A CBCT Based Three-Dimensional Assessment of Mandibular Posterior Region for Evaluating the Possibility of Bypassing the Inferior Alveolar Nerve While Placing Dental Implants


 ,
,  , , ,
, , ,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
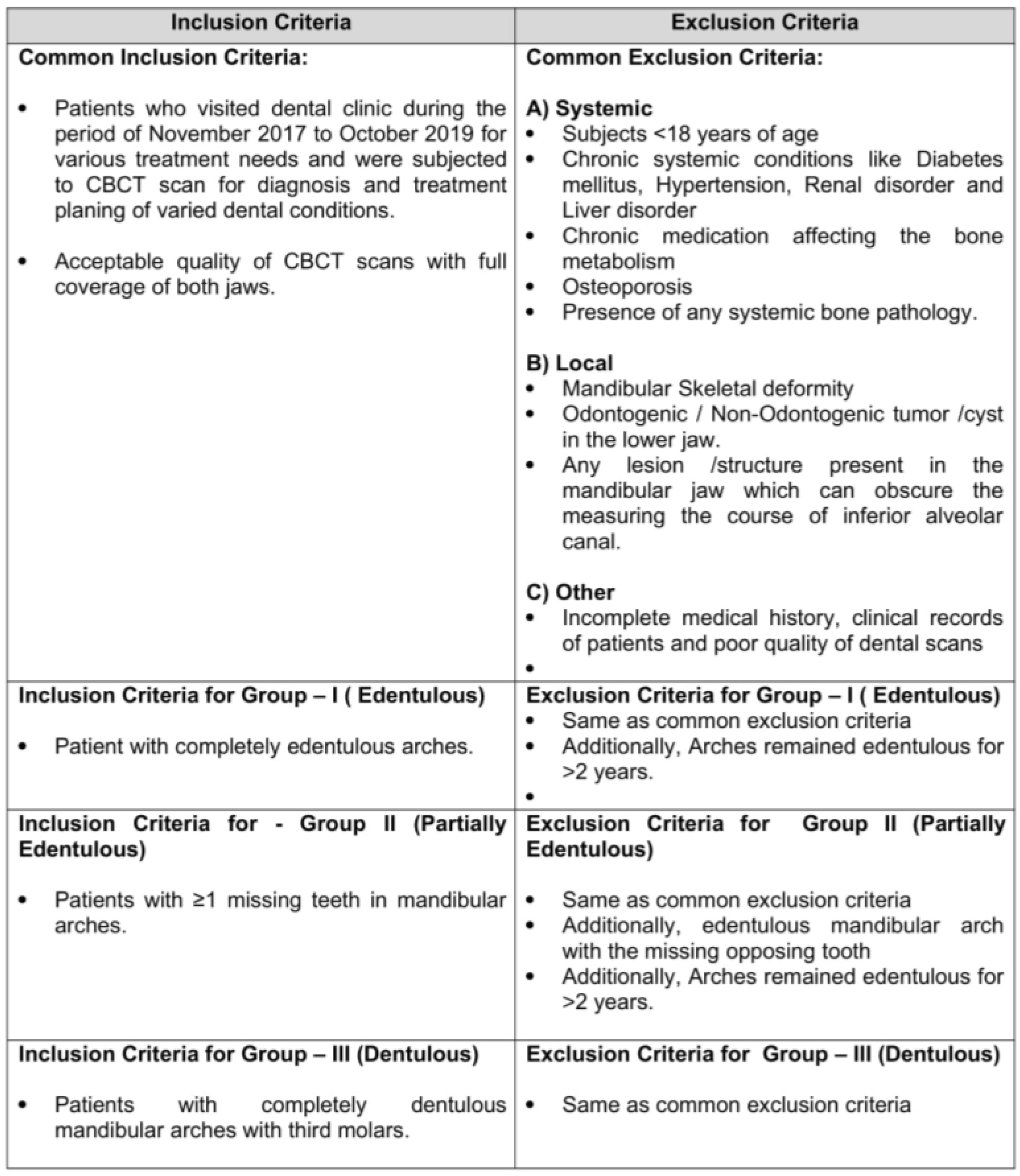
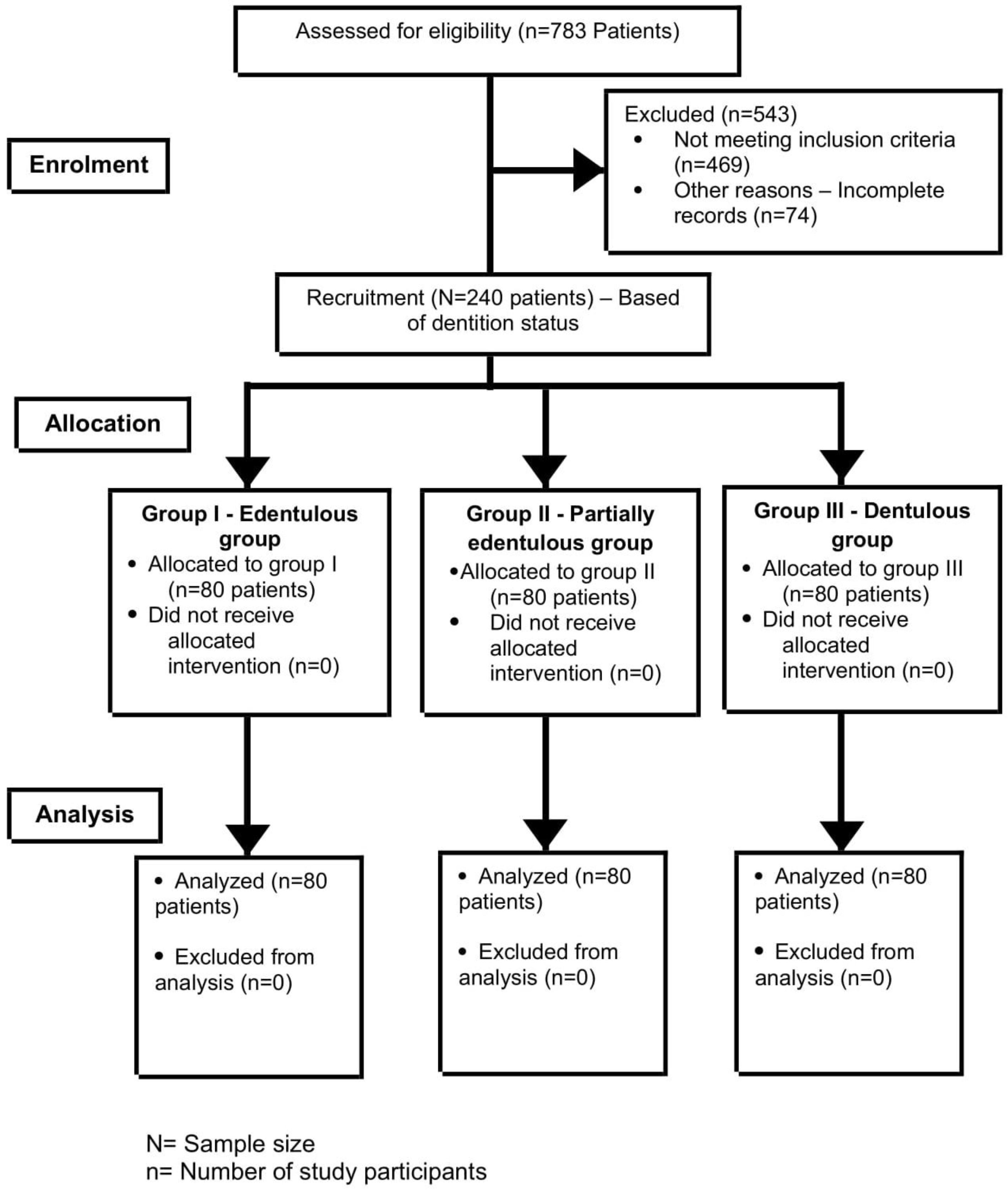
2.1. Study and Sample Characteristics
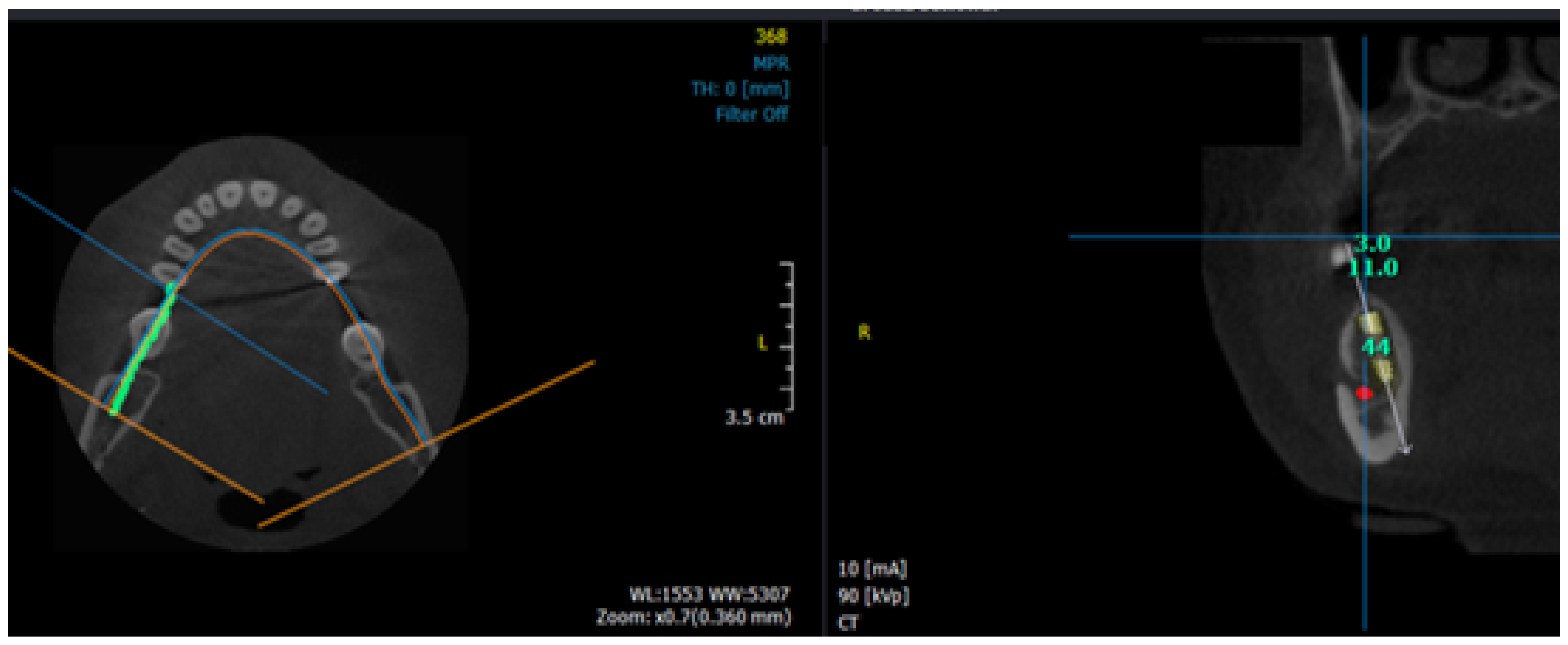
2.2. Specifications of CBCT Machine and Workstation
2.3. Standardization of Examiners and Reliability Analysis
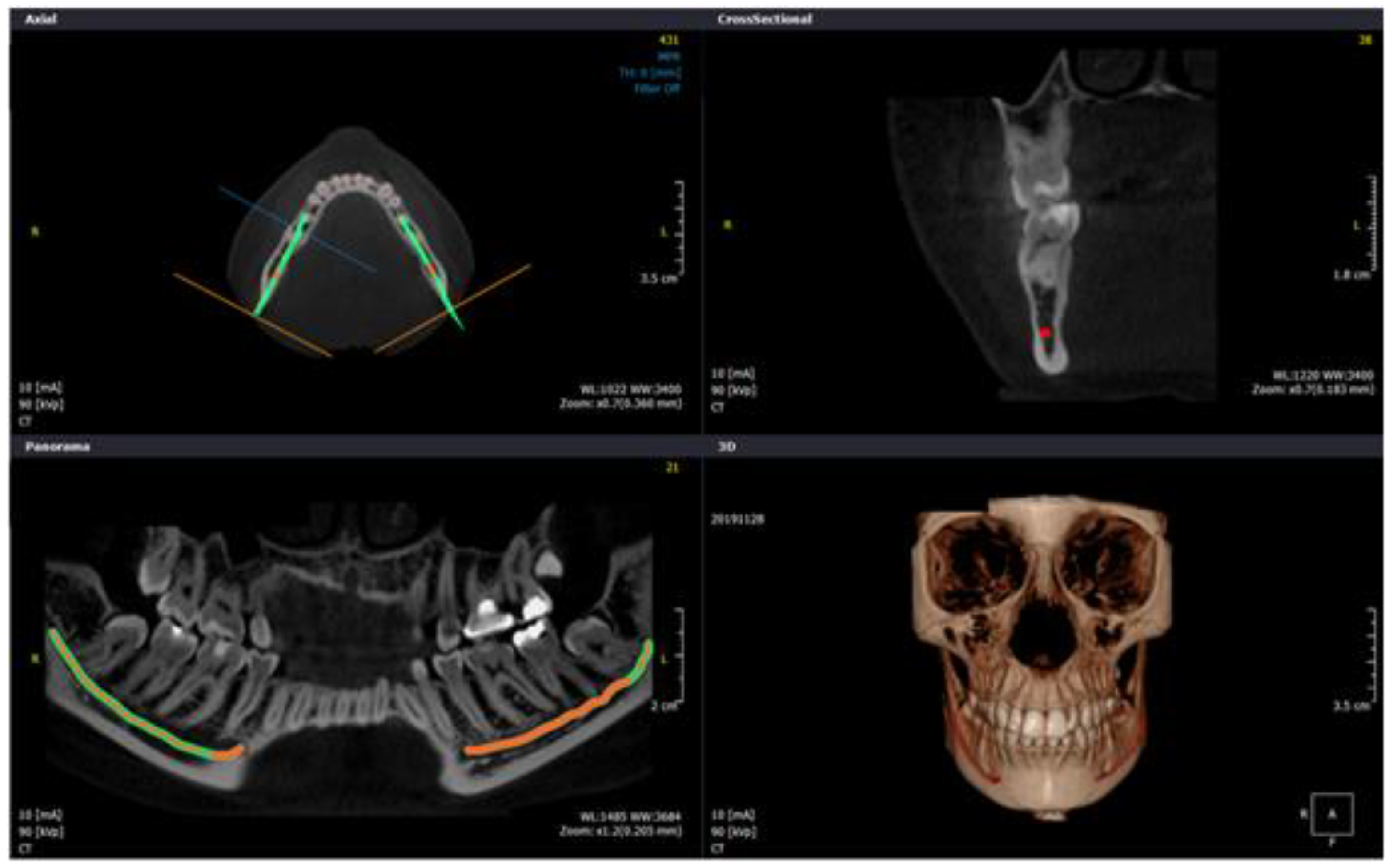
2.4. Study Protocol and Image Analysis
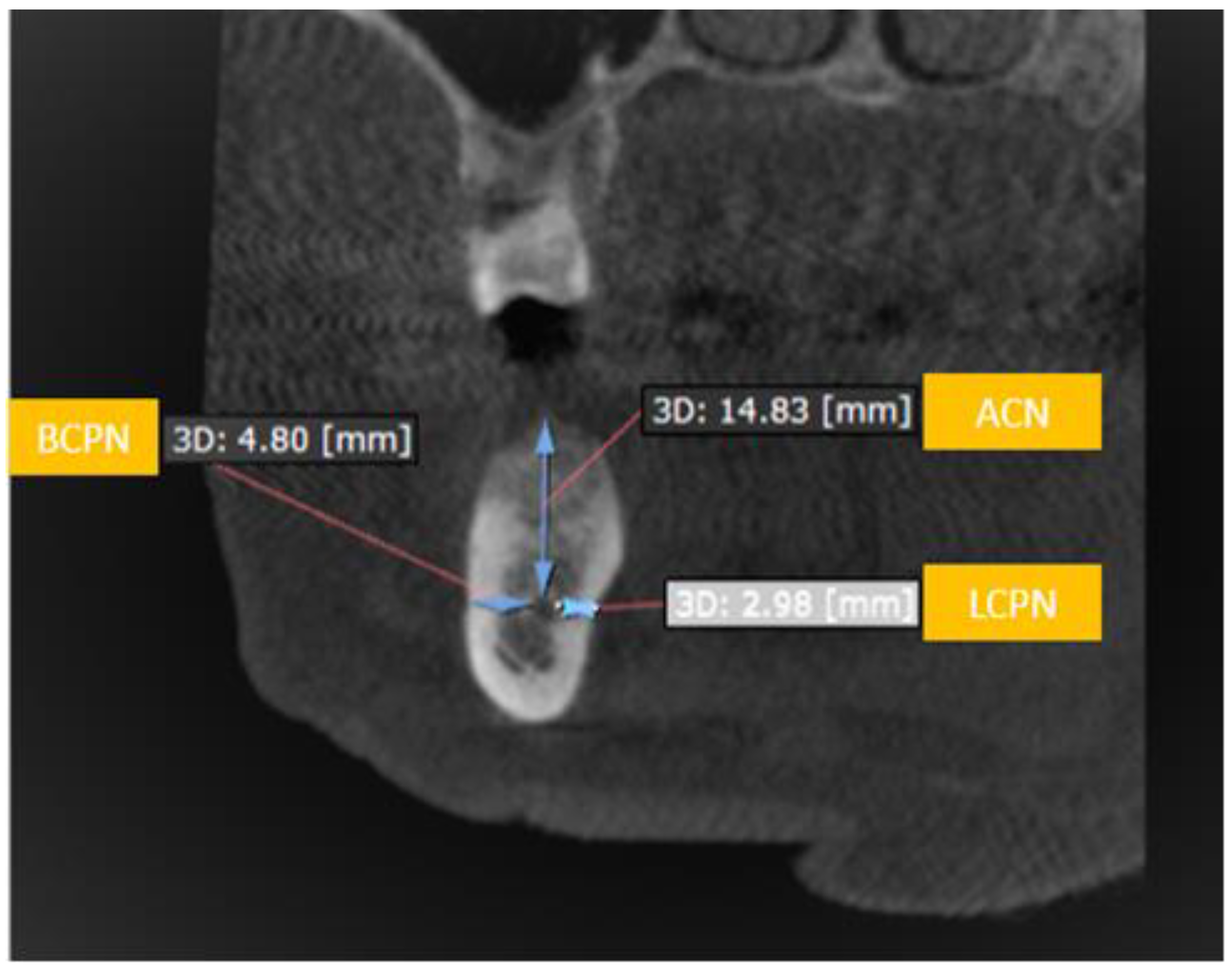
- I.
- Buccalcortical plate to IAN dimension (BCPN): Linear distance from the IAN to the nearest corresponding buccal outer cortical plate.
- II.
- Lingual cortical plate to IAN dimension (LCPN): Linear distance from the IAN to the nearest corresponding lingual outer cortical plate.
- III.
- Alveolar crest to IAN dimension (ACN): Linear distance from the IAN coronally to the midpoint of alveolar crest bone corresponding to the long axis of tooth.
2.5. Statistical Analysis
2.5.1. Sample Size and Power of the Study
2.5.2. Data Entry, Descriptive and Inferential Analysis
3. Results
3.1. Descriptive Statistical Analysis of the Baseline Sample Characteristics
3.2. Inferential Analysis of the BPCN, LCPN and ACN Among the Study Groups
3.3. Inferential Analysis of the BPCN, LCPN and ACN among the Various Independent Variables-Side of Jaw, Gender and Age
4. Discussion
4.1. Comparison of BCPN, LCPN and ACN Dimensions among the Patients with Different Dentition Status
4.2. Comparison of BCPN, LCPN and ACN Dimensions among the Patients with Different Dentition Status and Side of the Jaw
4.3. Comparison of BCPN, LCPN and ACN Dimensions among the Patients with Different Dentition Status and Gender
4.4. Comparison of Buccal-Lingual-Coronal Dimensions among Patients with Different Dentition Status and Age Groups
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Weiss, R.; Read-Fuller, A.M. Cone Beam Computed Tomography in Oral and Maxillofacial Surgery: An Evidence-Based Review. Dent. J. 2019, 7, 52. [Google Scholar] [CrossRef] [Green Version]
