Evaluation of MicroRNAs as Non-Invasive Diagnostic Markers in Urinary Cells from Patients with Suspected Prostate Cancer


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Cohort
2.2. Collection and Processing of Urine Samples
2.3. RNA Isolation and cDNA Synthesis
2.4. Quantitative Polymerase Chain Reaction
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Patients Undergoing Prostate Biopsy
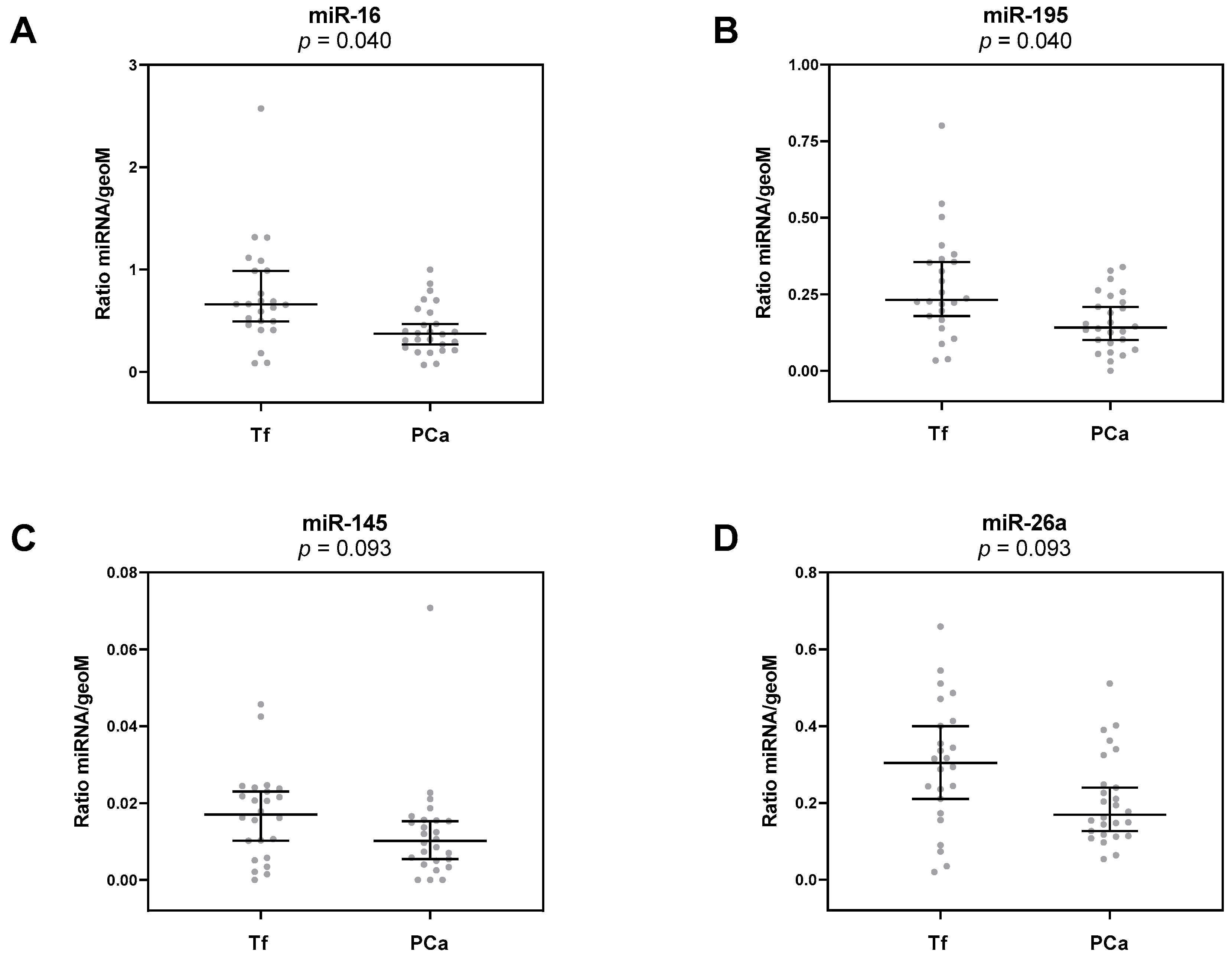
3.2. Deregulation of Urinary miRNAs in PCa
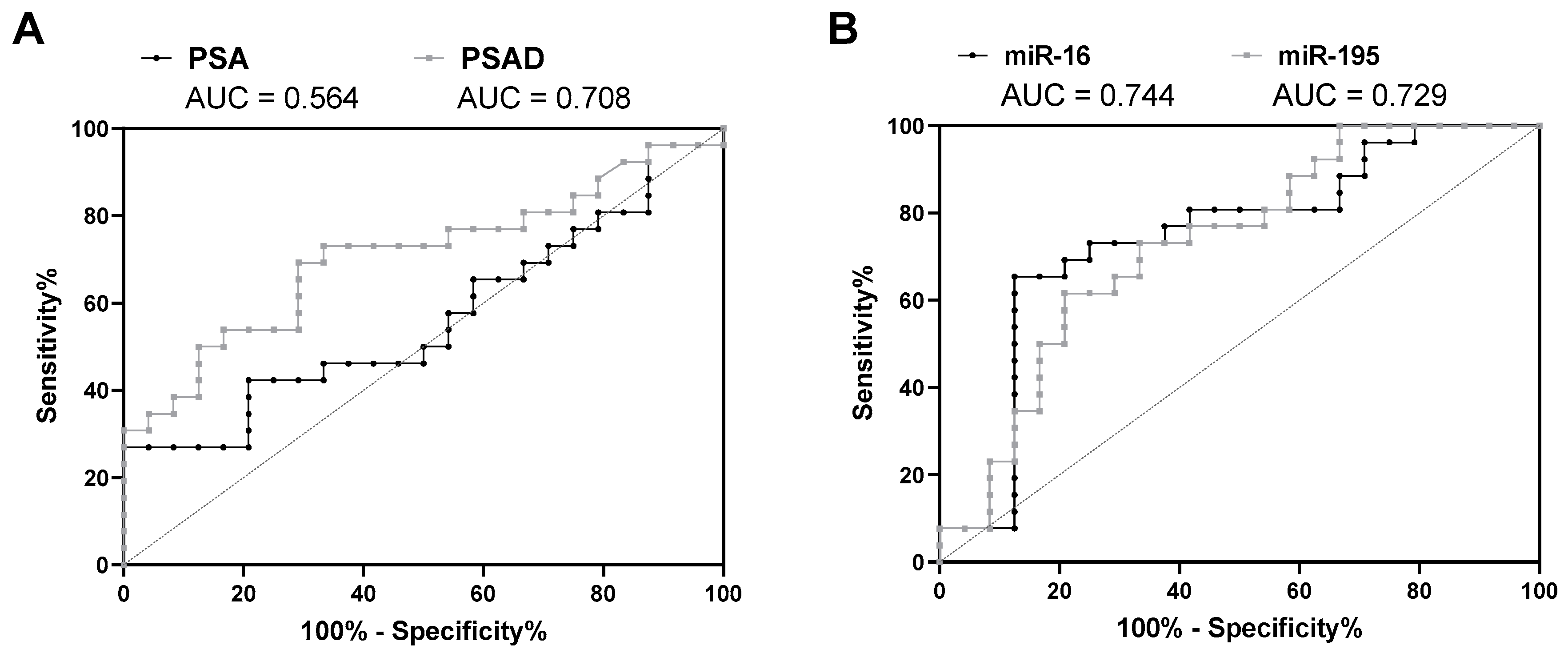
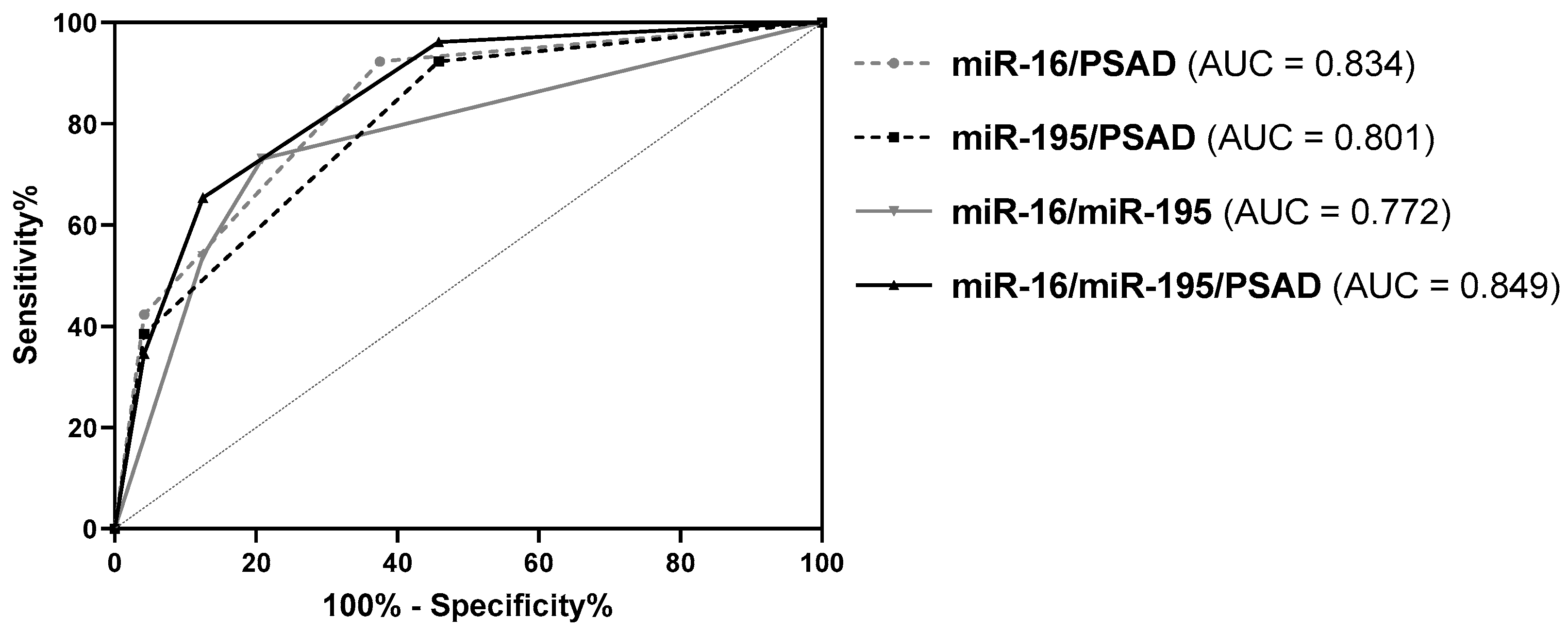
3.3. Diagnostic Potential of miRNA Expression Levels in Urinary Cells
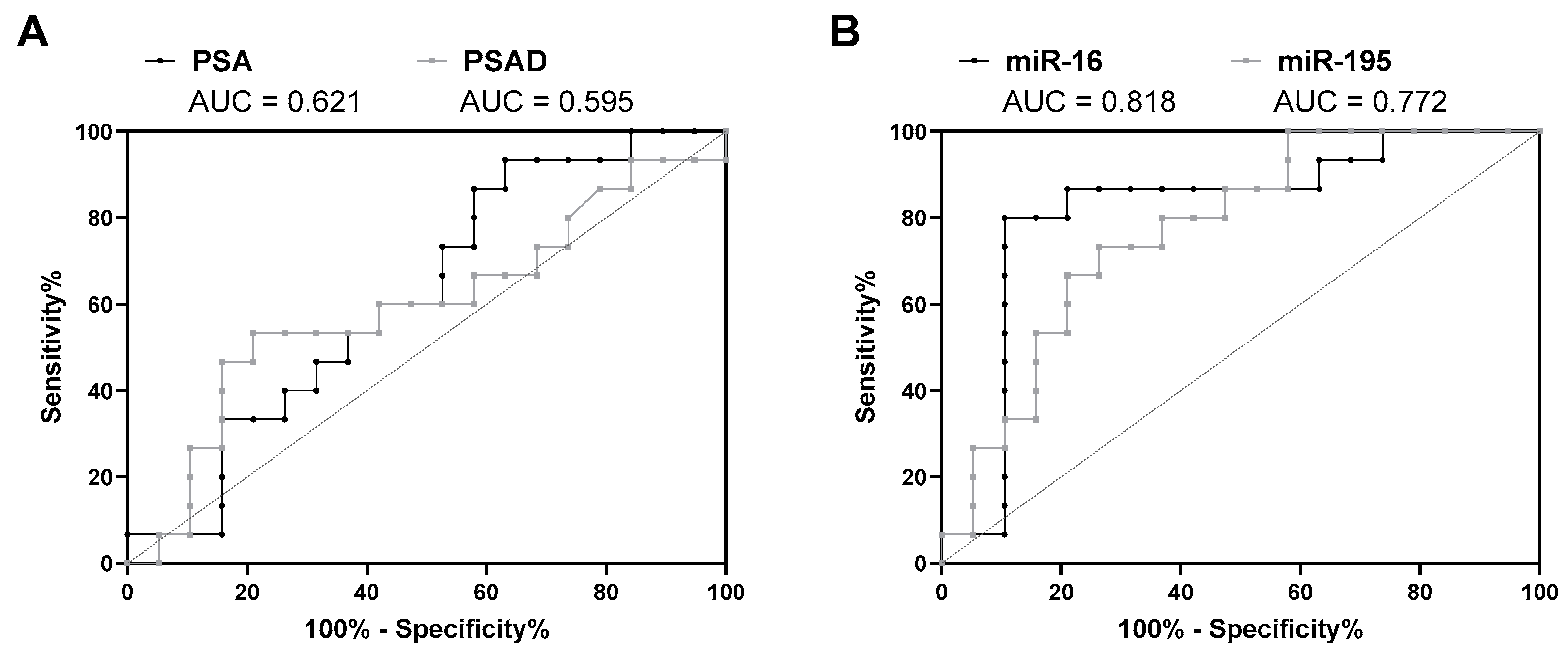
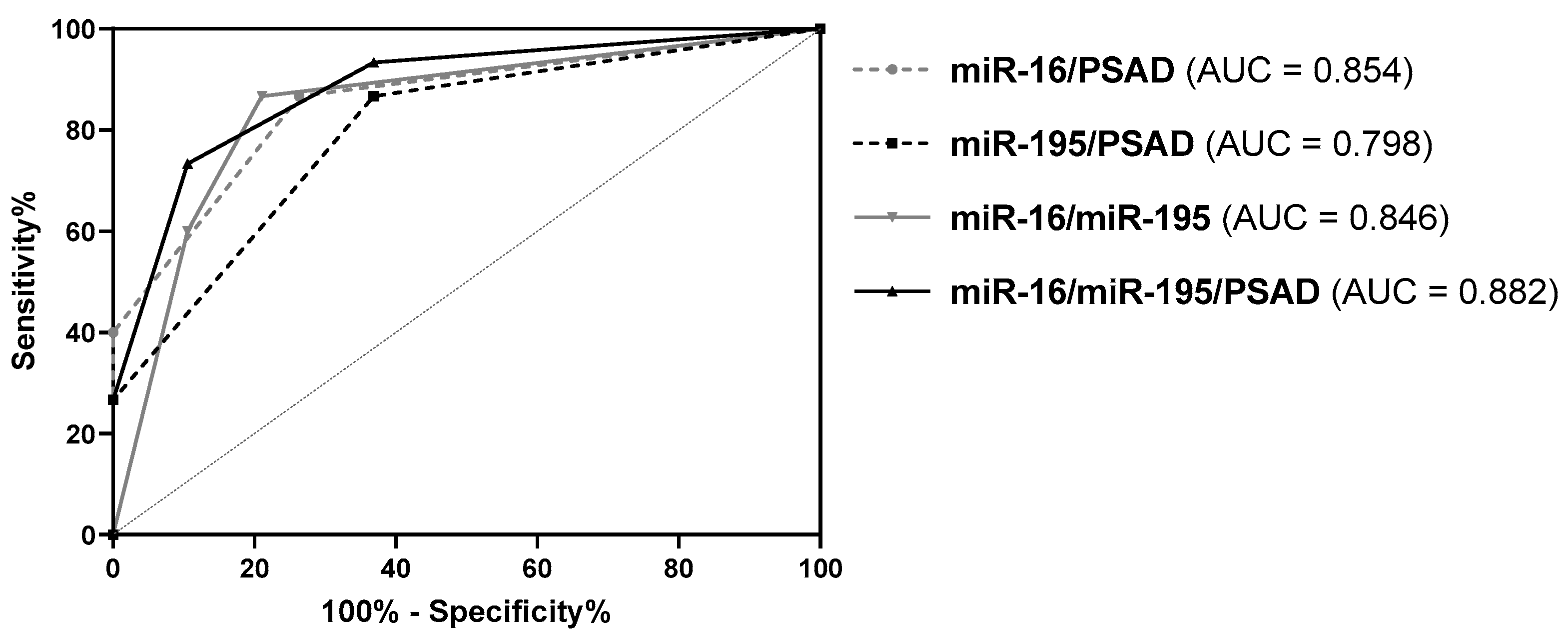
3.4. Diagnostic Potential of miRNA Expression Levels in Urinary Cells in the Sub-Cohort of Patients with PSA Levels ≤ 10 ng/mL
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luengo-Fernandez, R.; Leal, J.; Gray, A.; Sullivan, R. Economic burden of cancer across the European Union: A population-based cost analysis. Lancet Oncol. 2013, 14, 1165–1174. [Google Scholar] [CrossRef]
- Mottet, N.; Bellmunt, J.; Bolla, M.; Briers, E.; Cumberbatch, M.G.; De Santis, M.; Fossati, N.; Gross, T.; Henry, A.M.; Joniau, S.; et al. EAU-ESTRO-SIOG Guidelines on Prostate Cancer. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2017, 71, 618–629. [Google Scholar] [CrossRef] [PubMed]
- Tosoian, J.; Loeb, S. PSA and Beyond: The Past, Present, and Future of Investigative Biomarkers for Prostate Cancer. Sci. World J. 2010, 10, 1919–1931. [Google Scholar] [CrossRef]
- Marra, G.; Ploussard, G.; Futterer, J.; Valerio, M. EAU-YAU Prostate Cancer Working Party. Controversies in MR targeted biopsy: Alone or combined, cognitive versus software-based fusion, transrectal versus transperineal approach? World J. Urol. 2019, 37, 277–287. [Google Scholar] [CrossRef]
- Nordström, T.; Akre, O.; Aly, M.; Grönberg, H.; Eklund, M. Prostate-specific antigen (PSA) density in the diagnostic algorithm of prostate cancer. Prostate Cancer Prostatic Dis. 2017, 21, 57–63. [Google Scholar] [CrossRef]
- Raja, N.; Russell, C.M.; George, A.K. Urinary markers aiding in the detection and risk stratification of prostate cancer. Transl. Androl. Urol. 2018, 7, S436–S442. [Google Scholar] [CrossRef]
- Filella, X.; Foj, L.; Milà, M.; Augé, J.M.; Molina, R.; Jiménez, W. PCA3 in the detection and management of early prostate cancer. Tumor Biol. 2013, 34, 1337–1347. [Google Scholar] [CrossRef]
