
Computed Tomography Angiography (CTA) before Reconstructive Jaw Surgery Using Fibula Free Flap: Retrospective Analysis of Vascular Architecture

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
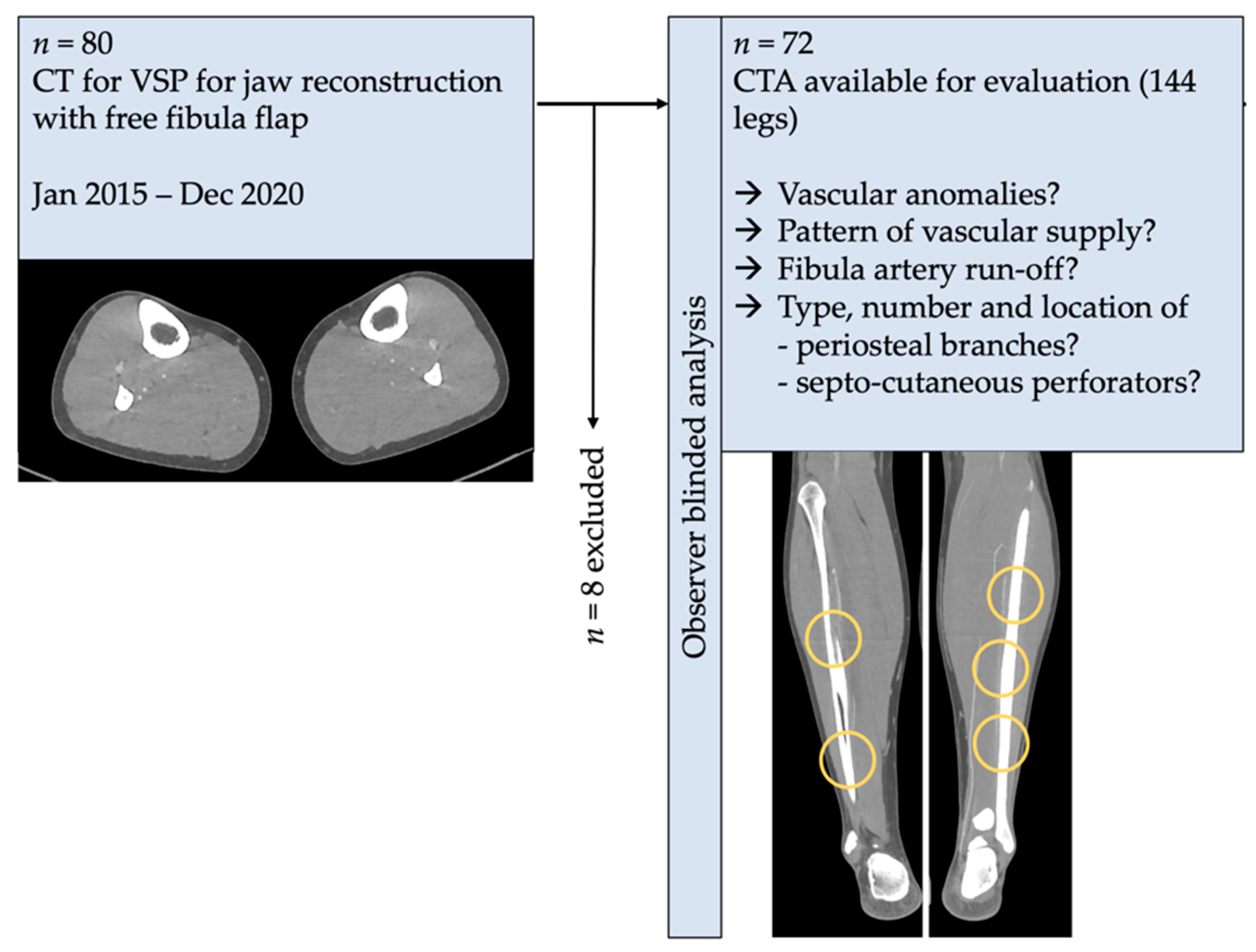
2.1. Study Design and Patient Population
2.2. Inclusion and Exclusion Criteria for Study Subjects
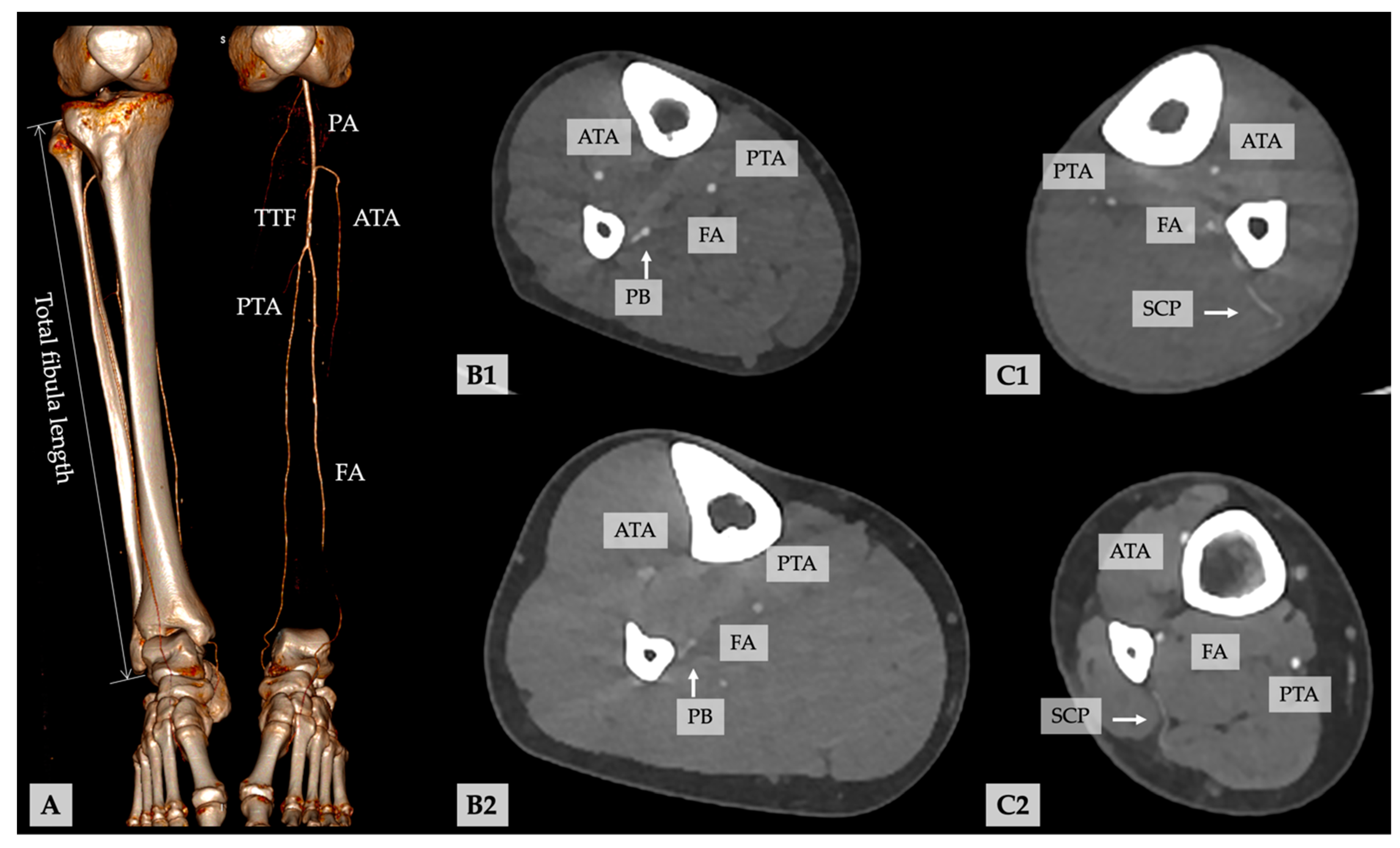
2.3. Methods, Study Parameters, and Evaluator Calibration
2.4. Statistical Analyses
2.5. Ethics Statement/Confirmation of Patients’ Permission
3. Results
4. Discussion
4.1. What Is the Prevalence of Vascular Anomalies in the Present Sample?
4.2. Is It Possible to Record and to Distinguish Periosteal Branches and Septo-Cutaneous Perforators of the FA, and up to Which Diameter Can These Vessels Be Detected in Routinely Run Preoperative CTA for VSP?
