Clinical Remission in a 72-Year-Old Patient with a Massive Primary Cutaneous Peripheral T-Cell Lymphoma-NOS of the Eyelid, Following Combination Chemotherapy with Etoposide Plus COP

 , , and
, , and
Abstract
:1. Introduction
2. Patient Information
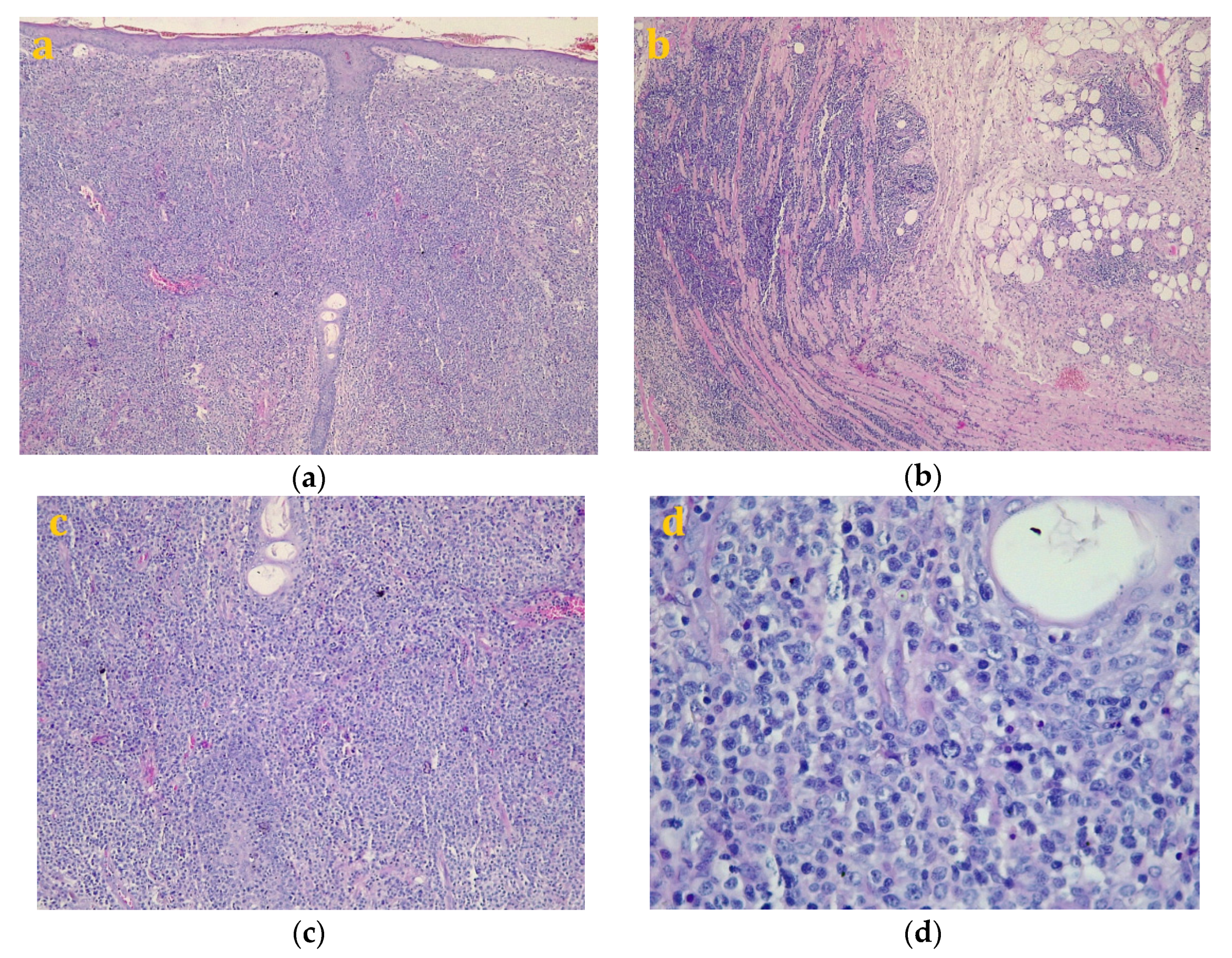
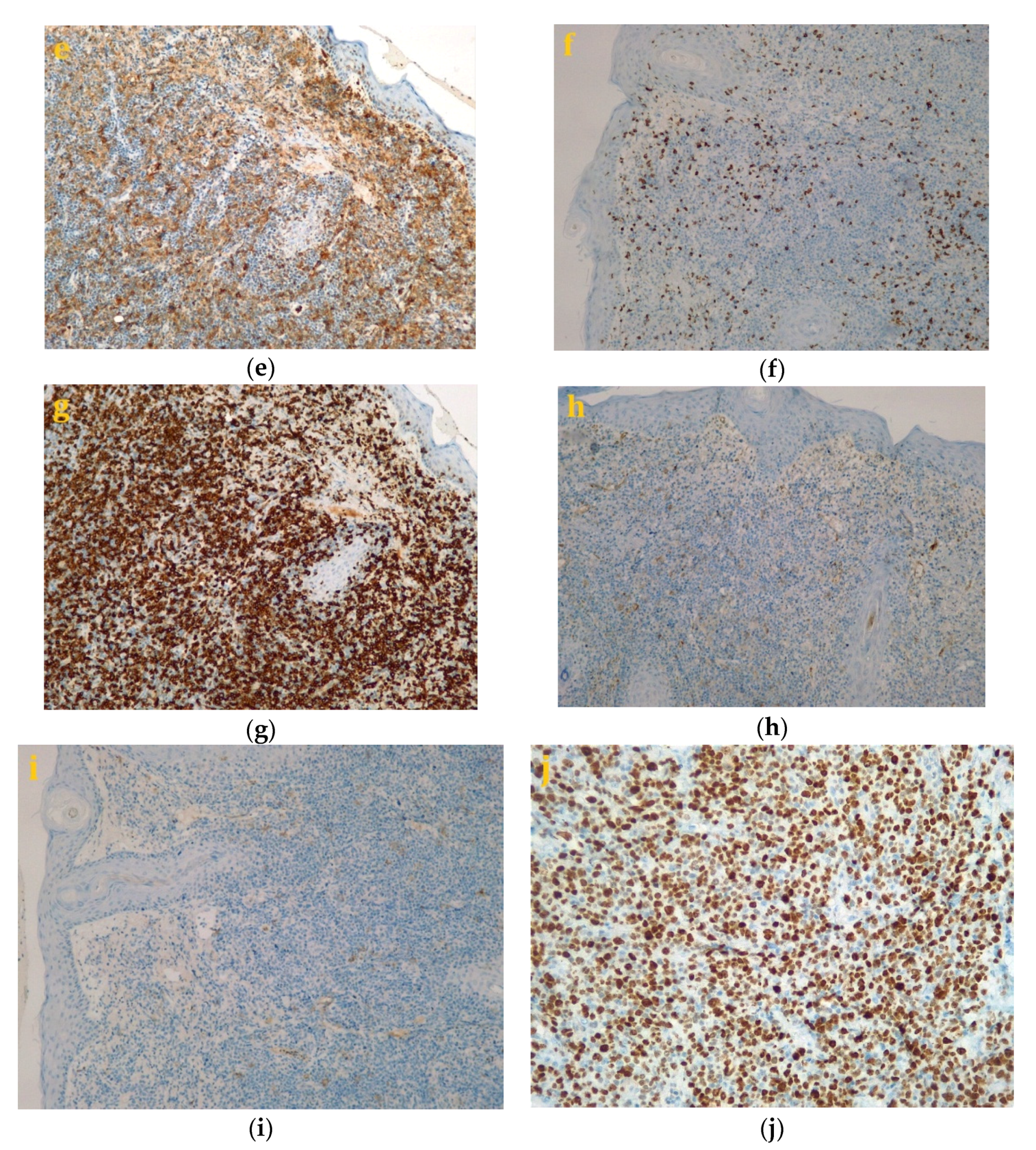
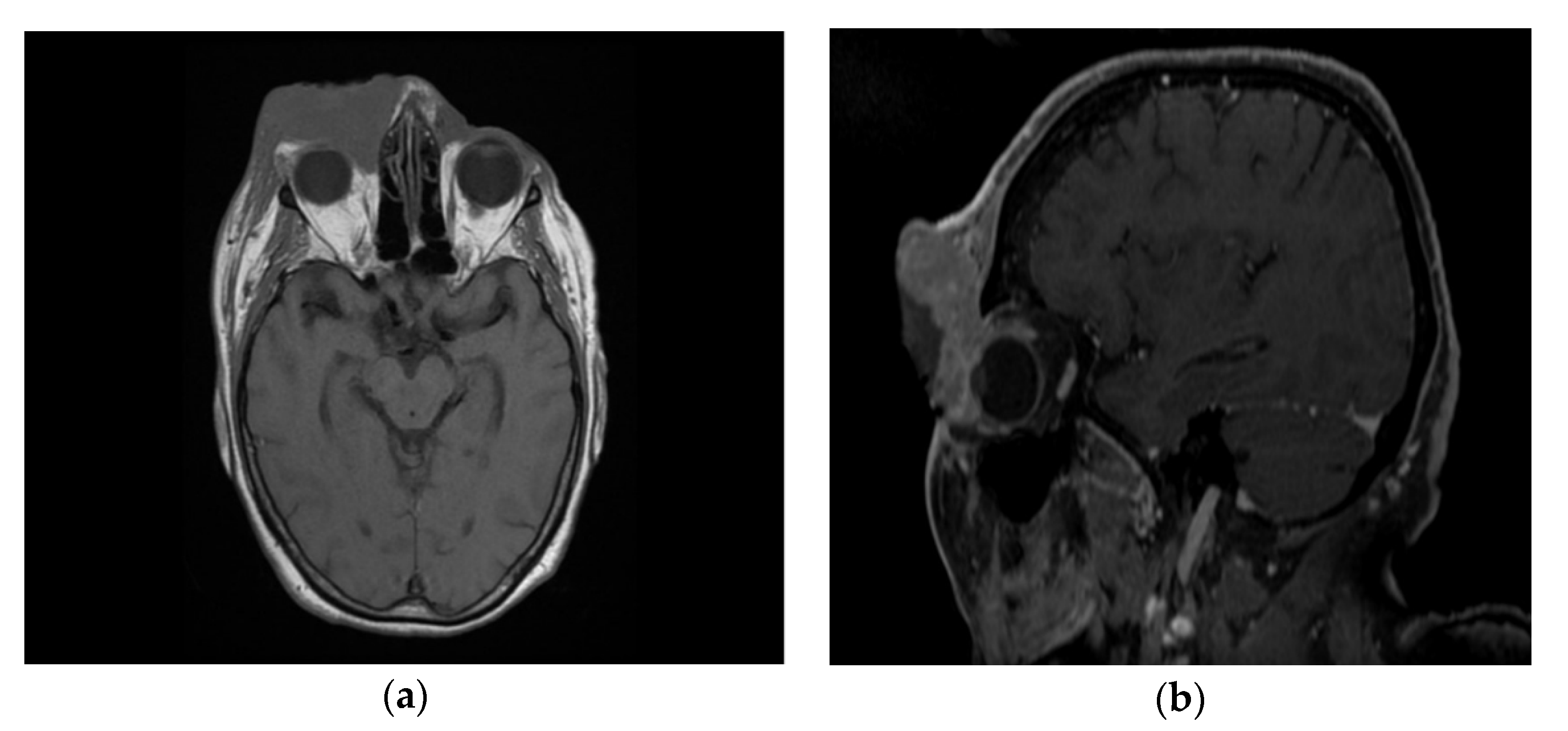
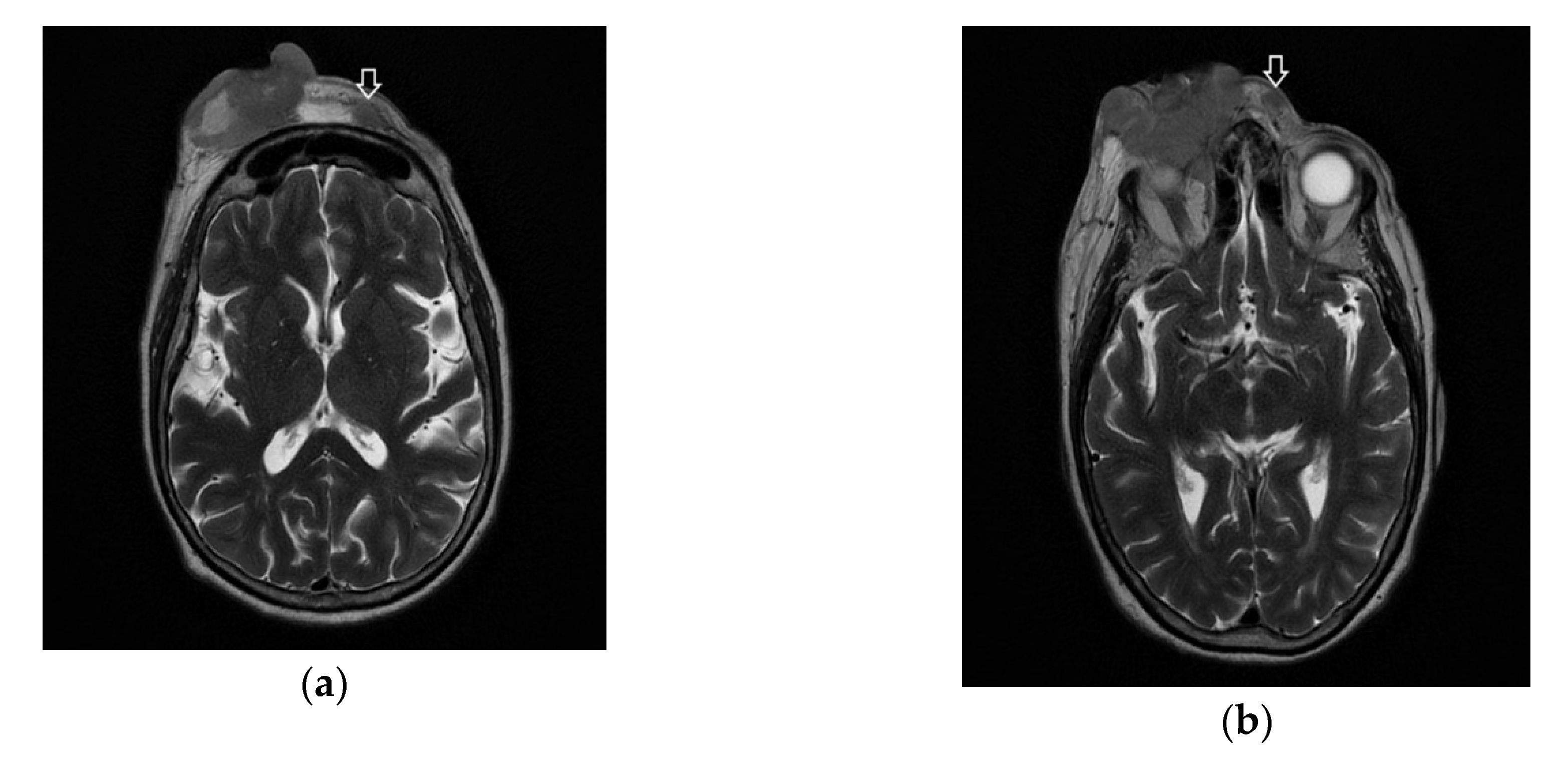
3. Diagnostics
4. Therapy
5. Follow-Up
6. Discussions
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cucuianu, A.; Petrushev, B.; Crisan, D.; Buiga, R.; Rosu, A.-M.; Dima, D.; Tomuleasa, C. Chronic granulomatous dermatosis as a presenting sign of cutaneous T-cell lymphomas. Eur. J. Dermatol. 2015, 25, 210. [Google Scholar] [CrossRef] [PubMed]
- Desmirean, M.; Deak, D.; Rus, I.; Dima, D.; Iluta, S.; Preda, A.; Moldovan, T.; Roman, A.; Tomuleasa, C.; Petrushev, B. Paraneoplastic hypereosinophilia in a patient with peripheral T cell lymphoma, not otherwise specified. Med. Pharm. Rep. 2019, 92, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Gafencu, G.A.; Selicean, S.E.; Petrushev, B.; Cucuianu, A.; Dima, D.; Frinc, I.; Irimie, A.; Pileczki, V.; Berindan-Neagoe, I.; Berce, C.; et al. Clinicopathological analysis of a case series of peripheral T-cell lymphomas, not otherwise specified, of lymphoepithelioid variant (Lennert’s lymphoma). A Central European single-center study. Hum. Pathol. 2016, 53, 192–194. [Google Scholar] [CrossRef] [PubMed]