- Di Meo, A.; Bartlett, J.; Cheng, Y.; Pasic, M.D.; Mac-Way, F. Liquid biopsy: A step forward towards precision medicine in urologic malignancies. Mol. Cancer 2017, 16, 80. [Google Scholar] [CrossRef]
- Mlcochova, H.; Hezova, R.; Stanik, M.; Capoor, M.N. Urine microRNAs as potential noninvasive biomarkers in urologic cancers. Urol. Oncol. Semin. Orig. Investig. 2014, 32, 41.e1–41.e9. [Google Scholar] [CrossRef]
- Filella, X.; Foj, L. miRNAs as novel biomarkers in the management of prostate cancer. Clin. Chem. Lab. Med. 2017, 55, 715–736. [Google Scholar] [CrossRef] [PubMed]
- Iorio, M.V.; Croce, C.M. microRNA involvement in human cancer. Carcinogenesis 2012, 33, 1126–1133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erdmann, K.; Kaulke, K.; Thomae, C.; Huebner, D.; Sergon, M.; Froehner, M.; Wirth, M.P.; Fuessel, S. Elevated expression of prostate cancer-associated genes is linked to down-regulation of microRNAs. BMC Cancer 2014, 14, 82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porkka, K.P.; Pfeiffer, M.J.; Waltering, K.K.; Vessella, R.L.; Tammela, T.L.; Visakorpi, T. MicroRNA Expression Profiling in Prostate Cancer. Cancer Res. 2007, 67, 6130–6135. [Google Scholar] [CrossRef] [Green Version]
- Schubert, M.; Spahn, M.; Kneitz, S.; Scholz, C.J.; Joniau, S.; Stroebel, P.; Riedmiller, H.; Kneitz, B. Distinct microRNA Expression Profile in Prostate Cancer Patients with Early Clinical Failure and the Impact of let-7 as Prognostic Marker in High-Risk Prostate Cancer. PLoS ONE 2013, 8, e65064. [Google Scholar] [CrossRef] [Green Version]
- Lupold, S.E.; Kumar, B. MicroRNA expression and function in prostate cancer: A review of current knowledge and opportunities for discovery. Asian J. Androl. 2016, 18, 559–567. [Google Scholar] [CrossRef]
- Paiva, R.M.; Zauli, D.A.G.; Neto, B.S.; Brum, I.S. Urinary microRNAs expression in prostate cancer diagnosis: A systematic review. Clin. Transl. Oncol. 2020, 1–13. [Google Scholar] [CrossRef]
- Munteanu, V.C.; Munteanu, R.; Onaciu, A.; Zimta, A.-A.; Petrut, B.; Coman, I. MiRNA-Based Inspired Approach in Diagnosis of Prostate Cancer. Medicina 2020, 56, 94. [Google Scholar] [CrossRef] [Green Version]
