]
- Cruz, I.B.; Snijders, P.J.; Steenbergen, R.D.; Meijer, C.J.; Snow, G.B.; Walboomers, J.M.; van der Waal, I. Age-dependence of human papillomavirus DNA presence in oral squamous cell carcinomas. Eur. J. Cancer B Oral Oncol. 1996, 32B, 55–62. [Google Scholar] [CrossRef]
- Premoli-De-Percoco, G.; Ramírez, J.L.; Galindo, I. Correlation between HPV types associated with oral squamous cell carcinoma and cervicovaginal cytology: An in situ hybridization study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1998, 86, 77–81. [Google Scholar] [CrossRef]
- Olshan, A.F. Epidemiology, Pathogenesis, and Prevention of Head and Neck Cancer, 1st ed.; Springer: New York, NY, USA, 2010; pp. 87–116. [Google Scholar] [CrossRef]
- Quabius, E.S.; Fazel, A.; Knieling, C.; Gebhardt, S.; Laudien, M.; Moore, C.; Kühnel, A.; Hoppe, F.; Mlynski, R.; Heinrichs, A.; et al. No association between HPV-status in tonsillar tissue and sexual behavior of the patients in a northern German population Critical view of the link between HPV natural history and HPV-driven carcinogenesis. Papillomavirus Res. 2020, 10, 100207. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.Y.; Sdek, P.; Cao, J.; Chen, W.T. Human papillomavirus type 16 and 18 DNA in oral squamous cell carcinoma and normal mucosa. Int. J. Oral. Maxillofac. Surg. 2004, 33, 71–74. [Google Scholar] [CrossRef]
- Balaram, P.; Nalinakumari, K.R.; Abraham, E.; Balan, A.; Hareendran, N.K.; Bernard, H.U.; Chan, S.Y. Human papillomaviruses in 91 oral cancers from Indian betel quid chewers-high prevalence and multiplicity of infections. Int. J. Cancer 1995, 61, 450–454. [Google Scholar] [CrossRef] [PubMed]
- Lu, X.J.D.; Liu, K.Y.P.; Prisman, E.; Wu, J.; Zhu, Y.S.; Poh, C. Prognostic value and cost benefit of HPV testing for oropharyngeal cancer patients. Oral. Dis. 2021, in press. [Google Scholar] [CrossRef]
- Dogantemur, S.; Ozdemir, S.; Uguz, A.; Surmelioglu, O.; Dagkiran, M.; Tarkan, O.; Tuncer, U. Assessment of HPV 16, HPV 18, p16 expression in advanced stage laryngeal cancer patients and prognostic significance. Braz. J. Otorhinolaryngol. 2020, 86, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Flores-Miramontes, M.G.; Torres-Reyes, L.A.; Alvarado-Ruíz, L.; Romero-Martínez, S.A.; Ramírez-Rodríguez, V.; Balderas-Peña, L.M.; Vallejo-Ruíz, V.; Piña-Sánchez, P.; Cortés-Gutiérrez, E.I.; Jave-Suárez, L.F.; et al. Human papillomavirus genotyping by Linear Array and Next-Generation Sequencing in cervical samples from Western Mexico. Virol. J. 2015, 12, 161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salehi-Vaziri, M.; Sadeghi, F.; Hashemi, F.S.; Haeri, H.; Bokharaei-Salim, F.; Monavari, S.H.; Keyvani, H. Distribution of Human Papillomavirus Genotypes in Iranian Women According to the Severity of the Cervical Lesion. Iran. Red Crescent Med. J. 2016, 18, e24458. [Google Scholar] [CrossRef] [Green Version]
- Ahmadi, S.; Goudarzi, H.; Jalilvand, A.; Esmaeilzadeh, A. Human Papilloma Virus Genotype Distribution in Cervical lesions in Zanjan, Iran. Asian Pac. J. Cancer Prev. 2017, 18, 3373–3377. [Google Scholar] [CrossRef] [PubMed]
