
Autofluorescence Imaging of the Skin Is an Objective Non-Invasive Technique for Diagnosing Pseudoxanthoma Elasticum

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Data
2.2. Dermoscopic and Clinical Image Acquisition
2.3. Autofluorescence and Diffuse Reflectance Imaging with Narrow-Band LED Excitation
2.4. Statistical Analysis
3. Results
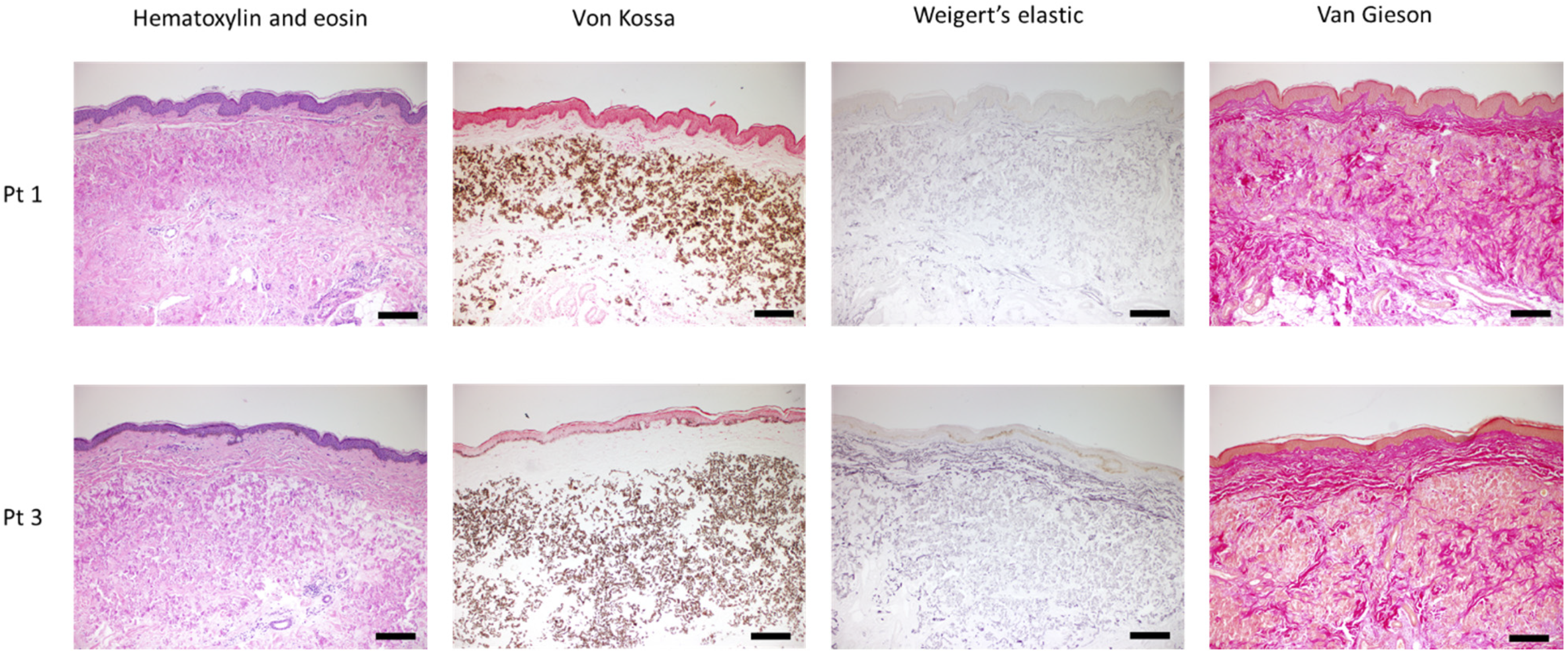
3.1. Clinical Presentation and Histopathological Features
3.2. Dermoscopy Images
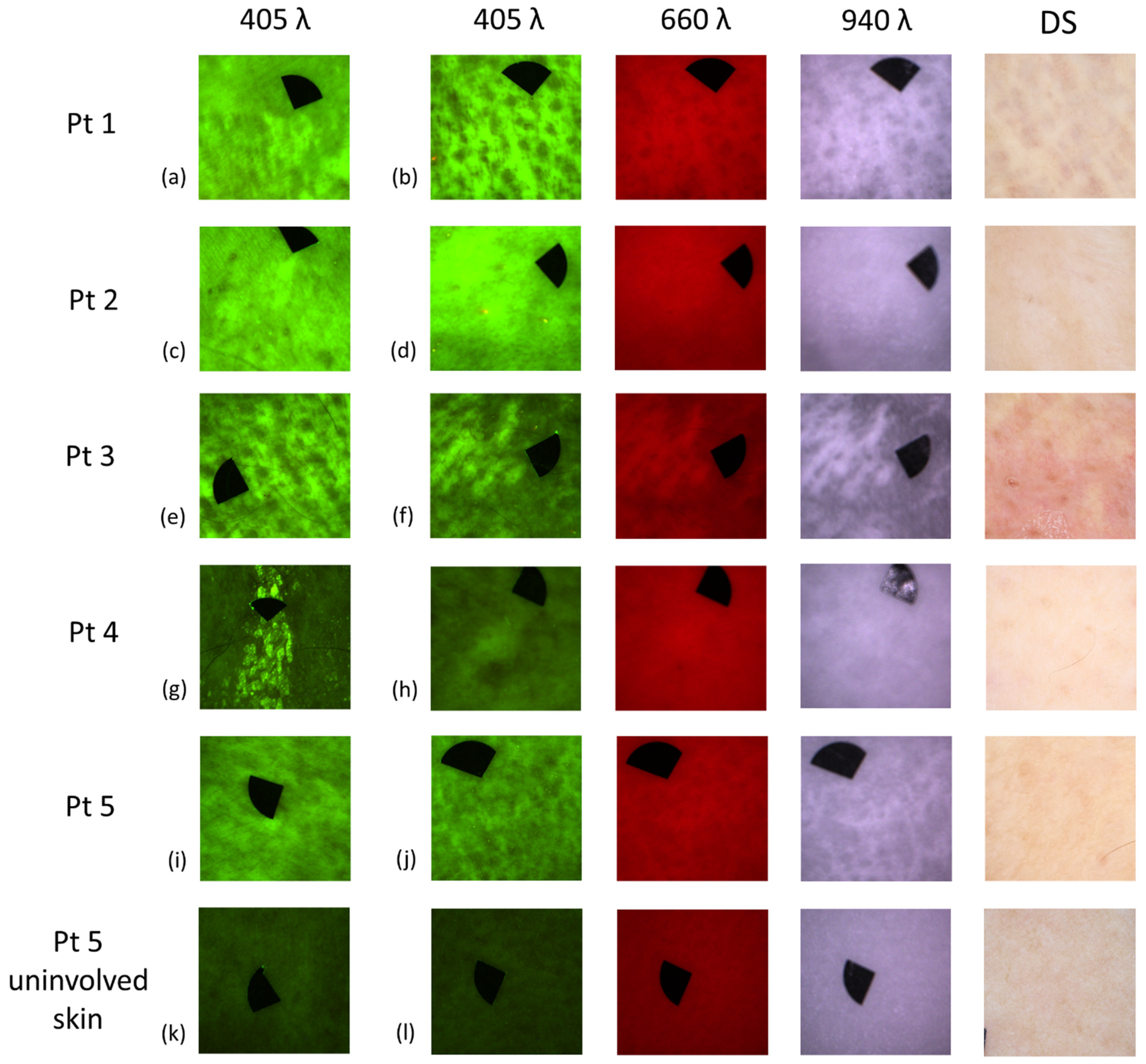
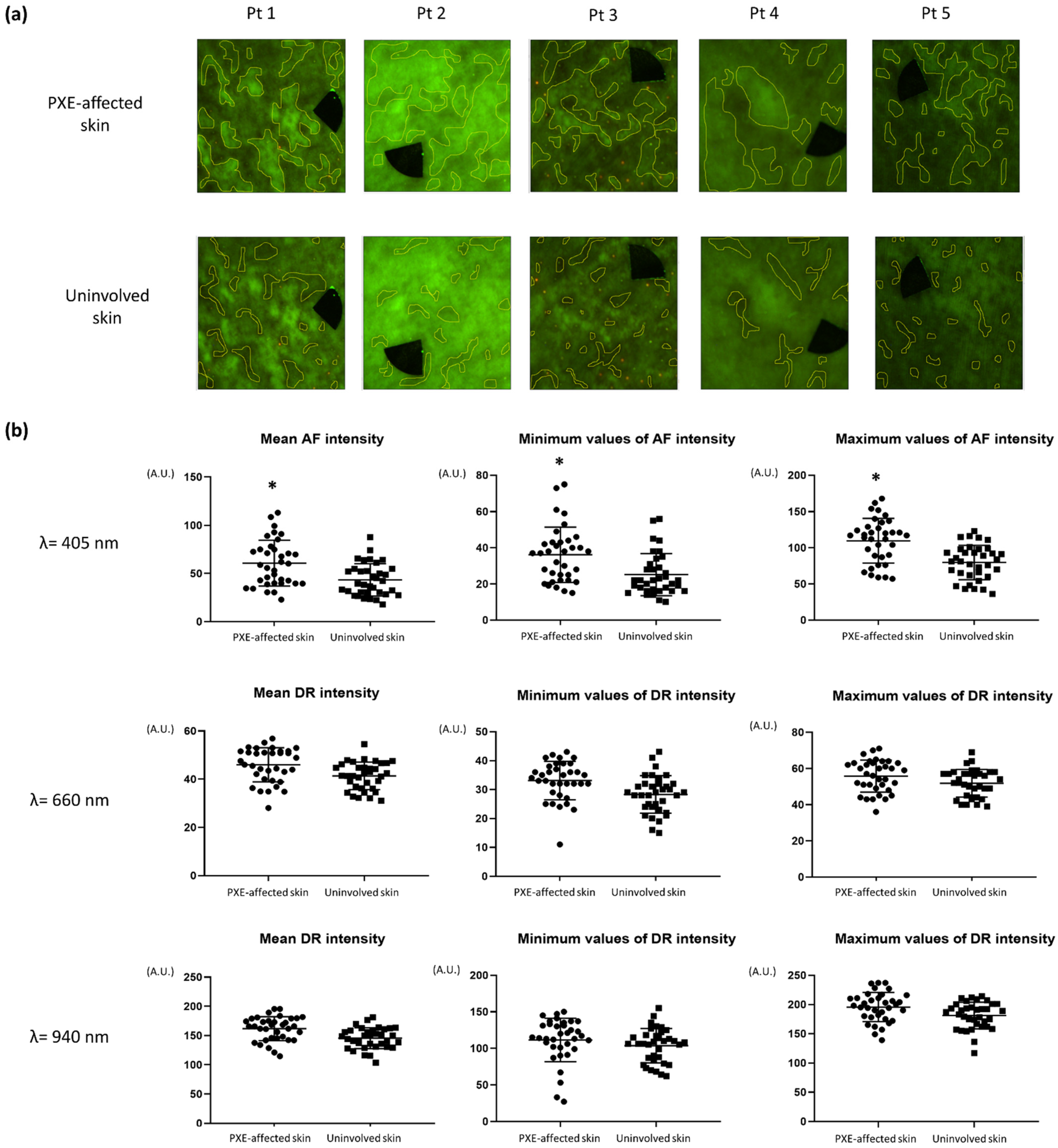
3.3. Autofluorescence and Diffuse Reflectance Imaging
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferreira, C.R. The burden of rare diseases. Am. J. Med. Genet. A 2019, 179, 885–892. [Google Scholar] [CrossRef] [PubMed]
- Köblös, G.; Andrikovics, H.; Prohászka, Z.; Tordai, A.; Váradi, A.; Arányi, T. The R1141X loss-of-function mutation of the ABCC6 gene is a strong genetic risk factor for coronary artery disease. Genet. Test. Mol. Biomark. 2010, 14, 75–78. [Google Scholar] [CrossRef] [Green Version]
- Verschuere, S.; Navassiolava, N.; Martin, L.; Nevalainen, P.I.; Coucke, P.J.; Vanakker, O.M. Reassessment of causality of ABCC6 missense variants associated with pseudoxanthoma elasticum based on Sherloc. Genet. Med. 2021, 23, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Jansen, R.S.; Duijst, S.; Mahakena, S.; Sommer, D.; Szeri, F.; Váradi, A.; Plomp, A.; Bergen, A.A.; Oude Elferink, R.P.; Borst, P.; et al. ABCC6-mediated ATP secretion by the liver is the main source of the mineralization inhibitor inorganic pyrophosphate in the systemic circulation-brief report. Arterioscler. Thromb. Vasc. Biol 2014, 34, 1985–1989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uitto, J.; Jiang, Q.; Váradi, A.; Bercovitch, L.G.; Terry, S.F. Pseudoxanthoma elasticum: Diagnostic features, classification and treatment options. Expert Opin. Orphan Drugs 2014, 2, 567–577. [Google Scholar] [CrossRef] [Green Version]
