
Epithelial-Myoepithelial Carcinoma of the Minor Salivary Glands: Case Series with Comprehensive Review

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Case Presentation
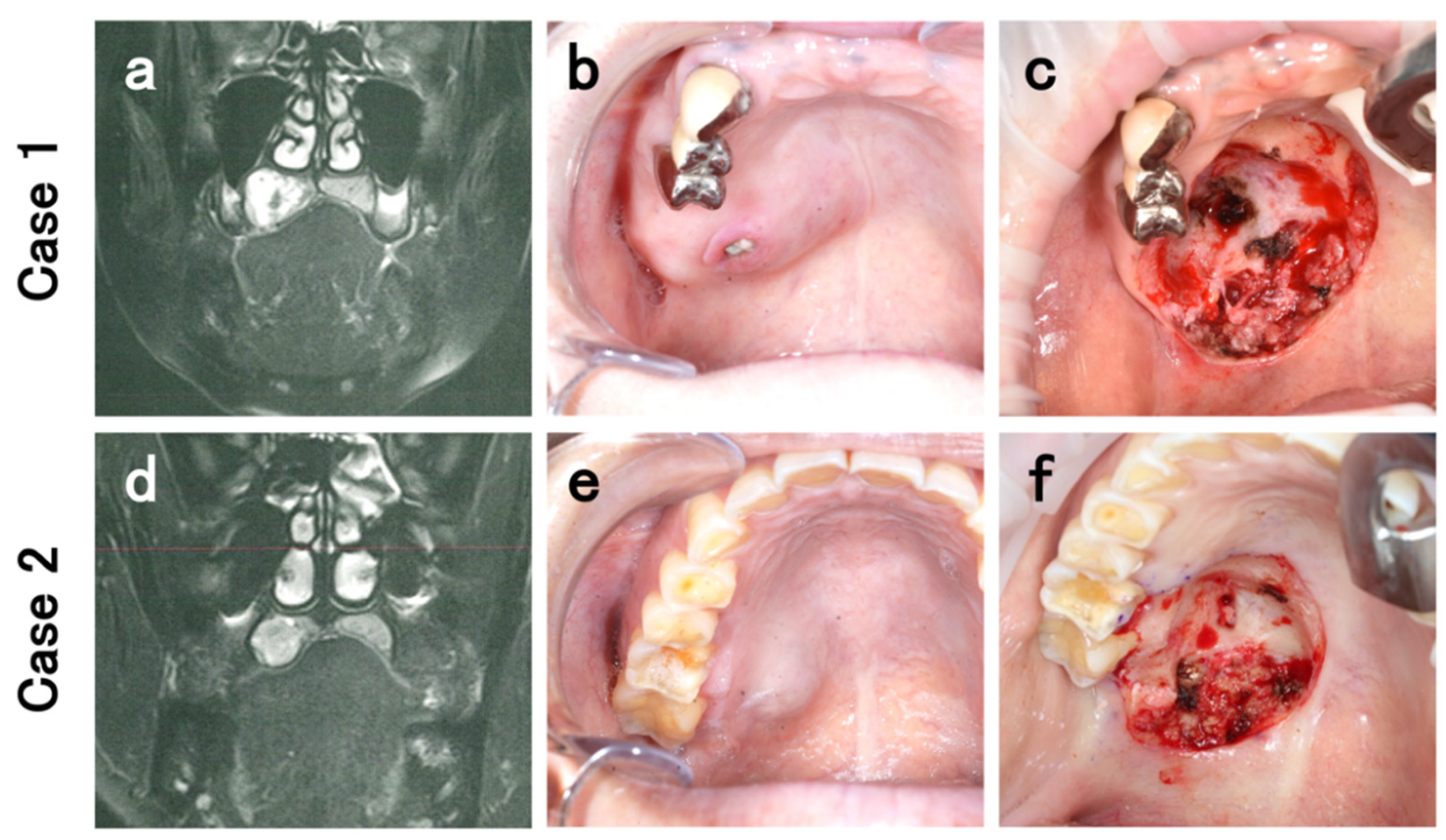
2.1. Case 1
2.2. Case 2
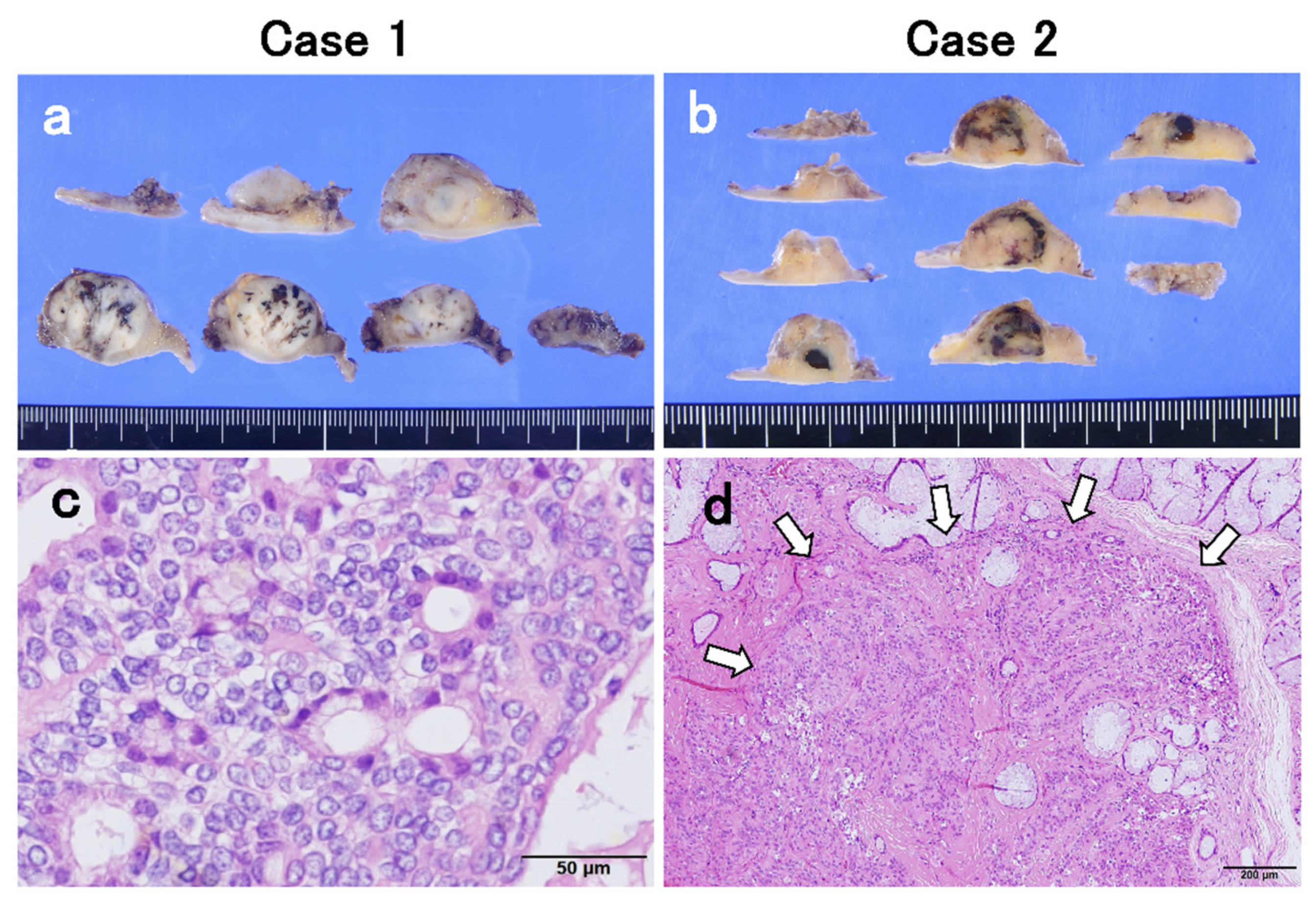
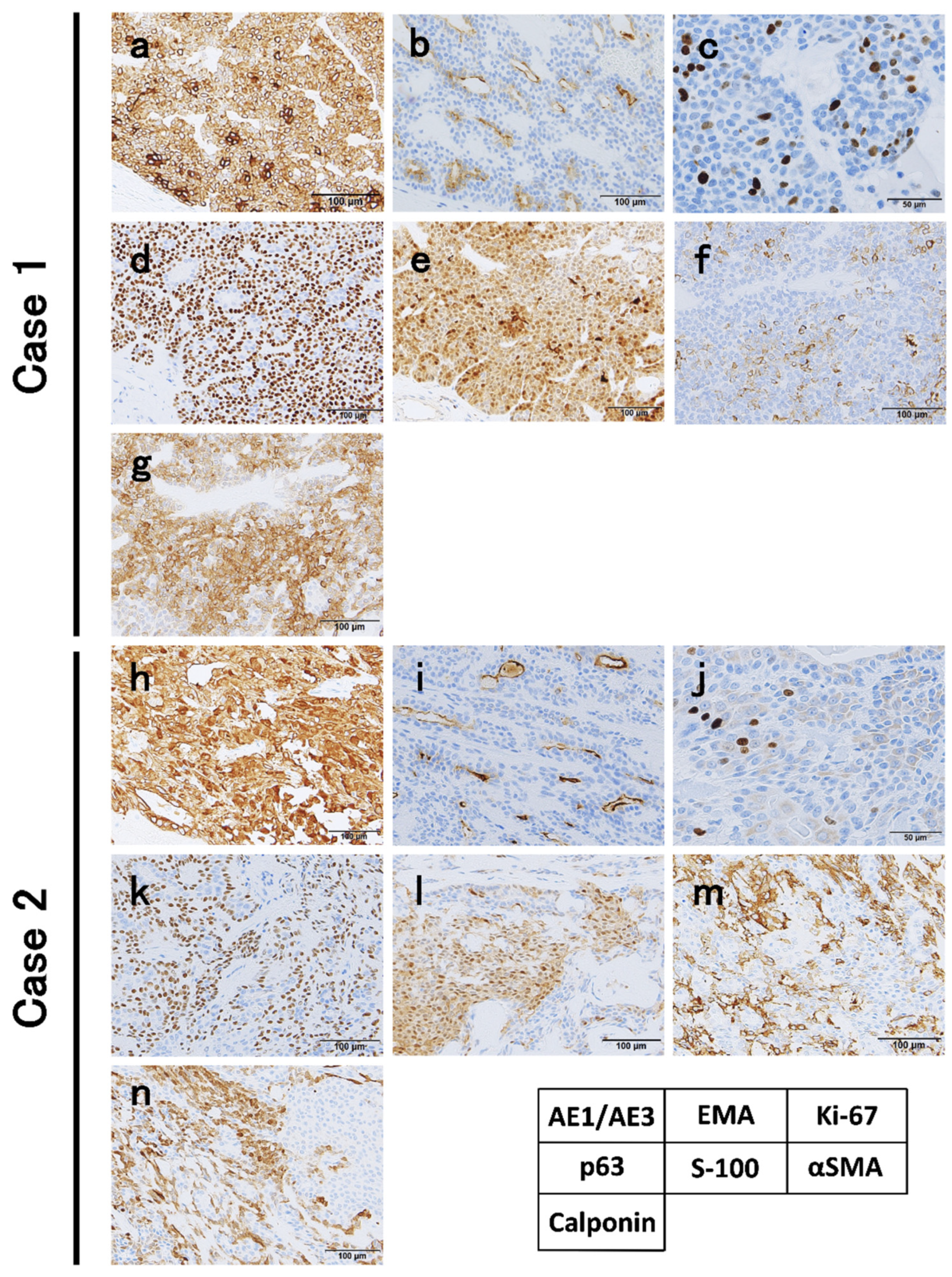
2.3. Microscopical Findings
3. Materials and Methods
Review of Literature
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Ellis, G.L.; Auclair, P. Epithelial-myoepithelial carcinoma. In Tumors of the Salivary Glands (AFIP Atlas of Tumor Pathology: Series 4); American Registry of Pathology: Washington, DC, USA, 2008; pp. 309–322. [Google Scholar]
- Seethala, R.; Bell, D.; Fonseca, I.; El-Naggar, A.; Chan, J.K.; Grandis, J.; Takata, T.; Slootweg, P. Epithelial-myoepithelial carcinoma. In WHO Classification of Head and Neck Tumours; International Agency for Research on Cancer: Lyon, France, 2017; pp. 309–322. [Google Scholar]
- Sedassari, B.T.; Dos Santos, H.T.; Mariano, F.V.; da Silva Lascane, N.A.; Altemani, A.; Sousa, S. Carcinoma ex pleomorphic adenoma of minor salivary glands with major epithelial-myoepithelial component: Clinicopathologic and immunohistochemical study of 3 cases. Ann. Diagn. Pathol. 2015, 19, 164–168. [Google Scholar] [CrossRef] [PubMed]
- Gore, M.R. Epithelial-myoepithelial carcinoma: A population-based survival analysis. BMC. Ear. Nose. Throat. Disord. 2018, 18, 15. [Google Scholar] [CrossRef] [PubMed]
- Seethala, R.R.; Barnes, E.L.; Hunt, J.L. Epithelial-myoepithelial carcinoma: A review of the clinicopathologic spectrum and immunophenotypic characteristics in 61 tumors of the salivary glands and upper aerodigestive tract. Am. J. Surg. Pathol. 2007, 31, 44–57. [Google Scholar] [CrossRef] [PubMed]
- Vazquez, A.; Patel, T.D.; D’Aguillo, C.M.; Abdou, R.Y.; Farver, W.; Baredes, S.; Eloy, J.A.; Park, R.C.W. Epithelial-myoepithelial carcinoma of the salivary glands: An analysis of 246 cases. Otolaryngol. Head Neck Surg. 2015, 153, 569–574. [Google Scholar] [CrossRef] [PubMed]