- Guimerà, N.; Lloveras, B.; Lindeman, J.; Alemany, L.; van de Sandt, M.; Alejo, M.; Hernandez-Suarez, G.; Bravo, I.G.; Molijn, A.; Jenkins, D.; et al. The occasional role of low-risk human papillomaviruses 6, 11, 42, 44, and 70 in anogenital carcinoma defined by laser capture microdissection/PCR methodology: Results from a global study. Am. J. Surg. Pathol. 2013, 37, 1299–1310. [Google Scholar] [CrossRef]
- Saliba, M.; Shaheen, M.; Hajj, R.E.; Abbas, F.; Bashir, S.; Sheikh, U.N.; Mahfouz, R.; Loya, A.; Khalifeh, I. PD-L1 expression in sebaceous carcinomas. Cancer Immunol. Immunother. 2021, 70, 1907–1915. [Google Scholar] [CrossRef]
- Noble-Topham, S.E.; Fliss, D.M.; Hartwick, R.W.; McLachlin, C.M.; Freeman, J.L.; Noyek, A.M.; Andrulis, I.L. Detection and typing of human papillomavirus in verrucous carcinoma of the oral cavity using the polymerase chain reaction. Arch. Otolaryngol. Head Neck Surg. 1993, 119, 1299–1304. [Google Scholar] [CrossRef] [PubMed]
- Stanford-Moore, G.; Bradshaw, P.T.; Weissler, M.C.; Zevallos, J.P.; Brennan, P.; Anantharaman, D.; Abedi-Ardekani, B.; Olshan, A.F. Interaction between known risk factors for head and neck cancer and socioeconomic status: The Carolina Head and Neck Cancer Study. Cancer Causes Control. 2018, 29, 863–873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raczkowska-Łabuda, K.; Gorzelnik, A.; Jadczyszyn, J.; Zawadzka-Głos, L. HPV-related head and neck tumors—10 years of experience with human papillomavirus vaccinations. New Med. 2017, 21, 145–157. [Google Scholar] [CrossRef]
- Ramqvist, T.; Dalianis, T. Oropharyngeal cancer epidemic and human papillomavirus. Emerg. Infect. Dis. 2010, 16, 1671–1677. [Google Scholar] [CrossRef]
- Lindquist, D.; Romanitan, M.; Hammarstedt, L.; Näsman, A.; Dahlstrand, H.; Lindholm, J.; Onelöv, L.; Ramqvist, T.; Ye, W.; Munck-Wikland, E.; et al. Human papillomavirus is a favourable prognostic factor in tonsillar cancer and its oncogenic role is supported by the expression of E6 and E7. Mol. Oncol. 2007, 1, 350–355. [Google Scholar] [CrossRef] [Green Version]
- Ang, K.K.; Harris, J.; Wheeler, R.; Weber, R.; Rosenthal, D.I.; Nguyen-Tân, P.F.; Westra, W.H.; Chung, C.H.; Jordan, R.C.; Lu, C.; et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N Eng. J. Med. 2010, 363, 24–35. [Google Scholar] [CrossRef] [Green Version]
- Merne, M.; Rautava, J.; Ruutu, M.; Syrjänen, S. Smokeless tobacco increases aneuploidy in oral HPV16 E6/E7-transformed keratinocytes in vitro. J. Oral. Pathol. Med. 2014, 43, 685–690. [Google Scholar] [CrossRef] [PubMed]
- Haukioja, A.; Asunta, M.; Söderling, E.; Syrjänen, S. Persistent oral human papillomavirus infection is associated with smoking and elevated salivary immunoglobulin G concentration. J. Clin. Virol. 2014, 61, 101–106. [Google Scholar] [CrossRef]
- Pintos, J.; Black, M.J.; Sadeghi, N.; Ghadirian, P.; Zeitouni, A.G.; Viscidi, R.P.; Herrero, R.; Coutlée, F.; Franco, E.L. Human papillomavirus infection and oral cancer: A case-control study in Montreal, Canada. Oral. Oncol. 2008, 44, 242–250. [Google Scholar] [CrossRef]
- de Martel, C.; Plummer, M.; Vignat, J.; Franceschi, S. Worldwide burden of cancer attributable to HPV by site, country and HPV type. Int. J. Cancer. 2017, 141, 664–670. [Google Scholar] [CrossRef] [Green Version]