- de Vilder, E.Y.; Vanakker, O.M. From variome to phenome: Pathogenesis, diagnosis and management of ectopic mineralization disorders. World J. Clin. Cases 2015, 3, 556–574. [Google Scholar] [CrossRef]
- Hosen, M.J.; Lamoen, A.; de Paepe, A.; Vanakker, O.M. Histopathology of Pseudoxanthoma Elasticum and Related Disorders: Histological Hallmarks and Diagnostic Clues. Scientifica 2012, 2012, 598262. [Google Scholar] [CrossRef] [Green Version]
- Panagou, E.; Ratynska, M.; Heelan, K. Pseudoxanthoma elasticum-like papillary dermal elastolysis: A case report and review of literature. Int. J. Dermatol. 2019, 58, 93–97. [Google Scholar] [CrossRef]
- Aydin, E.; Demir, H.D.; Batioglu, F.; Sezer, E. Atypical Fundus Lesions in Juvenile Pseudoxanthoma Elasticum. Ophthalmic Res. 2007, 39, 344–347. [Google Scholar] [CrossRef] [PubMed]
- Bertamino, M.; Severino, M.; Grossi, A.; Rusmini, M.; Tortora, D.; Gandolfo, C.; Pederzoli, S.; Malattia, C.; Picco, P.; Striano, P.; et al. ABCC6 mutations and early onset stroke: Two cases of a typical Pseudoxanthoma Elasticum. Eur. J. Paediatr. Neurol. 2018, 22, 725–728. [Google Scholar] [CrossRef] [PubMed]
- Dibi, A.; El Fahime, E.L.; Mouane, N.; Dafiri, R.; Bentahila, A. Pseudoxanthoma elasticum: A rare cause of gastrointestinal bleeding in children. Arch. Pediatr. 2016, 23, 591–594. [Google Scholar] [CrossRef]
- Gliem, M.; Birtel, J.; Müller, P.L.; Hendig, D.; Faust, I.; Herrmann, P.; Holz, F.G.; Adamus, G.; Issa, P.C. Acute Retinopathy in Pseudoxanthoma Elasticum. JAMA Ophthalmol. 2019, 137, 1165–1173. [Google Scholar] [CrossRef] [PubMed]
- Risseeuw, S.; van Norel, J.O.; Klaver, C.C.W.; Colijn, J.M.; Imhof, S.M.; van Leeuwen, R. Visual acuity in pseudoxanthoma elasticum. Retina 2019, 39, 1580–1587. [Google Scholar] [CrossRef]
- Lefthériotis, G.; Omarjee, L.; Saux, O.L.; Henrion, D.; Abraham, P.; Prunier, F.; Willoteaux, S.; Martin, L. The vascular phenotype in Pseudoxanthoma elasticum and related disorders: Contribution of a genetic disease to the understanding of vascular calcification. Front. Genet. 2013, 4, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berthin, C.; Phan, A.; Navasiolava, N.; Michalak, S.; Humeau, H.; Grimaux, X.; Martin, L. Dermoscopic phenotype of pseudoxanthoma elasticum skin lesions: A study of 16 patients. J. Eur. Acad. Dermatol. Venereol. 2019, 33, e262–e265. [Google Scholar] [CrossRef] [PubMed]