- Ma, H.; Cheng, B.; Falchi, L.; Marchi, E.; Sawas, A.; Bhagat, G.; O’Connor, O.A. Survival benefit in patients with peripheral T-cell lymphomas after treatments with novel therapies and clinical trials. Hematol. Oncol. 2019, 38, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Zain, J.M. Aggressive T-cell lymphomas: 2019 updates on diagnosis, risk stratification, and management. Am. J. Hematol. 2019, 94, 929–946. [Google Scholar] [CrossRef] [Green Version]
- Janíková, A.; Chloupkova, R.; Campr, V.; Klener, P.; Hamouzova, J.; Belada, D.; Prochazka, V.; Pytlik, R.; Pirnos, J.; Duras, J.; et al. First-line therapy for T cell lymphomas: A retrospective population-based analysis of 906 T cell lymphoma patients. Ann. Hematol. 2019, 98, 1961–1972. [Google Scholar] [CrossRef]
- Siaghani, P.J.; Wong, J.T.; Chan, J.; Weisenburger, D.D.; Song, J.Y. Epidemiology and Pathology of T-and NK-Cell Lymphomas. Cancer Treat. Res. 2018, 176, 1–29. [Google Scholar] [CrossRef]
- Griesel, C.; Desmirean, M.; Esterhuizen, T.; Pașca, S.; Petrushev, B.; Selicean, C.; Roman, A.; Fetica, B.; Teodorescu, P.; Swanepoel, C.; et al. Differential Diagnosis of Malignant Lymphadenopathy Using Flow Cytometry on Fine Needle Aspirate: Report on 269 Cases. J. Clin. Med. 2020, 9, 283. [Google Scholar] [CrossRef] [Green Version]
- Willemze, R.; Cerroni, L.; Kempf, W.; Berti, E.; Facchetti, F.; Swerdlow, S.H.; Jaffe, E.S. The 2018 update of the WHO-EORTC classification for primary cutaneous lymphomas. Blood 2019, 133, 1703–1714. [Google Scholar] [CrossRef]
- Willemze, R.; Meijer, C.J. Classification of cutaneous T-cell lymphoma: From Alibert to WHO-EORTC. J. Cutan. Pathol. 2006, 33, 18–26. [Google Scholar] [CrossRef]