- Ziai, H.; Warner, A.; Mundi, N.; Patel, K.; Chung, E.J.; Howlett, C.J.; Plantinga, P.; Yoo, J.; MacNeil, S.D.; Fung, K.; et al. Does HPV Subtype Predict Outcomes in Head and Neck Cancers? Int. J. Otolaryngol. 2021, 6672373. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Dong, P.; Yu, Z. Detection of human papillomavirus infection in laryngeal and hypopharyngeal carcinoma using droplet digital PCR and its correlation with prognosis. Postgrad. Med. 2021, 133, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Menegaldo, A.; Schroeder, L.; Holzinger, D.; Tirelli, G.; Dal Cin, E.; Tofanelli, M.; Rigo, S.; Mantovani, M.; Stellin, M.; Del Mistro, A.; et al. Detection of HPV16/18 E6 Oncoproteins in Head and Neck Squamous Cell Carcinoma Using a Protein Immunochromatographic Assay. Laryngoscope 2021, 131, 1042–1048. [Google Scholar] [CrossRef]
- Maver, P.J.; Kocjan, B.J.; Seme, K.; Poljak, M. Genomic diversity of low-risk human papillomavirus genotypes HPV 40, HPV 42, HPV 43, and HPV 44. J. Med. Virol. 2014, 86, 272–282. [Google Scholar] [CrossRef] [PubMed]
- Meyer, A.; Alicea, D.A.; Ferrandino, R.M.; Miles, B.A. Behavioral analysis of HPV+ oropharyngeal cancer: Do you know your patients? Am. J. Otolaryngol. 2019, 40, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Kreimer, A.R.; Pierce Campbell, C.M.; Lin, H.Y.; Fulp, W.; Papenfuss, M.R.; Abrahamsen, M.; Hildesheim, A.; Villa, L.L.; Salmerón, J.J.; Lazcano-Ponce, E.; et al. Incidence and clearance of oral human papillomavirus infection in men: The HIM cohort study. Lancet 2013, 382, 877–887. [Google Scholar] [CrossRef] [Green Version]
- Mirabello, L.; Clarke, M.A.; Nelson, C.W.; Dean, M.; Wentzensen, N.; Yeager, M.; Cullen, M.; Boland, J.F.; NCI HPV Workshop; Schiffman, M.; et al. The Intersection of HPV Epidemiology, Genomics and Mechanistic Studies of HPV-Mediated Carcinogenesis. Viruses 2018, 10, 80. [Google Scholar] [CrossRef] [Green Version]
- Burk, R.D.; Chen, Z.; Van Doorslaer, K. Human papillomaviruses: Genetic basis of carcinogenicity. Public Health Genom. 2009, 12, 281–290. [Google Scholar] [CrossRef] [Green Version]
- Ernster, J.A.; Sciotto, C.G.; O’Brien, M.M.; Robinson, L.J.; Willson, T. Prevalence of oncogenic human papillomavirus 16 and 18 in the palatine tonsils of the general adult population. Arch. Otolaryngol. Head Neck Surg. 2009, 135, 554–557. [Google Scholar] [CrossRef] [Green Version]
- Palmer, E.; Newcombe, R.G.; Green, A.C.; Kelly, C.; Noel Gill, O.; Hall, G.; Fiander, A.N.; Pirotte, E.; Hibbitts, S.J.; Homer, J.; et al. Human papillomavirus infection is rare in nonmalignant tonsil tissue in the UK: Implications for tonsil cancer precursor lesions. Int. J. Cancer 2014, 135, 2437–2443. [Google Scholar] [CrossRef]
- Ilmarinen, T.; Munne, P.; Hagström, J.; Haglund, C.; Auvinen, E.; Virtanen, E.I.; Haesevoets, A.; Speel, E.J.M.; Aaltonen, L.M. Prevalence of high-risk human papillomavirus infection and cancer gene mutations in nonmalignant tonsils. Oral. Oncol. 2017, 73, 77–82. [Google Scholar] [CrossRef] [Green Version]
