Melanoma Diagnosis Using Deep Learning and Fuzzy Logic


Abstract
:1. Introduction
2. Preliminaries
2.1. Definition of Interval Number
Lemma
2.2. Definition of Fuzzy Set
2.3. Definition of Fuzzy Number
- is normal. That is, exists such that .
- .
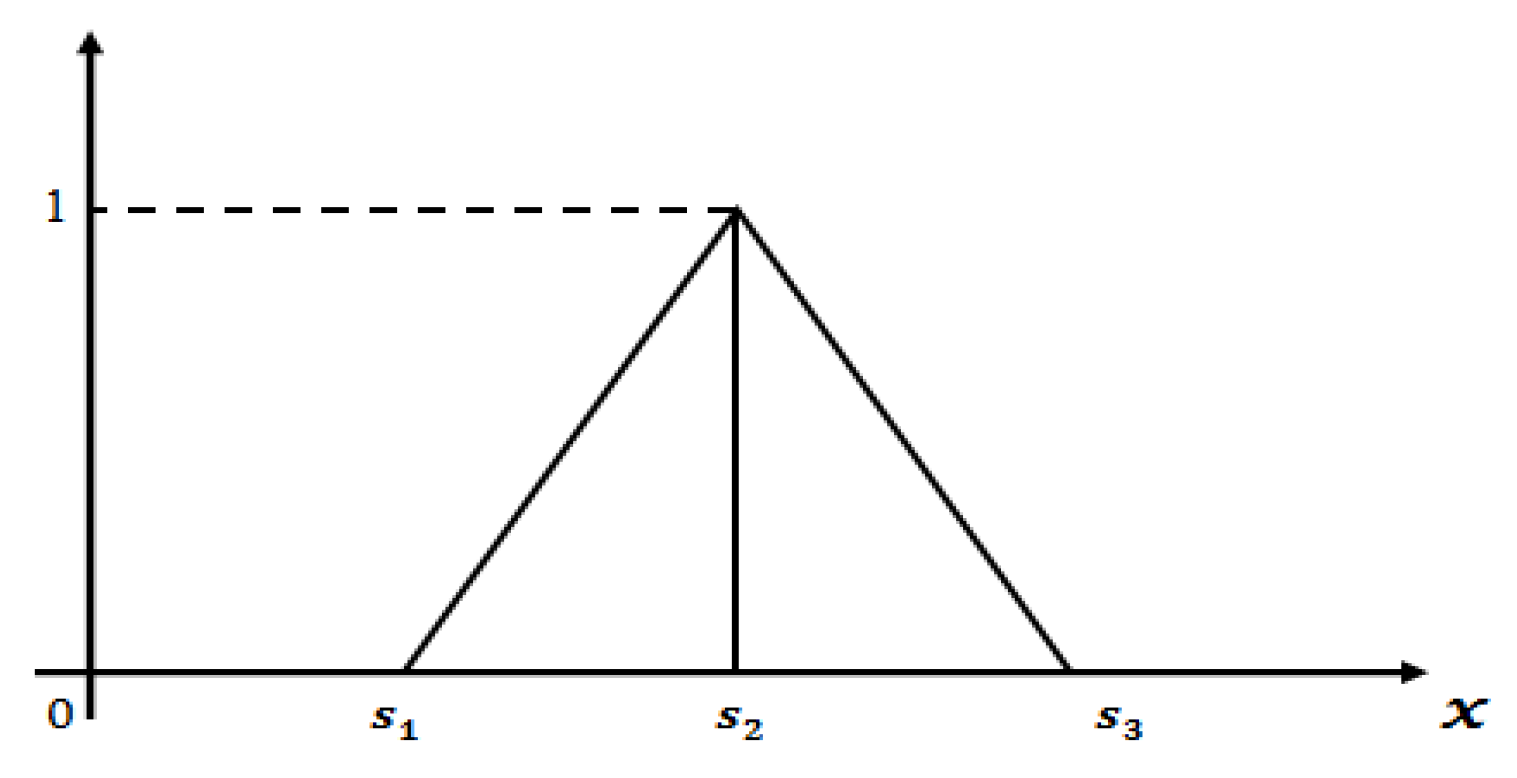
2.4. Definition of Triangular Fuzzy Number
- is a continuous function which is in the interval [0,1].
- is a strictly increasing and continuous function on the interval .
- is a strictly decreasing and continuous function on the interval .
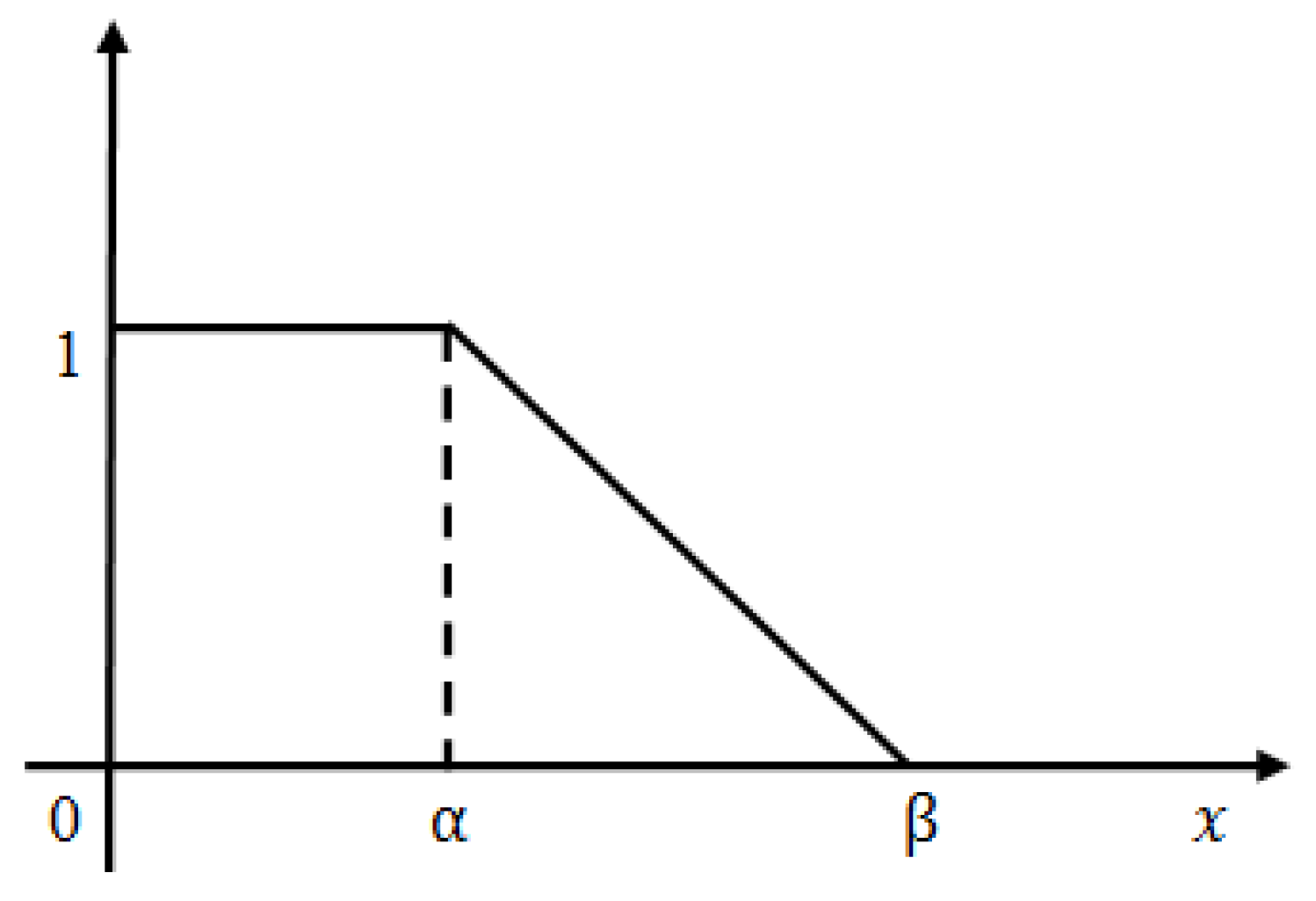