- Walia, R.; Yeung, C. An Update on Molecular Biology of Cutaneous T Cell Lymphoma. Front. Oncol. 2020, 9, 1558. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, C.R.; Zhao, S.; Sanches, J.A.; Miyashiro, D.; Cury-Martins, J.; Azevedo, R.S.; Zerbini, M.C.N.; Natkunam, Y.; Gratzinger, D. Clinicopathologic and microenvironmental analysis of primary cutaneous CD30-positive lymphoproliferative disorders: A 26 year experience from an academic medical center in Brazil. Diagn. Pathol. 2019, 14, 115–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martires, K.J.; Ra, S.; Abdulla, F.; Cassarino, D.S. Characterization of primary cutaneous CD8+/CD30+ lymphoproliferative disorders. Am. J. Dermatopathol. 2015, 37, 822–833. [Google Scholar] [CrossRef] [PubMed]
- Kempf, W. A new era for cutaneous CD30-positive T-cell lymphoproliferative disorders. Semin. Diagn. Pathol. 2017, 34, 22–35. [Google Scholar] [CrossRef]
- Szpor, J.; Dyduch, G.; Gałazka, K.; Bahyrycz, J.; Stój, A.; Tomaszewska, R. Primary cutaneous CD30+ lymphoproliferative disorder--a 10-year follow-up. A case report and differential diagnosis. Pol. J. Pathol. 2009, 60, 43–48. [Google Scholar] [PubMed]
- Kempf, W.; Kerl, K.; Mitteldorf, C. Cutaneous CD30-positive T-cell lymphoproliferative disorders—Clinical and histopathologic features, differential diagnosis, and treatment. Semin. Cutan. Med. Surg. 2018, 37, 24–29. [Google Scholar] [CrossRef]
- Rezania, D.; Sokol, L.; Cualing, H.D. Classification and treatment of rare and aggressive types of peripheral T-cell/natural killer-cell lymphomas of the skin. Cancer Control 2007, 14, 112–123. [Google Scholar] [CrossRef] [Green Version]