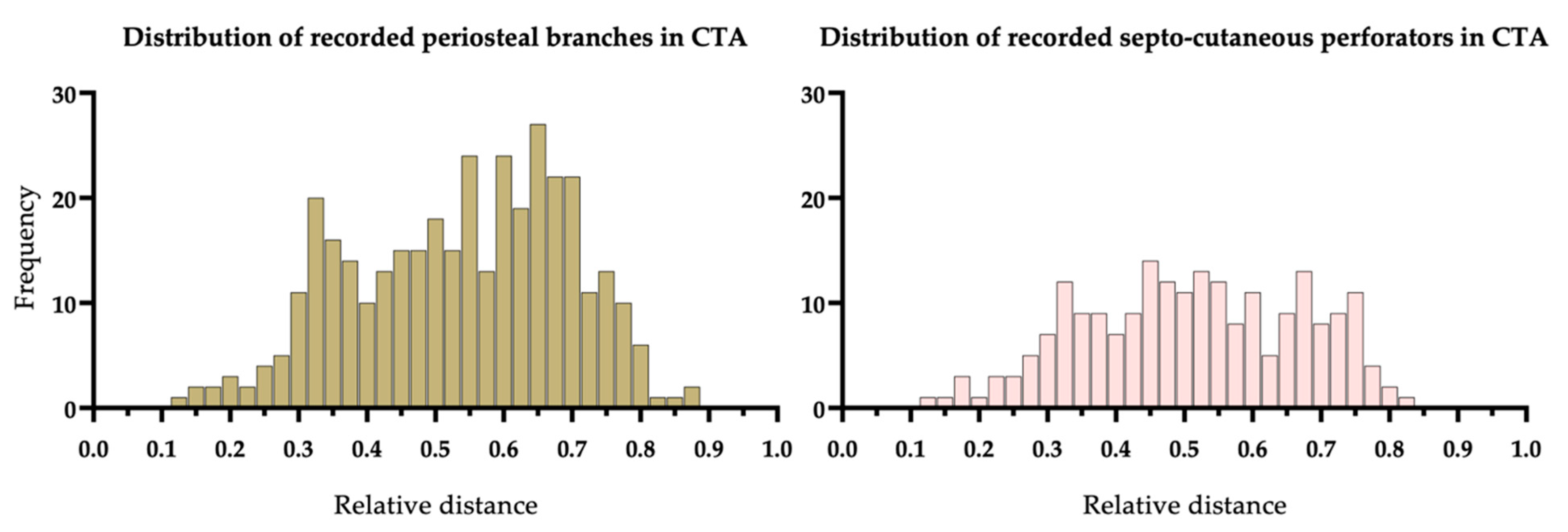
4.3. What Is the Frequency and Distribution of PBs and SCPs of the FA?
4.4. Limitations of the Study
4.5. Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Taylor, G.I.; Miller, G.D.H.; Ham, F.J. The free vascularized bone graft: A clinical extension of microvascular techniques. Plast. Reconstr. Surg. 1975, 55, 533–544. [Google Scholar] [CrossRef]
- Hidalgo, A.D. Fibula free flap: A new method of mandible reconstruction. Plast. Reconstr. Surg. 1989, 84, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Cordeiro, P.G.; Disa, J.J.; Hidalgo, D.A.; Hu, Q.Y. Reconstruction of the mandible with osseous free flaps: A 10-year experience with 150 consecutive patients. Plast. Reconstr. Surg. 1999, 104, 1314–1320. [Google Scholar] [CrossRef] [PubMed]
- Kumar, B.P.; Venkatesh, V.; Kumar, K.A.J.; Yadav, B.Y.; Mohan, S.R. Mandibular reconstruction: Overview. J. Maxillofac. Oral Surg. 2015, 15, 425–441. [Google Scholar] [CrossRef] [PubMed]
- Nyberg, M.; Karlsson, T.; Thórarinsson, A.; Kjeller, G.; Lidén, M.; Fröjd, V.; Löfstrand, J. Quality of life after free fibula flap reconstruction of segmental mandibular defects. J. Reconstr. Microsurg. 2017, 34, 108–120. [Google Scholar] [CrossRef] [PubMed]
- Tarsitano, A.; Ciocca, L.; Cipriani, R.; Scotti, R.; Marchetti, C. Mandibular reconstruction using fibula free flap harvested using a customised cutting guide: How we do it. Acta Otorhinolaryngol. Ital. 2015, 35, 198–201. [Google Scholar]
- Attia, S.; Wiltfang, J.; Streckbein, P.; Wilbrand, J.-F.; El Khassawna, T.; Mausbach, K.; Howaldt, H.-P.; Schaaf, H. Functional and aesthetic treatment outcomes after immediate jaw reconstruction using a fibula flap and dental implants. J. Cranio Maxillofac. Surg. 2019, 47, 786–791. [Google Scholar] [CrossRef] [PubMed]
- Petrovic, I.; Baser, R.; Blackwell, T.; McCarthy, C.; Ganly, I.; Patel, S.; Cordeiro, P.; Shah, J. Long-term functional and esthetic outcomes after fibula free flap reconstruction of the mandible. Head Neck 2019, 41, 2123–2132. [Google Scholar] [CrossRef] [Green Version]
- Hölzle, F.; Franz, E.P.; von Diepenbroick, V.H.; Wolff, K.D. Evaluation of the lower leg vessels before microsurgical fibula transfer—Magnetic resonance angiography versus digital subtraction angiography. Mund Kiefer Gesichtschir. 2003, 7, 246–253. [Google Scholar] [CrossRef]
- Hölzle, F.; Ristow, O.; Rau, A.; Mücke, T.; Loeffelbein, D.J.; Mitchell, D.A.; Wolff, K.D.; Kesting, M.R. Evaluation of the vessels of the lower leg before microsurgical fibular transfer. Part I: Anatomical variations in the arteries of the lower leg. Br. J. Oral Maxillofac. Surg. 2011, 49, 270–274. [Google Scholar] [CrossRef]
- Young, D.; Trabulsy, P.; Anthony, J. The Need for preoperative leg angiography in fibula free flaps. J. Reconstr. Microsurg. 1994, 10, 283–287. [Google Scholar] [CrossRef]
- Kelly, A.M.; Cronin, P.; Hussain, H.K.; Londy, F.J.; Chepeha, D.B.; Carlos, R.C. Preoperative MR angiography in free fibula flap transfer for head and neck cancer: Clinical application and influence on surgical decision making. Am. J. Roentgenol. 2007, 188, 268–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosson, G.D.; Singh, N.K. Devascularizing complications of free fibula harvest: Peronea arteria magna. J. Reconstr. Microsurg. 2005, 21, 533–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abou-Foul, A.; Fasanmade, A.; Prabhu, S.; Borumandi, F. Anatomy of the vasculature of the lower leg and harvest of a fibular flap: A systematic review. Br. J. Oral Maxillofac. Surg. 2017, 55, 904–910. [Google Scholar] [CrossRef] [PubMed]
- Battaglia, S.; Maiolo, V.; Savastio, G.; Zompatori, M.; Contedini, F.; Antoniazzi, E.; Cipriani, R.; Marchetti, C.; Tarsitano, A. Osteomyocutaneous fibular flap harvesting: Computer-assisted planning of perforator vessels using Computed Tomographic Angiography scan and cutting guide. J. Cranio Maxillofac. Surg. 2017, 45, 1681–1686. [Google Scholar] [CrossRef]