2.5. Definition of Linear Triangular Fuzzy Number (TFN)
2.6. Definition of -cut Form of Linear TFN
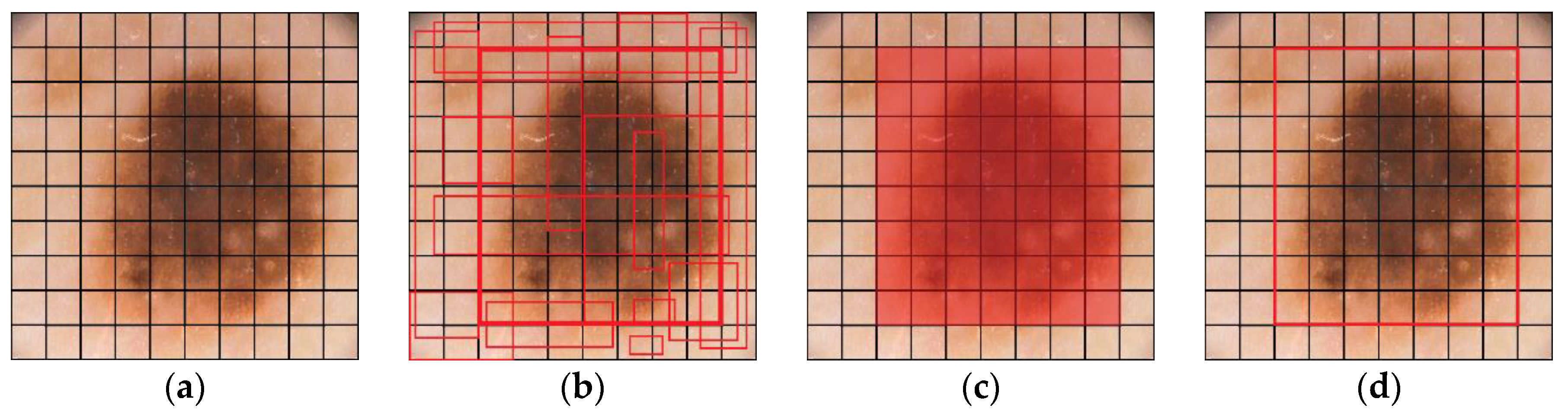
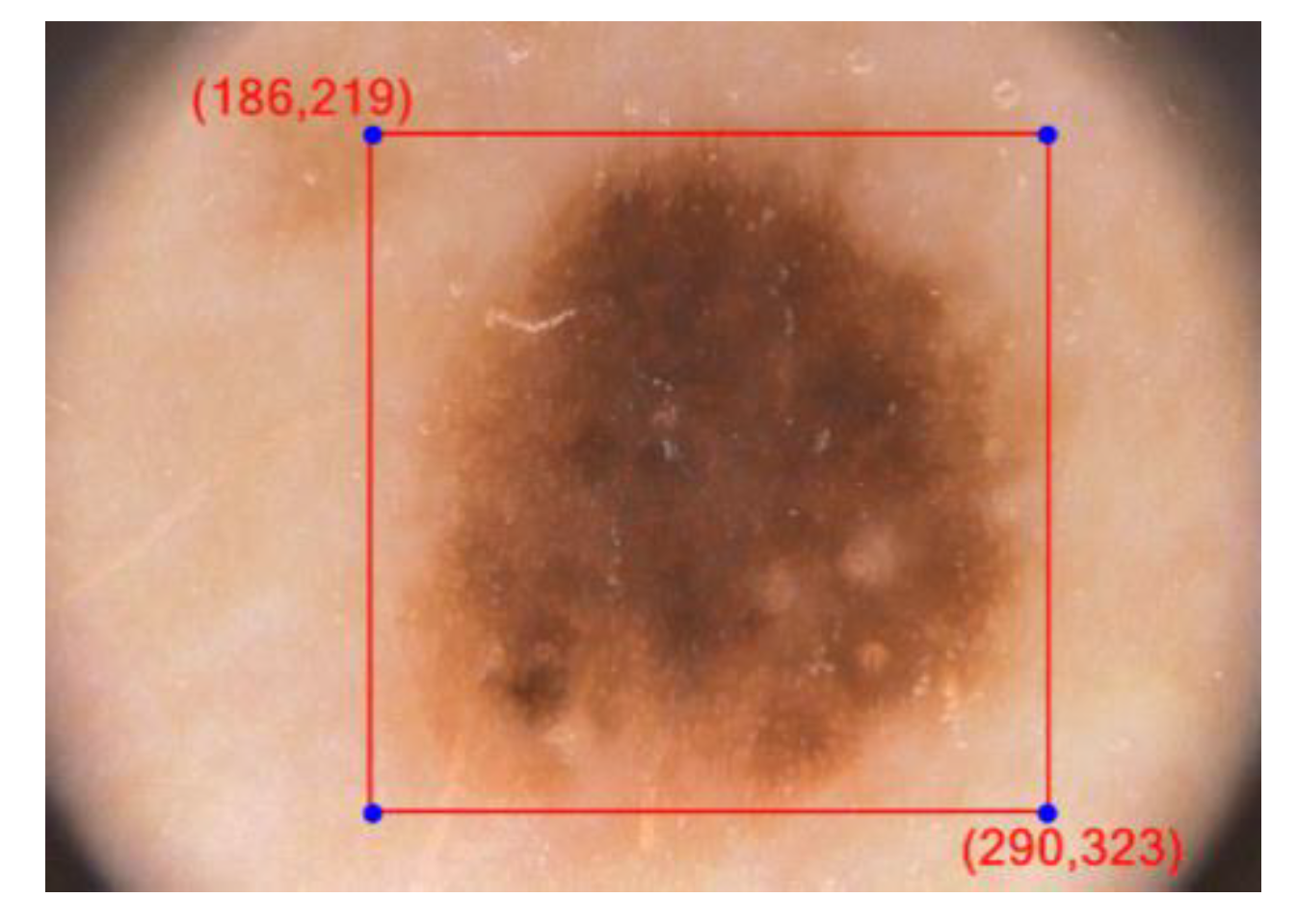
3. Implementation of YOLOv3 Classifier
4. Proposed Methodology
4.1. Training YOLOv3 with PH2, ISBI 2017 and ISIC 2019 Dataset
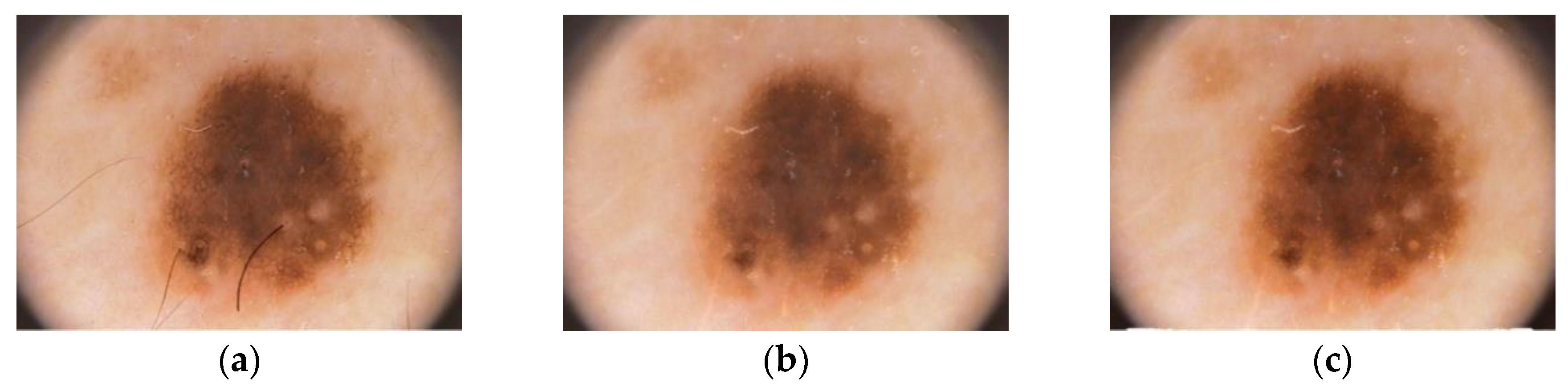
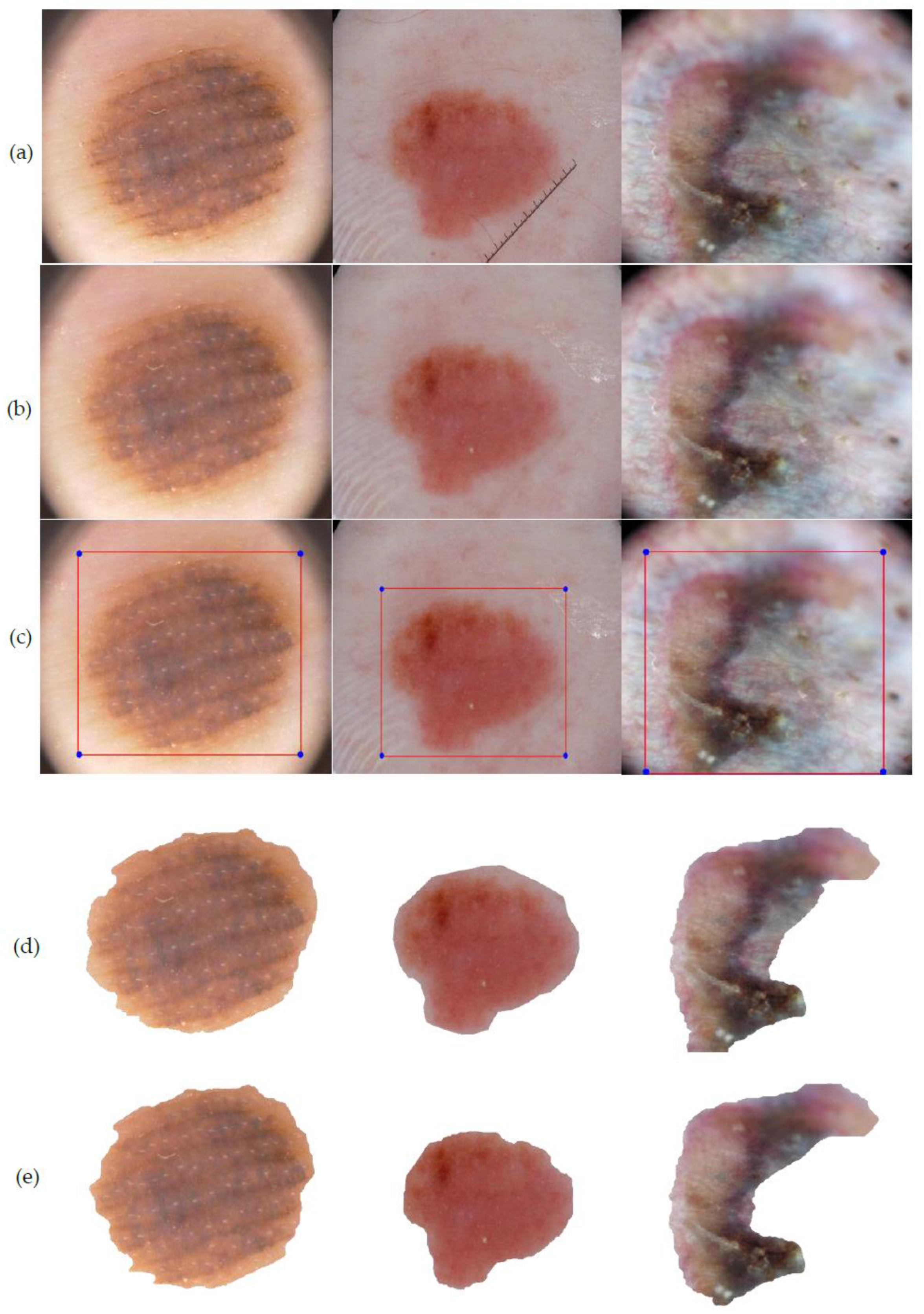
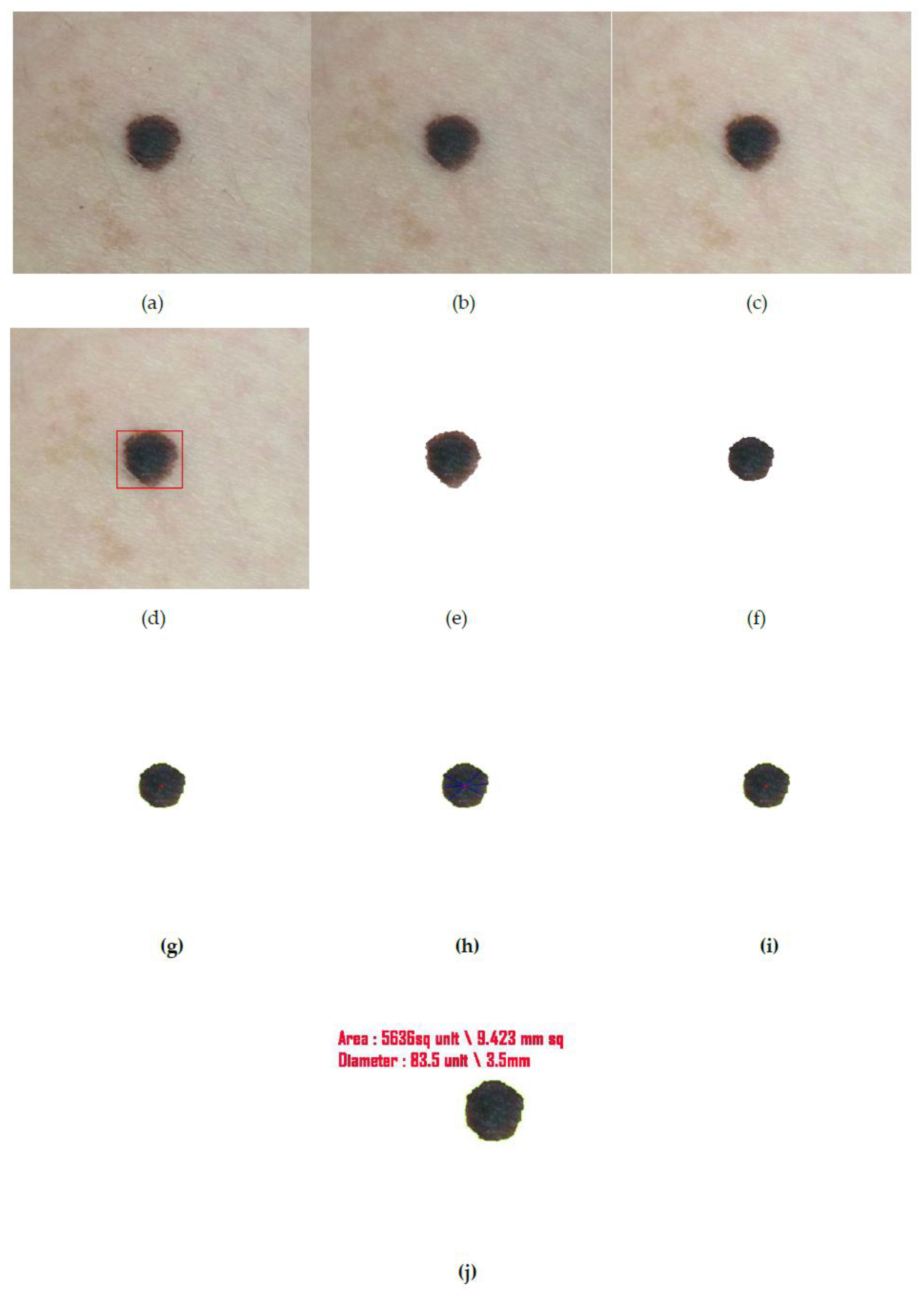
4.2. Pre-Processing
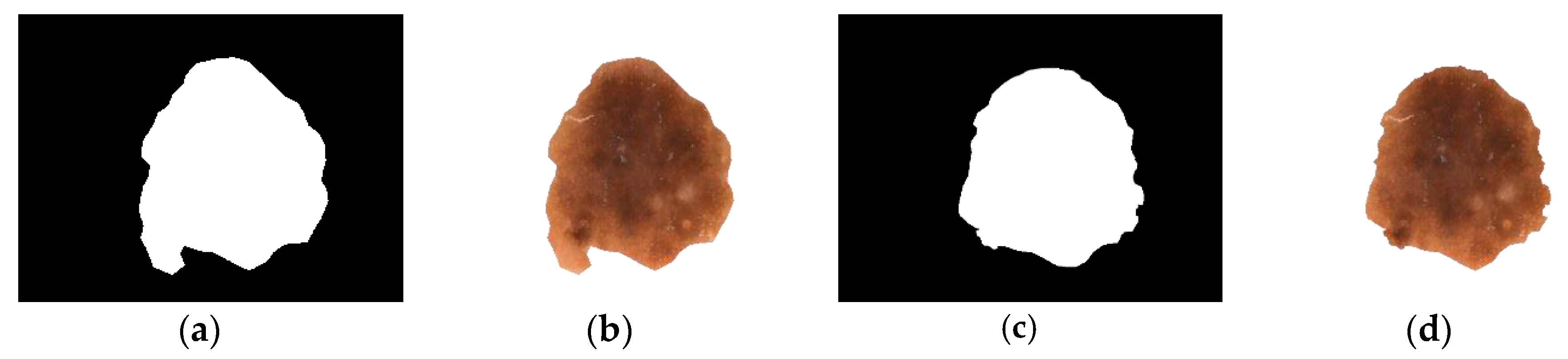
4.3. Segmentation
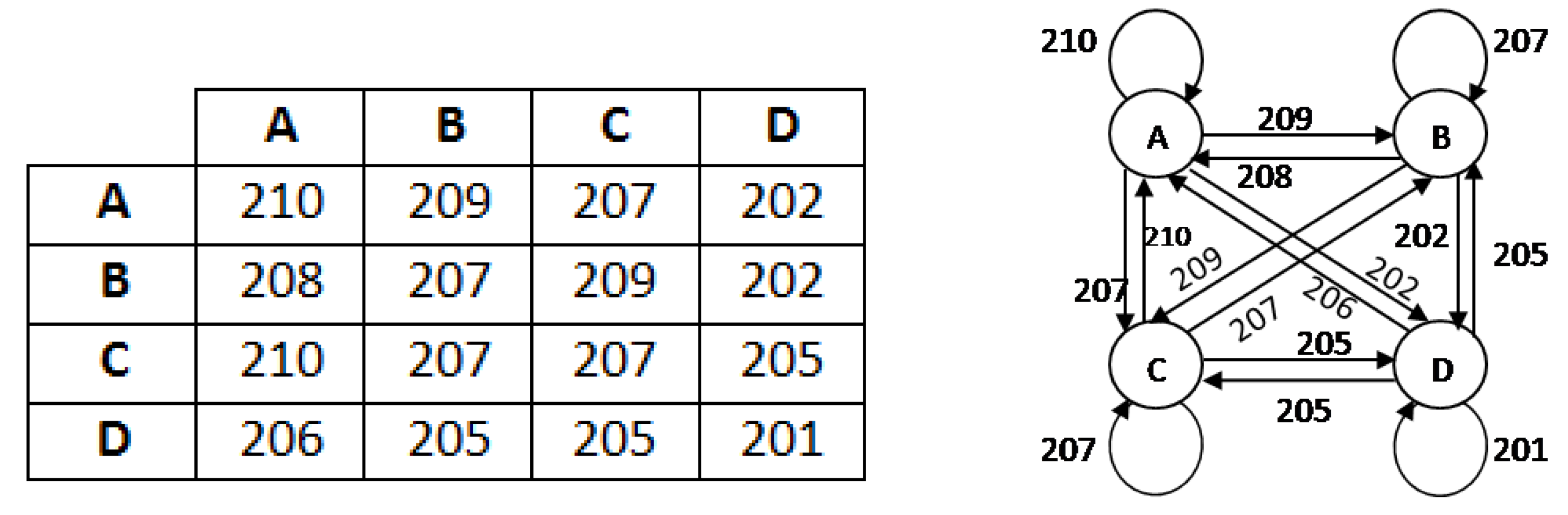
4.3.1. Iteration-I
- Construct an adjacent matrix.