- Chen, R.; Sehr, P.; Waterboer, T.; Leivo, I.; Pawlita, M.; Vaheri, A.; Aaltonen, L.M. Presence of DNA of human papillomavirus 16 but no other types in tumor-free tonsillar tissue. J. Clin. Microbiol. 2005, 43, 1408–1410. [Google Scholar] [CrossRef] [Green Version]
- Wojtera, M.; Paradis, J.; Husein, M.; Nichols, A.C.; Barrett, J.W.; Salvadori, M.I.; Strychowsky, J.E. The prevalence of human papillomavirus in pediatric tonsils: A systematic review of the literature. J. Otolaryngol. Head Neck Surg. 2018, 47, 8. [Google Scholar] [CrossRef] [Green Version]
- Grün, N.; Mbuya, W.; Ternhag, A.; Ramqvist, T.; Ahlberg, A.; Jangard, M.; Dalianis, T.; Hammarstedt-Nordenvall, L. Human papillomavirus prevalence in mouthwashes of patients undergoing tonsillectomy shows dominance of HPV69, without the corresponding finding in the tonsils. Infect. Dis. 2017, 49, 588–593. [Google Scholar] [CrossRef] [PubMed]
- Sisk, J.; Schweinfurth, J.M.; Wang, X.T.; Chong, K. Presence of human papillomavirus DNA in tonsillectomy specimens. Laryngoscope 2006, 116, 1372–1374. [Google Scholar] [CrossRef] [PubMed]
- Syrjänen, S. Current concepts on human papillomavirus infections in children. APMIS 2010, 118, 494–509. [Google Scholar] [CrossRef] [PubMed]
- Blioumi, E.; Chatzidimitriou, D.; Pazartzi, C.; Katopodi, T.; Tzimagiorgis, G.; Emmanouil-Nikoloussi, E.N.; Markopoulos, A.; Kalekou, C.; Lazaridis, N.; Diza, E.; et al. Detection and typing of human papillomaviruses (HPV) in malignant, dysplastic, nondysplastic and normal oral epithelium by nested polymerase chain reaction, immunohistochemistry and transitional electron microscopy in patients of northern Greece. Oral. Oncol. 2014, 50, 840–847. [Google Scholar] [CrossRef]
- Jamieson, L.M.; Garvey, G.; Hedges, J.; Leane, C.; Hill, I.; Brown, A.; Ju, X.; Sethi, S.; Roder, D.; Logan, R.M.; et al. Cohort profile: Indigenous human papillomavirus and oropharyngeal squamous cell carcinoma study—A prospective longitudinal cohort. BMJ Open 2021, 11, e046928. [Google Scholar] [CrossRef]
- Terai, M.; Hashimoto, K.; Yoda, K.; Sata, T. High prevalence of human papillomaviruses in the normal oral cavity of adults. Oral. Microbiol. Immunol. 1999, 14, 201–205. [Google Scholar] [CrossRef]
- Nejo, Y.T.; Olaleye, D.O.; Odaibo, G.N. Molecular characterisation of genital human papillomavirus among women in Southwestern, Nigeria. PLoS ONE 2019, 14, e0224748. [Google Scholar] [CrossRef]
- Koyalta, D.; Mboumba Bouassa, R.S.; Maiga, A.; Balde, A.; Bagendabanga, J.B.; Alinity, A.A.; Veyer, D.; Péré, H.; Bélec, L. High Prevalence of Anal Oncogenic Human Papillomavirus Infection in Young Men Who Have Sex with Men Living in Bamako, Mali. Infect. Agent Cancer 2021, 16, 51. [Google Scholar] [CrossRef]
- Zhi, Y.F.; Cha, X.X.; Li, X.F.; Qiu, C.; Rong, S.H. Prevalence and genotype distribution of human papillomavirus in women in the Henan Province. Genet. Mol. Res. 2015, 14, 5452–5461. [Google Scholar] [CrossRef] [PubMed]
- Baloch, Z.; Yue, L.; Yuan, T.; Feng, Y.; Tai, W.; Liu, Y.; Wang, B.; Li, X.; Liu, L.; Zhang, A.M.; et al. Status of Human Papillomavirus Infection in the Ethnic Population in Yunnan Province, China. Biomed. Res. Int. 2015, 2015, 314815. [Google Scholar] [CrossRef]