- Ribuffo, D.; Atzeni, M.; Saba, L.; Guerra, M.; Mallarini, G.; Proto, E.B.; Grinsell, D.; Ashton, M.W.; Rozen, W.M. Clinical study of peroneal artery perforators with computed tomographic angiography: Implications for fibular flap harvest. Surg. Radiol. Anat. 2010, 32, 329–334. [Google Scholar] [CrossRef]
- Abou-Foul, A.K.; Borumandi, F. Anatomical variants of lower limb vasculature and implications for free fibula flap: Systematic review and critical analysis. Microsurgery 2016, 36, 165–172. [Google Scholar] [CrossRef]
- Ettinger, K.S.; Alexander, A.E.; Arce, K. Computed Tomographic angiography perforator localization for virtual surgical planning of osteocutaneous fibular free flaps in head and neck reconstruction. J. Oral Maxillofac. Surg. 2018, 76, 2220–2230. [Google Scholar] [CrossRef] [Green Version]
- Wales, C.J.; Morrison, J.; Drummond, R.; Devine, J.C.; McMahon, J. Pre-operative evaluation of vascularised fibula donor sites: A UK maxillofacial e-survey. Br. J. Oral Maxillofac. Surg. 2010, 48, 192–194. [Google Scholar] [CrossRef]
- Akashi, M.; Nomura, T.; Sakakibara, S.; Sakakibara, A.; Hashikawa, K. Preoperative MR angiography for free fibula osteocutaneous flap transfer. Microsurgery 2013, 33, 454–459. [Google Scholar] [CrossRef]
- Schuderer, J.; Meier, J.; Klingelhöffer, C.; Gottsauner, M.; Reichert, T.; Wendl, C.; Ettl, T. Magnetic resonance angiography for free fibula harvest: Anatomy and perforator mapping. Int. J. Oral Maxillofac. Surg. 2020, 49, 176–182. [Google Scholar] [CrossRef]
- Sendeski, M.M.; Persson, A.B.; Liu, Z.Z.; Busch, J.F.; Weikert, S.; Persson, P.; Hippenstiel, S.; Patzak, A. Iodinated contrast media cause endothelial damage leading to vasoconstriction of human and rat vasa recta. Am. J. Physiol. Physiol. 2012, 303, F1592–F1598. [Google Scholar] [CrossRef] [Green Version]
- Levy, E.M.; Viscoli, C.M.; Horwitz, I.R. The effect of acute renal failure on mortality—A cohort analysis. JAMA 1996, 275, 1489–1494. [Google Scholar] [CrossRef]
- McCullough, A.P.; Wolyn, R.; Rocher, L.L.; Levin, R.N.; O’Neill, W.W. Acute renal failure after coronary intervention: Incidence, risk factors, and relationship to mortality. Am. J. Med. 1997, 103, 368–375. [Google Scholar] [CrossRef]
- Mitchell, A.M.; Kline, J.A.; Jones, A.E.; Tumlin, J.A. Major Adverse events one year after acute kidney injury after contrast-enhanced computed tomography. Ann. Emerg. Med. 2015, 66, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Ten Dam, M.A.; Wetzels, J.F. Toxicity of contrast media: An update. Neth. J. Med. 2008, 66, 416–422. [Google Scholar] [PubMed]
- Napoli, A.; Anzidei, M.; Zaccagna, F.; Marincola, B.C.; Zini, C.; Brachetti, G.; Cartocci, G.; Fanelli, F.; Catalano, C.; Passariello, R. Peripheral arterial occlusive disease: Diagnostic performance and effect on therapeutic management of 64-Section CT angiography. Radiology 2011, 261, 976–986. [Google Scholar] [CrossRef] [PubMed]
- Shwaiki, O.; Rashwan, B.; Fink, M.A.; Kirksey, L.; Gadani, S.; Karuppasamy, K.; Melzig, C.; Thompson, D.; D’Amico, G.; Rengier, F.; et al. Lower extremity CT angiography in peripheral arterial disease: From the established approach to evolving technical developments. Int. J. Cardiovasc. Imaging 2021, 1–14. [Google Scholar] [CrossRef]
- Rozen, W.M.; Phillips, T.; Ashton, M.W.; Stella, D.; Gibson, R.N.; Taylor, G.I. Preoperative imaging for diea perforator flaps: A comparative study of computed tomographic angiography and doppler ultrasound. Plast. Reconstr. Surg. 2008, 121, 1–8. [Google Scholar] [CrossRef]
- Razek, A.A.; Denewer, A.; Hegazy, M.; Hafez, M. Role of computed tomography angiography in the diagnosis of vascular stenosis in head and neck microvascular free flap reconstruction. Int. J. Oral Maxillofac. Surg. 2014, 43, 811–815. [Google Scholar] [CrossRef]