- Benavides, E.; Rios, H.F.; Ganz, S.D.; An, C.-H.; Resnik, R.; Reardon, G.T.; Feldman, S.J.; Mah, J.K.; Hatcher, D.; Kim, M.-J.; et al. Use of Cone Beam Computed Tomography in Implant Dentistry. Implant. Dent. 2012, 21, 78–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Srivastava, K.C.; Ijar; Shrivastava, D.; Austin, D. Journey towards the 3d dental imaging- the milestones in the advancement of dental imaging. Int. J. Adv. Res. 2016, 4, 377–382. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, R.; Salmon, B.; Codari, M.; Hassan, B.; Bornstein, M.M. Cone beam computed tomography in implant dentistry: Recommendations for clinical use. BMC Oral Heal. 2018, 18, 88. [Google Scholar] [CrossRef] [Green Version]
- Massey, N.D.; A Galil, K.; Wilson, T.D. Determining position of the inferior alveolar nerve via anatomical dissection and micro-computed tomography in preparation for dental implants. J. Can. Dent. Assoc. 2013, 79, 1–7. [Google Scholar]
- Murat, S.; Kamburoglu, K.; Kilic, C.; Özen, T.; Gurbuz, A. Nerve Damage Assessment Following Implant Placement in Human Cadaver Jaws: An Ex Vivo Comparative Study. J. Oral Implant. 2014, 40, 76–82. [Google Scholar] [CrossRef]
- Yatzkair, G.; Cheng, A.; Brodie, S.; Raviv, E.; Boyan, B.; Schwartz, Z. Accuracy of computer-guided implantation in a human cadaver model. Clin. Oral Implant. Res. 2014, 26, 1143–1149. [Google Scholar] [CrossRef] [PubMed]
- Balaji, S.M.; Krishnaswamy, N.R.; Kumar, S.M.; Rooban, T. Inferior alveolar nerve canal position among South Indians: A cone beam computed tomographic pilot study. Ann. Maxillofac. Surg. 2012, 2, 51–55. [Google Scholar] [CrossRef]
- Khorshidi, H.; Raoofi, S.; Ghapanchi, J.; Shahidi, S.; Paknahad, M. Cone Beam Computed Tomographic Analysis of the Course and Position of Mandibular Canal. J. Maxillofac. Oral Surg. 2016, 16, 306–311. [Google Scholar] [CrossRef]
- Shokry, S.M.; Alshaib, S.A.; Al Mohaimeed, Z.Z.; Ghanimah, F.; Altyebe, M.M.; Alenezi, M.A.; Shadd, F.; Aldali, S.Z.; Alotaibi, M.M. Assessment of the Inferior Alveolar Nerve Canal Course Among Saudis by Cone Beam Computed Tomography (Pilot Study). J. Maxillofac. Oral Surg. 2018, 18, 452–458. [Google Scholar] [CrossRef]
- Aljarbou, F.A.; Aldosimani, M.A.; Althumairy, R.I.; Alhezam, A.A.; Aldawsari, A.I. An analysis of the first and second mandibular molar roots proximity to the inferior alveolar canal and cortical plates using cone beam computed tomography among the Saudi population. Saudi Med. J. 2019, 40, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Cartes, G.; Garay, I.; Deana, N.F.; Navarro, P.; Alves, N. Mandibular