- Kovachev, S.; Slavov, V. Prevalence of human papillomavirus infection in women in Bulgaria: A 2017 update. J. Med. Virol. 2018, 90, 1142–1149. [Google Scholar] [CrossRef] [PubMed]
- Tsao, A.S.; Papadimitrakopoulou, V.; Lin, H.; Guo, M.; Lee, J.J.; Holsinger, F.C.; Hong, W.K.; Sturgis, E.M. Concordance of oral HPV prevalence between patients with oropharyngeal cancer and their partners. Infect. Agent Cancer. 2016, 11, 21. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Quintanilla, M.; Méndez-Martínez, R.; Vázquez-Vega, S.; Espinosa-Romero, R.; Sotelo-Regil, R.; Pérez-Montiel, M.D.; Ramos-Alamillo, U.; Cabrera-López, T.J.; Barquet-Muñoz, S.A.; Pérez-Plascencia, C.; et al. High prevalence of human papillomavirus and European variants of HPV 16 infecting concomitantly to cervix and oral cavity in HIV positive women. PLoS ONE 2020, 15, e0227900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doorbar, J. The papillomavirus life cycle. J. Clin. Virol. 2005, 32 (Suppl. 1), S7–S15. [Google Scholar] [CrossRef]
- Walker, K.K.; Jackson, R.D.; Sommariva, S.; Neelamegam, M.; Desch, J. USA dental health providers’ role in HPV vaccine communication and HPV-OPC protection: A systematic review. Hum. Vaccin. Immunother. 2019, 15, 1863–1869. [Google Scholar] [CrossRef]
- Fiorito, T.M.; Krilov, L.R.; Nonaillada, J. Human Papillomavirus Knowledge and Communication Skills: A Role-Play Activity for Providers. MedEdPORTAL 2021, 17, 11150. [Google Scholar] [CrossRef]
- Lowy, D.R.; Herrero, R.; Hildesheim, A. Participants in the IARC/NCI workshop on Primary Endpoints for Prophylactic HPV Vaccine Trials. Primary endpoints for future prophylactic human papillomavirus vaccine trials: Towards infection and immunobridging. Lancet Oncol. 2015, 16, e226–e233. [Google Scholar] [CrossRef]
- Chaturvedi, A.K.; Graubard, B.I.; Broutian, T.; Pickard, R.K.L.; Tong, Z.Y.; Xiao, W.; Kahle, L.; Gillison, M.L. Effect of Prophylactic Human Papillomavirus (HPV) Vaccination on Oral HPV Infections among Young Adults in the United States. J. Clin. Oncol. 2018, 36, 262–267. [Google Scholar] [CrossRef]
- Grün, N.; Ährlund-Richter, A.; Franzén, J.; Mirzaie, L.; Marions, L.; Ramqvist, T.; Dalianis, T. Oral human papillomavirus (HPV) prevalence in youth and cervical HPV prevalence in women attending a youth clinic in Sweden, a follow up-study 2013-2014 after gradual introduction of public HPV vaccination. Infect. Dis. 2015, 47, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Enerly, E.; Flingtorp, R.; Christiansen, I.K.; Campbell, S.; Hansen, M.; Myklebust, T.Å.; Weiderpass, E.; Nygård, M. An observational study comparing HPV prevalence and type distribution between HPV-vaccinated and -unvaccinated girls after introduction of school-based HPV vaccination in Norway. PLoS ONE 2019, 14, e0223612. [Google Scholar] [CrossRef]
- Brisson, M.; Kim, J.J.; Canfell, K.; Drolet, M.; Gingras, G.; Burger, E.A.; Martin, D.; Simms, K.T.; Bénard, É.; Boily, M.C.; et al. Impact of HPV vaccination and cervical screening on cervical cancer elimination: A comparative modelling analysis in 78 low-income and lower-middle-income countries. Lancet 2020, 395, 575–590. [Google Scholar] [CrossRef] [Green Version]
