Oxidative Stress Markers in Inflammatory Bowel Diseases: Systematic Review

 , and
, and
Abstract
:1. Introduction
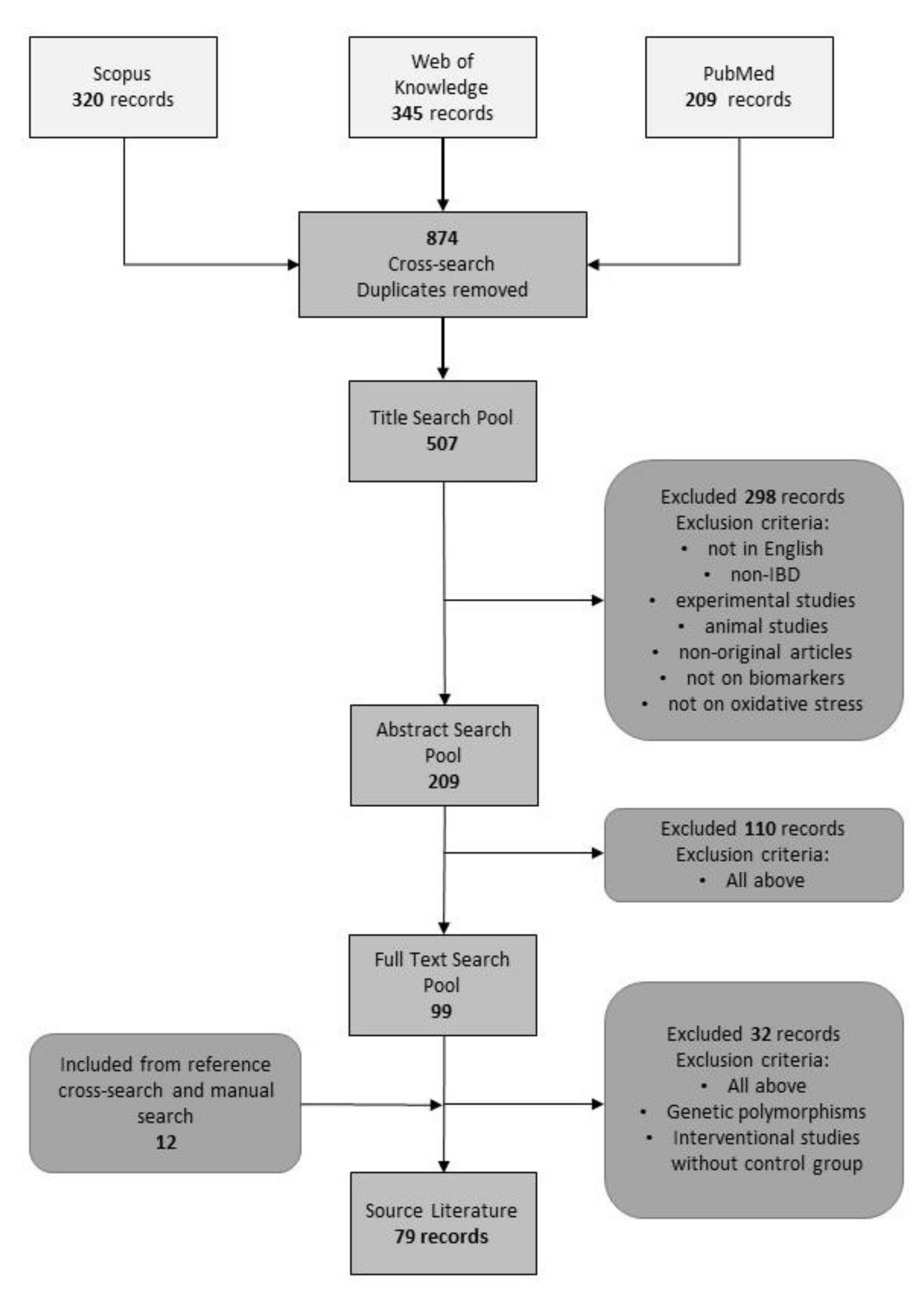
2. Materials and Methods
3. Results
3.1. Interpretative Synthesis of Data: Diagnostic Markers
3.1.1. Diagnostic Markers in IBD (Markers Not Specific for Either UC or CD)
3.1.2. Diagnostic Markers in UC
3.1.3. Diagnostic Markers in CD
3.2. Interpretative Synthesis of Data: Differential Markers
3.2.1. Crohn’s Disease and Ulcerative Colitis
3.2.2. IBD and Other Gastrointestinal Disorders
3.3. Interpretative Synthesis of Data: Markers of Disease Progression (Activity, Severity, Mucosal Healing, and Colorectal Cancer)
3.3.1. Progression Markers in IBD (Markers Not Specific for Either UC or CD)
3.3.2. Progression Markers in UC
3.3.3. Progression Markers in CD
3.3.4. Markers of Mucosal Healing
3.3.5. Markers of Colorectal Cancer
3.4. Interpretative Synthesis of Data: Prognostic Markers
3.5. Interpretative Synthesis of Data: Adult vs. Pediatric IBD
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Kim, D.H.; Cheon, J.H. Pathogenesis of Inflammatory Bowel Disease and Recent Advances in Biologic Therapies. Immune Netw. 2017, 17, 25–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cantoro, L.; Di Sabatino, A.; Papi, C.; Margagnoni, G.; Ardizzone, S.; Giuffrida, P.; Giannarelli, D.; Massari, A.; Monterubbianesi, R.; Lenti, M.V.; et al. The Time Course of Diagnostic Delay in Inflammatory Bowel Disease Over the Last Sixty Years: An Italian Multicentre Study. J. Crohn’s Colitis 2017, 11, 975–980. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coward, S.; Clement, F.; Benchimol, E.I.; Bernstein, C.N.; Avina-Zubieta, J.A.; Bitton, A.; Carroll, M.W.; Hazlewood, G.; Jacobson, K.; Jelinski, S.; et al. Past and Future Burden of Inflammatory Bowel Diseases Based on Modeling of Population-Based Data. Gastroenterology 2019, 156, 1345–1353.e4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaplan, G.G. The Global Burden of IBD: From 2015 to 2025. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 720–727. [Google Scholar] [CrossRef]
- Ng, S.C.; Shi, H.Y.; Hamidi, N.; Underwood, F.E.; Tang, W.; Benchimol, E.I.; Panaccione, R.; Ghosh, S.; Wu, J.C.Y.; Chan, F.K.L.; et al. Worldwide Incidence and Prevalence of Inflammatory Bowel Disease in the 21st Century: A Systematic Review of Population-Based Studies. Lancet 2018, 390, 2769–2778. [Google Scholar] [CrossRef]
- Molodecky, N.A.; Soon, I.S.; Rabi, D.M.; Ghali, W.A.; Ferris, M.; Chernoff, G.; Benchimol, E.I.; Panaccione, R.; Ghosh, S.; Barkema, H.W.; et al. Increasing Incidence and Prevalence of the Inflammatory Bowel Diseases With Time, Based on Systematic Review. Gastroenterology 2012, 142, 46–54.e42. [Google Scholar] [CrossRef] [Green Version]
- Everhov, Å.H.; Halfvarson, J.; Myrelid, P.; Sachs, M.C.; Nordenvall, C.; Söderling, J.; Ekbom, A.; Neovius, M.; Ludvigsson, J.F.; Askling, J.; et al. Incidence and Treatment of Patients Diagnosed With Inflammatory Bowel Diseases at 60 Years or Older in Sweden. Gastroenterology 2018, 154, 518–528.e15. [Google Scholar] [CrossRef]
- Arnott, I.; Rogler, G.; Halfvarson, J. The Management of Inflammatory Bowel Disease in Elderly: Current Evidence and Future Perspectives. Inflamm. Intest. Dis. 2018, 2, 189–199. [Google Scholar] [CrossRef]
- Savage, W.; Everett, A. Biomarkers in Pediatrics: Children as Biomarker Orphans. Proteomics. Clin. Appl. 2010, 4, 915–921. [Google Scholar] [CrossRef]
- Tian, T.; Wang, Z.; Zhang, J. Pathomechanisms of Oxidative Stress in Inflammatory Bowel Disease and Potential Antioxidant Therapies. Oxid. Med. Cell. Longev. 2017, 2017, 4535194. [Google Scholar] [CrossRef]
- Ighodaro, O.M.; Akinloye, O.A. First Line Defence Antioxidants-Superoxide Dismutase (SOD), Catalase (CAT) and Glutathione Peroxidase (GPX): Their Fundamental Role in the Entire Antioxidant Defence Grid. Alexandria J. Med. 2018, 54, 287–293. [Google Scholar] [CrossRef] [Green Version]
- Nimse, S.B.; Pal, D. Free Radicals, Natural Antioxidants, and Their Reaction Mechanisms. RSC Adv. 2015, 5, 27986–28006. [Google Scholar] [CrossRef] [Green Version]
- Mirończuk-Chodakowska, I.; Witkowska, A.M.; Zujko, M.E. Endogenous Non-Enzymatic Antioxidants in the Human Body. Adv. Med. Sci. 2018, 63, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Gomollón, F.; Dignass, A.; Annese, V.; Tilg, H.; Van Assche, G.; Lindsay, J.O.; Peyrin-Biroulet, L.; Cullen, G.J.; Daperno, M.; Kucharzik, T.; et al. 3rd European Evidence-Based Consensus on the Diagnosis and Management of Crohn’s Disease 2016: Part 1: Diagnosis and Medical Management. J. Crohns. Colitis 2017, 11, 3–25. [Google Scholar] [CrossRef] [Green Version]
- Ayling, R.M.; Kok, K. Chapter Six - Fecal Calprotectin. In Advances in Clinical Chemistry; Makowski, G.S., Ed.; Elsevier: Amsterdam, The Netherlands, 2018; Volume 87. [Google Scholar] [CrossRef]
- Jahanshahi, G.; Motavasel, V.; Rezaie, A.; Hashtroudi, A.; Daryani, N.; Abdollahi, M. Alterations in Antioxidant Power and Levels of Epidermal Growth Factor and Nitric Oxide in Saliva of Patients with Inflammatory Bowel Diseases. Dig. Dis. Sci. 2004, 49, 1752–1757. [Google Scholar] [CrossRef] [PubMed]
- Rezaie, A.; Ghorbani, F.; Eshghtork, A.; Zamani, M.J.; Dehghan, G.; Taghavi, B.; Nikfar, S.; Mohammadirad, A.; Daryani, N.E.; Abdollahi, M. Alterations in Salivary Antioxidants, Nitric Oxide, and Transforming Growth Factor-Β1 in Relation to Disease Activity in Crohn’s Disease Patients. Ann. N. Y. Acad. Sci. 2006, 1091, 110–122. [Google Scholar] [CrossRef]
- Rezeie, A.L.I.; Khalaj, S.; Shabihkhani, M.; Nikfar, S.; Zamani, M.J.; Mohammadirad, A.; Daryani, N.E.; Abdollahi, M. Study on the Correlations among Disease Activity Index and Salivary Transforming Growth Factor-Β1 and Nitric Oxide in Ulcerative Colitis Patients. Ann. N. Y. Acad. Sci. 2007, 1095, 305–314. [Google Scholar] [CrossRef]