Canal Course and the Position of the Mental Foramen by Panoramic X-Ray in Chilean Individuals. BioMed Res. Int. 2018, 2018, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Al-Mahalawy, H.A.; Al-Aithan, H.; Al-Kari, B.; Al-Jandan, B.; Shujaat, S. Determination of the position of mental foramen and frequency of anterior loop in Saudi population. A retrospective CBCT study. Saudi Dent. J. 2017, 29, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Alam, M.K.; Alhabib, S.; AlZarea, B.; Irshad, M.; Faruqi, S.; Sghaireen, M.G.; Patil, S.R.; Basri, R. 3D CBCT morphometric assessment of mental foramen in Arabic population and global comparison: Imperative for invasive and non-invasive procedures in mandible. Acta Odontol. Scand. 2017, 76, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Demir, A.; Izgi, E.; Pekiner, F. Anterior Loop of the Mental foramen in a Turkish Subpopulation with Dentate Patients: A Cone Beam Computed Tomography Study. J. Marmara Univ. Inst. Heal. Sci. 2015, 5, 1. [Google Scholar] [CrossRef]
- Greenstein, G.; Tarnow, D. The Mental Foramen and Nerve: Clinical and Anatomical Factors Related to Dental Implant Placement: A Literature Review. J. Periodontol. 2006, 77, 1933–1943. [Google Scholar] [CrossRef]
- Wei, X.; Gu, P.; Hao, Y.; Wang, J. Detection and characterization of anterior loop, accessory mental foramen, and lateral lingual foramen by using cone beam computed tomography. J. Prosthet. Dent. 2019. [Google Scholar] [CrossRef]
- Lin, M.-H.; Mau, L.-P.; Cochran, D.L.; Shieh, Y.-S.; Huang, P.-H.; Huang, R.-Y. Risk assessment of inferior alveolar nerve injury for immediate implant placement in the posterior mandible: A virtual implant placement study. J. Dent. 2014, 42, 263–270. [Google Scholar] [CrossRef]
- Mirbeigi, S.; Safaee, A.; Ezoddini, F.; Khojastepour, L.; Navab-Azam, A. Buccolingual course of the inferior alveolar canal in different mental foramen locations: A cone beam computed tomography study of an Iranian population. Int. J. Appl. Basic Med Res. 2016, 6, 262–266. [Google Scholar] [CrossRef] [Green Version]
- Velasco-Torres, M.; Padial-Molina, M.; Avila-Ortiz, G.; García-Delgado, R.; Catena, A.; Galindo-Moreno, P. Inferior alveolar nerve trajectory, mental foramen location and incidence of mental nerve anterior loop. Medicina Oral Patología Oral y Cirugia Bucal 2017, 22, e630–e635. [Google Scholar] [CrossRef]