- Discard all self loops from the graph and take one minimum edge in place of multi edge expressions.
- Find one minimum weight from the 1st row and place one connection. In case of a tie, take any one connection arbitrarily.
- Find one minimum weight from 1st and previously selected vertex row and add it into one. In case of a tie take any one connection arbitrarily, ensuring that it will not form any circuit.
- Continue this process until all the vertices are covered but does not form any circuit such that it will generate a spanning tree.
- Then calculate weight
4.3.2. Iteration-II
- A fuzzy number is said to be an L-R type fuzzy number if and only ifwhere, L is for left and R for right reference. M is the mean value of . are called left and right spreads, respectively.
- A fuzzy number is said to be an L-type fuzzy number if and only if
4.4. Feature Extraction
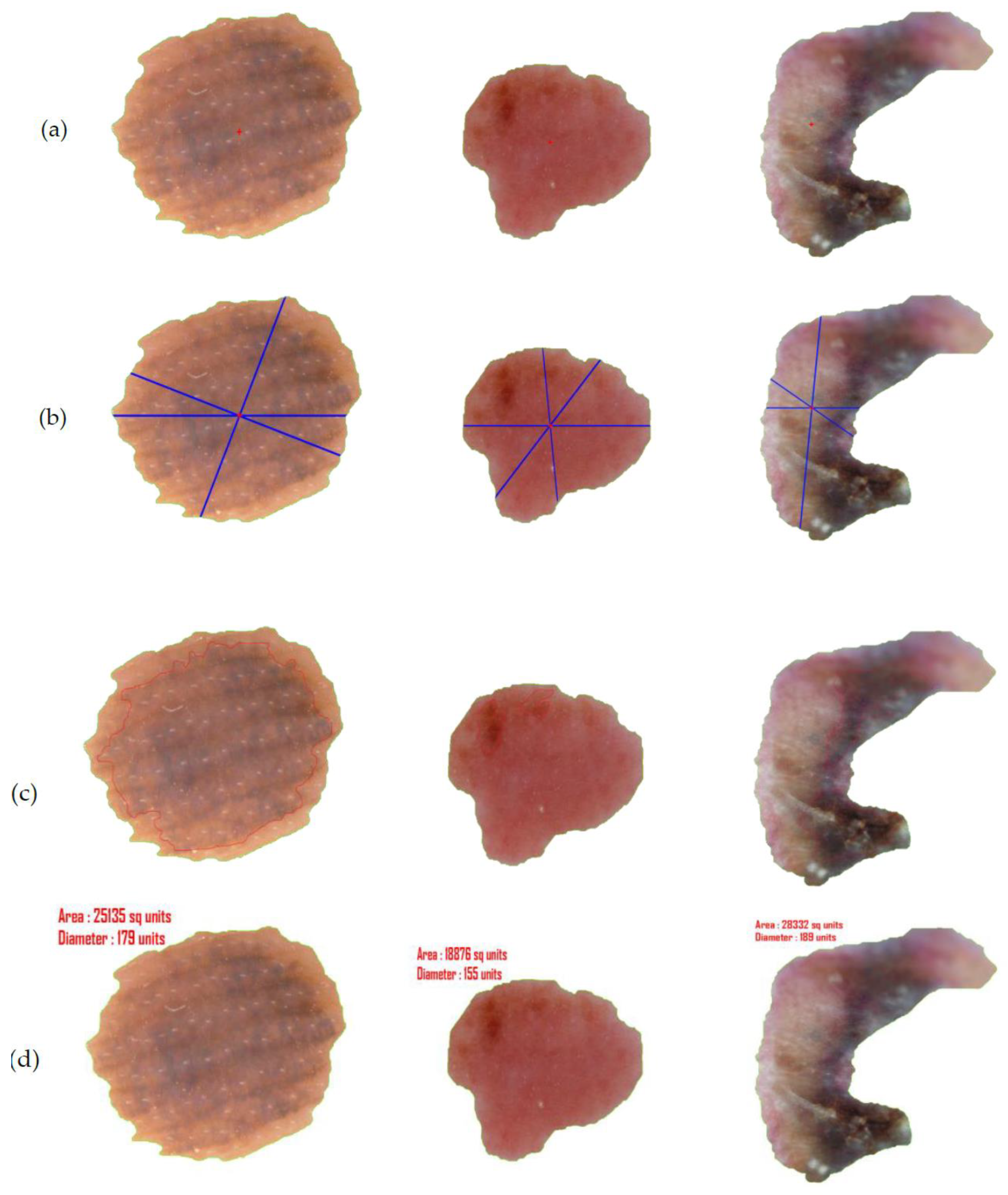
4.4.1. Asymmetry and Border
4.4.2. Color
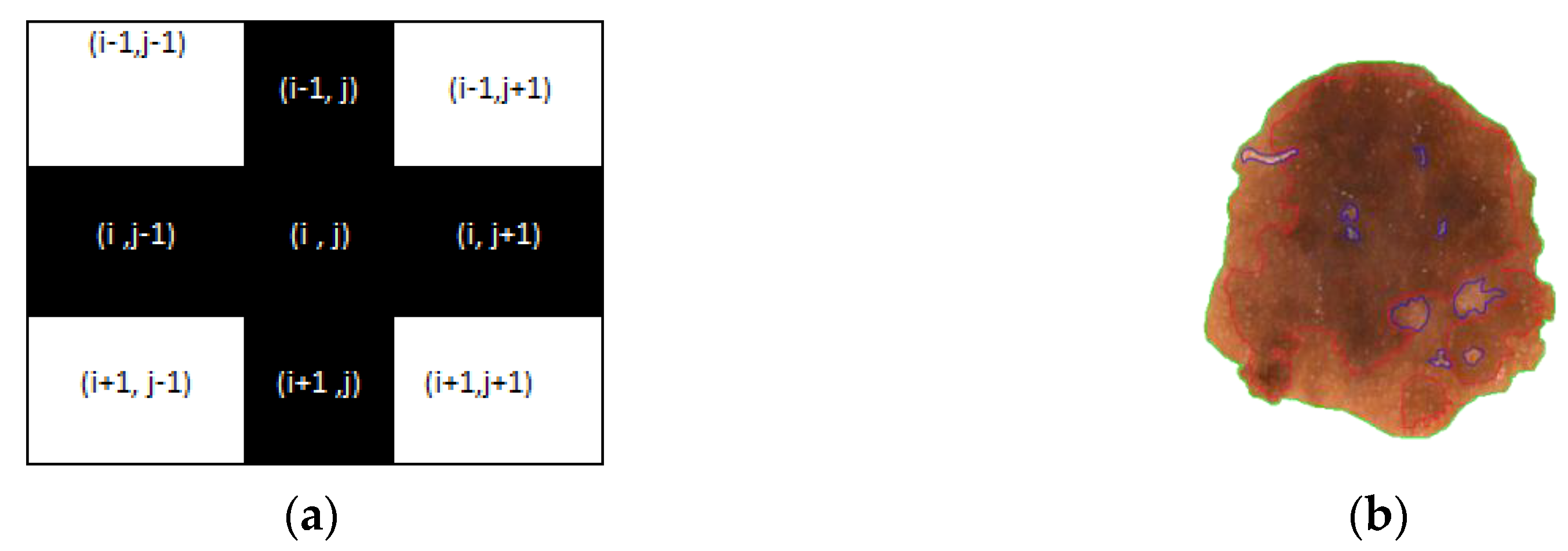
- Calculate the shape (M × N) of the segmented image X1 and every pixel is checked. Simultaneously an image F1 (M × N) is generated where is considered a pixel value at the location (i,j).