- Shinozaki, A.; Nagao, T.; Endo, H.; Kato, N.; Hirokawa, M.; Mizobuchi, K.; Komatsu, M.; Igarashi, T.; Yokoyama, M.; Masuda, S.; et al. Sebaceous epithelial-myoepithelial carcinoma of the salivary gland: Clinicopathologic and immunohistochemical analysis of 6 cases of a new histologic variant. Am. J. Surg. Pathol. 2008, 32, 913–923. [Google Scholar] [CrossRef]
- Seethala, R.R. Oncocytic and apocrine epithelial myoepithelial carcinoma: Novel variants of a challenging tumor. Head Neck Pathol. 2013, 7 (Suppl. 1), 77–84. [Google Scholar] [CrossRef] [Green Version]
- Seethala, R.R.; Richmond, J.A.; Hoschar, A.P.; Barnes, E.L. New variants of epithelial-myoepithelial carcinoma: Oncocytic-sebaceous and apocrine. Arch. Pathol. Lab. Med. 2009, 133, 950–959. [Google Scholar] [CrossRef]
- Hussaini, H.M.; Angel, C.M.; Speight, P.M.; Firth, N.A.; Rich, A.M. A double-clear variant of epithelial-myoepithelial carcinoma of the parotid gland. Head Neck Pathol. 2012, 6, 471–475. [Google Scholar] [CrossRef] [Green Version]
- Fonseca, I.; Soares, J.; Barnes, L.; Eveson, J.W.; Reichart, P.; Sidransky, D. Epithelial-myoepithelial carcinoma. In Pathology and Genetics of Head and Neck Tumours; IARC Press: Lyon, France, 2005; pp. 225–226. [Google Scholar]
- Alos, L.; Carrillo, R.; Ramos, J.; Baez, J.M.; Mallofre, C.; Fernandez, P.L.; Cardesa, A. High-grade carcinoma component in epithelial-myoepithelial carcinoma of salivary glands clinicopathological, immunohistochemical and flow-cytometric study of three cases. Virchows. Arch. 1999, 434, 291–299. [Google Scholar] [CrossRef]
- Roy, P.; Bullock, M.J.; Perez-Ordonez, B.; Dardick, I.; Weinreb, I. Epithelial-myoepithelial carcinoma with high grade transformation. Am. J. Surg. Pathol. 2010, 34, 1258–1265. [Google Scholar] [CrossRef]
- Cheuk, W.; Chan, J.C. Dedifferentiation in salivary gland carcinomas. Am. J. Surg. Pathol. 2000, 24, 469–471. [Google Scholar] [CrossRef]