- Kavarthapu, A.; Thamaraiselvan, M. Assessing the variation in course and position of inferior alveolar nerve among south Indian population: A cone beam computed tomographic study. Indian J. Dent. Res. 2018, 29, 405. [Google Scholar] [CrossRef] [PubMed]
- Juodzbalys, G.; Wang, H.-L. Identification of the Mandibular Vital Structures: Practical Clinical Applications of Anatomy and Radiological Examination Methods. J. Oral Maxillofac. Res. 2010, 1. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement. Epidemiology 2007, 18, 800–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Omiri, M.; Sghaireen, M.G.; Alhijawi, M.M.; Alzoubi, I.A.; Lynch, C.D.; Lynch, E. Maximum bite force following unilateral implant-supported prosthetic treatment: Within-subject comparison to opposite dentate side. J. Oral Rehabil. 2014, 41, 624–629. [Google Scholar] [CrossRef]
- Na, J.Y.; Han, S.-S.; Jeon, K.J.; Choi, Y.J.; Choi, S.-H.; Lee, C. Prognosis in case of nerve disturbance after mandibular implant surgery in relation to computed tomography findings and symptoms. J. Periodontal Implant. Sci. 2019, 49, 127–135. [Google Scholar] [CrossRef]
- Liang, X.; Jacobs, R.; Hassan, B.; Li, L.; Pauwels, R.; Corpas, L.; Souza, P.H.C.; Martens, W.; Shahbazian, M.; Alonso, A.; et al. A comparative evaluation of Cone Beam Computed Tomography (CBCT) and Multi-Slice CT (MSCT). Eur. J. Radiol. 2010, 75, 265–269. [Google Scholar] [CrossRef]
- Monsour, P.; Dudhia, R. Implant radiography and radiology. Aust. Dent. J. 2008, 53, S11–S25. [Google Scholar] [CrossRef]
- Agbaje, J.; Van De Casteele, E.; Salem, A.S.; Anumendem, D.; Lambrichts, I.; Politis, C. Tracking of the inferior alveolar nerve: Its implication in surgical planning. Clin. Oral Investig. 2016, 21, 2213–2220. [Google Scholar] [CrossRef]
- Angel, J.S.; Mincer, H.H.; Chaudhry, J.; Scarbecz, M. Cone-beam Computed Tomography for Analyzing Variations in Inferior Alveolar Canal Location in Adults in Relation to Age and Sex*. J. Forensic Sci. 2011, 56, 216–219. [Google Scholar] [CrossRef]
- Ali, S.P.; Gupta, J. Cone beam computed tomography in oral implants. Natl. J. Maxillofac. Surg. 2013, 4, 2–6. [Google Scholar] [CrossRef] [Green Version]
- Worthington, P. Injury to the inferior alveolar nerve during implant placement: A formula for protection of the patient and clinician. Int. J. Oral Maxillofac. Implant. 2004, 19, 731–734. [Google Scholar]