- Keshavarzian, A.; Banan, A.; Farhadi, A.; Komanduri, S.; Mutlu, E.; Zhang, Y.; Fields, J.Z. Increases in Free Radicals and Cytoskeletal Protein Oxidation and Nitration in the Colon of Patients with Inflammatory Bowel Disease. Gut 2003, 52, 720–728. [Google Scholar] [CrossRef] [Green Version]
- Yuksel, M.; Ates, I.; Kaplan, M.; Arikan, M.F.; Ozin, Y.O.; Kilic, Z.M.Y.; Topcuoglu, C.; Kayacetin, E. Is Oxidative Stress Associated with Activation and Pathogenesis of Inflammatory Bowel Disease? J. Med. Biochem. 2017, 36, 341–348. [Google Scholar] [CrossRef]
- Boehm, D.; Krzystek-Korpacka, M.; Neubauer, K.; Matusiewicz, M.; Paradowski, L.; Gamian, A. Lipid Peroxidation Markers in Crohn’s Disease: The Associations and Diagnostic Value. Clin. Chem. Lab. Med. 2012, 50. [Google Scholar] [CrossRef]
- Grzybowska-Chlebowczyk, U.; Wysocka-Wojakiewicz, P.; Jasielska, M.; Cukrowska, B.; Więcek, S.; Kniażewska, M.; Chudek, J. Oxidative and Antioxidative Stress Status in Children with Inflammatory Bowel Disease as a Result of a Chronic Inflammatory Process. Mediators Inflamm. 2018, 2018, 4120973. [Google Scholar] [CrossRef] [PubMed]
- Aslan, M.; Nazligul, Y.; Bolukbas, C.; Bolukbas, F.F.; Horoz, M.; Dulger, A.C.; Erdur, F.M.; Celik, H.; Kocyigit, A. Peripheral Lymphocyte DNA Damage and Oxidative Stress in Patients with Ulcerative Colitis. Pol. Arch. Med. Wewn. 2011, 121, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Hengstermann, S.; Valentini, L.; Schaper, L.; Buning, C.; Koernicke, T.; Maritschnegg, M.; Buhner, S.; Tillinger, W.; Regano, N.; Guglielmi, F.; et al. Altered Status of Antioxidant Vitamins and Fatty Acids in Patients with Inactive Inflammatory Bowel Disease. Clin. Nutr. 2008, 27. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, E.; Qujeq, D.; Taheri, H.; Hajian-Tilaki, K. Evaluation of Serum Trace Element Levels and Superoxide Dismutase Activity in Patients with Inflammatory Bowel Disease: Translating Basic Research into Clinical Application. Biol. Trace Elem. Res. 2017, 177, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Dudzińska, E.; Gryzinska, M.; Ognik, K.; Gil-Kulik, P.; Kocki, J. Oxidative Stress and Effect of Treatment on the Oxidation Product Decomposition Processes in IBD. Oxid. Med. Cell. Longev. 2018, 2018, 7918261. [Google Scholar] [CrossRef]
- Baskol, M.; Başkol, G.; Kocer, D.; Ozbakir, O.; Yucesoy, M. Advanced Oxidation Protein Products: A Novel Marker of Oxidative Stress in Ulcerative Colitis. J. Clin. Gastroenterol. 2008, 42, 687–691. [Google Scholar] [CrossRef]
- Hong, S.-K.S.; Chaturvedi, R.; Piazuelo, M.B.; Coburn, L.A.; Williams, C.S.; Delgado, A.G.; Casero Jr, R.A.; Schwartz, D.A.; Wilson, K.T. Increased Expression and Cellular Localization of Spermine Oxidase in Ulcerative Colitis and Relationship to Disease Activity. Inflamm. Bowel Dis. 2010, 16, 1557–1566. [Google Scholar] [CrossRef] [Green Version]
- Christophi, G.P.; Rong, R.; Holtzapple, P.G.; Massa, P.T.; Landas, S.K. Immune Markers and Differential Signaling Networks in Ulcerative Colitis and Crohn’s Disease. Inflamm. Bowel Dis. 2012, 18, 2342–2356. [Google Scholar] [CrossRef] [Green Version]
- Kumagae, Y.; Hirahashi, M.; Takizawa, K.; Yamamoto, H.; Gushima, M.; Esaki, M.; Matsumoto, T.; Nakamura, M.; Kitazono, T.; Oda, Y. Overexpression of MTH1 and OGG1 Proteins in Ulcerative Colitis-Associated Carcinogenesis. Oncol. Lett. 2018, 16, 1765–1776. [Google Scholar] [CrossRef] [Green Version]
- Krzystek-Korpacka, M.; Neubauer, K.; Berdowska, I.; Zielinski, B.; Paradowski, L.; Gamian, A. Impaired Erythrocyte Antioxidant Defense in Active Inflammatory Bowel Disease: Impact of Anemia and Treatment. Inflamm. Bowel Dis. 2009, 16, 1467–1475. [Google Scholar] [CrossRef]
- Rana, S.V.; Sharma, S.; Prasad, K.K.; Sinha, S.K.; Singh, K. Role of Oxidative Stress & Antioxidant Defence in Ulcerative Colitis Patients from North India. Indian J. Med. Res. 2014, 139, 568–571. [Google Scholar] [PubMed]
- Koláček, M.; Muchová, J.; Dvořáková, M.; Paduchová, Z.; Žitňanová, I.; Čierna, I.; Országhová, Z.; Székyová, D.; Jajcaiová-Zedníčková, N.; Kovács, L.; et al. Effect of Natural Polyphenols (Pycnogenol) on Oxidative Stress Markers in Children Suffering from Crohn’s Disease--a Pilot Study. Free Radic. Res. 2013, 47, 624–634. [Google Scholar] [CrossRef]
- Akman, T.; Akarsu, M.; Akpinar, H.; Resmi, H.; Taylan, E. Erythrocyte Deformability and Oxidative Stress in Inflammatory Bowel Disease. Dig. Dis. Sci. 2012, 57, 458–464. [Google Scholar] [CrossRef]
- Pacal, L.; Varvařovská, J.; Sýkora, J.; Koželuhová, J.; Rušavý, Z.; Racek, J.; Stetina, R.; Kanková, K. Crohn’s Disease Activity versus Extent of DNA Damage/Repair and Variability in the Rage Gene. Scr. Medica Fac. Medicae Univ. Brun. Masaryk. 2010, 83, 72–80. [Google Scholar]
- Beltrán, B.; Nos, P.; Dasí, F.; Iborra, M.; Bastida, G.; Martínez, M.; O’Connor, J.-E.; Sáez, G.; Moret, I.; Ponce, J. Mitochondrial Dysfunction, Persistent Oxidative Damage, and Catalase Inhibition in Immune Cells of Naïve and Treated Crohn’s Disease. Inflamm. Bowel Dis. 2010, 16, 76–86. [Google Scholar] [CrossRef] [PubMed]
- Szczeklik, K.; Krzyściak, W.; Cibor, D.; Domagała-Rodacka, R.; Pytko-Polończyk, J.; Mach, T.; Owczarek, D. Markers of Lipid Peroxidation and Antioxidant Status in the Serum and Saliva of Patients with Active Crohn Disease. Polish Arch. Intern. Med. 2018, 128, 362–370. [Google Scholar] [CrossRef]
- Achitei, D.; Ciobica, A.; Balan, G.; Gologan, E.; Stanciu, C.; Stefanescu, G. Different Profile of Peripheral Antioxidant Enzymes and Lipid Peroxidation in Active and Non-Active Inflammatory Bowel Disease Patients. Dig. Dis. Sci. 2013, 58, 1244–1249. [Google Scholar] [CrossRef] [PubMed]
- Tüzün, A.; Erdil, A.; İnal, V.; Aydın, A.; Bağcı, S.; Yeşilova, Z.; Sayal, A.; Karaeren, N.; Dağalp, K. Oxidative Stress and Antioxidant Capacity in Patients with Inflammatory Bowel Disease. Clin. Biochem. 2002, 35, 569–572. [Google Scholar] [CrossRef]