- Extra border padding in plotting matrix F1, for calculation.
- Calculate RGB value of each pixel and convert it to corresponding HSV
- if HSV value of ranges from 30,62,77 to 30,68,57 then = 1 // for light brown
- if HSV value of ranges from 30,67,51 to 30,67,28 then = 2 // for dark brown
- if HSV value of ranges from 30,67,22 to 30,67,11 then = 3 // for tan black
- if HSV value of ranges from 60,2,17 to 30,0,10 then = 4 // for blue gray
- if HSV value of ranges from 0,100,46 to 0,87,70 then = 5 // for red
- if HSV value of ranges from 0,0,94 to 0,0,98 then = 6 // for white
- if > 0 and lies in the border line then plot that pixel with color according to clusters.
- else if ( ) then continue // plus (+) operation (see Figure 11a).
- else plotting the pixel with different colors for different clusters as per Figure 11b.
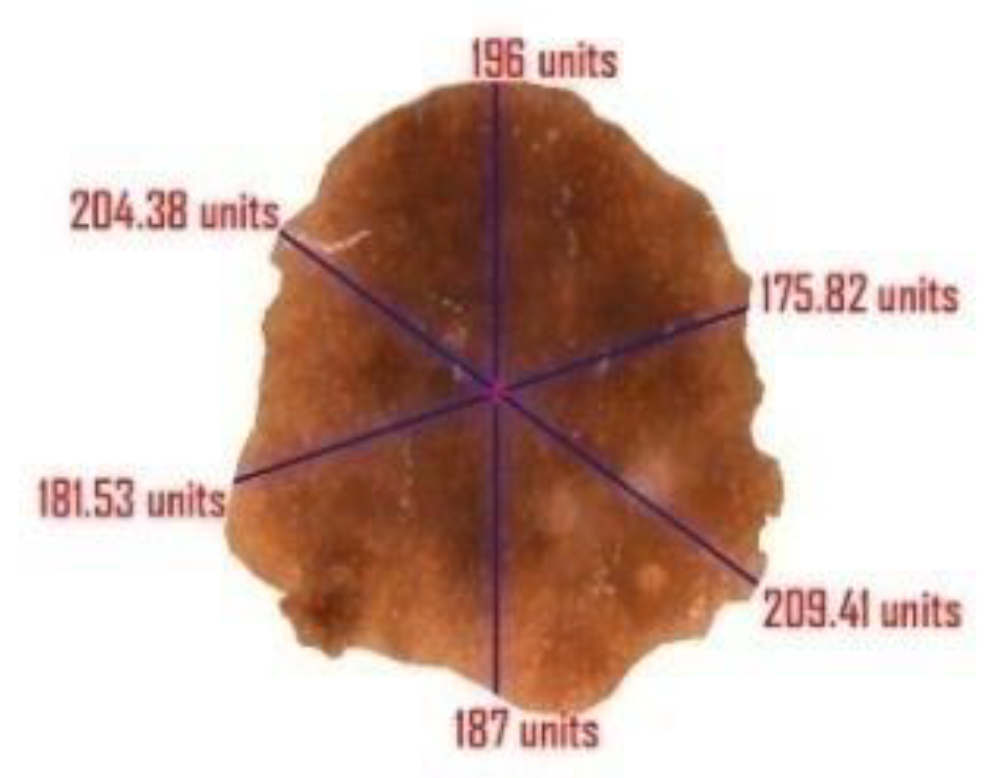
4.4.3. Diameter
5. Parameters for Performance Evaluation
6. Result Analysis
7. Discussion
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Feng, J.; Isern, N.G.; Burton, S.D.; Hu, J.Z. Studies of secondary melanoma on C57BL/6J mouse liver using 1H NMR metabolomics. Metabolites 2013, 3, 1011–1035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abuzaghleh, O.; Faezipour, M.; Barkana, B.D. SKINcure: An Innovative Smartphone-Based Application to Assist in Melanoma Early Detection and Prevention. Signal Image Process. Int. J. 2014, 15, 1–13. [Google Scholar] [CrossRef]
- Orazio, D.J.; Jarrett, S.; Amaro-Ortiz, A.; Scott, T. UV Radiation and the Skin. Int. J. Mol. Sci. 2013, 14, 12222–12248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karimkhani, C.; Green, A.; Nijsten, T.; Weinstock, M.; Dellavalle, R.; Naghavi, M.; Fitzmaurice, C. The global burden of melanoma: Results from the Global Burden of Disease Study 2015. Br. J. Dermatol. 2017, 177, 134–140. [Google Scholar] [CrossRef]
- Gandhi, S.A.; Kampp, J. Skin Cancer Epidemiology, Detection, and Management. Med. Clin. N. Am. 2015, 99, 1323–1335. [Google Scholar] [CrossRef]
- Giotis, I.; Molders, N.; Land, S.; Biehl, M.; Jonkman, M.F.; Petkov, N. MED-NODE: A computer-assisted melanoma diagnosis system using non-dermoscopic images. Expert Syst. Appl. 2015, 42, 6578–6585. [Google Scholar] [CrossRef]
- Abbas, Q.; Celebi, M.E.; García, I.F. Hair removal methods: A comparative study for dermoscopy images. Biomed. Signal Process. Control 2011, 6, 395–404. [Google Scholar] [CrossRef]
- Jemal, A.; Siegel, R.; Ward, E.; Hao, Y.; Xu, J.; Thun, M.J. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar]
- Mayer, J.E.; Swetter, S.M.; Fu, T.; Geller, A.C. Screening, early detection, education, and trends for melanoma: Current status (2007–2013) and future directions Part II. Screening, education, and future directions. J. Am. Acad. Dermatol. 2014, 71, e1–e611. [Google Scholar]
- Rigel, D.S.; Russak, J.; Friedman, R. The evolution of melanoma diagnosis: 25 years beyond the ABCDs. CA Cancer J. Clin. 2010, 60, 301–316. [Google Scholar] [CrossRef]
- Lodha, S.; Saggar, S.; Celebi, J.T.; Silvers, D.N. Discordance in the histopathologic diagnosis of difficult melanocytic neoplasms in the clinical setting. J. Cutan. Pathol. 2008, 35, 349–352. [Google Scholar] [CrossRef]
- Brochez, L.; Verhaeghe, E.; Grosshans, E. Inter-observer variation in the histopathological diagnosis of clinically suspicious pigmented skin lesions. J. Pathol. 2002, 196, 459–466. [Google Scholar] [CrossRef]
- Dadzie, O.E.; Goerig, J.; Bhawan, J. Incidental microscopic foci of nevic aggregates in skin. Am. J. Dermatopathol. 2008, 30, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Togawa, Y. Dermoscopy for the Diagnosis of Melanoma: An Overview. Austin J. Dermatol. 2017, 4, 1080. [Google Scholar]
- Kroemer, S.; Frühauf, J.; Campbell, T.M.; Massone, C.; Schwantzer, G.; Soyer, H.P.; Hofmann-Wellenhof, R. Mobile teledermatology for skin tumour screening: Diagnostic accuracy of clinical and dermoscopic image tele-evaluation using cellular phones. Br. J. Dermatol. 2011, 164, 973–979. [Google Scholar] [CrossRef]
- Harrington, E.; Clyne, B.; Wesseling, N.; Sandhu, H.; Armstrong, L.; Bennett, H.; Fahey, T. Diagnosing malignant melanoma in ambulatory care: A systematic review of clinical prediction rules. BMJ Open 2017, 7, e014096. [Google Scholar] [CrossRef]
- Robinson, J.K.; Turrisi, R. Skills training to learn discrimination of ABCDE criteria by those at risk of developing melanoma. Arch. Dermatol. 2006, 142, 447–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karargyris, A.; Karargyris, O.; Pantelopoulos, A. DERMA/Care: An advanced image-processing mobile application for monitoring skin cancer. In Proceedings of the 24th International Conference on Tools with Artificial Intelligence, Athens, Greece, 7–9 November 2012; Volume 2, pp. 1–7. [Google Scholar]
- Do, T.T.; Zhou, Y.; Zheng, H.; Cheung, N.M.; Koh, D. Early melanoma diagnosis with mobile imaging. In Proceedings of the 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; pp. 6752–6757. [Google Scholar]
- Yen, K.K.; Ghoshray, S.; Roig, G. A linear regression model using triangular fuzzy number coefficients. Fuzzy Sets Syst. 1999, 106, 166–167. [Google Scholar] [CrossRef]
- Chakraborty, A.; Mondal, S.P.; Ahmadian, A.; Senu, N.; Dey, D.; Alam, S.; Salahshour, S. The Pentagonal Fuzzy Number: Its Different Representations, Properties, Ranking, Defuzzification and Application in Game Problem. Symmetry 2019, 11, 248. [Google Scholar] [CrossRef] [Green Version]
- Chakraborty, A.; Maity, S.; Jain, S.; Mondal, S.P.; Alam, S. Hexagonal Fuzzy Number and its Distinctive Representation, Ranking, Defuzzification Technique and Application in Production Inventory Management Problem. Granul. Comput. 2020. [Google Scholar] [CrossRef]