- Juodzbalys, G.; Wang, H.-L.; Sabalys, G. Injury of the Inferior Alveolar Nerve during Implant Placement: A Literature Review. J. Oral Maxillofac. Res. 2011, 2. [Google Scholar] [CrossRef] [PubMed]
- Gurler, G.; Tufekcioglu, S.; Delilbasi, C.; Dilaver, E.; Ozer, N. Is 2 mm a safe distance from the inferior alveolar canal to avoid neurosensory complications in implant surgery? Niger. J. Clin. Pr. 2017, 20, 274. [Google Scholar] [CrossRef] [PubMed]
- Sammartino, G.; Marenzi, G.; Citarella, R.; Ciccarelli, R.; Wang, H.-L. Analysis of the Occlusal Stress Transmitted to the Inferior Alveolar Nerve by an Osseointegrated Threaded Fixture. J. Periodontol. 2008, 79, 1735–1744. [Google Scholar] [CrossRef]
- Froum, S.J.; Casanova, L.; Byrne, S.; Cho, S.-C. Risk Assessment before Extraction for Immediate Implant Placement in the Posterior Mandible: A Computerized Tomographic Scan Study. J. Periodontol. 2011, 82, 395–402. [Google Scholar] [CrossRef] [Green Version]
- Cho, H.-J.; Jeon, J.-Y.; Ahn, S.-J.; Lee, S.-W.; Chung, J.-R.; Park, C.-J.; Hwang, K.-G. The preliminary study for three-dimensional alveolar bone morphologic characteristics for alveolar bone restoration. Maxillofac. Plast. Reconstr. Surg. 2019, 41, 33–37. [Google Scholar] [CrossRef] [Green Version]
- Hansson, S.; Halldin, A. Alveolar ridge resorption after tooth extraction: A consequence of a fundamental principle of bone physiology. J. Dent. Biomech. 2012, 3. [Google Scholar] [CrossRef]
- Wong, S.K.; Patil, P.G. Measuring anterior loop length of the inferior alveolar nerve to estimate safe zone in implant planning: A CBCT study in a Malaysian population. J. Prosthet. Dent. 2018, 120, 210–213. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Response | Study Group | Total | ||
|---|---|---|---|---|---|
| Study Group I—Completely Edentulous (n = 80) | Study Group II—Partially Edentulous (n = 80) | Study Group III—Dentulous (n = 80) | |||
| Age (Mean ± SD) | 58.41 ± 2.928 | 41.54 ± 12.702 | 38.83 ± 14.389 | - | |
| Age | 18–35 Years | - | 28 (35) | 35 (43.8) | 63 (26.25) |
| 36–53 Years | - | 28 (35) | 24 (30) | 52 (21.66) | |
| ≥54 Years | 80 (100) | 24 (30) | 21 (26.3) | 125 (52.08) | |
| Gender | Male | 40 (50) | 43 (53.8) | 44 (55) | 127 (52.91) |
| Female | 40 (50) | 37 (46.3) | 36 (45) | 113 (47.08) | |