- Garvey, P.B.; Chang, E.I.; Selber, J.C.; Skoracki, R.J.; Madewell, J.E.; Liu, J.; Yu, P.; Hanasono, M.M. A prospective study of preoperative computed tomographic angiographic mapping of free fibula osteocutaneous flaps for head and neck reconstruction. Plast. Reconstr. Surg. 2012, 130, 541e–549e. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukaya, E.; Saloner, D.; León, P.; Wintermark, M.; Grossman, R.F.; Nozaki, M. Magnetic resonance angiography to evaluate septocutaneous perforators in free fibula flap transfer. J. Plast. Reconstr. Aesthetic Surg. 2010, 63, 1099–1104. [Google Scholar] [CrossRef] [PubMed]
- Varga-Szemes, A.; Wichmann, J.L.; Schoepf, U.J.; Suranyi, P.; De Cecco, C.N.; Muscogiuri, G.; Caruso, D.; Yamada, R.T.; Litwin, S.E.; Tesche, C.; et al. Accuracy of noncontrast quiescent-interval single-shot lower extremity MR angiography versus CT angiography for diagnosis of peripheral artery disease: Comparison with digital subtraction angiography. JACC Cardiovasc. Imaging 2017, 10, 1116–1124. [Google Scholar] [CrossRef] [PubMed]
- Jens, S.; Koelemay, M.J.W.; Reekers, J.A.; Bipat, S. Diagnostic performance of computed tomography angiography and contrast-enhanced magnetic resonance angiography in patients with critical limb ischaemia and intermittent claudication: Systematic review and meta-analysis. Eur. Radiol. 2013, 23, 3104–3114. [Google Scholar] [CrossRef] [PubMed]
- Wilde, F.; Hanken, H.; Probst, F.; Schramm, A.; Heiland, M.; Cornelius, C.-P. Multicenter study on the use of patient-specific CAD/CAM reconstruction plates for mandibular reconstruction. Int. J. Comput. Assist. Radiol. Surg. 2015, 10, 2035–2051. [Google Scholar] [CrossRef]
- Wilde, F.; Winter, K.; Kletsch, K.; Lorenz, K.; Schramm, A. Mandible reconstruction using patient-specific pre-bent reconstruction plates: Comparison of standard and transfer key methods. Int. J. Comput. Assist. Radiol. Surg. 2015, 10, 129–140. [Google Scholar] [CrossRef]
- Wilde, F.; Schramm, A. Computer-aided reconstruction of the facial skeleton: Planning and implementation in clinical routine. HNO 2016, 64, 641–649. [Google Scholar] [CrossRef]
- Cornelius, C.-P.; Smolka, W.; Giessler, G.A.; Wilde, F.; Probst, F.A. Patient-specific reconstruction plates are the missing link in computer-assisted mandibular reconstruction: A showcase for technical description. J. Cranio Maxillofac. Surg. 2015, 43, 624–629. [Google Scholar] [CrossRef]
- Wilde, F.; Cornelius, C.-P.; Schramm, A. Computer-assisted mandibular reconstruction using a patient-specific reconstruction plate fabricated with computer-aided design and manufacturing techniques. Craniomaxillofac. Trauma Reconstr. 2014, 7, 158–166. [Google Scholar] [CrossRef] [Green Version]
- Geusens, J.; Sun, Y.; Luebbers, H.-T.; Bila, M.; Darche, V.; Politis, C. Accuracy of computer-aided design/computer-aided manufacturing-assisted mandibular reconstruction with a fibula free flap. J. Craniofacial Surg. 2019, 30, 2319–2323. [Google Scholar] [CrossRef]
- Kansy, K.; Mueller, A.A.; Mücke, T.; Kopp, J.-B.; Koersgen, F.; Wolff, K.D.; Zeilhofer, H.-F.; Hölzle, F.; Pradel, W.; Schneider, M.; et al. Microsurgical reconstruction of the head and neck—Current concepts of maxillofacial surgery in Europe. J. Cranio Maxillofac. Surg. 2014, 42, 1610–1613. [Google Scholar] [CrossRef]
- Shroff, S.S.; Nair, S.C.; Shah, A.; Kumar, B. Versatility of fibula free flap in reconstruction of facial defects: A center study. J. Maxillofac. Oral Surg. 2017, 16, 101–107. [Google Scholar] [CrossRef] [Green Version]
- Hölzle, F.; Kesting, M.; Hölzle, G.; Watola, A.; Loeffelbein, D.; Ervens, J.; Wolff, K.-D. Clinical outcome and patient satisfaction after mandibular reconstruction with free fibula flaps. Int. J. Oral Maxillofac. Surg. 2007, 36, 802–806. [Google Scholar] [CrossRef]