- Vaghari-Tabari, M.; Moein, S. Positive Correlation of Fecal Calprotectin with Serum Antioxidant Enzymes in Patients with Inflammatory Bowel Disease: Is It an Accidental Numerical Correlation or a New Finding? Am. J. Med. Sci. 2018, 355. [Google Scholar] [CrossRef]
- Maor, I.; Rainis, T.; Lanir, A.; Lavy, A. Oxidative Stress, Inflammation and Neutrophil Superoxide Release in Patients with Crohn’s Disease: Distinction between Active and Non-Active Disease. Dig. Dis. Sci. 2008, 53, 2208–2214. [Google Scholar] [CrossRef]
- Szczeklik, K.; Krzysciak, W.; Domagala-Rodacka, R.; Mach, P.; Darczuk, D.; Cibor, D.; Pytko-Polonczyk, J.; Rodacki, T.; Owczarek, D. Alterations in Glutathione Peroxidase and Superoxide Dismutase Activities in Plasma and Saliva in Relation to Disease Activity in Patients with Crohn’s Disease. J. Physiol. Pharmacol. Off. J. Pol. Physiol. Soc. 2016, 67, 709–715. [Google Scholar]
- Wendland, B.; Aghdassi, E.; Tam, C.; Carrrier, J.; Steinhart, A.; Wolman, S.; Baron, D.; Allard, J. Lipid Peroxidation and Plasma Antioxidant Micronutrients in Crohn Disease. Am. J. Clin. Nutr. 2001, 74, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Bouzid, D.; Gargouri, B.; Mansour, R.B.; Amouri, A.; Tahri, N.; Lassoued, S.; Masmoudi, H. Oxidative Stress Markers in Intestinal Mucosa of Tunisian Inflammatory Bowel Disease Patients. Saudi J. Gastroenterol. Off. J. Saudi Gastroenterol. Assoc. 2013, 19, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Boehm, D.; Krzystek-Korpacka, M.; Neubauer, K.; Matusiewicz, M.; Berdowska, I.; Zielinski, B.; Paradowski, L.; Gamian, A. Paraoxonase-1 Status in Crohn’s Disease and Ulcerative Colitis. Inflamm. Bowel Dis. 2009, 15, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Sahin, M.; Bobusoglu, O.; Yetim, A.; Ates, F. Paraoxonase-1 and Arylesterase Levels in Patients with Ulcerative Colitis. Arab J. Gastroenterol. Off. Publ. Pan-Arab Assoc. Gastroenterol. 2019, 20, 14–18. [Google Scholar] [CrossRef]
- Szczeklik, K.; Mach, T.; Cibor, D.; Owczarek, D.; Sapa, J.; Papież, M.; Pytko-Polończyk, J.; Krzyściak, W. Correlation of Paraoxonase-1 with the Severity of Crohn’s Disease. Molecules 2018, 23, 2603. [Google Scholar] [CrossRef] [Green Version]
- Baskol, G.; Baskol, M.; Yurci, A.; Ozbakir, O.; Yucesoy, M. Serum Paraoxonase 1 Activity and Malondialdehyde Levels in Patients with Ulcerative Colitis. Cell Biochem. Funct. 2006, 24, 283–286. [Google Scholar] [CrossRef]
- La Du, B.N.; Billecke, S.; Hsu, C.; Haley, R.W.; Broomfield, C.A. Serum Paraoxonase (PON1) Isozymes: The Quantitative Analysis of Isozymes Affecting Individual Sensitivity to Environmental Chemicals. Drug Metab. Dispos. 2001, 29, 566–569. [Google Scholar]
- Sen, H. Relationship Between Bilirubin Level and Disease Activity in Crohns Disease. J. Clin. Anal. Med. 2016, 7. [Google Scholar] [CrossRef]
- Krzystek-Korpacka, M.; Neubauer, K.; Berdowska, I.; Boehm, D.; Zielinski, B.; Petryszyn, P.; Terlecki, G.; Paradowski, L.; Gamian, A. Enhanced Formation of Advanced Oxidation Protein Products in IBD. Inflamm. Bowel Dis. 2008, 14, 794–802. [Google Scholar] [CrossRef]
- Kaplan, M.; Yuksel, M.; Ates, I.; Kilic, Z.M.Y.; Kilic, H.; Kuzu, U.B.; Kayacetin, E. Is Ischemia Modified Albumin a Disease Activity Marker for Inflammatory Bowel Diseases? J. Gastroenterol. Hepatol. 2016, 31, 1120–1125. [Google Scholar] [CrossRef] [PubMed]
- Su, Q.; Li, X.; Mo, W.; Yang, Z. Low Serum Bilirubin, Albumin, and Uric Acid Levels in Patients with Crohn’s Disease. Medicine 2019, 98, e15664. [Google Scholar] [CrossRef] [PubMed]
- Bourgonje, A.R.; von Martels, J.Z.H.; Bulthuis, M.L.C.; van Londen, M.; Faber, K.N.; Dijkstra, G.; van Goor, H. Crohn’s Disease in Clinical Remission Is Marked by Systemic Oxidative Stress. Front. Physiol. 2019, 10, 499. [Google Scholar] [CrossRef] [PubMed]
- Kupcová, V.; Turecký, L.; Uhlíková, E. The Role of Oxidative Stress in Anti-Tumor Necrosis Factor Antibody Treatment in Crohn´s Disease. Curr. Med. Chem. 2012, 19. [Google Scholar] [CrossRef] [PubMed]
- Matusiewicz, M.; Neubauer, K.; Lewandowska, P.; Gamian, A.; Krzystek-Korpacka, M. Reduced Transferrin Levels in Active Inflammatory Bowel Disease. Biomed Res. Int. 2017, 2017, 9541370. [Google Scholar] [CrossRef] [Green Version]
- Casanova, M.J.; Chaparro, M.; Molina, B.; Merino, O.; Batanero, R.; Dueñas-Sadornil, C.; Robledo, P.; Garcia-Albert, A.M.; Gómez-Sánchez, M.B.; Calvet, X.; et al. Prevalence of Malnutrition and Nutritional Characteristics of Patients With Inflammatory Bowel Disease. J. Crohns. Colitis 2017, 11, 1430–1439. [Google Scholar] [CrossRef]
- Neselioglu, S.; Keske, P.; Senat, A.; Yurekli, O.; Erdogan, S.; Alisik, M.; Ergin, M.; Koseoglu, H.; Ersoy, O.; Erel, O. The Relationship between Severity of Ulcerative Colitis and Thiol-Disulphide Homeostasis. Bratislava Med. J. 2018, 119, 498–502. [Google Scholar] [CrossRef]
- Quinlan, G.J.; Martin, G.S.; Evans, T.W. Albumin: Biochemical Properties and Therapeutic Potential. Hepatology 2005, 41, 1211–1219. [Google Scholar] [CrossRef]
- Tufoni, M.; Baldassarre, M.; Zaccherini, G.; Antognoli, A.; Caraceni, P. Hemodynamic and Systemic Effects of Albumin in Patients with Advanced Liver Disease. Curr. Hepatol. Reports 2020. [Google Scholar] [CrossRef]
- Baba, S.P.; Bhatnagar, A. Role of Thiols in Oxidative Stress. Curr. Opin. Toxicol. 2018, 7, 133–139. [Google Scholar] [CrossRef]
- Nakatani, S.; Yasukawa, K.; Ishimura, E.; Nakatani, A.; Toi, N.; Uedono, H.; Tsuda, A.; Yamada, S.; Ikeda, H.; Mori, K.; et al. Non-Mercaptalbumin, Oxidized Form of Serum Albumin, Significantly Associated with Renal Function and Anemia in Chronic Kidney Disease Patients. Sci. Rep. 2018. [Google Scholar] [CrossRef] [PubMed]