- Fonseca, I.; Soares, J. Epithelial-myoepithelial carcinoma of the salivary glands. A study of 22 cases. Virchows Arch. A Pathol. Anat. Histopathol. 1993, 422, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Kusafuka, K.; Takizawa, Y.; Ueno, T.; Ishiki, H.; Asano, R.; Kamijo, T.; Iida, Y.; Ebihara, M.; Ota, Y.; Onitsuka, T.; et al. Dedifferentiated epithelial-myoepithelial carcinoma of the parotid gland: A rare case report of immunohistochemical analysis and review of the literature. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2008, 106, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Nagao, T. “Dedifferentiation” and high-grade transformation in salivary gland carcinomas. Head Neck Pathol. 2013, 7 (Suppl. 1), 37–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urano, M.; Nakaguro, M.; Yamamoto, Y.; Hirai, H.; Tanigawa, M.; Saigusa, N.; Shimizu, A.; Tsukahara, K.; Tada, Y.; Sakurai, K.; et al. Diagnostic significance of HRAS mutations in epithelial-myoepithelial carcinomas exhibiting a broad histopathologic spectrum. Am. J. Surg. Pathol. 2019, 43, 984–994. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Li, B.; Wang, Y.; Shen, Y.; Yang, H. Clinical and pathological analysis of 10 cases of salivary gland epithelial–myoepithelial carcinoma. Medicine 2020, 99, e22671. [Google Scholar] [CrossRef]
- Lee, Y.S.; Ha, S.M.; Paik, S.W.; Yang, H.J.; Jeon, H.J.; Park, D.J.; Hwang, C.S. Epithelial-myoepithelial carcinoma originating from a minor salivary gland in the nasal septum: A case report and literature review. Medicine 2020, 99, e19072. [Google Scholar] [CrossRef] [PubMed]
- Palaniappan, R.; Chandran, J.; Purushothaman, D.; Nandhagopal, V. Epithelial myoepithelial carcinoma of the hard palate: A case report with a review of the literature. EMJ. Oncol. 2019, 7, 63–67. [Google Scholar]
- Tsuji, T.; Kitada, H.; Abe, S.; Ikeda, H.; Nakayama, E. Epithelial–myoepithelial carcinoma of a minor salivary gland in the buccal mucosa. Oral. Radiol. 2016, 32, 130–135. [Google Scholar] [CrossRef]