- Amber, K.T.; Bloom, R.; Nouri, K. Second Primary Malignancies in CTCL Patients from 1992 to 2011: A SEER-Based, Population-Based Study Evaluating Time from CTCL Diagnosis, Age, Sex, Stage, and CD30+ Subtype. Am. J. Clin. Dermatol. 2015, 17, 71–77. [Google Scholar] [CrossRef]
- Fujii, K.; Hamada, T.; Shimauchi, T.; Asai, J.; Fujisawa, Y.; Ihn, H.; Katoh, N. Cutaneous lymphoma in Japan, 2012–2017: A nationwide study. J. Dermatol. Sci. 2020, 97, 187–193. [Google Scholar] [CrossRef]
- Zhang, J.-C.; Wang, Y.; Wang, X.-F.; Zhang, F.-X. Type I enteropathy-associated T-cell lymphoma in the colon of a 29-year-old patient and a brief literature review. OncoTargets Ther. 2016, 9, 863–868. [Google Scholar] [CrossRef] [Green Version]
- Phan, A.; Veldman, R.; Lechowicz, M.J. T-cell Lymphoma Epidemiology: The Known and Unknown. Curr. Hematol. Malign. Rep. 2016, 11, 492–503. [Google Scholar] [CrossRef] [PubMed]
- Satou, A.; Asano, N.; Kato, S.; Katsuya, H.; Ishitsuka, K.; Elsayed, A.A.; Nakamura, S. FoxP3-positive T-cell Lymphoma Arising in non-HTLV1 carrier: Clinicopathological analysis of 11 cases of PTCL-NOS and 2 cases of Mycosis Fungoides. Histopathology 2015, 68, 1099–1108. [Google Scholar] [CrossRef] [PubMed]
- Jawed, S.I.; Myskowski, P.L.; Horwitz, S.; Moskowitz, A.; Querfeld, C. Primary cutaneous T-cell lymphoma (mycosis fungoides and Sézary syndrome): Part I. Diagnosis: Clinical and histopathologic features and new molecular and biologic markers. J. Am. Acad. Dermatol. 2014, 70, 205-e1. [Google Scholar] [CrossRef] [PubMed]