- Colletti, G.; Autelitano, L.; Rabbiosi, D.; Biglioli, F.; Chiapasco, M.; Mandalà, M.; Allevi, F. Technical refinements in mandibular reconstruction with free fibula flaps: Outcome-oriented retrospective review of 99 cases. Acta Otorhinolaryngol. Ital. 2014, 34, 342–348. [Google Scholar]
- Barry, C.; MacDhabheid, C.; Tobin, K.; Stassen, L.; Lennon, P.; Toner, M.; O’Regan, E.; Clark, J. ‘Out of house’ virtual surgical planning for mandible reconstruction after cancer resection: Is it oncologically safe? Int. J. Oral Maxillofac. Surg. 2021, 50, 999–1002. [Google Scholar] [CrossRef] [PubMed]
- Knitschke, M.; Bäcker, C.; Schmermund, D.; Böttger, S.; Streckbein, P.; Howaldt, H.-P.; Attia, S. Impact of planning method (conventional versus virtual) on time to therapy initiation and resection margins: A retrospective analysis of 104 immediate jaw reconstructions. Cancers 2021, 13, 3013. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.; Wang, L.; Tian, Z.; Qin, X.; Zhu, D.; Qin, J.; Shen, Y. Standardize routine angiography assessment of leg vasculatures before fibular flap harvest: Lessons of congenital and acquired vascular anomalies undetected by color Doppler and physical examinations. Acta Radiol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Goetze, E.; Kämmerer, P.W.; Al-Nawas, B.; Moergel, M. Integration of perforator vessels in CAD/CAM free fibula graft planning: A clinical feasibility study. J. Maxillofac. Oral Surg. 2020, 19, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Napel, S.; Rubin, G.D.; Jeffrey, R.B., Jr. STS-MIP: A new reconstruction technique for CT of the chest. J. Comput. Assist. Tomogr. 1993, 17, 832–838. [Google Scholar] [CrossRef] [PubMed]
- Prokop, M.; Shin, H.O.; Schanz, A.; Schaefer-Prokop, C.M. Use of maximum intensity projections in CT angiography: A basic review. Radiographics 1997, 17, 433–451. [Google Scholar] [CrossRef]
- Johnson, P.T.; Heath, D.G.; Kuszyk, B.S.; Fishman, E.K. CT angiography with volume rendering: Advantages and applications in splanchnic vascular imaging. Radiology 1996, 200, 564–568. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Orron, D.E.; Skillman, J.J. Surgical significance of popliteal arterial variants: A unified angiographic classification. Ann. Surg. 1989, 210, 776–781. [Google Scholar] [CrossRef] [PubMed]
- Freeman, G.H.; Halton, J.H. Note on an exact treatment of contingency, goodness of fit and other problems of significance. Biometrika 1951, 38, 141–149. [Google Scholar] [CrossRef]
- Oxford, L.; Ducic, Y. Use of fibula-free tissue transfer with preoperative 2-vessel runoff to the lower extremity. Arch. Facial Plast. Surg. 2005, 7, 261–264. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Burgos, A.; García-Tutor, E.; Bastarrika, G.; Cano, D.; Martínez-Cuesta, A.; Pina, L. Preoperative planning of deep inferior epigastric artery perforator flap reconstruction with multislice-CT angiography: Imaging findings and initial experience. J. Plast. Reconstr. Aesthetic Surg. 2006, 59, 585–593. [Google Scholar] [CrossRef]
- Chiu, W.-K.; Lin, W.-C.; Chen, S.-Y.; Tzeng, W.-D.; Liu, S.-C.; Lee, T.-P.; Chen, S.-G. Computed tomography angiography imaging for the chimeric anterolateral thigh flap in reconstruction of full thickness buccal defect. ANZ J. Surg. 2011, 81, 142–147. [Google Scholar] [CrossRef]
- Duymaz, A.; Karabekmez, F.E.; Vrtiska, T.J.; Mardini, S.; Moran, S.L. Free Tissue transfer for lower extremity reconstruction: A study of the role of computed angiography in the planning of free tissue transfer in the posttraumatic setting. Plast. Reconstr. Surg. 2009, 124, 523–529. [Google Scholar] [CrossRef]
- Gelati, C.; Miralles, M.E.L.; Morselli, P.G.; Fabbri, E.; Cipriani, R. Deep inferior epigastric perforator breast reconstruction with computer-aided design/computer-aided manufacturing sizers. Ann. Plast. Surg. 2020, 84, 24–29. [Google Scholar] [CrossRef]