- Kleinman, W.A.; Richie, J.P. Status of Glutathione and Other Thiols and Disulfides in Human Plasma. Biochem. Pharmacol. 2000, 60, 19–29. [Google Scholar] [CrossRef]
- Fu, X.; Cate, S.A.; Dominguez, M.; Osborn, W.; Özpolat, T.; Konkle, B.A.; Chen, J.; López, J.A. Cysteine Disulfides (Cys-SS-X) as Sensitive Plasma Biomarkers of Oxidative Stress. Sci. Rep. 2019, 9, 115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bocedi, A.; Cattani, G.; Stella, L.; Massoud, R.; Ricci, G. Thiol Disulfide Exchange Reactions in Human Serum Albumin: The Apparent Paradox of the Redox Transitions of Cys 34. FEBS J. 2018, 285, 3225–3237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oettl, K.; Marsche, G. Redox State of Human Serum Albumin in Terms of Cysteine-34 in Health and Disease. In Methods in Enzymology; Academic Press: Cambridge, MA, USA, 2010; Volume 474, pp. 181–195. [Google Scholar] [CrossRef]
- Nagumo, K.; Tanaka, M.; Chuang, V.T.G.; Setoyama, H.; Watanabe, H.; Yamada, N.; Kubota, K.; Tanaka, M.; Matsushita, K.; Yoshida, A.; et al. Cys34-Cysteinylated Human Serum Albumin Is a Sensitive Plasma Marker in Oxidative Stress-Related Chronic Diseases. PLoS ONE 2014, 9, e85216. [Google Scholar] [CrossRef] [PubMed]
- Bal, W.; Sokołowska, M.; Kurowska, E.; Faller, P. Binding of Transition Metal Ions to Albumin: Sites, Affinities and Rates. Biochim. Biophys. Acta Gen. Subj. 2013, 1830, 5444–5455. [Google Scholar] [CrossRef]
- Hamouda, H.E.; Zakaria, S.S.; Ismail, S.A.; Khedr, M.A.; Mayah, W.W. P53 Antibodies, Metallothioneins, and Oxidative Stress Markers in Chronic Ulcerative Colitis with Dysplasia. World J. Gastroenterol. 2011, 17, 2417–2423. [Google Scholar] [CrossRef]
- Koutroubakis, I.; Malliaraki, N.; Dimoulios, P.; Karmiris, K.; Castanas, E.; Kouroumalis, E. Decreased Total and Corrected Antioxidant Capacity in Patients with Inflammatory Bowel Disease. Dig. Dis. Sci. 2004, 49, 1433–1437. [Google Scholar] [CrossRef]
- Pereira, C.; Coelho, R.; Grácio, D.; Dias, C.; Silva, M.; Peixoto, A.; Lopes, P.; Costa, C.; Teixeira, J.P.; Macedo, G.; et al. DNA Damage and Oxidative DNA Damage in Inflammatory Bowel Disease. J. Crohn’s Colitis 2016, 10, 1316–1323. [Google Scholar] [CrossRef] [Green Version]
- Sampietro, G.; Cristaldi, M.; Cervato, G.; Maconi, G.; Danelli, P.; Cervellione, R.; Rovati, M.; Porro, G.; Taschieri, A. Oxidative Stress, Vitamin A and Vitamin E Behaviour in Patients Submitted to Conservative Surgery for Complicated Crohn’s Disease. Dig. Liver Dis. 2002, 34, 696–701. [Google Scholar] [CrossRef]
- Neubauer, K.; Kempinski, R.; Matusiewicz, M.; Bednarz-Misa, I.; Krzystek-Korpacka, M. Nonenzymatic Serum Antioxidant Capacity in IBD and Its Association with the Severity of Bowel Inflammation and Corticosteroids Treatment. Medicina 2019, 55, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lenicek, M.; Duricová, D.; Hradský, O.; Dusatkova, P.; Jiraskova, A.; Lukáš, M.; Nachtigal, P.; Vítek, L. The Relationship Between Serum Bilirubin and Crohn’s Disease. Inflamm. Bowel Dis. 2014, 20. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Li, L.; Li, X.; Li, J.; Wang, D.; Zhang, H. The Relationship between Serum Bilirubin and Inflammatory Bowel Disease. Mediators Inflamm. 2019, 2019, 5256460. [Google Scholar] [CrossRef] [PubMed]
- Schieffer, K.M.; Bruffy, S.M.; Rauscher, R.; Koltun, W.A.; Yochum, G.S.; Gallagher, C.J. Reduced Total Serum Bilirubin Levels Are Associated with Ulcerative Colitis. PLoS ONE 2017, 12, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tian, S.; Li, J.; Li, R.; Liu, Z.; Dong, W. Decreased Serum Bilirubin Levels and Increased Uric Acid Levels Are Associated with Ulcerative Colitis. Med. Sci. Monit. 2018, 24, 6298–6304. [Google Scholar] [CrossRef]
- Zhu, F.; Feng, D.; Zhang, T.; Gu, L.; Zhu, W.; Guo, Z.; Li, Y.; Lu, N.; Gong, J.; Li, N. Altered Uric Acid Metabolism in Isolated Colonic Crohn’s Disease but Not Ulcerative Colitis. J. Gastroenterol. Hepatol. 2019, 34, 154–161. [Google Scholar] [CrossRef] [Green Version]
- Gîlcă-Blanariu, G.-E.; Diaconescu, S.; Ciocoiu, M.; Ștefănescu, G. New Insights into the Role of Trace Elements in IBD. Biomed Res. Int. 2018, 2018, 1813047. [Google Scholar] [CrossRef]
- Forbes, A.; Escher, J.; Hébuterne, X.; Kłęk, S.; Krznaric, Z.; Schneider, S.; Shamir, R.; Stardelova, K.; Wierdsma, N.; Wiskin, A.E.; et al. ESPEN Guideline: Clinical Nutrition in Inflammatory Bowel Disease. Clin. Nutr. 2017, 36, 321–347. [Google Scholar] [CrossRef] [Green Version]
- Siva, S.; Rubin, D.T.; Gulotta, G.; Wroblewski, K.; Pekow, J. Zinc Deficiency Is Associated with Poor Clinical Outcomes in Patients with Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2017, 23, 152–157. [Google Scholar] [CrossRef] [Green Version]
- Castro Aguilar-Tablada, T.; Navarro-Alarcón, M.; Quesada Granados, J.; Samaniego Sánchez, C.; Rufián-Henares, J.Á.; Nogueras-Lopez, F. Ulcerative Colitis and Crohn’s Disease Are Associated with Decreased Serum Selenium Concentrations and Increased Cardiovascular Risk. Nutrients 2016, 8, 780. [Google Scholar] [CrossRef]
- Pinto, M.A.S.; Lopes, M.S.-M.S.; Bastos, S.T.O.; Reigada, C.L.L.; Dantas, R.F.; Neto, J.C.B.; Luna, A.S.; Madi, K.; Nunes, T.; Zaltman, C. Does Active Crohn’s Disease Have Decreased Intestinal Antioxidant Capacity? J. Crohns. Colitis 2013, 7, e358–e366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, E.J. The Role of Carotenoids in Human Health. Nutr. Clin. Care 2002, 5, 56–65. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, P.S.; Li, B.; Vachali, P.P.; Gorusupudi, A.; Shyam, R.; Henriksen, B.S.; Nolan, J.M. Lutein, Zeaxanthin, and Meso-Zeaxanthin: The Basic and Clinical Science Underlying Carotenoid-Based Nutritional Interventions against Ocular Disease. Prog. Retin. Eye Res. 2016, 50, 34–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levy, E.; Rizwan, Y.; Thibault, L.; Lepage, G.; Brunet, S.; Bouthillier, L.; Seidman, E. Altered Lipid Profile, Lipoprotein Composition, and Oxidant and Antioxidant Status in Pediatric Crohn Disease. Am. J. Clin. Nutr. 2000, 71, 807–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardin, A. Reduced Plasma Antioxidant Concentrations and Increased Oxidative DNA Damage in Inflammatory Bowel Disease. Scand. J. Gastroenterol. 2001, 36, 1289–1294. [Google Scholar] [CrossRef]