| Intragroup Comparison | Intergroup Comparison | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Dimension | Tooth Position | Side of Jaw | Study Groups | p Value | |||||
| Study Group I | p Value | Study Group II | p Value | Study Group III | p Value | ||||
| BCPN | 3rd Molar | Right | 5.90 ± 1.16 | 0.056 b | 6.05 ± 1.04 | 0.005 **b | 6.23 ± 1.14 | 0.130 b | 0.141 a |
| Left | 5.50 ± 1.17 | 5.85 ± 0.90 | 6.19 ± 0.99 | 0.491 a | |||||
| 2nd Molar | Right | 5.17 ± 1.261 | 0.230 b | 5.36 ± 1.04 | 0.015 *b | 5.54 ± 1.09 | 0.884 b | 0.122 a | |
| Left | 5.12 ± 1.32 | 5.20 ± 0.80 | 5.52 ± 1.04 | 0.978 a | |||||
| 1st Molar | Right | 3.70 ± 1.33 | 0.209 b | 3.70 ± 1.00 | 0.117 b | 3.87 ± 1.29 | 0.338 b | 0.594 a | |
| Left | 3.90 ± 1.19 | 3.95 ± 0.86 | 4.05 ± 1.07 | 0.654 a | |||||
| 2nd Premolar | Right | 2.03 ± 1.13 | 0.042 *b | 2.08 ± 0.56 | 0.899 b | 2.14 ± 0.65 | 0.002 **b | 0.847 a | |
| Left | 1.48 ± 0.56 | 1.70 ± 0.72 | 1.74 ± 0.53 | 0.512 a | |||||
| 1st Premolar | Right | 0 | - | 0 | - | 0 | - | - | |
| Left | 0 | 1.60 ± 0 | 0 | - | |||||
| LCPN | 3rd Molar | Right | 1.90 ± 0.65 | 0.853 b | 1.82 ± 0.76 | 0.312 b | 2.07 ± 0.65 | 0.795 b | 0.070 a |
| Left | 1.92 ± 0.60 | 2.01 ± 1.45 | 2.04 ± 0.64 | 0.714 a | |||||
| 2nd Molar | Right | 2.40 ± 0.72 | 0.286 b | 2.53 ± 0.93 | 0.533 b | 2.79 ± 0.85 | 0.616 b | 0.113 a | |
| Left | 2.42 ± 0.63 | 2.48 ± 0.71 | 2.73 ± 0.76 | 0.015 a* | |||||
| 1st Molar | Right | 3.82 ± 1.14 | 0.583 b | 4.00 ± 1.24 | 0.475 b | 4.27 ± 1.28 | 0.238 b | 0.070 a | |
| Left | 3.73 ± 1.07 | 3.87 ± 1.02 | 4.05 ± 1.08 | 0.165 a | |||||
| 2nd Premolar | Right | 6.32 ± 1.90 | 0.987 b | 6.51 ± 1.62 | 0.095 b | 6.68 ± 1.75 | 0.906 b | 0.203 a | |
| Left | 6.09 ± 1.67 | 6.35 ± 1.44 | 6.52 ± 1.55 | 0.080 a | |||||
| 1st Premolar | Right | 6.50 ± 1.20 | 0.298 b | 6.80 ± 1.46 | 0.364 b | 7.61 ± 1.34 | 0.302 b | 0.044 a* | |
| Left | 6.15 ± 1.17 | 6.44 ± 1.09 | 7.53 ± 0.77 | 0.286 a | |||||
| ACN | 3rd Molar | Right | 14.41 ± 1.39 | 0.500 b | 16.30 ± 2.07 | 0.011 b* | 16.68 ± 2.16 | 0.945 b | 0.000 a*** |
| Left | 16.90 ± 2.09 | 16.11 ± 2.42 | 14.39 ± 1.95 | 0.000 a*** | |||||
| 2nd Molar | Right | 14.98 ± 1.75 | 0.954 b | 17.98 ± 2.31 | 0.007 b** | 17.80 ± 2.36 | 0.952 b | 0.000 a*** | |
| Left | 17.78 ± 2.12 | 16.96 ± 2.43 | 14.96 ± 2.39 | 0.000 a*** | |||||
| 1st Molar | Right | 15.59 ± 2.45 | 0.727 b | 18.54 ± 2.65 | 0.003 b** | 18.95 ± 2.48 | 0.749 b | 0.000 a*** | |