- Epstein, J.I.; Egevad, L.; Amin, M.B.; Delahunt, B.; Srigley, J.R.; Humphrey, P.A. The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma. Am. J. Surg. Pathol. 2015, 40, 1. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Ahmed, H.U.; Bosaily, A.E.-S.; Brown, L.C.; Gabe, R.; Kaplan, R.; Parmar, M.K.; Collaco-Moraes, Y.; Ward, K.; Hindley, R.G.; Freeman, A.; et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): A paired validating confirmatory study. Lancet 2017, 389, 815–822. [Google Scholar] [CrossRef] [Green Version]
- Turkbey, B.; Pinto, P.A.; Mani, H.; Bernardo, M.; Pang, Y.; McKinney, Y.L.; Khurana, K.; Ravizzini, G.C.; Albert, P.S.; Merino, M.J.; et al. Prostate Cancer: Value of Multiparametric MR Imaging at 3 T for Detection—Histopathologic Correlation1. Radiology 2010, 255, 89–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasivisvanathan, V.; Rannikko, A.; Borghi, M.; Panebianco, V.; Mynderse, L.A.; Vaarala, M.H.; Briganti, A.; Budäus, L.; Hellawell, G.; Hindley, R.G.; et al. MRI-Targeted or Standard Biopsy for Prostate-Cancer Diagnosis. N. Engl. J. Med. 2018, 378, 1767–1777. [Google Scholar] [CrossRef]
- Van Der Leest, M.; Cornel, E.; Israël, B.; Hendriks, R.; Padhani, A.R.; Hoogenboom, M.; Zamecnik, P.; Bakker, D.; Setiasti, A.Y.; Veltman, J.; et al. Head-to-head Comparison of Transrectal Ultrasound-guided Prostate Biopsy Versus Multiparametric Prostate Resonance Imaging with Subsequent Magnetic Resonance-guided Biopsy in Biopsy-naïve Men with Elevated Prostate-specific Antigen: A Large Prospective Multicenter Clinical Study. Eur. Urol. 2019, 75, 570–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drost, F.-J.H.; Osses, D.F.; Nieboer, D.; Steyerberg, E.W.; Bangma, C.H.; Roobol, M.J.; Schoots, I.G. Prostate MRI, with or without MRI-targeted biopsy, and systematic biopsy for detecting prostate cancer. Cochrane Database Syst. Rev. 2019, 4, CD012663. [Google Scholar] [CrossRef] [PubMed]
- Borkowetz, A.; Platzek, I.; Toma, M.; Renner, T.; Herout, R.; Baunacke, M.; Laniado, M.; Baretton, G.; Froehner, M.; Zastrow, S.; et al. Direct comparison of multiparametric magnetic resonance imaging (MRI) results with final histopathology in patients with proven prostate cancer in MRI/ultrasonography-fusion biopsy. BJU Int. 2016, 118, 213–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, D.C.; Raman, S.S.; Mirak, S.A.; Kwan, L.; Bajgiran, A.M.; Hsu, W.; Maehara, C.K.; Ahuja, P.; Faiena, I.; Pooli, A.; et al. Detection of Individual Prostate Cancer Foci via Multiparametric Magnetic Resonance Imaging. Eur. Urol. 2018, 75, 712–720. [Google Scholar] [CrossRef] [Green Version]