- Oh, H.J.; Do, N.Y.; Kee, K.H.; Park, J.H. Epithelial-myoepithelial carcinoma arising from the subglottis: A case report and review of the literature. J. Med. Case. Rep. 2016, 10, 45. [Google Scholar] [CrossRef] [Green Version]
- Lima, F.J.; Porto, D.E.; Cavalcante, J.R.; Oka, S.C.; Godoy, G.P. Epithelial-myoepithelial carcinoma of high grade transformation: The case report in the buccal mucosa. Open. Dent. J. 2012, 6, 111–117. [Google Scholar] [CrossRef] [Green Version]
- Angiero, F.; Sozzi, D.; Seramondi, R.; Valente, M.G. Epithelial-myoepithelial carcinoma of the minor salivary glands: Immunohistochemical and morphological features. Anticancer Res. 2009, 29, 4703–4709. [Google Scholar]
- Teppo, H.; Paronen, I. Epithelial-myoepithelial carcinoma in minor salivary gland of the hard palate. J. Craniofac. Surg. 2008, 19, 1689–1691. [Google Scholar] [CrossRef] [PubMed]
- Yamanegi, K.; Uwa, N.; Hirokawa, M.; Ohyama, H.; Hata, M.; Yamada, N.; Ogino, K.; Toh, K.; Terada, T.; Tanaka, A.; et al. Epithelial-myoepithelial carcinoma arising in the nasal cavity. Auris. Nasus. Larynx. 2008, 35, 408–413. [Google Scholar] [CrossRef]
- Inoue, Y.; Nomura, J.; Hashimoto, M.; Tagawa, T. Epithelial-myoepithelial carcinoma of the palate: A case report. J. Oral. Maxillofac. Surg. 2001, 59, 1502–1505. [Google Scholar] [CrossRef] [PubMed]
- Li, C.Y.; Shirasuna, K.; Ishibashi, H.; Nakayama, H.; Kiyoshima, T. Epithelial-myoepithelial carcinoma arising in pleomorphic adenoma of the palate. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2000, 90, 460–465. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, R.E.; Donath, K. Epithelial-myoepithelial carcinoma of the parotid gland with multiple distant metastases: A case report. J. Oral. Maxillofac. Surg. 2000, 58, 690–694. [Google Scholar] [CrossRef]
- Hamper, K.; Brügmann, M.; Koppermann, R.; Caselitz, J.; Arps, H.; Askensten, U.; Auer, G.; Seifert, G. Epithelial–myoepithelial duct carcinoma of salivary glands: A follow-up and cytophotometric study of 21 cases. J. Oral. Pathol. Med. 1989, 18, 299–304. [Google Scholar] [CrossRef]