- Atanassov, K. Intuitionistic fuzzy sets. Fuzzy Sets Syst. 1986, 20, 87–96. [Google Scholar] [CrossRef]
- Chakraborty, A.; Mondal, S.P.; Ahmadian, A.; Senu, N.; Alam, S.; Salahshour, S. Different Forms of Triangular Neutrosophic Numbers, De-Neutrosophication Techniques, and their Applications. Symmetry 2018, 10, 327. [Google Scholar] [CrossRef] [Green Version]
- Chakraborty, A.; Mondal, S.; Broumi, S. De-neutrosophication technique of pentagonal neutrosophic number and application in minimal spanning tree. Neutrosophic Sets Syst. 2019, 29, 1–18. [Google Scholar]
- Chakraborty, A. A New Score Function of Pentagonal Neutrosophic Number and its Application in Networking Problem. Int. J. NeutrosophicSci. 2020, 1, 35–46. [Google Scholar]
- Mahata, A.; Mondal, S.P.; Alam, S.; Chakraborty, A.; Goswami, A.; Dey, S. Mathematical model for diabetes in fuzzy environment and stability analysis. J. Intell. Fuzzy Syst. 2018, 36, 2923–2932. [Google Scholar] [CrossRef]
- Redmon, J.; Farhadi, A. Yolov3: An incremental improvement. arXiv 2018, arXiv:1804.02767. [Google Scholar]
- Andreas, B.; Giacomel, J. Tape dermatoscopy: Constructing a low-cost dermatoscope using a mobile phone, immersion fluid and transparent adhesive tape. Derm. Pr. Concept 2015, 5, 87–93. [Google Scholar]
- Ganster, H.; Pinz, P.; Rohrer, R.; Wildling, E.; Binder, M.; Kittler, H. Automated melanoma recognition. IEEE Trans. Med. Imaging 2001, 20, 233–239. [Google Scholar] [CrossRef]
- Celebi, M.E.; Iyatomi, H.; Schaefer, G.; Stoecker, W.V. Lesion border detection in dermoscopy images. Comput. Med. Imaging Graph. 2009, 33, 148–153. [Google Scholar] [CrossRef] [Green Version]
- Korotkov, K.; Garcia, R. Computerized analysis of pigmented skin lesions: A review. Artif. Intell. Med. 2012, 56, 69–90. [Google Scholar] [CrossRef]
- Filho, M.; Ma, Z.; Tavares, J.M.R.S. A Review of the Quantification and Classification of Pigmented Skin Lesions: From Dedicated to Hand-Held Devices. J. Med. Syst. 2015, 39, 177. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, R.B.; Filho, M.E.; Ma, Z.; Papa, J.P.; Pereira, A.S.; Tavares, J.M.R. Withdrawn: Computational methods for the image segmentation of pigmented skin lesions: A Review. Comput. Methods Programs Biomed. 2016, 131, 127–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashour, A.S.; Hawas, A.R.; Guo, Y.; Wahba, M.A. A novel optimized neutrosophic k-means using genetic algorithm for skin lesion detection in dermoscopy images. Signal Image Video Process. 2018, 12, 1311–1318. [Google Scholar] [CrossRef] [Green Version]
- Pathan, S.; Prabhu, K.G.; Siddalingaswamy, P. Techniques and algorithms for computer aided diagnosis of pigmented skin lesions—A review. Biomed. Signal Process. Control 2018, 39, 237–262. [Google Scholar] [CrossRef]
- Rodriguez-Ruiz, A.; Mordang, J.J.; Karssemeijer, N.; Sechopoulos, I.; Mann, R.M. Can radiologists improve their breast cancer detection in mammography when using a deep learning-based computer system as decision support? In Proceedings of the Society of Photo-Optical Instrumentation Engineers (SPIE) Conference Series; International Society for Optics and Photonics: Bellingham, WA, USA, 2018. [Google Scholar]
- Litjens, G.; Kooi, T.; Bejnordi, B.E.; Setio, A.A.A.; Ciompi, F.; Ghafoorian, M.; Van Der Laak, J.A.; Van Ginneken, B.; Sánchez, C.I. A survey on deep learning in medical image analysis. Med. Image Anal. 2017, 42, 60–88. [Google Scholar] [CrossRef] [Green Version]
- Badrinarayanan, V.; Kendall, A.; Cipolla, R. Segnet: A deep convolutional encoder-decoder architecture for image segmentation. arXiv 2015, arXiv:1511.00561. [Google Scholar] [CrossRef]
- Chen, L.-C.; Papandreou, G.; Kokkinos, I.; Murphy, K.; Yuille, A.L. DeepLab: Semantic Image Segmentation with Deep Convolutional Nets, Atrous Convolution, and Fully Connected CRFs. IEEE Trans. Pattern Anal. Mach. Intell. 2018, 40, 834–848. [Google Scholar] [CrossRef]
- García-García, A.; Orts-Escolano, S.; Oprea, S.; Villena-Martínez, V.; García-Rodríguez, J. A review on deep learning techniques applied to semantic segmentation. arXiv 2017, arXiv:1704.06857. [Google Scholar]
- Yu, Z.; Jiang, X.; Zhou, F.; Qin, J.; Ni, D.; Chen, S.; Lei, B.; Wang, T. Melanoma Recognition in Dermoscopy Images via Aggregated Deep Convolutional Features. IEEE Trans. Biomed. Eng. 2018, 66, 1006–1016. [Google Scholar] [CrossRef]
- Codella, N.C.; Gutman, D.; Celebi, M.E.; Helba, B.; Marchetti, M.A.; Dusza, S.W.; Kalloo, A.; Liopyris, K.; Mishra, N.; Kittler, H.; et al. Skin lesion analysis toward melanoma detection: A challenge at the 2017 international symposium on biomedical imaging (ISBI), hosted by the international skin imaging collaboration (ISIC). In Proceedings of the 2018 IEEE 15th International Symposium on Biomedical Imaging (ISBI 2018), Washington, DC, USA, 4–7 April 2018. [Google Scholar]
- Yuan, Y.; Chao, M.; Lo, Y.-C. Automatic Skin Lesion Segmentation Using Deep Fully Convolutional Networks with Jaccard Distance. IEEE Trans. Med. Imaging 2017, 36, 1876–1886. [Google Scholar] [CrossRef]
- Li, H.; He, X.; Zhou, F.; Yu, Z.; Ni, D.; Chen, S.; Wang, T.; Lei, B. Dense Deconvolutional Network for Skin Lesion Segmentation. IEEE J. Biomed. Health Inform. 2018, 23, 527–537. [Google Scholar] [CrossRef] [PubMed]
- Roesch, A.; Berking, C. Melanoma. In Braun-Falco’s Dermatology; Springer: Berlin, Germany, 2020; pp. 1–17. [Google Scholar]
- Wolf, I.H.; Smolle, J.; Soyer, H.P.; Kerl, H. Sensitivity in the clinical diagnosis of malignant melanoma. Melanoma Res. 1998, 8, 425–429. [Google Scholar] [CrossRef] [PubMed]