- Borkowetz, A.; Hadaschik, B.; Platzek, I.; Toma, M.; Torsev, G.; Renner, T.; Herout, R.; Baunacke, M.; Laniado, M.; Baretton, G.; et al. Prospective comparison of transperineal magnetic resonance imaging/ultrasonography fusion biopsy and transrectal systematic biopsy in biopsy-naïve patients. BJU Int. 2017, 121, 53–60. [Google Scholar] [CrossRef] [Green Version]
- Filson, C.P.; Natarajan, S.; Margolis, D.J.; Huang, J.; Lieu, P.; Dorey, F.J.; Reiter, R.E.; Marks, L.S. Prostate cancer detection with magnetic resonance-ultrasound fusion biopsy: The role of systematic and targeted biopsies. Cancer 2016, 122, 884–892. [Google Scholar] [CrossRef]
- Salido-Guadarrama, A.I.; Morales-Montor, J.G.; Rangel-Escareño, C.; Langley, E.; Peralta-Zaragoza, O.; Colin, J.L.C.; Rodríguez-Dorantes, M. Urinary microRNA-based signature improves accuracy of detection of clinically relevant prostate cancer within the prostate-specific antigen grey zone. Mol. Med. Rep. 2016, 13, 4549–4560. [Google Scholar] [CrossRef]
- Tao, Z.; Xu, S.; Ruan, H.; Wang, T.; Song, W.; Qian, L.; Chen, K. MiR-195/-16 Family Enhances Radiotherapy via T Cell Activation in the Tumor Microenvironment by Blocking the PD-L1 Immune Checkpoint. Cell. Physiol. Biochem. 2018, 48, 801–814. [Google Scholar] [CrossRef] [PubMed]
- Takeshita, F.; Patrawala, L.; Osaki, M.; Takahashi, R.-U.; Yamamoto, Y.; Kosaka, N.; Kawamata, M.; Kelnar, K.; Bader, A.G.; Brown, D.; et al. Systemic Delivery of Synthetic MicroRNA-16 Inhibits the Growth of Metastatic Prostate Tumors via Downregulation of Multiple Cell-cycle Genes. Mol. Ther. 2010, 18, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Mao, A.; Tang, J.; Zhang, Q.; Yan, J.; Wang, Y.; Di, C.; Gan, L.; Sun, C.; Zhang, H. microRNA-16-5p enhances radiosensitivity through modulating Cyclin D1/E1–pRb–E2F1 pathway in prostate cancer cells. J. Cell. Physiol. 2018, 234, 13182–13190. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Wang, M.; Liu, X. MicroRNA-195 suppresses tumor cell proliferation and metastasis by directly targeting BCOX1 in prostate carcinoma. J. Exp. Clin. Cancer Res. 2015, 34, 91. [Google Scholar] [CrossRef] [Green Version]