- Erichsen, K.; Hausken, T.; Ulvik, R.J.; Svardal, A.; Berstad, A.; Berge, R.K. Ferrous Fumarate Deteriorated Plasma Antioxidant Status in Patients with Crohn Disease. Scand. J. Gastroenterol. 2003, 38, 543–548. [Google Scholar] [CrossRef]
- Starczak, M.; Zarakowska, E.; Modrzejewska, M.; Dziaman, T.; Szpila, A.; Linowiecka, K.; Guz, J.; Szpotan, J.; Gawronski, M.; Labejszo, A.; et al. In Vivo Evidence of Ascorbate Involvement in the Generation of Epigenetic DNA Modifications in Leukocytes from Patients with Colorectal Carcinoma, Benign Adenoma and Inflammatory Bowel Disease. J. Transl. Med. 2018, 16, 204. [Google Scholar] [CrossRef]
- Ayala, A.; Muñoz, M.F.; Argüelles, S. Lipid Peroxidation: Production, Metabolism, and Signaling Mechanisms of Malondialdehyde and 4-Hydroxy-2-Nonenal. Oxid. Med. Cell. Longev. 2014, 2014, 360438. [Google Scholar] [CrossRef]
- Piłacik, B.; Nofer, T.W.; Wasowicz, W. F2-Isoprostanes Biomarkers of Lipid Peroxidation: Their Utility in Evaluation of Oxidative Stress Induced by Toxic Agents. Int. J. Occup. Med. Environ. Health 2002, 15, 19–27. [Google Scholar]
- Alagozlu, H.; Gorgul, A.; Bilgihan, A.; Tuncer, C.; Unal, S. Increased Plasma Levels of Advanced Oxidation Protein Products (AOPP) as a Marker for Oxidative Stress in Patients with Active Ulcerative Colitis. Clin. Res. Hepatol. Gastroenterol. 2012, 37. [Google Scholar] [CrossRef]
- Forrest, C.; Gould, S.; Darlington, L.; Stone, T. Levels of Purine, Kynurenine and Lipid Peroxidation Products in Patients with Inflammatory Bowel Disease. Adv. Exp. Med. Biol. 2003, 527, 395–400. [Google Scholar] [CrossRef] [PubMed]
- van Langenberg, D.R.; Della Gatta, P.; Warmington, S.A.; Kidgell, D.J.; Gibson, P.R.; Russell, A.P. Objectively Measured Muscle Fatigue in Crohn’s Disease: Correlation with Self-Reported Fatigue and Associated Factors for Clinical Application. J. Crohn’s Colitis 2014, 8, 137–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cracowski, J.-L.; Bonaz, B.; Bessard, G.; Bessard, J.; Anglade, C.; Fournet, J. Increased Urinary F2-Isoprostanes in Patients with Crohn’s Disease. Am. J. Gastroenterol. 2002, 97, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Owczarek, D.; Cibor, D.; Mach, T. Asymmetric Dimethylarginine (ADMA), Symmetric Dimethylarginine (SDMA), Arginine, and 8-Iso-Prostaglandin F2alpha (8-Iso-PGF2alpha) Level in Patients with Inflammatory Bowel Diseases. Inflamm. Bowel Dis. 2010, 16, 52–57. [Google Scholar] [CrossRef]
- Di Sabatino, A.; Santilli, F.; Guerci, M.; Simeone, P.; Ardizzone, S.; Massari, A.; Giuffrida, P.; Tripaldi, R.; Malara, A.; Liani, R.; et al. Oxidative Stress and Thromboxane-Dependent Platelet Activation in Inflammatory Bowel Disease: Effects of Anti-TNF-α Treatment. Thromb. Haemost. 2016, 116, 486–495. [Google Scholar] [CrossRef]
- Monasta, L.; Pierobon, C.; Princivalle, A.; Martelossi, S.; Marcuzzi, A.; Pasini, F.; Perbellini, L. Inflammatory Bowel Disease and Patterns of Volatile Organic Compounds in the Exhaled Breath of Children: A Case-Control Study Using Ion Molecule Reaction-Mass Spectrometry. PLoS ONE 2017, 12, 1–24. [Google Scholar] [CrossRef]
- Davies, M.J. Oxidative Damage to Proteins. In Encyclopedia of Radicals in Chemistry, Biology and Materials; American Cancer Society: Atlanta, GA, USA, 2012. [Google Scholar] [CrossRef]
- Knutson, C.G.; Mangerich, A.; Zeng, Y.; Raczynski, A.R.; Liberman, R.G.; Kang, P.; Ye, W.; Prestwich, E.G.; Lu, K.; Wishnok, J.S.; et al. Chemical and Cytokine Features of Innate Immunity Characterize Serum and Tissue Profiles in Inflammatory Bowel Disease. Proc. Natl. Acad. Sci. USA 2013, 110, E2332–E2341. [Google Scholar] [CrossRef] [Green Version]
- Guntas, G.; Sahin, A.; Duran, S.; Kahraman, R.; Duran, I.; Sonmez, C.; Calhan, T.; Sokmen, H.M. Evaluation of Ischemia-Modified Albumin in Patients with Inflammatory Bowel Disease. Clin. Lab. 2017, 63, 341–347. [Google Scholar] [CrossRef]
- Cooke, M.S.; Evans, M.D.; Dizdaroglu, M.; Lunec, J. Oxidative DNA Damage: Mechanisms, Mutation, and Disease. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2003, 17, 1195–1214. [Google Scholar] [CrossRef] [Green Version]
- Nair, J.; Gansauge, F.; Beger, H.; Dolara, P.; Winde, G.; Bartsch, H. Increased Etheno-DNA Adducts in Affected Tissues of Patients Suffering from Crohn’s Disease, Ulcerative Colitis, and Chronic Pancreatitis. Antioxid. Redox Signal. 2006, 8, 1003–1010. [Google Scholar] [CrossRef]
- Küçük, İ.; Tanoğlu, A.; Öncü, K.; Yılmaz, İ.; Kara, M.; Beyazıt, Y.; Akyol, T.; Kaplan, M.; Özarı, H.O.; Yazgan, Y. Immunohistochemical Activity of Prohibitin-2 and Stomatin-Like Protein-2 in Patients with Ulcerative Colitis. Turkish J. Gastroenterol. Off. J. Turk. Soc. Gastroenterol. 2016, 27, 233–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tontini, G.E.; Vecchi, M.; Pastorelli, L.; Neurath, M.F.; Neumann, H. Differential Diagnosis in Inflammatory Bowel Disease Colitis: State of the Art and Future Perspectives. World J. Gastroenterol. 2015, 21, 21–46. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Deeke, S.A.; Ning, Z.; Starr, A.E.; Butcher, J.; Li, J.; Mayne, J.; Cheng, K.; Liao, B.; Li, L.; et al. Metaproteomics Reveals Associations between Microbiome and Intestinal Extracellular Vesicle Proteins in Pediatric Inflammatory Bowel Disease. Nat. Commun. 2018, 9, 2873. [Google Scholar] [CrossRef] [PubMed]