- Corio, R.L.; Sciubba, J.J.; Brannon, R.B.; Batsakis, J.G. Epithelial–myoepithelial carcinoma of intercalated duct origin. A clinico-pathologic and ultrastructural assessment of sixteen cases. Oral. Surg. Oral. Med. Oral. Pathol. 1982, 53, 280–287. [Google Scholar] [CrossRef]
- Simpson, R.H.; Clarke, T.J.; Sarsfield, P.T.; Gluckman, P.G. Epithelial–myoepithelial carcinoma of salivary glands. J. Clin. Pathol. 1991, 44, 419–423. [Google Scholar] [CrossRef] [Green Version]
- Cerda, T.; Sun, X.S.; Vignot, S.; Marcy, P.Y.; Baujat, B.; Baglin, A.C.; Ali, A.M.; Testelin, S.; Reyt, E.; Janot, F.; et al. A rationale for chemoradiation (vs radiotherapy) in salivary gland cancers? On behalf of the REFCOR (French rare head and neck cancer network). Crit. Rev. Oncol. Hematol. 2014, 91, 142–158. [Google Scholar] [CrossRef]
- Knoepp, S.M.; Roh, M.H. Ancillary techniques on direct-smear aspirate slides: A significant evolution for cytopathology techniques. Cancer Cytopathol. 2013, 121, 120–128. [Google Scholar] [CrossRef] [Green Version]
- Evrard, S.M.; Meilleroux, J.; Daniel, G.; Basset, C.; Lacoste-Collin, L.; Vergez, S.; Uro-Coste, E.; Courtade-Saidi, M. Use of fluorescent in-situ hybridisation in salivary gland cytology: A powerful diagnostic tool. Cytopathology. 2017, 28, 312–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hudson, J.B.; Collins, B.T. MYB gene abnormalities t(6;9) in adenoid cystic carcinoma fine-needle aspiration biopsy using fluorescence in situ hybridization. Arch. Pathol. Lab. Med. 2014, 138, 403–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hornick, J.L.; Fletcher, C.D. Myoepithelial tumors of soft tissue: A clinicopathologic and immunohistochemical study of 101 cases with evaluation of prognostic parameters. J. Thorac. Dis. 2003, 27, 1183–1196. [Google Scholar] [CrossRef] [PubMed]
- Naggar, A.; Batsakis, J.G.; Luna, M.A.; Goepfert, H.; Tortoledo, M.E. DNA content and proliferative activity of myoepitheliomas. J. Laryngol. Otol. 1989, 103, 1192–1197. [Google Scholar] [CrossRef]