- Lacarrubba, F.; Verzì, A.E.; Caltabiano, R.; Micali, G. Dermoscopy of pseudoxanthoma elasticum. J. Am. Acad. Dermatol. 2017, 76, S69–S70. [Google Scholar] [CrossRef]
- Kawashima, S.; Togawa, Y.; Miyachi, H.; Matsue, H. Dermoscopic features of pseudoxanthoma elasticum. Clin. Exp. Dermatol. 2018, 43, 175–179. [Google Scholar] [CrossRef]
- Mandel, V.; Boraldi, F.; Pellacani, G.; Ciardo, S.; Mazzaglia, G.; Farnetani, F. Pseudoxanthoma elasticum and reflectance confocal microscopy: Report of two affected young sisters. J. Pediatr. Neonatal Individ. Med. 2015, 4, e040125. [Google Scholar] [CrossRef]
- Guérin-Moreau, M.; Leftheriotis, G.; Corre, Y.L.; Etienne, M.; Amode, R.; Hamel, J.F.; Croué, A.; Saux, O.L.; Machet, L.; Martin, L. High-frequency (20-50 MHz) ultrasonography of pseudoxanthoma elasticum skin lesions. Br. J. Dermatol. 2013, 169, 1233–1239. [Google Scholar] [CrossRef] [Green Version]
- Murata, T.; Honda, T.; Miyachi, Y.; Kabashima, K. Morphological character of pseudoxanthoma elasticum observed by multiphoton microscopy. J. Dermatol. Sci. 2013, 72, 199–201. [Google Scholar] [CrossRef]
- Kiss, N.; Fésűs, L.; Bozsányi, S.; Szeri, F.; van Gils, M.; Szabó, V.; Nagy, A.I.; Hidvégi, B.; Szipőcs, R.; Martin, L.; et al. Nonlinear optical microscopy is a novel tool for the analysis of cutaneous alterations in pseudoxanthoma elasticum. Lasers Med. Sci. 2020, 35, 1821–1830. [Google Scholar] [CrossRef]
- Kiss, N.; Haluszka, D.; Lorincz, K.; Kuroli, E.; Harsing, J.; Mayer, B.; Karpati, S.; Fekete, G.; Szipocs, R.; Wikonkal, N.; et al. Ex vivo nonlinear microscopy imaging of Ehlers-Danlos syndrome-affected skin. Arch. Dermatol. Res. 2018, 310, 463–473. [Google Scholar] [CrossRef]