- Friedman, R.J.; Rigel, D.S.; Kopf, A.W. Early Detection of Malignant Melanoma: The Role of Physician Examination and Self-Examination of the Skin. CA Cancer J. Clin. 1985, 35, 130–151. [Google Scholar] [CrossRef] [PubMed]
- She, Z.; Liu, Y.; Damatoa, A. Combination of features from skin pattern and ABCD analysis for lesion classification. Skin Res. Technol. 2007, 13, 25–33. [Google Scholar] [CrossRef] [Green Version]
- Yagerman, S.E.; Chen, L.; Jaimes, N.; Dusza, S.W.; Halpern, A.C.; Marghoob, A. “Do UC the melanoma?” Recognising the importance of different lesions displaying unevenness or having a history of change for early melanoma detection. Aust. J. Dermatol. 2014, 55, 119–124. [Google Scholar] [CrossRef]
- Kim, J.K.; Nelson, K.C. Dermoscopicfeatures of common nevi: A review. G. Ital. Dermatol. Venereol. 2012, 147, 141–148. [Google Scholar]
- Saida, T.; Koga, H.; Uhara, H. Key points in dermoscopic differentiation between early acral melanoma and acral nevus. J. Dermatol. 2011, 38, 25–34. [Google Scholar] [CrossRef]
- Kolm, I.; French, L.; Braun, R.P. Dermoscopypatterns of nevi associated with melanoma. G. Ital. Dermatol. Venereol. 2010, 145, 99–110. [Google Scholar] [PubMed]
- Zhou, Y.; Smith, M.; Smith, L.; Warr, R. A new method describing border irregularity of pigmented lesions. Skin Res. Technol. 2010, 16, 66–76. [Google Scholar] [CrossRef]
- Forsea, A.M.; Tschandl, P.; Zalaudek, I.; del Marmol, V.; Soyer, H.P.; Argenziano, G.; Geller, A.C.; Arenbergerova, M.; Azenha, A.; Blum, A.; et al. The impact of dermoscopy on melanoma detection in the practice of dermatologists in Europe: Results of a pan-European survey. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 1148–1156. [Google Scholar] [CrossRef]
- Henning, J.S.; Dusza, S.W.; Wang, S.Q.; Marghoob, A.A.; Rabinovitz, H.S.; Polsky, D.; Kopf, A.W. The CASH (color, architecture, symmetry, and homogeneity) algorithm for dermoscopy. J. Am. Acad. Dermatol. 2007, 56, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Saba, T.; Khan, M.A.; Rehman, A. Region Extraction and Classification of Skin Cancer: A Heterogeneous framework of Deep CNN Features Fusion and Reduction. J. Med. Syst. 2019, 43, 2–19. [Google Scholar] [CrossRef] [PubMed]
- Lin, B.S.; Michael, K.; Kalra, S.; Tizhoosh, H.R. Skin lesion segmentation: U-nets versus clustering. In Proceedings of the 2017 IEEE Symposium Series on Computational Intelligence (SSCI), Honolulu, HI, USA, 27 November–1 December 2017. [Google Scholar]
- Soudani, A.; Barhoumi, W. An image-based segmentation recommender using crowdsourcing and transfer learning for skin lesion extraction. Expert Syst. Appl. 2019, 118, 400–410. [Google Scholar] [CrossRef]
- Xie, Y.; Zhang, J.; Xia, Y.; Shen, C. A Mutual Bootstrapping Model for Automated Skin Lesion Segmentation and Classification. IEEE Trans. Med Imaging 2020, 39, 2482–2493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akram, T.; Lodhi, J.M.H.; Naqvi, R.S.; Naeem, S.; Alhaisoni, M.; Ali, M.; Haider, A.S.; Qadri, N.N. A multilevel features selection framework for skin lesion classification. Hum. Cent. Comput. Inf. Sci. 2020, 10, 1–26. [Google Scholar] [CrossRef]
- Hasan, K.M.; Dahal, L.; Samarakoon, N.P.; Tushar, I.F.; Martí, R. DSNet: Automatic dermoscopic skin lesion segmentation. Comput. Biol. Med. 2020, 120, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Bi, L.; Kim, J.; Ahn, E.; Feng, D. Automatic skin lesion analysis using large-scale dermoscopy images anddeep residual networks. arXiv 2017, arXiv:1703.04197. [Google Scholar]
- Bi, L.; Kim, J.; Ahn, E.; Kumar, A.; Feng, D.; Fulham, M. Step-wise integration of deep class-specific learning for dermoscopic image segmentation. Pattern Recognit 2019, 85, 78–89. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Shen, L. Skin Lesion Analysis towards Melanoma Detection Using Deep Learning Network. Sensors 2018, 18, 556. [Google Scholar] [CrossRef] [Green Version]
- Al-masni, M.A.; Al-antari, M.A.; Choi, M.T.; Han, S.M. Skin lesion segmentation in dermoscopy images via deep full resolution convolutional networks. Comput. Methods Programs Biomed. 2018, 162, 221–231. [Google Scholar] [CrossRef]
- Al-masni, A.M.; Kim, D.; Kim, T. Multiple skin lesions diagnostics via integrated deep convolutional networks for segmentation and classification. Comput. Methods Programs Biomed. 2020, 190, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y. Automatic skin lesion segmentation with fully convolutional-deconvolutional networks. arXiv 2017, arXiv:1703.05165. [Google Scholar]
- Ünver, H.M.; Ayan, E. Skin Lesion Segmentation in Dermoscopic Images with Combination of YOLO and GrabCut Algorithm. Diagnostics 2019, 9, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Datasets | Test Data | Total | ||
|---|---|---|---|---|
| Label | B | M | AT | |
| PH2 | 80 | 40 | 80 | 200 |
| Datasets | Training Data | Validation Data | Test Data | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Label | B | M | SK | B | M | SK | B | M | SK | |
| ISBI 2017 | 1372 | 374 | 254 | 78 | 30 | 42 | 393 | 117 | 90 | 2750 |
| Dataset | NV | M | BKL | BCC | SCC | VL | DF | AK | Total |
|---|---|---|---|---|---|---|---|---|---|
| ISIC 2019 | 12,875 | 4522 | 2624 | 3323 | 628 | 253 | 239 | 867 | 25,331 |
| Datasets | Training Data | Validation Data | Test Data | Total | |||
|---|---|---|---|---|---|---|---|
| Label | M | NM | M | NM | M | NM | |
| ISIC 2019 | 3622 | 10,218 | 450 | 1280 | 450 | 1280 | 17,300 |
| Datasets | Training Data | Validation Data | Test Data | Total | |||
|---|---|---|---|---|---|---|---|