- El Hallani, S.; Udager, A.M.; Bell, D.; Fonseca, I.; Thompson, L.D.R.; Assaad, A.; Agaimy, A.; Luvison, A.M.; Miller, C.; Seethala, R.R.; et al. Epithelial-myoepithelial carcinoma: Frequent morphologic and molecular evidence of preexisting pleomorphic adenoma, common HRAS mutations in PLAG1-intact and HMGA2-intact cases, and occasional TP53, FBXW7, and SMARCB1 alterations in high-grade cases. Am. J. Surg. Pathol. 2018, 42, 18–27. [Google Scholar] [CrossRef]
- Hernandez-Prera, J.C.; Skálová, A.; Franchi, A.; Rinaldo, A.; Poorten, V.V.; Zbären, P.; Ferlito, A.; Wenig, B.M. Pleomorphic adenoma: The great mimicker of malignancy. Histopatholopy 2021, 79, 279–290. [Google Scholar] [CrossRef]
- Eneroth, C.M. Histological and clinical aspects of parotid tumours. Acta Otolaryngol. Suppl. 1964, 188, 1–99. [Google Scholar]
- Phillips, P.P.; Olsen, K.D. Recurrent pleomorphic adenoma of the parotid gland: A report of 126 cases and a review of the literature. Ann. Otol. Rhinol. Laryngol. 1995, 104, 100–104. [Google Scholar] [CrossRef]
- Gerughty, R.M.; Scofield, H.H.; Brown, F.M.; Hennigar, G.R. Malignant mixed tumors of salivary gland origin. Cancer 1969, 24, 471–486. [Google Scholar] [CrossRef]
- Nakaguro, M.; Tanigawa, M.; Hirai, H.; Yamamoto, Y.; Urano, M.; Takahashi, R.H.; Sukeda, A.; Okumura, Y.; Honda, S.; Tasaki, K.; et al. The Diagnostic Utility of RAS Q61R Mutation-specific Immunohistochemistry in Epithelial-Myoepithelial Carcinoma. Am. J. Surg. Pathol. 2021, 45, 885–894. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Case No. | Author/Year | Age | Sex | Subsite | Size (mm) | cT | cN | Surgery | Surgical Margin Status | Adjuvant Treatment (Gy) | Local Recurrence | Metastasis | Prognosis | Disease Duration (Month) | f/u Duration (Month) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Wang, et al./2020 | 29 | F | palate | n/a | 1 | 0 | R | n/a | - | - | - | Alive | n/a | 84 |
| 2 | 41 | F | oropharynx | n/a | 2 | 0 | R | n/a | - | - | - | Alive | 48 | ||