| Left | 18.82 ± 2.28 | 17.01 ± 3.75 | 15.73 ± 2.76 | 0.000 a*** | |||||
| 2nd Premolar | Right | 12.49 ± 1.34 | 0.864 b | 13.34 ± 0.75 | 0.008 b** | 13.80 ± 1.64 | 0.686 b | 0.000 a*** | |
| Left | 13.84 ± 1.46 | 13.00 ± 0.82 | 12.41 ± 1.32 | 0.000 a*** | |||||
| 1st Premolar | Right | 8.85 ± 1.42 | 0.989 b | 10.66 ± 0.91 | 0.563 b | 11.88 ± 2 | 0.763 b | 0.000 a*** | |
| Left | 11.87 ± 1.49 | 10.46 ± 0.89 | 8.96 ± 1.08 | 0.000 a*** | |||||
| Side of Arch | Dimension | Tooth # | Study Group I | Study Group II | Study Group III | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | p Value | Male | Female | p Value | Male | Female | p Value | |||
| Right | BCPN | 3rd Molar | 6.02 ± 1.04 | 5.85 ± 1.31 | 0.520 | 6.20 ± 1.10 | 5.57 ± 0.85 | 0.006 ** | 6.07 ± 0.99 | 6.38 ± 1.27 | 0.231 |
| 2nd Molar | 5.36 ± 1.23 | 5.16 ± 1.29 | 0.475 | 5.43 ± 1.18 | 4.90 ± 0.78 | 0.024 * | 5.48 ± 0.94 | 5.60 ± 1.24 | 0.648 | ||
| 1st Molar | 3.82 ± 1.40 | 3.55 ± 1.22 | 0.372 | 3.65 ± 1.17 | 3.75 ± 0.78 | 0.678 | 3.96 ± 1.30 | 3.78 ± 1.29 | 0.535 | ||
| 2nd Premolar | 2.25 ± 1.34 | 1.88 ± 0.83 | 0.367 | 2.10 ± 0.55 | 1.98 ± 0.58 | 0.548 | 2.27 ± 0.43 | 2.00 ± 0.82 | 0.170 | ||
| 1st Premolar | 0 | 0 | - | 0 | 0 | - | 0 | 0 | - | ||
| LCPN | 3rd Molar | 1.85 ± 0.65 | 1.97 ± 0.66 | 0.415 | 1.51 ± 0.67 | 2.18 ± 0.69 | 0.000 *** | 2.17 ± 0.73 | 1.97 ± 0.55 | 0.169 | |
| 2nd Molar | 2.57 ± 0.79 | 2.49 ± 0.64 | 0.652 | 2.07 ± 0.77 | 2.79 ± 0.96 | 0.000 *** | 3.11 ± 0.96 | 2.47 ± 0.59 | 0.001 ** | ||
| 1st Molar | 4.05 ± 1.36 | 3.55 ± 0.72 | 0.053 | 3.89 ± 1.32 | 4.12 ± 1.13 | 0.427 | 4.37 ± 1.43 | 4.17 ± 1.13 | 0.476 | ||
| 2nd Premolar | 6.92 ± 2.13 | 6.03 ± 1.46 | 0.036 * | 6.62 ± 0.71 | 6.36 ± 1.50 | 0.500 | 6.07 ± 1.88 | 6.09 ± 1.62 | 0.970 | ||
| 1st Premolar | 6.21 ± 0.04 | 6.94 ± 1.43 | 0.235 | 6.82 ± 1.62 | 6.77 ± 1.29 | 0.944 | 7.83 ± 1.49 | 6.71 ± 0.73 | 0.012 * | ||
| ACN | 3rd Molar | 14.94 ± 1.21 | 13.89 ± 1.38 | 0.001 ** | 17.22 ± 2.13 | 16.81 ± 1.99 | 0.386 | 16.83 ± 2.19 | 16.49 ± 2.13 | 0.489 | |
| 2nd Molar | 15.54 ± 1.60 | 14.42 ± 1.73 | 0.004 ** | 18.24 ± 2.38 | 17.68 ± 2.23 | 0.281 | 18.20 ± 2.39 | 17.31 ± 2.26 | 0.094 | ||
| 1st Molar | 15.79 ± 2.55 | 15.40 ± 2.36 | 0.475 | 19.34 ± 2.01 | 17.62 ± 3.02 | 0.003 ** | 19.75 ± 2.30 | 17.97 ± 2.35 | 0.001 ** | ||
| 2nd Premolar | 12.57 ± 1.37 | 12.42 ± 1.32 | 0.626 | 13.45 ± 0.75 | 13.21 ± 0.74 | 0.181 | 13.81 ± 1.23 | 13.78 ± 2.04 | 0.931 | ||