- Higueras Sune, M.C.; Lopez Ojeda, A.; Narvaez Garcia, J.A.; De Albert De Las Vigo, M.; Roca Mas, O.; Perez Sidelnikova, D.; Carrasco Lopez, C.; Palacin Porte, J.A.; Serra Payro, J.M.; Vinals, J.M. Use of angioscanning in the surgical planning of perforator flaps in the lower extremities. J. Plast. Reconstr. Aesthetic Surg. 2011, 64, 1207–1213. [Google Scholar] [CrossRef]
- Masia, J.; Clavero, J.; Larrañaga, J.; Alomar, X.; Pons, G.; Serret, P. Multidetector-row computed tomography in the planning of abdominal perforator flaps. J. Plast. Reconstr. Aesthetic Surg. 2006, 59, 594–599. [Google Scholar] [CrossRef]
- Ngaage, L.M.; Hamed, R.; Oni, G.; Di Pace, B.; Ghorra, D.T.; Koo, B.B.C.; Malata, C.M. The Role of CT angiography in assessing deep inferior epigastric perforator flap patency in patients with pre-existing abdominal scars. J. Surg. Res. 2019, 235, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Prokop, M. Multislice CT angiography. Eur. J. Radiol. 2000, 36, 86–96. [Google Scholar] [CrossRef]
- Zhang, Y.; Pan, X.; Yang, H.; Yang, Y.; Huang, H.; Rui, Y. Computed tomography angiography for the chimeric anterolateral thigh flap in the reconstruction of the upper extremity. J. Reconstr. Microsurg. 2016, 33, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Yanik, B.; Bulbul, E.; Demirpolat, G. Variations of the popliteal artery branching with multidetector CT angiography. Surg. Radiol. Anat. 2015, 37, 223–230. [Google Scholar] [CrossRef]
- Futran, N.D.; Stack, B.C., Jr.; Zachariah, A.P. Ankle-arm index as a screening examination for fibula free tissue transfer. Ann. Otol. Rhinol. Laryngol. 1999, 108, 777–780. [Google Scholar] [CrossRef]
- Astarci, P.; Siciliano, S.; Verhelst, R.; Lacroix, V.; Noirhomme, P.; Rubay, J.; Poncelet, A.; Funken, J.; Glineur, D.; El Kourhy, G. Intra-operative acute leg ischaemia after free fibula flap harvest for mandible reconstruction. Acta Chir. Belg. 2006, 106, 423–426. [Google Scholar] [CrossRef]
- Sandhu, G.S.; Rezaee, R.P.; Wright, K.; Jesberger, J.A.; Griswold, M.A.; Gulani, V. Time-Resolved and bolus-chase MR angiography of the leg: Branching pattern analysis and identification of septocutaneous perforators. Am. J. Roentgenol. 2010, 195, 858–864. [Google Scholar] [CrossRef] [Green Version]
- Carroll, W.R.; Esclamado, R. Preoperative vascular imaging for the fibular osteocutaneous flap. Arch. Otolaryngol. Head Neck Surg. 1996, 122, 708–712. [Google Scholar] [CrossRef]
- Blackwell, K.E. Donor site evaluation for fibula free flap transfer. Am. J. Otolaryngol. 1998, 19, 89–95. [Google Scholar] [CrossRef]
- Seres, L.; Császár, J.; Borbély, L.; Vörös, E. Donor site digital subtraction angiography before mandible reconstruction with free fibula transplantation. Fogorvosi Szle. 2001, 94, 15–20. [Google Scholar]
- Doobay, A.V.; Anand, S.S. Sensitivity and specificity of the ankle–brachial index to predict future cardiovascular outcomes: A systematic review. Arter. Thromb. Vasc. Biol. 2005, 25, 1463–1469. [Google Scholar] [CrossRef] [Green Version]
- Yao, S.T.; Hobbs, J.T.; Irvine, W.T. Ankle pressure measurement in arterial disease of the lower extremities. Br. J. Surg. 1968, 55, 859–860. [Google Scholar] [PubMed]
- Fowkes, F.G.R. The measurement of atherosclerotic peripheral arterial disease in epidemiological surveys. Int. J. Epidemiol. 1988, 17, 248–254. [Google Scholar] [CrossRef]
- Fowkes, F.G.; Housley, E.; Macintyre, C.C.; Prescott, R.J.; Ruckley, C.V. Variability of ankle and brachial systolic pressures in the measurement of atherosclerotic peripheral arterial disease. J. Epidemiol. Community Health 1988, 42, 128–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anzidei, M.; Lucatelli, P.; Napoli, A.; Jens, S.; Saba, L.; Cartocci, G.; Sedati, P.; D’Adamo, A.; Catalano, C. CT angiography and magnetic resonance angiography findings after surgical and interventional radiology treatment of peripheral arterial obstructive disease. J. Cardiovasc. Comput. Tomogr. 2015, 9, 165–182. [Google Scholar] [CrossRef] [PubMed]