- Cui, J.Z.; Tehrani, A.Y.; Jett, K.A.; Bernatchez, P.; van Breemen, C.; Esfandiarei, M. Quantification of aortic and cutaneous elastin and collagen morphology in Marfan syndrome by multiphoton microscopy. J. Struct. Biol. 2014, 187, 242–253. [Google Scholar] [CrossRef] [PubMed]
- Omarjee, L.; Mention, P.J.; Janin, A.; Kauffenstein, G.; Pabic, E.L.; Meilhac, O.; Blanchard, S.; Navasiolava, N.; Leftheriotis, G.; Couturier, O.; et al. Assessment of Inflammation and Calcification in Pseudoxanthoma Elasticum Arteries and Skin with 18F-FluroDeoxyGlucose and 18F-Sodium Fluoride Positron Emission Tomography/Computed Tomography Imaging: The GOCAPXE Trial. J. Clin. Med. 2020, 9, 3448. [Google Scholar] [CrossRef]
- Lesins, J.; Lihachev, A.; Rudys, R.; Bagdonas, S.; Spigulis, J. Skin Autofluorescence Photo-Bleaching and Photo-Memory. In Proceedings of the Medical Laser Applications and Laser-Tissue Interactions V, Munich, Germany, 22–26 May 2011; p. 80920N. [Google Scholar]
- Lihachev, A.; Lihacova, I.; Plorina, E.V.; Lange, M.; Derjabo, A.; Spigulis, J. Differentiation of seborrheic keratosis from basal cell carcinoma, nevi and melanoma by RGB autofluorescence imaging. Biomed. Opt. Express 2018, 9, 1852–1858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lange, M.; Kiss, N.; Fesus, L.; Plorina, E.; Derjabo, A.; Spigulis, J. Non-Invasive LED-Based Screening Solution for Skin Cancer. In Clinical and Preclinical Optical Diagnostics; OSA Publishing: Washington, DC, USA, 2019; p. 17. [Google Scholar] [CrossRef]
- Lihacova, I.; Cibulska, E.; Lihachev, A.; Lange, M.; Plorina, E.V.; Bliznuks, D.; Derjabo, A.; Kiss, N. Challenges of Automatic Processing of Large amount of Skin Lesion Multispectral Data. Proc. SPIE 2020, 11585, 115850C. [Google Scholar] [CrossRef]
- Marta, L.; Szabolcs, B.; Emilija, V.P.; Lihachev, A.; Derjabo, A. Spectral Imaging as A Tool for the Evaluation of Skin Cancer Post-Operative Scars. Proc. SPIE 2020, 11585, 1158506. [Google Scholar] [CrossRef]
- Rust, J.A.; Nóbrega, J.A.; Calloway, C.P.; Jones, B.T. Fraunhofer Effect Atomic Absorption Spectrometry. Anal. Chem. 2005, 77, 1060–1067. [Google Scholar] [CrossRef]