- Cai, C.; Chen, Q.-B.; Han, Z.-D.; Zhang, Y.-Q.; He, H.-C.; Chen, J.-H.; Chen, Y.-R.; Yang, S.-B.; Wu, Y.-D.; Zeng, Y.-R.; et al. miR-195 Inhibits Tumor Progression by Targeting RPS6KB1 in Human Prostate Cancer. Clin. Cancer Res. 2015, 21, 4922–4934. [Google Scholar] [CrossRef] [Green Version]
- Foj, L.; Ferrer, F.; Serra, M.; Arévalo, A.; Gavagnach, M.; Giménez, N.; Filella, X. Exosomal and Non-Exosomal Urinary miRNAs in Prostate Cancer Detection and Prognosis. Prostate 2016, 77, 573–583. [Google Scholar] [CrossRef]
- Stephan, C.; Jung, M.; Rabenhorst, S.; Kilic, E.; Jung, K. Urinary miR-183 and miR-205 do not surpass PCA3 in urine as predictive markers for prostate biopsy outcome despite their highly dysregulated expression in prostate cancer tissue. Clin. Chem. Lab. Med. 2015, 53, 1109–1118. [Google Scholar] [CrossRef]
- Casanova-Salas, I.; Rubio-Briones, J.; Calatrava, A.; Mancarella, C.; Masiá, E.; Casanova, J.; Fernandez-Serra, A.; Rubio, L.; Ramírez-Backhaus, M.; Armiñán, A.; et al. Identification of miR-187 and miR-182 as Biomarkers of Early Diagnosis and Prognosis in Patients with Prostate Cancer Treated with Radical Prostatectomy. J. Urol. 2014, 192, 252–259. [Google Scholar] [CrossRef]
- Nayak, B.; Khan, N.; Garg, H.; Rustagi, Y.; Singh, P.; Seth, A.; Dinda, A.K.; Kaushal, S. Role of miRNA-182 and miRNA-187 as potential biomarkers in prostate cancer and its correlation with the staging of prostate cancer. Int. Braz. J. Urol. 2020, 46, 614–623. [Google Scholar] [CrossRef]
- Bryant, R.J.; Pawlowski, T.; Catto, J.W.; Marsden, G.; Vessella, R.L.; Rhees, B.; Kuslich, C.; Visakorpi, T.; Hamdy, F.C. Changes in circulating microRNA levels associated with prostate cancer. Br. J. Cancer 2012, 106, 768–774. [Google Scholar] [CrossRef] [Green Version]
- Stuopelyte, K.; Daniūnaitė, K.; Bakavicius, A.; Lazutka, J.R.; Jankevicius, F.; Jarmalaitė, S. The utility of urine-circulating miRNAs for detection of prostate cancer. Br. J. Cancer 2016, 115, 707–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stuopelytė, K.; Daniūnaitė, K.; Jankevicius, F.; Jarmalaitė, S. Detection of miRNAs in urine of prostate cancer patients. Medicina 2016, 52, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Xie, X.; Dai, J.; Huang, X.; Fang, C.; He, W. MicroRNA-145 inhibits proliferation and induces apoptosis in human prostate carcinoma by upregulating long non-coding RNA GAS5. Oncol. Lett. 2019, 18, 1043–1048. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, J.-H.; Han, Z.-P.; Zou, M.-X.; He, M.-L.; Li, Y.-G.; Zheng, L. CDX2/mir-145-5p/SENP1 Pathways Affect LNCaP Cells Invasion and Migration. Front. Oncol. 2019, 9, 477. [Google Scholar] [CrossRef] [PubMed]