- Yumeen, S.; Girardi, M. Insights into the Molecular and Cellular Underpinnings of Cutaneous T Cell Lymphoma. Yale J. Biol. Med. 2020, 93, 111–121. [Google Scholar] [PubMed]
- Wilcox, R.A. Cutaneous T-cell lymphoma: 2017 update on diagnosis, risk-stratification, and management. Am. J. Hematol. 2017, 92, 1085–1102. [Google Scholar] [CrossRef] [Green Version]
- Wilcox, R.A. Cutaneous T-cell lymphoma: 2014 Update on diagnosis, risk-stratification, and management. Am. J. Hematol. 2014, 89, 837–851. [Google Scholar] [CrossRef]
- Jiang, M.; Bennani, N.N.; Feldman, A.L. Lymphoma classification update: T-cell lymphomas, Hodgkin lymphomas, and histiocytic/dendritic cell neoplasms. Expert Rev. Hematol. 2017, 10, 239–249. [Google Scholar] [CrossRef] [Green Version]
- Satou, A.; Bennani, N.N.; Feldman, A.L. Update on the classification of T-cell lymphomas, Hodgkin lymphomas, and histiocytic/dendritic cell neoplasms. Expert Rev. Hematol. 2019, 12, 833–843. [Google Scholar] [CrossRef]
- Marchi, E.; O’Connor, O.A. The rapidly changing landscape in mature T-cell lymphoma (MTCL) biology and management. CA A Cancer J. Clin. 2019, 70, 47–70. [Google Scholar] [CrossRef] [Green Version]
- Reddy, N.M.; Evens, A.M. Chemotherapeutic Advancements in Peripheral T-Cell Lymphoma. Semin. Hematol. 2014, 51, 17–24. [Google Scholar] [CrossRef]
- Choi, E.-J.; Hong, J.Y.; Yoon, D.H.; Kang, J.; Park, C.-S.; Huh, J.; Chae, E.J.; Lee, Y.; Ryu, J.-S.; Suh, C. Treatment outcomes of dose-attenuated CHOP chemotherapy in elderly patients with peripheral T cell lymphoma. Blood Res. 2017, 52, 270–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fox, C.P.; Civallero, M.; Ko, Y.