- Siddiqui, A.A.; Paulus, Y.M.; Scott, A.W. Use of Fundus Autofluorescence to Evaluate Retinal Artery Occlusions. Retina 2014, 34, 2490–2491. [Google Scholar] [CrossRef]
- Rajesh, B.; Hussain, R.; Giridhar, A. Autofluorescence and Infrared Fundus Imaging for Detection of Retinal Emboli and Unmasking Undiagnosed Systemic Abnormalities. J. Ophthalmic Vis. Res. 2016, 11, 449–451. [Google Scholar] [CrossRef] [Green Version]
- Plomp, A.S.; Toonstra, J.; Bergen, A.A.; van Dijk, M.R.; de Jong, P.T. Proposal for updating the pseudoxanthoma elasticum classification system and a review of the clinical findings. Am. J. Med. Genet. A 2010, 152a, 1049–1058. [Google Scholar] [CrossRef]
- Legrand, A.; Cornez, L.; Samkari, W.; Mazzella, J.M.; Venisse, A.; Boccio, V.; Auribault, K.; Keren, B.; Benistan, K.; Germain, D.P.; et al. Mutation spectrum in the ABCC6 gene and genotype-phenotype correlations in a French cohort with pseudoxanthoma elasticum. Genet. Med. 2017, 19, 909–917. [Google Scholar] [CrossRef] [PubMed]
- Tamošiūnas, M.; Plorina, E.V.; Lange, M.; Derjabo, A.; Kuzmina, I.; Bļizņuks, D.; Spigulis, J. Autofluorescence imaging for recurrence detection in skin cancer postoperative scars. J. Biophotonics 2020, 13, e201900162. [Google Scholar] [CrossRef]
- Lihachev, A.; Derjabo, A.; Ferulova, I.; Lange, M.; Lihacova, I.; Spigulis, J. Autofluorescence imaging of basal cell carcinoma by smartphone RGB camera. J. Biomed. Opt. 2015, 20, 120502. [Google Scholar] [CrossRef]
- Bliznuks, D.; Jakovels, D.; Saknite, I.; Spigulis, J. Mobile Platform for Online Processing of Multimodal Skin Optical Images: Using Online Matlab Server for Processing Remission, Fluorescence and Laser Speckle Images, Obtained by Using Novel Handheld Device. In Proceedings of the 2015 International Conference on BioPhotonics (BioPhotonics), Florence, Italy, 20–22 May 2015; pp. 1–4. [Google Scholar]
- Michael, N.; Boisseau, C.; Bonicel, P.; Daudon, P.; Bonneau, D.; Chassaing, N.; Martin, L. Manifestations of pseudoxanthoma elasticum in childhood. Br. J. Dermatol. 2009, 161, 635–639. [Google Scholar] [CrossRef]