- Erdmann, K.; Kaulke, K.; Rieger, C.; Salomo, K.; Wirth, M.P.; Fuessel, S. MiR-26a and miR-138 block the G1/S transition by targeting the cell cycle regulating network in prostate cancer cells. J. Cancer Res. Clin. Oncol. 2016, 142, 2249–2261. [Google Scholar] [CrossRef]
- Leite, K.R.M.; Reis, S.T.; Viana, N.; Morais, D.R.; Moura, C.M.; Silva, I.A.; Pontes, J.; Katz, B.; Srougi, M. Controlling RECK miR21 Promotes Tumor Cell Invasion and Is Related to Biochemical Recurrence in Prostate Cancer. J. Cancer 2015, 6, 292–301. [Google Scholar] [CrossRef] [Green Version]
- Li, T.; Li, R.-S.; Li, Y.-H.; Zhong, S.; Chen, Y.-Y.; Zhang, C.-M.; Hu, M.-M.; Shen, Z.-J. miR-21 as an Independent Biochemical Recurrence Predictor and Potential Therapeutic Target for Prostate Cancer. J. Urol. 2012, 187, 1466–1472. [Google Scholar] [CrossRef]
- Guan, Y.; Wu, Y.; Liu, Y.; Ni, J.; Nong, S. Association of microRNA-21 expression with clinicopathological characteristics and the risk of progression in advanced prostate cancer patients receiving androgen deprivation therapy. Prostate 2016, 76, 986–993. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Total Cohort | Tf Group | PCa Group | p Value PCa vs. Tf |
|---|---|---|---|---|
| Number of Patients | n = 50 | n = 24 | n = 26 | NA |
| Median Age (Years) (Range) | 69.1 (46.8–81.0) | 67.4 (46.8–79.4) | 71.5 (50.8–81.0) | 0.428 |
| Median PSA Level (ng/mL) (Range) | 7.90 (1.69–50.26) | 7.95 (1.81–15.54) | 7.86 (1.69–50.26) | 0.714 |
| PSA Level ≤ 10 ng/mL | n = 34 | n = 19 | n = 15 | NA |
| Median PSAD (ng/mL2) (Range) | 0.15 (0.03–1.24) | 0.12 (0.05–0.34) | 0.19 (0.03–1.24) | 0.060 |
| Pre-Biopsy DRE Status Negative Positive | n = 32 (64%) n = 18 (36%) | n = 19 (79.2%) n = 5 (20.8%) | n = 13 (50%) n = 13 (50%) | 0.093 |
| T Stage cT1 cT2 cT3 cT4 | NA | NA | n = 20 (76.9%) n = 5 (19.2%) n = 0 (0%) n = 1 (3.8%) | NA |
| N Stage cN0 cN1 Unknown | NA | NA | n = 24 (92.3%) n = 1 (3.8%) n = 1 (3.8%) | NA |
| M Stage cM0 cM1 | NA | NA | n = 24 (92.3%) n = 2 (7.7%) | NA |
| Gleason Grade Group 1 (GS ≤ 6) 2 (GS = 3 + 4) 3 (GS = 4 + 3) 4 (GS = 8) 5 (GS = 9–10) | NA | NA | n = 7 (26.9%) n = 9 (34.6%) n = 5 (19.2%) n = 0 (0%) n = 5 (19.2%) | NA |