| 3 | 52 | M | palate | n/a | 1 | 0 | R | n/a | R (n/a) | - | - | Alive | 24 | ||
| 4 | Lee, et al./2020 | 75 | F | nasal septum | 37 × 25 | 2 | 0 | R | n/a | - | - | - | Alive | 36 | 18 |
| 5 | Palaniappan, et al./2019 | 58 | F | palate | 15 × 15 | 1 | 0 | PM | N | - | - | - | Alive | 1 | 12 |
| 6 | Tsuji, et al./2016 | 71 | M | buccal | 19 × 15 | 1 | 0 | R | P | R (60) | - | - | Alive | 48 | 48 |
| 7 | Oh, et al./2016 | 78 | F | subglottis | 10 × 10 | 1 | 0 | R | N | - | - | - | Alive | 1 | 12 |
| 8 | Sedassari, et al./2015 | 42 | M | palate | n/a | 4 | 0 | R | P | - | - | - | Alive | n/a | 18 |
| 9 | 56 | F | palate | n/a | 4 | 0 | R | P | R (n/a) | + | - | Death | 48 | ||
| 10 | 70 | M | buccal | n/a | 3 | 0 | R | P | R (n/a) | + | - | Alive | 12 | ||
| 11 | Lima, et al./2012 | 61 | M | buccal | 20 × 20 | 2 | 0 | R | N | - | n/a | n/a | Alive | 96 | n/a |
| 12 | Angiero, et al./2009 | 83 | M | palate | 15 × 15 | 1 | 0 | R | N | - | - | - | Alive | n/a | 15 |
| 13 | 58 | F | palate | 35 × 20 | 2 | 0 | R | N | - | - | - | Alive | n/a | 13 | |
| 14 | 75 | M | buccal | 25 × 25 | 2 | 0 | R | N | - | - | - | Alive | 6 | 6 | |
| 15 | Teppo, et al./2008 | 53 | M | h/palate | 15 × 15 | 1 | 0 | R | N | R (60) | - | - | Alive | n/a | 54 |
| 16 | Yamanegi, et al./2008 | 70 | F | nasal cavity | 36 × 30 | 2 | 0 | R | N | - | - | - | Alive | 3 | 12 |
| 17 | Inoue, et al./2001 | 66 | F | palate | 20 × 20 | 2 | 0 | PM | N | - | - | - | Alive | 12 | 24 |
| 18 | Li, et al./2000 | 72 | F | palate | 26 × 20 | 2 | 0 | R | N | - | - | - | Alive | n/a | 24 |
| 19 | Present case 1./2021 | 75 | F | palate | 25 × 20 | 2 | 0 | R | N | - | - | - | Alive | 15 | 31 |
| 20 | Present case 2./2021 | 44 | F | palate | 18 × 16 | 1 | 0 | R | N | - | - | - | Alive | 6 | 16 |
| Case No. | CK (Details Unknown) | CK 5/6 | CK 7 | pan-CK | CK CAM5.2 | EMA | CD 10/117 | p63 | CEA | Vimentin | S-100 | α-SMA | Calponin | GFAP | PCNA | Actin | Laminin | Type IV Collagen | PAS | Ki-67 Labeling Index (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | + | + | + | + | ++ | n/a | ||||||||||||||