- Jensen, O.A. Bruch’s membrane in pseudoxanthoma elasticum. Histochemical, ultrastructural, and x-ray microanalytical study of the membrane and angioid streak areas. Graefe Arch. Clin. Exp. Ophthalmol. 1977, 203, 311–320. [Google Scholar] [CrossRef] [PubMed]
- Walker, E.R.; Frederickson, R.G.; Mayes, M.D. The mineralization of elastic fibers and alterations of extracellular matrix in pseudoxanthoma elasticum. Ultrastructure, immunocytochemistry, and X-ray analysis. Arch. Dermatol. 1989, 125, 70–76. [Google Scholar] [CrossRef]
- Machado, T.R.; Leite, I.S.; Inada, N.M.; Li, M.S.; da Silva, J.S.; Andrés, J.; Beltrán-Mir, H.; Cordoncillo, E.; Longo, E. Designing biocompatible and multicolor fluorescent hydroxyapatite nanoparticles for cell-imaging applications. Mater. Today Chem. 2019, 14, 100211. [Google Scholar] [CrossRef]
- Uchida, Y.; Uchida, Y.; Kawai, S.; Kanamaru, R.; Sugiyama, Y.; Tomaru, T.; Maezawa, Y.; Kameda, N. Detection of vulnerable coronary plaques by color fluorescent angioscopy. JACC Cardiovasc. Imaging 2010, 3, 398–408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, Q.; Zhegalova, N.; Wang, S.; Akers, W.; Berezin, M. Multispectral imaging in the extended near-infrared window based on endogenous chromophores. J. Biomed. Opt. 2013, 18, 101318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spigulis, J.; Rubins, U.; Kviesis-Kipge, E.; Rubenis, O. SkImager: A concept device for in-vivo skin assessment by multimodal imaging. Proc. Est. Acad. Sci. 2014, 63, 213. [Google Scholar] [CrossRef]
- Giovannacci, I.; Magnoni, C.; Vescovi, P.; Painelli, A.; Tarentini, E.; Meleti, M. Which are the main fluorophores in skin and oral mucosa? A review with emphasis on clinical applications of tissue autofluorescence. Arch. Oral Biol 2019, 105, 89–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navasiolava, N.; Gnanou, M.; Douillard, M.; Saulnier, P.; Aranyi, T.; Ebran, J.M.; Henni, S.; Humeau, H.; Lefthériotis, G.; Martin, L. The extent of pseudoxanthoma elasticum skin changes is related to cardiovascular complications and visual loss: A cross-sectional study. Br. J. Dermatol. 