- Stanley, M. HPV vaccination in boys and men. Hum. Vaccin. Immunother. 2014, 10, 2109–2111. [Google Scholar] [CrossRef] [PubMed]
- Grandahl, M.; Nevéus, T. Barriers towards HPV Vaccinations for Boys and Young Men: A Narrative Review. Viruses 2021, 13, 1644. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| All | HNSCC | Chronic Tonsillitis | Control | |||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| Age | 42.66 | ±16.39 | 57.83 | ±10.02 | 33.35 | ±11.11 | 39.73 | ±16.06 |
| n | % | n | % | n | % | n | % | |
| Age ≥ 40 | 167 | 53.0 | 72 | 94.7 | 18 | 25.4 | 77 | 45.8 |
| Age < 40 | 148 | 47.1 | 4 | 5.3 | 53 | 74.7 | 91 | 54.2 |
| Female | 170 | 54.0 | 21 | 27.6 | 37 | 52.1 | 112 | 66.7 |
| Male | 145 | 46.0 | 55 | 72.4 | 34 | 47.9 | 56 | 33.3 |
| Smokers | 94 | 29.8 | 53 | 69.7 | 10 | 14.1 | 31 | 18.5 |
| Non-smokers | 221 | 70.2 | 23 | 30.3 | 61 | 85.9 | 137 | 81.6 |
| Alcohol users | 190 | 60.3 | 48 | 63.2 | 21 | 29.6 | 121 | 72.0 |
| Alcohol non-users | 125 | 39.7 | 28 | 36.8 | 50 | 70.4 | 47 | 28.0 |
| Smokers and alcohol users | 75 | 23.8 | 40 | 52.6 | 6 | 8.5 | 29 | 17.3 |
| Smokers or alcohol users | 209 | 66.4 | 61 | 80.3 | 25 | 35.2 | 123 | 73.2 |
| All N = 315 | HNSCC N = 76 | Chronic Tonsillitis N = 71 | Control N = 168 | |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | |
| HPV-positive | 113 (35.9) | 32 (42.1) | 18 (25.4) | 63 (37.5) |
| HPV 16 | 94 (28.8) | 23 (30.3) | 16 (22.5) | 55 (32.7) |
| HPV 43/44 | 13 (4.1) | 8 (10.5) | 1 (1.4) | 4 (2.4) |
| HPV 18 | 6 (1.9) | 1 (1.3) | 1 (1.4) | 4 (2.4) |
| HPV 35 | 2 (0.6) | - | - | 2 (1.2) |
| HPV 51 | 1 (0.3) | - | - | 1 (0.6) |
| HPV 56 | 1 (0.3) | - | 1 (1.4) | - |
| HPV 73 | 2 (0.6) | 1 (1.3) | - | 1 (0.6) |
| Groups | HPV-Positive | HPV 16 | HPV 43/44 | HPV 18 | HPV 35 | HPV 51 | HPV 56 | HPV 73 |
|---|---|---|---|---|---|---|---|---|
| Control vs. HNSCC | 0.497 | 0.704 | <0.001 | 0.589 | 0.341 | 0.503 | - | 0.562 |
| Chronic tonsillitis vs. HNSCC | <0.05 | 0.289 | <0.05 | 0.960 | - | - | 0.298 | 0.332 |
| Control vs. chronic tonsillitis | 0.070 | 0.114 | 0.631 | 0.631 | 0.357 | 0.516 | 0.124 | 0.516 |
| Study Group | Variable | Variant | HPV-Positive | HPV-Negative | χ2 | p |
|---|---|---|---|---|---|---|
| HNSCC N = 76 | sex | women | 8 | 13 | 0.19 | 0.662 |
| men | 24 | 31 | ||||
| smoking | yes | 19 | 34 | 2.81 | 0.094 | |
| no | 13 | 10 | ||||
| drinking | yes | 19 | 29 | 0.34 | 0.560 | |
| no | 13 | 15 | ||||
| smoking and drinking | yes | 16 | 24 | 0.15 | 0.695 | |
| no | 16 | 20 | ||||
| smoking or drinking | yes | 22 | 39 | 4.63 | <0.05 | |
| no | 10 | 5 | ||||
| Chronic tonsillitis N = 71 | sex | women | 12 | 25 | 2.04 | 0.152 |
| men | 6 | 28 | ||||
| smoking | yes | 3 | 7 | 0.001 | 0.978 | |
| no | 15 | 46 | ||||
| drinking | yes | 5 | 13 | 0.04 | 0.846 | |
| no | 16 | 37 | ||||
| smoking and drinking | yes | 1 | 17 | 0.0004 | 0.983 | |
| no | 5 | 48 | ||||
| smoking or drinking | yes | 7 | 11 | 0.14 | 0.705 | |
| no | 18 | 35 | ||||
| Control N = 168 | sex | women | 47 | 65 | 2.86 | 0.091 |
| men | 16 | 40 | ||||
| smoking | yes | 12 | 19 | 0.02 | 0.878 | |
| no | 51 | 86 | ||||
| drinking | yes | 45 | 76 | 0.02 | 0.894 | |