-H.; Manni, M.; Skrypets, T.; Pileri, S.; Kim, S.J.; Cabrera, M.E.; Shustov, A.R.; Chiattone, C.S.; et al. Survival outcomes of patients with extranodal natural-killer T-cell lymphoma: A prospective cohort study from the international T-cell Project. Lancet Haematol. 2020, 7, e284–e294. [Google Scholar] [CrossRef]
- Tanase, A.D.; Colita, A.; Craciun, O.G.; Lipan, L.; Varady, Z.; Stefan, L.; Ranete, A.; Pasca, S.; Bumbea, H.; Andreescu, M.; et al. Allogeneic Stem Cell Transplantation for Adult T-Cell Leukemia/Lymphoma—Romanian Experience. J. Clin. Med. 2020, 9, 2417. [Google Scholar] [CrossRef] [PubMed]
- Colita, A.; Colita, A.; Bumbea, H.; Croitoru, A.; Orban, C.; Lipan, L.E.; Craciun, O.-G.; Soare, D.; Ghimici, C.; Manolache, R.; et al. LEAM vs. BEAM vs. CLV Conditioning Regimen for Autologous Stem Cell Transplantation in Malignant Lymphomas. Retrospective Comparison of Toxicity and Efficacy on 222 Patients in the First 100 Days after Transplant, On Behalf of the Romanian Society for Bone Marrow Transplantation. Front. Oncol. 2019, 9. [Google Scholar] [CrossRef]
- Grewal, R.-K.; Chetty, M.; Abayomi, E.-A.; Tomuleasa, C.; Fromm, J.R. Use of flow cytometry in the phenotypic diagnosis of hodgkin’s lymphoma. Cytom. Part B Clin. Cytom. 2018, 96, 116–127. [Google Scholar] [CrossRef]
- Grewal, R.; Irimie, A.; Naidoo, N.; Mohamed, N.; Petrushev, B.; Chetty, M.; Tomuleasa, C.; Abayomi, E.-A. Hodgkin’s lymphoma and its association with EBV and HIV infection. Crit. Rev. Clin. Lab. Sci. 2018, 55, 102–114. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Round | Marker | Status | Meaning |