| miRNA | Median Relative Expression Level (× 10−3) | Fold Change PCa vs. Tf | p Value | |
|---|---|---|---|---|
| in Tf | in PCa | |||
| miR-125b | 32.86 | 30.96 | 0.94 | 0.875 |
| miR-145 | 17.03 | 10.14 | 0.60 | 0.093 |
| miR-155 | 17.45 | 21.47 | 1.23 | 0.992 |
| miR-16 | 659.40 | 373.55 | 0.57 | 0.040 |
| miR-195 | 231.38 | 141.14 | 0.61 | 0.040 |
| miR-200c | 689.41 | 745.59 | 1.08 | 0.848 |
| miR-205 | 36.91 | 47.88 | 1.30 | 0.875 |
| miR-21 | 579.42 | 383.47 | 0.66 | 0.282 |
| miR-218 | 2.10 | 1.86 | 0.89 | 0.875 |
| miR-26a | 304.50 | 169.37 | 0.56 | 0.093 |
| miR-375 | 45.93 | 55.49 | 1.21 | 0.944 |
| miR-96 | 0.28 | 0.16 | 0.59 | 0.365 |
| Parameter | PSAD | miR-16 | miR-195 | miR-16/PSAD | miR-195/PSAD | miR-16/miR-195 | miR-16/miR-195/PSAD |
|---|---|---|---|---|---|---|---|
| AUC (95% CI) | 0.708 (0.562–0.853) | 0.744 (0.599–0.888) | 0.729 (0.587–0.871) | 0.834 (0.721–0.947) | 0.801 (0.679–0.924) | 0.772 (0.637–0.906) | 0.849 (0.741–0.957) |
| p value | 0.031 | 0.012 | 0.017 | < 0.001 | 0.002 | 0.005 | < 0.001 |
| Cutoff | > 0.15 1 | < 0.403 | < 0.162 | 1 of 2 | 1 of 2 | 1 of 2 | 2 of 3 |
| SNS | 69.2% | 65.4% | 61.5% | 92.3% | 92.3% | 73.1% | 65.4% |
| SPC | 70.8% | 87.5% | 79.2% | 87.5% | 83.3% | 79.2% | 87.5% |
| PPV | 72.0% | 85.0% | 76.2% | 88.9% | 85.7% | 79.2% | 85.0% |
| NPV | 68.0% | 70.0% | 65.5% | 91.3% | 90.9% | 73.1% | 70.0% |
| pLR | 2.374 | 5.231 | 2.954 | 7.385 | 5.538 | 3.508 | 5.231 |
| nLR | 0.434 | 0.396 | 0.486 | 0.088 | 0.092 | 0.340 | 0.396 |
| ACC | 70.0% | 76.0% | 70.0% | 90.0% | 88.0% | 76.0% | 76.0% |
| Ranking | 4. | 3. | 4. | 1. | 2. | 3. | 3. |
| Parameter | PSAD | miR-16 | miR-195 | miR-16/PSAD | miR-195/PSAD | miR-16/miR-195 | miR-16/miR-195/PSAD |
|---|---|---|---|---|---|---|---|
| AUC (95% CI) | 0.595 (0.394–0.795) | 0.818 (0.659–0.976) | 0.772 (0.614–0.930) | 0.854 (0.721–0.988) | 0.798 (0.646–0.951) | 0.846 (0.704–0.987) | 0.882 (0.764–1.000) |
| p value | 0.524 | 0.008 | 0.022 | 0.004 | 0.012 | 0.004 | 0.004 |
| Cutoff | >0.15 1 | <0.403 | <0.162 | 1 of 2 | 1 of 2 | 1 of 2 | 2 of 3 |
| SNS | 46.7% | 80.0% | 66.7% | 86.7% | 86.7% | 86.7% | 73.3% |
| SPC | 84.2% | 89.5% | 78.9% | 73.7% | 63.2% | 78.9% | 89.5% |
| PPV | 70.0% | 85.7% | 71.4% | 72.2% | 65.0% | 76.5% | 84.6% |
| NPV | 66.7% | 85.0% | 75.0% | 87.5% | 85.7% | 88.2% | 81.0% |
| pLR | 2.956 | 7.600 | 3.167 | 3.293 | 2.352 | 4.117 | 6.967 |