- Scaldaferri, F.; Pizzoferrato, M.; Lopetuso, L.R.; Musca, T.; Ingravalle, F.; Sicignano, L.L.; Mentella, M.; Miggiano, G.; Mele, M.C.; Gaetani, E.; et al. Nutrition and IBD: Malnutrition and/or Sarcopenia? A Practical Guide. Gastroenterol. Res. Pract. 2017, 2017, 8646495. [Google Scholar] [CrossRef] [PubMed]
- Caldwell, R.B.; Toque, H.A.; Narayanan, S.P.; Caldwell, R.W. Arginase: An Old Enzyme with New Tricks. Trends Pharmacol. Sci. 2015, 36, 395–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torres, J.; Mehandru, S.; Colombel, J.-F.; Peyrin-Biroulet, L. Crohn’s Disease. Lancet 2017, 389, 1741–1755. [Google Scholar] [CrossRef]
- Ozhegov, E.; Zhivotova, E.; Lebedko, O.; Fleishman, M.; Alexeenko, S.; Timoshin, S. Intensity of Proliferative Processes and Degree of Oxidative Stress in the Mucosa of the Ileum in Crohn’s Disease. Bull. Exp. Biol. Med. 2012, 152, 420–423. [Google Scholar] [CrossRef]
- Szczeklik, K.; Krzyściak, W.; Cibor, D.; Kozioł, K.; Pocztar, H.; Pytko-Polończyk, J.; Mach, T.; Owczarek, D. Evaluation of Plasma Concentrations of Selected Antioxidant Parameters in Patients with Active Crohn’s Disease. Folia Med. Cracov. 2018, 58, 119–130. [Google Scholar]
- Gracie, D.J.; Williams, C.J.; Sood, R.; Mumtaz, S.; Bholah, H.M.; Hamlin, J.P.; Ford, A.C. Poor Correlation Between Clinical Disease Activity and Mucosal Inflammation, and the Role of Psychological Comorbidity, in Inflammatory Bowel Disease. Am. J. Gastroenterol. 2016, 111, 541–551. [Google Scholar] [CrossRef]
- Saigusa, S.; Araki, T.; Tanaka, K.; Hashimoto, K.; Okita, Y.; Fujikawa, H.; Okugawa, Y.; Toiyama, Y.; Inoue, Y.; Uchida, K.; et al. Identification of Patients with Developing Ulcerative Colitis-Associated Neoplasia by Nitrative DNA Damage Marker 8-Nitroguanin Expression in Rectal Mucosa. J. Clin. Gastroenterol. 2013, 47, e80–e86. [Google Scholar] [CrossRef]
- D’Incà, R.; Cardin, R.; Benazzato, L.; Angriman, I.; Martines, D.; Sturniolo, G. Oxidative DNA Damage in the Mucosa of Ulcerative Colitis Increases With Disease Duration and Dysplasia. Inflamm. Bowel Dis. 2004, 10, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Peyrin-Biroulet, L.; Sandborn, W.; Sands, B.E.; Reinisch, W.; Bemelman, W.; Bryant, R.V.; D’Haens, G.; Dotan, I.; Dubinsky, M.; Feagan, B.; et al. Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE): Determining Therapeutic Goals for Treat-to-Target. Am. J. Gastroenterol. 2015, 110, 1324–1338. [Google Scholar] [CrossRef] [PubMed]
- Krzystek-Korpacka, M.; Kempiński, R.; Bromke, M.; Neubauer, K. Biochemical Biomarkers of Mucosal Healing for Inflammatory Bowel Disease in Adults. Diagnostics 2020, 10, 367. [Google Scholar] [CrossRef] [PubMed]
- Atreya, R.; Neurath, M.F. Current and Future Targets for Mucosal Healing in Inflammatory Bowel Disease. Visc. Med. 2017, 33, 82–88. [Google Scholar] [CrossRef]
- Ardizzone, S.; Cassinotti, A.; Duca, P.; Mazzali, C.; Penati, C.; Manes, G.; Marmo, R.; Massari, A.; Molteni, P.; Maconi, G.; et al. Mucosal Healing Predicts Late Outcomes after the First Course of Corticosteroids for Newly Diagnosed Ulcerative Colitis. Clin. Gastroenterol. Hepatol. 2011, 9, 483–489.e3. [Google Scholar] [CrossRef]
- Te Velde, A.A.; Pronk, I.; de Kort, F.; Stokkers, P.C.F. Glutathione Peroxidase 2 and Aquaporin 8 as New Markers for Colonic Inflammation in Experimental Colitis and Inflammatory Bowel Diseases: An Important Role for H2O2? Eur. J. Gastroenterol. Hepatol. 2008, 20, 555–560. [Google Scholar] [CrossRef]
- Poulsen, N.A.; Andersen, V.; Møller, J.C.; Møller, H.S.; Jessen, F.; Purup, S.; Larsen, L.B. Comparative Analysis of Inflamed and Non-Inflamed Colon Biopsies Reveals Strong Proteomic Inflammation Profile in Patients with Ulcerative Colitis. BMC Gastroenterol. 2012, 12, 76. [Google Scholar] [CrossRef] [Green Version]
- Magro, F.; Gionchetti, P.; Eliakim, R.; Ardizzone, S.; Armuzzi, A.; Barreiro-de Acosta, M.; Burisch, J.; Gecse, K.; Hart, A.; Hindryckx, P.; et al. Third European Evidence-Based Consensus on Diagnosis and Management of Ulcerative Colitis. Part 1: Definitions, Diagnosis, Extra-Intestinal Manifestations, Pregnancy, Cancer Surveillance, Surgery, and Ileo-Anal Pouch Disorders. J Crohns Colitis. 2017, 11, 649–670. [Google Scholar] [CrossRef]
- Annese, V.; Daperno, M.; Rutter, M.D.; Amiot, A.; Bossuyt, P.; East, J.; Ferrante, M.; Götz, M.; Katsanos, K.H.; Kießlich, R.; et al. European Evidence Based Consensus for Endoscopy in Inflammatory Bowel Disease. J. Crohns. Colitis 2013, 7, 982–1018. [Google Scholar] [CrossRef] [Green Version]
- Laine, L.; Kaltenbach, T.; Barkun, A.; McQuaid, K.R.; Subramanian, V.; Soetikno, R. SCENIC International Consensus Statement on Surveillance and Management of Dysplasia in Inflammatory Bowel Disease. Gastroenterology 2015, 148, 639–651.e28. [Google Scholar] [CrossRef]
- Chen, R.; Pan, S.; Lai, K.; Lai, L.; Crispin, D.; Bronner, M.; Brentnall, T. Up-Regulation of Mitochondrial Chaperone TRAP1 in Ulcerative Colitis Associated Colorectal Cancer. World J. Gastroenterol. 2014, 20, 17037–17048. [Google Scholar] [CrossRef] [PubMed]
- Feuerstein, J.D.; Cheifetz, A.S. Crohn Disease: Epidemiology, Diagnosis, and Management. Mayo Clin. Proc. 2017, 92, 1088–1103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuffari, C. Diagnostic Considerations in Pediatric Inflammatory Bowel Disease Management. Gastroenterol. Hepatol. 2009, 5, 775–783. [Google Scholar]
- Shores, D.R.; Everett, A.D. Children as Biomarker Orphans: Progress in the Field of Pediatric Biomarkers. J. Pediatr. 2018, 193, 14–20.e31. [Google Scholar] [CrossRef]


{kind=link}
| Analyte | Type | Disease | Evaluated Population 1 | Findings 2 | Diagnostic Characteristics | Ref. |
|---|---|---|---|---|---|---|
| OSI | BS | IBD | 40 CD (ns/CDAI, ns); 40 UC (ns/RI-EAI, ns); 80 HC | ↑ in CD and UC vs. HC; CDAI 0.87; CRP 3 0.39; RI-EAI 0.83; CRP 4 0.40 | IBD predictor: OR = 4.6 (2.7–7.7); predictor of log (CDAI) (B ± SE = 0.71 ± 0.06) and log (RI-EAI) (B ± SE = 0.6 ± 0.07) | [20] |