|---|---|---|---|
| 2nd Biopsy | CD3 | Positive | A marker typical for T-cell, used to validate T-cell origin of the tumor |
| CD4 | Positive | Specific with peripheral T-cell lymphoma, not otherwise specified (PTL-NOS), which is also commonly associated with loss of other T-cell markers | |
| CD8 | Positive | Excluding Reed−Sternberg-like cells (usually EBV+) diagnostic and subcutaneous panniculitis-like T-cell, high positivity of CD8 shows a more aggressive type of PTCL Lymphoma, which has a higher population of CD8+ cells | |
| CD20 | A very low proportion of cells | CD20+ should be less than 1% of stained cells | |
| CD68 | Positive | Specific with PTL-NOS, however little information is known about this marker | |
| CD30 | Negative | Usually negative in PTCL-NOS | |
| 3rd biopsy | CD3 | Positive | A marker typical for T-cell, used to validate T-cell origin of the tumor |
| CD7 | Positive | Typical T-cell marker, PTCL-NOS commonly express it | |
| CD2 | High number of positive cells | Typical T-cell marker, PTCL-NOS commonly express it | |
| CD4 | High number of positive cells | High positivity of CD4 shows a less aggressive type of PTCL lymphoma | |
| CD8 | Small population of positive cells | excluding Reed−Sternberg-like cells (usually EBV+) diagnostic and subcutaneous panniculitis-like T-cell, high positivity of CD8 shows a more aggressive type of PTCL lymphoma, which has a higher population of CD8+ cells | |
| CD30 | Negative | Exclusion of anaplastic large-cell lymphoma ALK-positive and ALK-negative (ALCL), which is strongly CD30+ | |
| CD5 | Negative | Loss of CD5 is specific for PTCL-NOS | |