- Mishra, A.; Jain, N.; Bhagwat, A. CT Angiography of peripheral arterial disease by 256-slice scanner: Accuracy, advantages and disadvantages compared to digital subtraction angiography. Vasc. Endovasc. Surg. 2017, 51, 247–254. [Google Scholar] [CrossRef]
- Futran, N.D.; Stack, B.C., Jr.; Zaccardi, M.J. Preoperative color flow doppler imaging for fibula free tissue transfers. Ann. Vasc. Surg. 1998, 12, 445–450. [Google Scholar] [CrossRef] [PubMed]
- Klein, S.; Hage, J.J.; van der Horst, C.M.; Lagerweij, M. Ankle-arm index versus angiography for the preassessment of the fibula free flap. Plast. Reconstr. Surg. 2003, 111, 735–743. [Google Scholar] [CrossRef]
- Smith, R.B.; Thomas, R.D.; Funk, G.F. Fibula free flaps: The role of angiography in patients with abnormal results on preoperative color flow Doppler studies. Arch. Otolaryngol. Head Neck Surg. 2003, 129, 712–715. [Google Scholar] [CrossRef] [Green Version]
- Bartella, A.K.; Luderich, C.; Kamal, M.; Braunschweig, T.; Steegmann, J.; Modabber, A.; Kloss-Brandstätter, A.; Hölzle, F.; Lethaus, B. Ankle brachial index predicts for difficulties in performing microvascular anastomosis. J. Oral Maxillofac. Surg. 2020, 78, 1020–1026. [Google Scholar] [CrossRef]
- Aboyans, V.; Criqui, M.H.; Abraham, P.; Allison, M.A.; Creager, M.A.; Diehm, C.; Fowkes, F.G.R.; Hiatt, W.R.; Jönsson, B.; Lacroix, P.; et al. Measurement and interpretation of the ankle-brachial index: A scientific statement from the American Heart Association. Circulation 2012, 126, 2890–2909. [Google Scholar] [CrossRef] [Green Version]
- Moyer, V.A.; Force, U.P.S.T. Screening for peripheral artery disease and cardiovascular disease risk assessment with the ankle-brachial index in adults: U.S. preventive services task force recommendation statement. Ann. Intern. Med. 2013, 159, 342–348. [Google Scholar] [CrossRef] [Green Version]
- Yu, P.; Chang, E.I.; Hanasono, M.M. Design of a reliable skin paddle for the fibula osteocutaneous flap: Perforator anatomy revisited. Plast. Reconstr. Surg. 2011, 128, 440–446. [Google Scholar] [CrossRef]
- Fukaya, E.; Grossman, R.F.; Saloner, D.; Leon, P.; Nozaki, M.; Mathes, S.J. Magnetic resonance angiography for free fibula flap transfer. J. Reconstr. Microsurg. 2007, 23, 205–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, N.F.; Monstrey, S.; Gambier, B.A. Reliability of the fibular osteocutaneous flap for mandibular reconstruction: Anatomical and surgical confirmation. Plast. Reconstr. Surg. 1996, 97, 707–716. [Google Scholar] [CrossRef] [PubMed]
- Fry, A.; Laugharne, D.; Jones, K. Osteotomising the fibular free flap: An anatomical perspective. Br. J. Oral Maxillofac. Surg. 2016, 54, 692–693. [Google Scholar] [CrossRef] [PubMed]
- Yadav, P.S.; Ahmad, Q.G.; Shankhdhar, V.K.; Nambi, G. Skin paddle vascularity of free fibula flap—A study of 386 cases and a classification based on contribution from axial vessels of the leg. Indian J. Plast. Surg. 2012, 45, 58–61. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n = 72 Patients | n (%) | n = 144 Lower Limbs | p-Value |
|---|---|---|---|
| Age at CT-scan (years), mean ± SD | |||
| Male | 44 (61.1) | 56.8 ± 14.6 | |
| Female | 28 (38.9) | 61.1 ± 16.1 | 0.257 |
| Body weight (kilogram), mean ± SD | |||
| Male (range) | 44 (61.1) | 77.7 ± 15.7 (37.5–113.0) | |
| Female (range) | 28 (38.9) | 66.5 ± 14.1 (43.2–104.0) | 0.003 |
| Body height (cm), mean ± SD | |||
| Male (range) | 44 (61.1) | 177.5 ± 7.2 (159.8–198.0) | |
| Female (range) | 28 (38.9) | 161.4 ± 5.6 (150.0–176.0) | ≤0.001 |
| BMI (kg/m2), mean ± SD | |||
| Male (range) | 44 (61.1) | 24.6 ± 4.9 (14.7–40.0) | |
| Female (range) | 28 (38.9) | 25.4 ± 5.4 (17.3–40.0) | 0.518 |
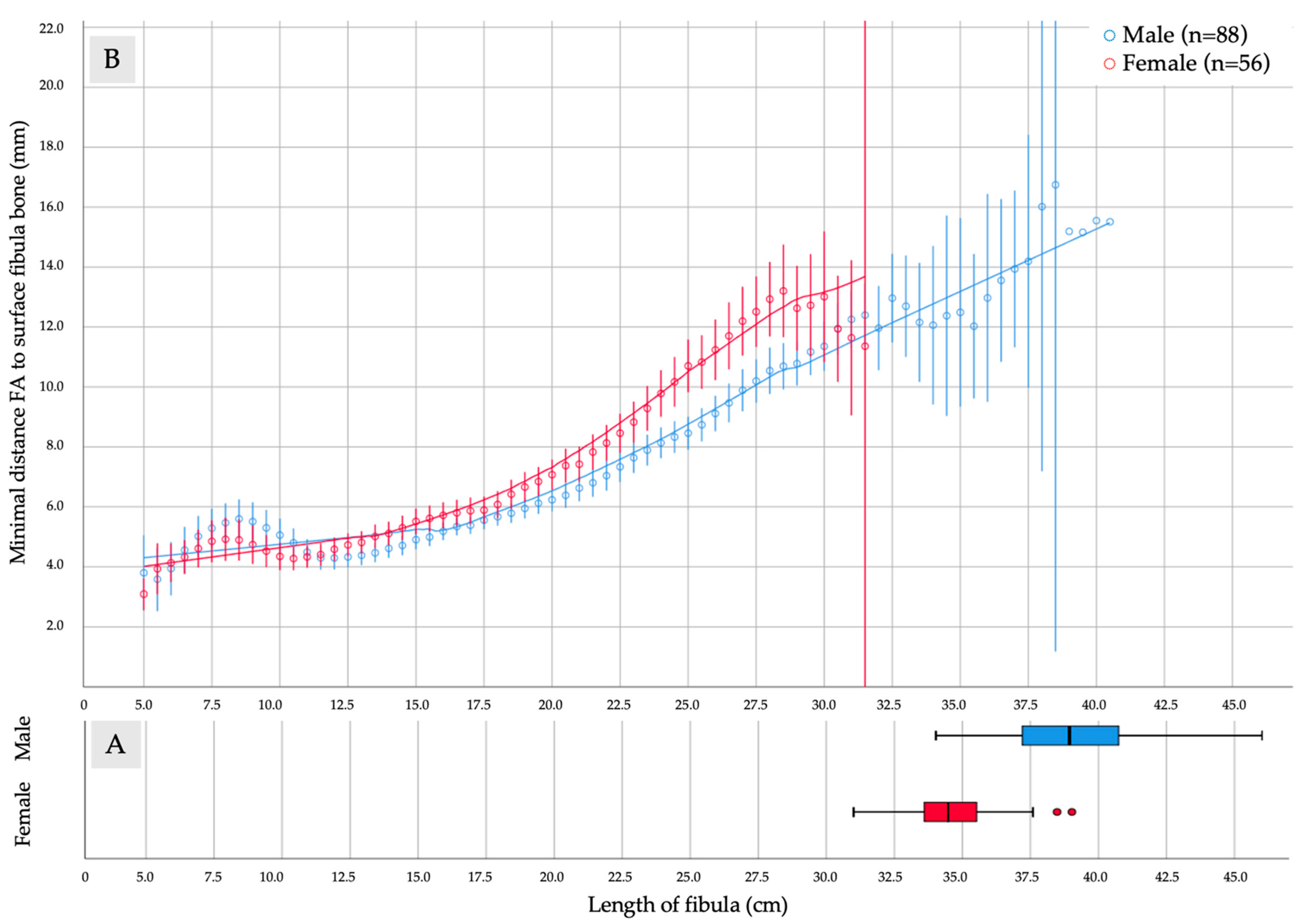
| Length of fibula, mean (mm) ± SD | |||
| Male (range) | 44 (61.1) | 390.8 ± 23.5 (340.2–460.1) | |
| Female (range) | 28 (38.9) | 346.0 ± 17.0 (310.0–390.2) | ≤0.001 |
| Length of TTF, mean (mm) ± SD ‡ | |||