| PON1A (E.C. 3.1.1.2) | BP | IBD | 52 CD (37/CDAI ≥ 150) 67 UC (30/MDAI, ns); 99 HC | ↓ in aCD and aUC vs. HC; ↓ in aCD vs. iCD; ↓ in aUC vs. iUC; CDAI −0.47; ESR3 −0.36; IL-63 −0.45; MDAI −0.50; CRP4 −0.29; ESR4 −0.37; IL-64: −0.45 | CD marker: AUC = 0.74 6; cut-off ≤ 122 U: sens. 48%, spec. 90% UC marker: AUC = 0.65 6; cut-off ≤ 138 U: sens. 51%, spec. 75% Differential CD/UC marker: AUC = 0.63 7; cut-off ≤ 101 U: sens. 35%, spec. 88% | [45] |
| PON1A (E.C. 3.1.1.2) | BS | IBD | 40 CD (ns/CDAI, ns) 40 UC (ns/RI-EAI, ns); 80 HC | ↓ in CD and UC vs. HC; ESR 4: 0.40 | IBD predictor: OR = 0.995 (0.992 0.997) | [20] |
| PON1P (E.C. 3.1.8.1) | BP | CD | 47 CD (28/CDAI ≥ 150); 23 HC | ↓ in CD vs. HC; ↓ in aCD vs. iCD; CRP: −0.61 | CD marker: AUC = 0.96; cut-off 378.25 U/L, sens. 94%, spec. 91%; Active CD marker: AUC = 0.87; cut-off 305.31 U/L, sens. 86%, spec. 84% | [47] |
| t-bil | BS | CD | 90 CD (ns/ns, ns); 229 HC | ↓ in CD; no association with Montreal classification | OR = 0.87 (0.82–0.92): each ↓ in t-bil by 1 mmol/L is associated with a 13% ↑ in the risk of CD manifestation | [74] |
| t-bil | BS | IBD | 254 CD and 254 HC (learning) 187 UC and 187 HC (learning) 233 CD and 233 HC (validation) 124 UC and 124 controls (validation) | ↓ in UC and CD vs. HC | For the lowest quartile of t-bil, an association with CD was OR: 1.91 (1.26–2.91) and with UC-OR: 1.98 (1.09–3.63) in the learning cohort and OR: 3.60 (2.19–5.99) and 6.07 (3.01–12.75) in the validation cohort | [76] |
| t-bil | BS | UC | 170 UC (94/MDAI ≥ 3); 200 HC | ↓ in UC; no association with UC activity | For the lowest quartile of t-bil, an association with UC was OR = 2.56, 95% CI: 1.54–4.25, P < 0.001 | [77] |
| UA | BS | UC | 170 UC (94/MDAI ≥ 3); 200 HC | ↑ in UC; no association with UC activity | For the highest quartile of UA, an association with UC was OR = 1.20, 95% CI: 1.05–1.77, P = 0.045 | [77] |
| MDA (TBARS) | BP | CD | 52 CD (37/CDAI ≥ 150); 99 HC | ↑ aCD and iCD vs. HC; IL-6 −0.31; no association with activity | General CD marker: AUC = 0.91 (0.85–0.95); cut-off 1.03 µM, sens. 75%, spec. 90%, LR+ 7.4 and LR− 0.28 | [21] |
| aAOPP | BS | IBD | 68 UC (33/MDAI, ns) 50 CD (38/CDAI, ns); 45 HC | ↑in aUC and iUC vs. HC; ↑ in aCD vs. HC CDAI 0.42; ESR 3 0.53; ESR 4 0.35 | IBD marker:AUC = 0.64 (0.56 − 0.72) 3; Cut-off: 1.67 µmol/g, sens. 52%, spec. = 80%, LR+ 2.6 and LR− 0.6 | [51] |
| IMA | BS | IBD | 35 UC (ns/RI-EAI ≥ 5) 33 CD (ns/CDAI ≥ 150); 65 HC | ↑ in UC and CD vs. HC; ↑ in UC vs. CD CDAI 0.32; CRP 3 0.30; ESR 3 0.32 RI-EAI 0.31; CRP 4 0.40; ESR 4 0.43 | 1 unit of ↑ in IMA projects 1.5× ↑ risk of being IBD: OR: 1.5 (1.1–1.9) log(IMA) is an independent predictor of log (CDAI) (B ± SE = 2.33 ± 0.72) and log (RI-EAI) (1.82 ± 0.59) | [52] |
| VOCs | ΔB | IBD | 34 pediatric CD (ns); 33 UC (ns); 65 GIS; 102 HC | Model for differentiating IBD from controls (GIS + HC): 18 VOCs + age: AUC 0.93 (0.89–0.96); could detect 96% of all IBD cases with 69% specificity Model for differentiating CD from UC: 13 VOCs + age: AUC 0.93 (0.88–0.99); 86.6% correctly classified cases, 94% sens. and 76% spec. in detecting CD Model for differentiating IBD from GIS: 15 VOCs + age: AUC 0.92 (0.87–0.96), identifies correctly 94% of IBDs, with a specificity of 65% | [98] | |
| Analyte | Type | Disease | Evaluated Population 1 | Findings 2 | Application | Ref. |
|---|---|---|---|---|---|---|
| IoFRP | T-H | CD | 45 CD (aa/ns); 30 IBS; IS | ↑ in CD vs. IBS | Diff. CD/IBS | [110] |
| RoPRG | T-H | CD | 45 CD (aa/ns); 30 IBS; IS | ↑ in CD vs. IBS | Diff. CD/IBS | [110] |
| StP | T-H | CD | 45 CD (aa/ns); 30 IBS; IS | ↑ in CD vs. IBS | Diff. CD/IBS | [110] |
| LOX5 (E.C. 1.13.11.34) | T-M | IBD | 25 pediatric CD (aa/PCDAI, ns); 22 pediatric UC (aa/PUCAI, ns); 24 GIS | ↑ in IBD vs. GIS; (8.2× in AsC, 9× in DesC, 11.6× in TI) 3 | Diff. IBD/GIS | [106] |
| NOS2 (E.C. 1.14.13.39) | T-M | IBD | 25 pediatric CD (aa/PCDAI, ns); 22 pediatric UC (aa/PUCAI, ns); 24 GIS | ↑ in IBD vs. GIS (16.3× in AsC, 9.5× in DesC, 5.3× in TI) 3 ↑ in UC in AsC (3.5×), DeC (3×), and TI (2.7×) 3 | Diff. IBD/GIS Diff. CD/UC | [106] |
| NO | T-H | IBD | 22 UC (15/ns), paired biopsies inf. & non-infl. colon (n = 6 aUC); 11 CD (6/ns); 14 specific colitis (infl.); 10 GIS | ↑ in aUC and iUC vs. GIS; ↑ in aCD and iCD vs. GIS; ↑ in spec. colitis vs. GIS; ↑ in aUC/aCD vs. iUC/iCD ↑ in infl. and non-infl. aUC vs. iUC and GIS; If stratified by severity into: GIS/iIBD/miIBD/moIBD/sIBD, r = 0.81 | Diff. IBD/GIS | [19] |
| CPP | T-M | IBD | 25 pediatric CD (aa/PCDAI, ns); 22 pediatric UC (aa/PUCAI, ns); 24 GIS | ↑ in IBD vs. GIS; (46× in AsC, 29× in DeC, 37× in TI) 3; ↑ in CD in DeC (1.4×) and TI (5.7×) but ↑ in UC in AsC (6.2×) 3 | Diff. IBD/GISDiff. CD/UC | [106] |
| mGPx (E.C. 1.11.1.9) | T-M | IBD | 25 pediatric CD (aa/PCDAI, ns); 22 pediatric UC (aa/PUCAI, ns); 24 GIS | ↑ in IBD vs. GIS; 4× (AsC), 14× (DeC), 11× (TI) 3 | Diff. IBD/GIS | [106] |
| Alb | BP | CD | 55 CD (35/CDAI ≥ 150); 25 GIS | ↓ in aCD vs. GIS; ↓ in aCD vs. iCD; CDAI −0.76; CRP −0.41 | Diff. CD/GIS | [111] |
| TAS (FRAP) | BP | CD | 55 CD (35/CDAI ≥ 150); 25 GIS | ↓ in aCD vs. GIS; ↓ in aCD vs. iCD; CDAI −0.57; CRP −0.46 | Diff. CD/GIS | [111] |
| TAS (SIND2) | T-H | CD | 45 CD (aa/ns); 30 IBS; IS | ↑ in CD vs. IBS | Diff. CD/IBS | [110] |
| t-bil | BP | CD | 55 CD (35/CDAI ≥ 150); 25 GIS | ↓ in aCD vs. GIS; ↓ in aCD vs. iCD; CDAI −0.52; CRP −0.48 | Diff. CD/GIS | [111] |
| GSH | BP | CD | 55 CD (35/CDAI ≥ 150); 25 GIS | ↓ in aCD vs. GIS; ↓ in aCD vs. iCD; CDAI −0.76; CRP −0.41 | Diff. CD/GIS | [111] |
| LOOH | T-H | CD | 45 CD (aa/ns); 30 IBS; IS | ↑ in CD vs. IBS | Diff. CD/IBS | [110] |
| Vit.C | BP | IBD | 51 IBD (ns); 67 AD (90% tubulare); 136 CRC; 79 HC | ↑ in IBD vs. CRC | Diff. IBD/CRC | [89] |
| Vit.A | BP | IBD | 51 IBD (ns); 67 AD (90% tubulare); 136 CRC; 79 HC | ↑ in IBD vs. CRC | Diff. IBD/CRC | [89] |