| no | 18 | 29 | ||||
| smoking and drinking | yes | 12 | 17 | 0.23 | 0.635 | |
| no | 51 | 88 | ||||
| smoking or drinking | yes | 45 | 78 | 0.16 | 0.686 | |
| no | 18 | 27 |
| Group | Variant | HPV Status | HPV 16 | HPV 43/44 |
|---|---|---|---|---|
| HNSCC | Positive | 58 ± 10 | 59 ± 11 | 56 ± 7 |
| Negative | 58 ± 10 | 57 ± 10 | 58 ± 10 | |
| p-value | 0.748 | 0.277 | 0.313 | |
| Chronic tonsillitis | Positive | 30 ± 9 | 20 ± 9 | |
| Negative | 35 ± 12 | 34 ± 12 | ||
| p-value | 0.071 | 0.177 | ||
| Control | Positive | 37 ± 15 | 36 ± 14 | 29 ± 2 |
| Negative | 41 ± 17 | 42 ± 17 | 40 ± 16 | |
| p-value | 0.083 | <0.05 | 0.165 | |
| All | Positive | 42 ± 17 | 41 ± 17 | 45 ± 16 |
| Negative | 43 ± 16 | 44 ± 16 | 43 ± 16 | |
| p-value | 0.434 | 0.116 | 0.599 |
| Study Group | HPV-Positive | HPV 16 | HPV 43/44 | HPV 18 | HPV 35 | HPV 51 | HPV 56 | HPV 73 | |
|---|---|---|---|---|---|---|---|---|---|
| HNSCC | Women | 8 (38.1%) | 5 (23.8%) | 2 (9.5%) | 1 (4.8%) | - | - | - | 1 (4.8%) |
| Men | 24 (43.6%) | 18 (32.7%) | 6 (10.9%) | 0 (0%) | - | - | - | 0 (0%) | |
| p | 0.664 | 0.452 | 0.861 | 0.106 | - | - | - | 0.106 | |
| Chronic tonsillitis | Women | 12 (32.4%) | 10 (27.0%) | 1 (2.7%) | 1 (2.7%) | - | - | 0 (0%) | - |
| Men | 6 (17.7%) | 6 (17.7%) | 0 (0%) | 0 (0%) | - | - | 1 (2.9%) | - | |
| p | 0.155 | 0.348 | 0.338 | 0.338 | - | - | 0.297 | - | |
| Control | Women | 47 (42.0%) | 42 (37.5%) | 2 (1.8%) | 3 (2.7%) | 2 (1.8%) | 0 (0%) | - | 0 (0%) |
| Men | 16 (28.6%) | 13 (23.2%) | 2 (3.6%) | 1 (1.8%) | 0(0%) | 1 (1.8%) | - | 1 (1.8%) | |
| p | 0.092 | 0.064 | 0.476 | 0.721 | 0.316 | 0.157 | - | 0.157 | |
| All | Women | 67 (39.4%) | 57 (33.5%) | 5 (2.9%) | 5 (2.9%) | 2 (1.2%) | 0 (0%) | 0 (0%) | 1 (0.6%) |
| Men | 46 (31.7%) | 37 (25.5%) | 8 (5.5%) | 1 (0.7%) | 0 (0%) | 1 (0.7%) | 1 (0.7%) | 1 (0.7%) | |
| p | 0.157 | 0.122 | 0.253 | 0.146 | 0.191 | 0.279 | 0.279 | 0.910 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Strzelczyk, J.K.; Biernacki, K.; Gaździcka, J.; Chełmecka, E.; Miśkiewicz-Orczyk, K.; Zięba, N.; Strzelczyk, J.; Misiołek, M. The Prevalence of High- and Low-Risk Types of HPV in Patients with Squamous Cell Carcinoma of the Head and Neck, Patients with Chronic Tonsillitis, and Healthy Individuals Living in Poland. Diagnostics 2021, 11, 2180. https://doi.org/10.3390/diagnostics11122180
Strzelczyk JK, Biernacki K, Gaździcka J, Chełmecka E, Miśkiewicz-Orczyk K, Zięba N, Strzelczyk J, Misiołek M. The Prevalence of High- and Low-Risk Types of HPV in Patients with Squamous Cell Carcinoma of the Head and Neck, Patients with Chronic Tonsillitis, and Healthy Individuals Living in Poland. Diagnostics. 2021; 11(12):2180. https://doi.org/10.3390/diagnostics11122180
Chicago/Turabian StyleStrzelczyk, Joanna Katarzyna, Krzysztof Biernacki, Jadwiga Gaździcka, Elżbieta Chełmecka, Katarzyna Miśkiewicz-Orczyk, Natalia Zięba, Janusz Strzelczyk, and Maciej Misiołek. 2021. "The Prevalence of High- and Low-Risk Types of HPV in Patients with Squamous Cell Carcinoma of the Head and Neck, Patients with Chronic Tonsillitis, and Healthy Individuals Living in Poland" Diagnostics 11, no. 12: 2180. https://doi.org/10.3390/diagnostics11122180