| nLR | 0.633 | 0.224 | 0.422 | 0.181 | 0.211 | 0.169 | 0.298 |
| ACC | 67.6% | 85.3% | 73.5% | 79.4% | 73.5% | 82.4% | 82.4% |
| Ranking | 5. | 1. | 4. | 3. | 4. | 2. | 2. |
| Study | Urine Collection | PCa Group | Tf Group | miRNA | Diagnostic Potential 1 |
|---|---|---|---|---|---|
| Present Work | post-DRE pre-biopsy | 26 PCa biopsy | 24 Tf biopsy | miR-16 miR-195 | yes yes |
| Foj 2017 [36] | post-DRE pre-biopsy (just PCa group) | 60 PCa biopsy | 10 healthy men | let-7c miR-21 miR-141 miR-214 miR-375 miR-21/375 | no yes yes yes yes yes |
| Salido-Guadarrama 2016 [30] | post-DRE pre-biopsy | 73 PCa biopsy (GS ≥ 7) | 70 Tf biopsy | miR-100/200b | yes |
| Stephan 2015 [37] | post-DRE pre-biopsy | 38 PCa biopsy | 38 Tf biopsy | miR-183 miR-205 | no no |
| Casanova-Salas 2014 [38] | post-DRE pre-biopsy | 47 PCa biopsy | 45 Tf biopsy | miR-182 miR-187 | no yes |
| Nayak 2020 [39] | post-DRE pre-biopsy | 33 PCa biopsy | 30 Tf biopsy | miR-182 miR-187 | not evaluated |
| Bryant 2012 [40] | post-DRE post-biopsy | 118 PCa biopsy | 17 Tf biopsy | miR-107 miR-574-3p | yes yes |
| Stuopelytė 2016 [42] | post-biopsy & pre-RPE | 143 PCa RPE | 23 BPH RPE | miR-21 miR-21/19a/19b | yes yes |
| Stuopelytė 2016 [41] | post-biopsy & pre-RPE (except healthy men) | (a) 143 PCa RPE (b) 72 PCa RPE | (a) 23 BPH RPE (b) 62 healthy men | miR-148a miR-375 miR-148a/375 | yes yes yes |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borkowetz, A.; Lohse-Fischer, A.; Scholze, J.; Lotzkat, U.; Thomas, C.; Wirth, M.P.; Fuessel, S.; Erdmann, K. Evaluation of MicroRNAs as Non-Invasive Diagnostic Markers in Urinary Cells from Patients with Suspected Prostate Cancer. Diagnostics 2020, 10, 578. https://doi.org/10.3390/diagnostics10080578
Borkowetz A, Lohse-Fischer A, Scholze J, Lotzkat U, Thomas C, Wirth MP, Fuessel S, Erdmann K. Evaluation of MicroRNAs as Non-Invasive Diagnostic Markers in Urinary Cells from Patients with Suspected Prostate Cancer. Diagnostics. 2020; 10(8):578. https://doi.org/10.3390/diagnostics10080578
Chicago/Turabian StyleBorkowetz, Angelika, Andrea Lohse-Fischer, Jana Scholze, Ulrike Lotzkat, Christian Thomas, Manfred P. Wirth, Susanne Fuessel, and Kati Erdmann. 2020. "Evaluation of MicroRNAs as Non-Invasive Diagnostic Markers in Urinary Cells from Patients with Suspected Prostate Cancer" Diagnostics 10, no. 8: 578. https://doi.org/10.3390/diagnostics10080578