| CD56 | Negative | Exclusion of extranodal NK-/T-Cell lymphoma, which is CD56+ | |
| Granzyme B | Small population of positive cells | Specific for cytotoxic T-cell lymphomas, a more aggressive phenotype | |
| Ki-67 | Proliferation index of 80–85% | Verify the proliferation activity of cells |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iluta, S.; Termure, D.-A.; Petrushev, B.; Fetica, B.; Badea, M.-E.; Moldovan-Lazar, M.; Lenghel, M.; Csutak, C.; Roman, A.; Pasca, S.; et al. Clinical Remission in a 72-Year-Old Patient with a Massive Primary Cutaneous Peripheral T-Cell Lymphoma-NOS of the Eyelid, Following Combination Chemotherapy with Etoposide Plus COP. Diagnostics 2020, 10, 629. https://doi.org/10.3390/diagnostics10090629
Iluta S, Termure D-A, Petrushev B, Fetica B, Badea M-E, Moldovan-Lazar M, Lenghel M, Csutak C, Roman A, Pasca S, et al. Clinical Remission in a 72-Year-Old Patient with a Massive Primary Cutaneous Peripheral T-Cell Lymphoma-NOS of the Eyelid, Following Combination Chemotherapy with Etoposide Plus COP. Diagnostics. 2020; 10(9):629. https://doi.org/10.3390/diagnostics10090629
Chicago/Turabian StyleIluta, Sabina, Dragos-Alexandru Termure, Bobe Petrushev, Bogdan Fetica, Mindra-Eugenia Badea, Madalina Moldovan-Lazar, Manuela Lenghel, Csaba Csutak, Andrei Roman, Sergiu Pasca, and et al. 2020. "Clinical Remission in a 72-Year-Old Patient with a Massive Primary Cutaneous Peripheral T-Cell Lymphoma-NOS of the Eyelid, Following Combination Chemotherapy with Etoposide Plus COP" Diagnostics 10, no. 9: 629. https://doi.org/10.3390/diagnostics10090629