2019, 180, 207–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Utani, A.; Tanioka, M.; Yamamoto, Y.; Taki, R.; Araki, E.; Tamura, H.; Miyachi, Y. Relationship between the distribution of pseudoxanthoma elasticum skin and mucous membrane lesions and cardiovascular involvement. J. Dermatol. 2010, 37, 130–136. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pt. No. | Sex | Age (y) | Phenodex Score |
|---|---|---|---|
| 1 | F | 53 | S3 E3 G0 V1 C0 R0 |
| 2 | F | 53 | S2 E3 G0 V1 C1 R0 |
| 3 | M | 69 | S3 E3 G0 V0 C0 R0 |
| 4 | M | 52 | S2 E3 G0 V0 C1 R0 |
| 5 | F | 48 | S2 E2 G0 V0 C0 R0 |
| Pt 1 | Pt 2 | Pt 3 | Pt 4 | Pt 5 | |
|---|---|---|---|---|---|
| neck | + | + | + | + | + |
| axilla | + | (+) | + | + | (+) |
| antecubital fossa | + | (+) | + | (+) | + |
| popliteal fossa | + | (+) | + | (+) | (+) |
| inguinal | + | + | + | (+) | |
| periumbilical | + | + | |||
| wrist | + | (+) | |||
| chest | (+) |
| Structure | Pt 1 | Pt 2 | Pt 3 | Pt 4 | Pt 5 | |
|---|---|---|---|---|---|---|
| neck | globules | plaques | dots, linear | mesh network | linear | dots, plaques |
| background | red | brownish | purple-red | red | brownish | |
| vessels | reticulated, linear | reticulated | reticulated | reticulated | no | |
| axilla | globules | plaques | dots | mesh network | dots | dots |
| background | purple | brownish | purple-red | pink | brownish | |
| vessels | linear | no | reticulated | no | no | |
| antecubital fossa | globules | linear | (non-typical) | linear | linear | plaque |
| background | purple-red | purple | brownish | purple | ||
| vessels | reticulated | reticulated | no | no | ||
| popliteal fossa | globules | linear | linear | linear | dots | linear |
| background | purple-red | brownish | purple | pink | purple | |
| vessels | several reticulated | no | reticulated | reticulated | reticulated | |