| Male (range) | 80 (62.5) | 35.15 ± 14.07 (6.0–67.2) | |
| Female (range) | 48 (37.5) | 28.20 ± 11.51 (10.0–64.5) | 0.0045 |
| Diameter of TTF, mean (mm) ± SD ‡ | |||
| Male (range) | 80 (62.5) | 4.44 ± 1.00 (2.67–6.78) | |
| Female (range) | 48 (37.5) | 3.64 ± 0.65 (2.30–5.12) | ≤0.001 |
| Length of FA, mean (mm) ± SD | |||
| Male (range) | 44 (61.1) | 25.66 ± 3.72 (7.0–35.85) | |
| Female (range) | 28 (38.9) | 22.42 ± 3.65 (4.65–26.6) | ≤0.001 |
| Diameter of FA, mean (mm) ± SD | |||
| Male (range) | 44 (61.1) | 3.41 ± 0.78 (1.88–5.40) | |
| Female (range) | 28 (38.9) | 2.78 ± 0.64 (1.46–4.27) | ≤0.001 |
| Diameter of SCP, mean (mm) ± SD | |||
| Male (range) | 127 (59.6) | 0.91 ± 0.26 (0.53–1.82) | |
| Female (range) | 86 (40.4) | 0.96 ± 0.35 (0.52–2.43) | 0.233 |
| Diameter of PB, mean (mm) ± SD | |||
| Male (range) | 230 (63.7) | 0.88 ± 0.25 (0.40–1.89) | |
| Female (range) | 131 (36.3) | 0.86 ± 0.26 (0.35–2.26) | 0.472 |
| n = 144 | Left Fibula n = 72 | Right Fibula n = 72 | p-Value | Total |
|---|---|---|---|---|
| Fibula length, mean (mm) ± SD | 373.5 ± 30.8 | 373.2 ± 30.4 | 0.953 | 144 |
| Fibula bone anomalies, n | - | |||
| Fracture | 1 | 0 | 1 | |
| Infrapopliteal branching pattern [52] | - | |||
| Regular (I-A to II-C) | 68 | 72 | 140 | |
| Absent ATA (III-A) | 2 | - | 2 | |
| Absent PTA (III-B) | 2 | - | 2 | |
| Stenoses, n | - | |||
| ATA | 1 | - | 1 | |
| PTA | 2 | - | 2 | |
| FA | 5 | 6 | 11 | |
| Length of TTF, mean (mm) ± SD ‡ | 30.37 ± 12.78 | 35.03 ± 14.26 | 0.053 | 128 |
| Diameter of TTF, mean (mm) ± SD ‡ | 4.06 ± 0.92 | 4.14 ± 0.97 | 0.663 | 128 |
| Length of FA, mean (mm) ± SD | 244.5 ± 41.3 | 243.4 ± 39.2 | 0.809 | 144 |
| Diameter of FA, mean (mm) ± SD | 3.17 ± 0.80 | 3.16 ± 0.78 | 1.0 | 144 |
| Distance to the fibular bone, mean (mm) ± SD | 8.58 ± 3.74 | 8.55 ± 3.81 | 0.974 | 144 |
| Overall found SCP, n | 104 | 109 | 213 | |
| Mean SCP per fibula (mm) ± SD | 1.44 ± 1.10 | 1.51 ± 1.13 | 0.647 | 1.48 ± 1.12 |
| Overall found PB, n | 168 | 193 | 361 | |
| Mean PB per fibula (mm) ± SD | 2.33 ± 1.46 | 2.68 ± 1.62 | 0.033 | 2.51 ± 1.55 |
| Type n (%) | Left Leg, n = 72 | Right Leg, n = 72 | All, n = 144 |
|---|---|---|---|
| I-A | 63 (87.5) | 65 (90.3) | 128 (88.9) |
| I-B | 2 (2.8) | 1 (1.4) | 3 (2.1) |
| I-C | 1 (1.4) | - | 1 (0.7) |
| II-A | 1 (1.4) | 2 (2.8) | 3 (2.1) |
| II-B | 1 (1.4) | 4 (5.6) | 5 (3.6) |
| II-C | - | - | - |
| III-A | 2 (2.8) | - | 2 (1.4) |
| III-B | 2 (2.8) | - | 2 (1.4) |
| III-C | - | - | - |
| Size of Segment (cm)/Vessel Type | None | One | Two or More |
|---|---|---|---|
| 1.0 PB | 89.05% | 10.77% | 0.18% |
| 2.0 PB | 78.33% | 21.07% | 0.68% |
| 3.0 PB | 68.28% | 29.17% | 2.55% |
| 1.0 SCP | 93.54% | 6.46% | 0 |
| 2.0 SCP | 87.22% | 12.25% | 0.54% |
| 3.0 SCP | 81.28% | 17.84% | 0.88% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Knitschke, M.; Baumgart, A.K.; Bäcker, C.; Adelung, C.; Roller, F.; Schmermund, D.; Böttger, S.; Howaldt, H.-P.; Attia, S. Computed Tomography Angiography (CTA) before Reconstructive Jaw Surgery Using Fibula Free Flap: Retrospective Analysis of Vascular Architecture. Diagnostics 2021, 11, 1865. https://doi.org/10.3390/diagnostics11101865
Knitschke M, Baumgart AK, Bäcker C, Adelung C, Roller F, Schmermund D, Böttger S, Howaldt H-P, Attia S. Computed Tomography Angiography (CTA) before Reconstructive Jaw Surgery Using Fibula Free Flap: Retrospective Analysis of Vascular Architecture. Diagnostics. 2021; 11(10):1865. https://doi.org/10.3390/diagnostics11101865
Chicago/Turabian StyleKnitschke, Michael, Anna Katrin Baumgart, Christina Bäcker, Christian Adelung, Fritz Roller, Daniel Schmermund, Sebastian Böttger, Hans-Peter Howaldt, and Sameh Attia. 2021. "Computed Tomography Angiography (CTA) before Reconstructive Jaw Surgery Using Fibula Free Flap: Retrospective Analysis of Vascular Architecture" Diagnostics 11, no. 10: 1865. https://doi.org/10.3390/diagnostics11101865