| Label | M | NM | M | NM | M | NM | |
| PH2 | * | * | * | * | 40 | 160 | 200 |
| ISBI 2017 | 374 | 1626 | 30 | 120 | 117 | 483 | 2750 |
| ISIC 2019 | 3622 | 10,218 | 450 | 1280 | 450 | 1280 | 17,300 |
| Total | 3996 | 11,844 | 480 | 1400 | 607 | 1923 | 20,250 |
| Datasets | Sensitivity | Specificity | IOU |
|---|---|---|---|
| PH2 | 97.5 | 98.75 | 95 |
| ISBI 2017 | 98.47 | 97.51 | 92 |
| ISIC 2019 | 97.77 | 97.65 | 90 |
| Datasets | Acc | Sen | Spe | Jac | Dic |
|---|---|---|---|---|---|
| PH2 | 96 | 95 | 96.25 | 82.60 | 90.47 |
| ISBI 2017 | 95.67 | 88.89 | 97.31 | 80.00 | 88.89 |
| ISIC 2019 | 92.94 | 88.88 | 94.37 | 76.62 | 86.76 |
| Datasets | Acc | Sen | Spe | Jac | Dic |
|---|---|---|---|---|---|
| PH2 | 97.50 | 97.50 | 97.50 | 88.64 | 93.97 |
| ISBI 2017 | 97.33 | 91.45 | 98.76 | 86.99 | 93.04 |
| ISIC 2019 | 93.98 | 91.55 | 94.84 | 79.84 | 88.79 |
| References | Year | Dataset | Acc | Sen | Spe | Jac | Dic |
|---|---|---|---|---|---|---|---|
| Bi et al. (ResNets) [63] | 2017 | PH2 | 94.24 | 94.89 | 93.98 | 83.99 | 90.66 |
| Bi et al. [64] | 2019 | PH2 | 95.03 | 96.23 | 94.52 | 85.9 | 92.1 |
| Saba etal. [57] | 2019 | PH2 | 95.41 | - | - | - | - |
| Unver etal. [69] | 2019 | PH2 | 92.99 | 83.63 | 94.02 | 79.54 | 88.13 |
| Xie et al. [60] | 2020 | PH2 | 96.5 | 96.7 | 94.6 | 89.4 | 94.2 |
| Hasan et al. [62] | 2020 | PH2 | 98.7 | 92.9 | 96.9 | - | - |
| Proposed Method | 2020 | PH2 | 97.5 | 97.5 | 97.5 | 88.64 | 93.97 |
| References | Year | Dataset | Acc | Sen | Spe | Jac | Dic |
|---|---|---|---|---|---|---|---|
| Yuan et al. (CDNN) [68] Lin et al. (U-Net) [58] Bi et al.(ResNets) [63] Li et al. [65] Al-Masni et al. [66] Bi et al. [64] Soudani et al. [59] Unver etal. [69] Xie et al. [60] Akram et al. [61] Hasan et al. [62] Al-Masni et al. [67] | 2017 2017 2017 2018 2018 2019 2019 2019 2020 2020 2020 2020 | ISBI 2017 ISBI 2017 ISBI 2017 ISBI 2017 ISBI 2017 ISBI 2017 ISBI 2017 ISBI 2017 ISBI 2017 ISBI 2017 ISBI 2017 ISBI 2017 | 93.4 - 93.4 93.2 94.03 94.08 94.95 93.39 94.7 95.9 95.3 81.57 | 82.5 - 80.2 82 85.4 86.2 85.87 90.82 87.4 - 87.5 75.67 | 97.5 - 98.5 97.8 96.69 96.17 95.66 92.68 96.8 - 95.5 80.62 | 76.5 62.00 76 76.2 77.11 77.73 78.92 74.81 80.4 - - - | 84.9 77.00 84.4 84.7 87.08 85.66 88.12 84.26 87.8 - - - |
| Proposed Method | 2020 | ISBI 2017 | 97.33 | 91.45 | 98.76 | 86.99 | 93.04 |
| References | Year | Dataset | Acc | Sen | Spe | Jac | Dic |
|---|---|---|---|---|---|---|---|
| Proposed Method | 2020 | ISIC 2019 | 93.98 | 91.55 | 94.84 | 79.84 | 88.79 |
| Classifier | Method | Acc (%) | Sen (%) | Spec (%) | Prec | AUC | Time (in sec) |
|---|---|---|---|---|---|---|---|
| TREE | CT | 75 | 75 | 75 | 42.85 | 0.83 | 17.11 |
| ST | 76.5 | 77.5 | 76.25 | 44.92 | 0.89 | 4.61 | |
| SVM | LSVM | 97 | 95 | 97.5 | 90.47 | 0.99 | 7.24 |
| CSVM | 96.5 | 90 | 98.12 | 92.30 | 0.96 | 9.43 | |
| QSVM | 97.5 | 95 | 98.12 | 92.68 | 0.98 | 5.81 | |
| MGSVM | 92 | 90 | 92.5 | 75 | 0.96 | 5.11 | |
| KNN | FKNN | 98 | 95 | 98.75 | 95 | 0.97 | 4.94 |
| MKNN | 96.5 | 92.5 | 97.5 | 90.24 | 0.98 | 3.96 | |
| Cosine | 96 | 92.5 | 96.87 | 88.09 | 0.99 | 4.65 | |
| Cubic | 98 | 95 | 98.75 | 95 | 0.98 | 5.78 | |
| WKNN | 94 | 97.5 | 93.12 | 78 | 0.99 | 4.15 | |
| YOLO | Proposed Method | 99 | 97.5 | 99.37 | 97.5 | 0.99 | 2.63 |
| Classifier | Method | Acc (%) | Sen (%) | Spec (%) | Prec | AUC | Time (in sec) |
|---|---|---|---|---|---|---|---|
| TREE | CT | 92.83 | 90.60 | 93.37 | 76.81 | 0.96 | 8.12 |
| ST | 88.00 | 88.89 | 87.78 | 63.80 | 0.92 | 12.67 | |
| SVM | LSVM | 96.67 | 93.16 | 97.52 | 90.08 | 0.95 | 11.42 |
| CSVM | 86.83 | 85.47 | 87.16 | 61.73 | 0.92 | 140.54 | |
| QSVM | 97.50 | 94.87 | 98.14 | 92.50 | 0.97 | 21.47 | |
| MGSVM | 96.67 | 94.87 | 97.10 | 88.80 | 0.98 | 13.45 | |
| KNN | FKNN | 94.00 | 92.31 | 94.41 | 80.00 | 0.90 | 9.04 |
| MKNN | 97.83 | 94.02 | 98.76 | 94.83 | 0.96 | 10.01 | |
| Cosine | 97.50 | 93.16 | 98.55 | 93.97 | 0.97 | 10.78 | |
| Cubic | 97.50 | 94.02 | 98.34 | 93.22 | 0.97 | 102.01 | |
| WKNN | 98.50 | 96.58 | 98.96 | 95.76 | 0.98 | 12.75 | |
| YOLO | Proposed Method | 99.00 | 97.44 | 99.38 | 97.44 | 0.99 | 7.14 |
| Classifier | Method | Acc (%) | Sen (%) | Spec (%) | Prec | AUC | Time (in sec) |
|---|---|---|---|---|---|---|---|
| TREE | CT | 91.68 | 90.67 | 92.03 | 80.00 | 0.95 | 15.21 |
| ST | 86.94 | 89.11 | 86.17 | 69.38 | 0.93 | 21.88 | |
| SVM | LSVM | 93.47 | 92.00 | 93.98 | 84.32 | 0.95 | 19.39 |
| CSVM | 88.09 | 88.44 | 87.97 | 72.10 | 0.93 | 246.98 | |
| QSVM | 93.06 | 91.56 | 93.59 | 83.40 | 0.98 | 37.01 | |
| MGSVM | 94.86 | 91.78 | 95.94 | 88.82 | 0.96 | 26.32 | |
| KNN | FKNN | 93.82 | 83.11 | 97.58 | 92.35 | 0.92 | 18.15 |
| MKNN | 90.69 | 86.00 | 92.34 | 79.79 | 0.96 | 17.47 | |
| Cosine | 92.02 | 93.11 | 91.64 | 79.66 | 0.99 | 19.19 | |
| Cubic | 94.74 | 88.00 | 97.11 | 91.45 | 0.97 | 176.45 | |
| WKNN | 95.84 | 93.56 | 96.64 | 90.73 | 0.99 | 22.39 | |
| YOLO | Proposed Method | 97.11 | 94.22 | 98.13 | 94.64 | 0.99 | 12.40 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Banerjee, S.; Singh, S.K.; Chakraborty, A.; Das, A.; Bag, R. Melanoma Diagnosis Using Deep Learning and Fuzzy Logic. Diagnostics 2020, 10, 577. https://doi.org/10.3390/diagnostics10080577
Banerjee S, Singh SK, Chakraborty A, Das A, Bag R. Melanoma Diagnosis Using Deep Learning and Fuzzy Logic. Diagnostics. 2020; 10(8):577. https://doi.org/10.3390/diagnostics10080577
Chicago/Turabian StyleBanerjee, Shubhendu, Sumit Kumar Singh, Avishek Chakraborty, Atanu Das, and Rajib Bag. 2020. "Melanoma Diagnosis Using Deep Learning and Fuzzy Logic" Diagnostics 10, no. 8: 577. https://doi.org/10.3390/diagnostics10080577