| 2 | + | + | + | + | ++ | n/a | ||||||||||||||
| 3 | + | + | + | + | ++ | n/a | ||||||||||||||
| 4 | ++ | + | + | 4 | ||||||||||||||||
| 5 | ++ | ++ | - | + | n/a | |||||||||||||||
| 6 | + | + | + | + | + | + | + | + | n/a | |||||||||||
| 7 | ++ | + | + | n/a | ||||||||||||||||
| 8 | + | + | ++ | + | + | + | 40 | |||||||||||||
| 9 | + | + | ++ | + | + | + | 40 | |||||||||||||
| 10 | + | + | ++ | + | + | + | 40 | |||||||||||||
| 11 | + | + | + | 25 | ||||||||||||||||
| 12 | + | + | ++ | ++ | + | ++ | - | + | - | + | - | 10 | ||||||||
| 13 | + | ++ | ++ | ++ | + | ++ | - | + | + | + | - | 5 | ||||||||
| 14 | + | ++ | ++ | ++ | + | ++ | - | + | - | + | - | 10 | ||||||||
| 15 | + | + | + | + | + | + | + | + | 30 | |||||||||||
| 16 | + | + | + | + | 10 | |||||||||||||||
| 17 | + | + | + | + | + | n/a | ||||||||||||||
| 18 | + | + | + | + | ++ | + | + | + | n/a | |||||||||||
| 19 | + | + | + | + | + | + | 11 | |||||||||||||
| 20 | + | + | + | + | + | + | 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okuyama, K.; Michi, Y.; Kashima, Y.; Tomioka, H.; Hirai, H.; Yokokawa, M.; Yamagata, Y.; Kuroshima, T.; Sato, Y.; Tsuchiya, M.; et al. Epithelial-Myoepithelial Carcinoma of the Minor Salivary Glands: Case Series with Comprehensive Review. Diagnostics 2021, 11, 2124. https://doi.org/10.3390/diagnostics11112124
Okuyama K, Michi Y, Kashima Y, Tomioka H, Hirai H, Yokokawa M, Yamagata Y, Kuroshima T, Sato Y, Tsuchiya M, et al. Epithelial-Myoepithelial Carcinoma of the Minor Salivary Glands: Case Series with Comprehensive Review. Diagnostics. 2021; 11(11):2124. https://doi.org/10.3390/diagnostics11112124
Chicago/Turabian StyleOkuyama, Kohei, Yasuyuki Michi, Yoshihisa Kashima, Hirofumi Tomioka, Hideaki Hirai, Misaki Yokokawa, Yuko Yamagata, Takeshi Kuroshima, Yuriko Sato, Maiko Tsuchiya, and et al. 2021. "Epithelial-Myoepithelial Carcinoma of the Minor Salivary Glands: Case Series with Comprehensive Review" Diagnostics 11, no. 11: 2124. https://doi.org/10.3390/diagnostics11112124