| PC | T-H | CD, UC | 22 UC (15/ns), paired biopsies inf. & non-infl. colon (n = 6 aUC); 11 CD (6/ns); 14 specific colitis (infl.); 10 GIS | ↑ in aUC and iUC vs. GIS; ↑ in aCD and iCD vs. GIS; ↑ in spec. colitis vs. GIS; ↑ in aUC/aCD vs. iUC/iCD; ↑ in infl. and non-infl. aUC vs. iUC and GIS; ↑ in infl. aUC vs. non-infl.; If stratified by severity into: CON/iIBD/miIBD/moIBD/sIBD, r = 0.81 | Diff. IBD/GIS | [19] |
| nTyr | T-H | CD, UC | 22 UC (15/ns), paired biopsies inf. & non-infl. colon (n = 6 aUC); 11 CD (6/ns); 14 specific colitis (infl.); 10 GIS | ↑ in aUC and iUC vs. GIS; ↑ in aCD and iCD vs. GIS; ↑ in spec. colitis vs. GIS; ↑ in aUC/aCD vs. iUC/iCD; ↑ in infl. and non-infl. aUC vs. iUC and GIS; ↑ in infl. aUC vs. non-infl.; If stratified by severity into: CON/iIBD/miIBD/moIBD/sIBD, r = 0.84 | Diff. IBD/GIS | [19] |
| 8-OHdG | BL | IBD | 51 IBD (ns); 67 AD (90% tubulare); 136 CRC; 79 HC | ↑ in IBD vs. AD and CRC and HC | Diff. IBD/N | [89] |
| Analyte | Type | Disease | Evaluated Population 1 | Findings 2 | Characteristics | Ref. |
|---|---|---|---|---|---|---|
| NOS2 | T-I | UC | 141 FFPE rectal UC mucosa slides: 18 N (9 D and 9 UCAC) | Insignificantly higher IHC-score in UC+N vs. UC alone | Progression marker: cut-of = 50 IHC-score: sens. 67%, spec. 49% | [113] |
| CAT | BE | IBD | 93 UC (42/RI, ns) 81 CD (53/CDAI ≥ 150); 105 HC | ↓ in aCD and aUC vs. HC; ↓ in aCD vs. iCD; CDAI −0.30; CRP 3 −0.34; ESR 3 −0.32; MES 4 −0.22; ESR 4 −0.22 | Active IBD marker: AUC = 0.63 5; cut-off ≤128 U/mL: sens. 86%, spec. 39% | [31] |
| GPx | BE | IBD | 93 UC (42/RI, ns) 81 CD (53/CDAI ≥ 150); 105 HC | ↓ in aCD and iCD vs. HC; ↓ in aUC and iUC vs. HC; ↓ in aCD vs. iCD; ↓ in aUC vs. iUC; CDAI −0.50; CRP 3 −0.36; IL-6 3: −0.42; RI −0.36; ESR 4 −0.37 | Active IBD marker: AUC = 0.73 5; Cut-off ≤5.88 U/mL: sens. 58%, spec. 80% | [31] |
| PON1P | BP | CD | 47 CD (28/CDAI≥150); 23 HC | ↓ in aCD vs. iCD; CRP: −0.61 | Active CD marker: AUC = 0.87; cut-off 305.31 U/L, sens. 86%, spec. 84% | [47] |
| F-SH | BS | IBD | 47 CD (37/CDAI ≥ 150) 71 UC (30/RI ≥ 6); 57 HC | ↓aCD and iCD vs. HC; ↓aUC and iUC vs. HC; CDAI −0.52; RI −0.40; MES 4 −0.27; CRP 3 −0.56; ESR 3 −0.51; IL-6 3 −0.45 | MH (MES = 0–1) marker; AUC = 0.69; >409 µM, sens. 74% and spec. 60% | [73] |
| Trf | BS | IBD | 63 CD (36/CDAI ≥ 150) 74 UC (28/RI ≥ 6); 97 HC | ↓aCD and aUC vs. iCD and iUC and HC; CDAI −0.49; CRP 3 −0.52; IL-6 3 −0.47; RI −0.52; MES 4 −0.37; CRP 4 −0.29; ESR 4 −0.31; IL-6 4 −0.49 | Active UC marker: AUC = 0.76 (0.65–0.85); cut-off ≤279 mg/dL, sens. 86%, spec. 65% | [56] |
| TAS (ABTS) | BS | IBD | 47 CD (37/CDAI ≥ 150) 71 UC (30/RI ≥ 6); 57 HC | ↓aCD and iCD vs. HC; ↓aUC and iUC vs. HC; CDAI −0.34; MES 4 −0.58; CRP 3 −0.56; CRP 4 −0.60 | MH (MES = 0–1) marker: AUC = 0.87; cut-off>1.4 mM, sens. 61%, spec. 100% | [73] |
| TAS (FRAP) | BS | CD | 58 CD (36/CDAI ≥ 150); 26 HC | ↓aCD vs. iCD and HC; CDAI −0.8; CRP −0.5 | Active CD marker: AUC = 0.94 (0.89–0.99) 7 | [37] |
| UA | BS | IBD | 47 CD (37/CDAI ≥ 150) 71 UC (30/RI ≥ 6); 57 HC | ↓aCD and aUC vs. iCD and iUC and HC; CDAI −0.35; MES 4 −0.41 | MH (MES = 0–1) marker: AUC = 0.77; cut-off>2.81 mg/dL, sens. 76%, spec. 80% | [73] |
| GSH (DTNB) | BS | CD | 58 CD (36/CDAI ≥ 150); 26 HC | ↓aCD vs. iCD and HC; CDAI −0.8; CRP −0.5 | Active CD marker: AUC = 0.86 (0.78–0.95) 4 | [37] |
| MDA (TBARS) | BS | CD | 58 CD (36/CDAI ≥ 150); 26 HC | ↑aCD vs. iCD and HC; CDAI 0.8; CRP 0.6 | Active CD marker: AUC = 0.95 (0.9–1) 4; cut-off >3.82 nmol/g, sens. 93%, spec. 80% | [37] |
| 8-OHdG | T-H | UC | Multiple biopsies from: 50 UC patients, 6 UC+LGD, 4 UC+HGD/UCAC, 5 sporadic CRC, 11 GIS; BES | ↑in UC and UC+LGD vs. GIS; ↑ in UC+LGD vs. UC; ↑ in SC vs. R;HA: r = 0.33; EA: r = 0.37 | Progression marker: AUC = 0.81 (SE = 0.06); cut-off: 100 adducts/10^5dG, sens. = 70%, spec. = 78%, PPV = 47%, NPV = 94% | [114] |
| 8-OHdG | T-I | UC | 141 FFPE rectal UC mucosa slides: 18 N (9 dysplasia and 9 UCAC) | ↑ IHC-score in UC+N vs. UC alone | Progression marker: cut-off = 196 IHC-score: sens. 89% and 55% spec. | [113] |
| 8-NG | T-I | UC | 141 FFPE rectal UC mucosa slides: 18 N (9 D and 9 UCAC) | ↑ IHC-score in UC+N vs. UC alone | Progression marker: cut-off = 52 IHC-score: sens. 83% and 83% spec. | [113] |
| Analyte | Type | Disease | Evaluated Population 1 | Findings 2 | Ref. |
|---|---|---|---|---|---|
| Zn | BS | IBD | 773 CD; 223 UC; patients stratified into Zn-deficient (Zn<0.66 mcg/ml) and Zn-normal; analysis of IBD registry data | Zn-deficient patients have ↑risk of: CD: hospitalizations OR = 1.44 (1.02–2.04), surgeries OR = 2.05 (1.38–3.05), complications OR = 1.50 (1.04–2.15); UC: hospitalizations, 2.14 (1.07–4.29), surgeries OR = 1.64 (0.59–4.52), complications OR = 1.97 (0.94–4.11) | [81] |
| MDA (TBARS) | BP | CD | 25 adult CD; 88 HC;21 pediatric CD; 11 HC | ↑in complications (abscess, fistula or stenosis) | [35] |
| GSH | BE | CD | 25 adult CD; 88 HC; 21 pediatric CD; 11 HC | ↓ in complications (abscess, fistula or stenosis) | [35] |
| t-bil | BS | IBD | 242 CD; 211 UC; 255 HC | ↓ in UC-E3 (extension); ↓ in colonic CD (L2); ↓ in penetrating CD(B3) | [75] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krzystek-Korpacka, M.; Kempiński, R.; Bromke, M.A.; Neubauer, K. Oxidative Stress Markers in Inflammatory Bowel Diseases: Systematic Review. Diagnostics 2020, 10, 601. https://doi.org/10.3390/diagnostics10080601
Krzystek-Korpacka M, Kempiński R, Bromke MA, Neubauer K. Oxidative Stress Markers in Inflammatory Bowel Diseases: Systematic Review. Diagnostics. 2020; 10(8):601. https://doi.org/10.3390/diagnostics10080601
Chicago/Turabian StyleKrzystek-Korpacka, Małgorzata, Radosław Kempiński, Mariusz A. Bromke, and Katarzyna Neubauer. 2020. "Oxidative Stress Markers in Inflammatory Bowel Diseases: Systematic Review" Diagnostics 10, no. 8: 601. https://doi.org/10.3390/diagnostics10080601