| inguinal | globules | dots | (non-typical) | (non-typical) | (non-typical) | |
| background | purple | |||||
| vessels | reticulated | |||||
| periumbilical | globules | dots | (absent) | |||
| background | purple-red | |||||
| vessels | reticulated | |||||
| wrist | globules | plaques | (absent) | |||
| background | purple | |||||
| vessels | reticulated | |||||
| chest | globules | (absent) | ||||
| background | ||||||
| vessels |
| Pt 1 | Pt 2 | Pt 3 | Pt 4 | Pt 5 | |
|---|---|---|---|---|---|
| Site 1 | popliteal fossa | popliteal fossa | popliteal fossa | popliteal fossa | periumbilical |
| Site 2 | Inguinal | inguinal | inguinal | axilla | inguinal |
| Site 3 | periumbilical | axilla | inguinal | axilla | axilla |
| Site 4 | axilla | axilla | axilla | axilla | antecubital fossa |
| Site 5 | wrist | antecubital fossa | antecubital fossa | wrist | antecubital fossa |
| Site 6 | antecubital fossa | neck | neck | antecubital fossa | neck |
| Site 7 | neck | neck | neck | neck | neck |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farkas, K.; Bozsányi, S.; Plázár, D.; Bánvölgyi, A.; Fésűs, L.; Anker, P.; Zakariás, S.; Lihacova, I.; Lihachev, A.; Lange, M.; et al. Autofluorescence Imaging of the Skin Is an Objective Non-Invasive Technique for Diagnosing Pseudoxanthoma Elasticum. Diagnostics 2021, 11, 260. https://doi.org/10.3390/diagnostics11020260
Farkas K, Bozsányi S, Plázár D, Bánvölgyi A, Fésűs L, Anker P, Zakariás S, Lihacova I, Lihachev A, Lange M, et al. Autofluorescence Imaging of the Skin Is an Objective Non-Invasive Technique for Diagnosing Pseudoxanthoma Elasticum. Diagnostics. 2021; 11(2):260. https://doi.org/10.3390/diagnostics11020260
Chicago/Turabian StyleFarkas, Klára, Szabolcs Bozsányi, Dóra Plázár, András Bánvölgyi, Luca Fésűs, Pálma Anker, Sára Zakariás, Ilze Lihacova, Alexey Lihachev, Marta Lange, and et al. 2021. "Autofluorescence Imaging of the Skin Is an Objective Non-Invasive Technique for Diagnosing Pseudoxanthoma Elasticum" Diagnostics 11, no. 2: 260. https://doi.org/10.3390/diagnostics11020260