| 1st Premolar | 7.39 ± 0.06 | 9.63 ± 1.14 | 0.000 *** | 10.07 ± 0.58 | 11.50 ± 0.54 | 0.002 ** | 11.14 ± 0.70 | 12.25 ± 2.11 | 0.234 | ||
| Left | BCPN | 3rd Molar | 6.27 ± 1.10 | 6.33 ± 1.27 | 0.837 | 6.44 ± 0.96 | 6.24 ± 0.83 | 0.310 | 6.37 ± 1.11 | 6.60 ± 0.87 | 0.317 |
| 2nd Molar | 5.57 ± 1.21 | 5.45 ± 1.46 | 0.673 | 5.66 ± 0.78 | 5.42 ± 0.82 | 0.186 | 5.53 ± 1.24 | 5.50 ± 0.82 | 0.890 | ||
| 1st Molar | 3.98 ± 1.11 | 3.93 ± 1.30 | 0.0848 | 4.02 ± 0.89 | 3.76 ± 0.81 | 0.168 | 3.97 ± 1.11 | 4.13 ± 1.04 | 0.497 | ||
| 2nd Premolar | 0.99 ± 0.06 | 1.85 ± 0.47 | 0.000 *** | 2.08 ± 0.81 | 1.92 ± 0.58 | 0.471 | 1.72 ± 0.59 | 1.76 ± 0.50 | 0.804 | ||
| 1st Premolar | 0 | 0 | - | 1.60 ± 0.0 | 0 | - | 0 | 0 | - | ||
| LCPN | 3rd Molar | 1.87 ± 0.60 | 1.98 ± 0.59 | 0.398 | 1.73 ± 0.58 | 2.32 ± 2.01 | 0.070 | 2.01 ± 0.62 | 2.07 ± 0.66 | 0.668 | |
| 2nd Molar | 2.32 ± 0.60 | 2.54 ± 0.66 | 0.132 | 2.36 ± 0.64 | 2.63 ± 0.76 | 0.089 | 2.69 ± 0.88 | 2.77 ± 0.62 | 0.640 | ||
| 1st Molar | 3.90 ± 1.11 | 3.52 ± 0.98 | 0.114 | 3.73 ± 0.96 | 4.03 ± 1.07 | 0.183 | 3.93 ± 0.91 | 4.17 ± 1.22 | 0.325 | ||
| 2nd Premolar | 6.76 ± 2.11 | 6.22 ± 0.79 | 0.158 | 6.12 ± 1.65 | 6.07 ± 1.17 | 0.878 | 6.58 ± 1.14 | 6.25 ± 1.17 | 0.828 | ||
| 1st Premolar | 6.10 ± 0.14 | 6.16 ± 1.27 | 0.950 | 6.24 ± 0.73 | 6.78 ± 1.52 | 0.257 | 7.88 ± 0.84 | 7.43 ± 0.65 | 0.109 | ||
| ACN | 3rd Molar | 15.03 ± 1.95 | 13.76 ± 1.77 | 0.003 ** | 16.26 ± 2.47 | 15.94 ± 2.37 | 0.564 | 17.47 ± 2.13 | 16.21 ± 1.84 | 0.007 ** | |
| 2nd Molar | 15.51 ± 2.30 | 14.41 ± 2.37 | 0.039 * | 17.03 ± 2.52 | 16.86 ± 2.36 | 0.758 | 18.37 ± 1.97 | 17.04 ± 2.10 | 0.005 ** | ||
| 1st Molar | 16.05 ± 2.89 | 15.41 ± 2.61 | 0.302 | 17.93 ± 2.69 | 15.94 ± 4.50 | 0.017 * | 19.33 ± 1.98 | 18.19 ± 2.50 | 0.027 * | ||
| 2nd Premolar | 12.41 ± 1.41 | 12.40 ± 1.25 | 0.967 | 13.08 ± 0.83 | 12.92 ± 0.80 | 0.377 | 13.72 ± 1.18 | 13.99 ± 1.76 | 0.417 | ||
| 1st Premolar | 8.85 ± 1.01 | 9.03 ± 1.15 | 0.710 | 10.04 ± 0.80 | 11.30 ± 0.12 | 0.004 ** | 11.50 ± 0.70 | 11.93 ± 1.59 | 0.723 | ||
| Side of Arch | Dimension | Tooth # | Study Group II | Study Group III | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Age Categories | p Value | Age Categories | p Value | |||||||
| 18–35 Years | 36–53 Years | ≥ 54 Years | 18–35 Years | 36–53 Years | ≥ 54 Years | |||||
| Right | BCPN | 3rd Molar | 5.99 ± 1.42 | 5.91 ± 0.89 | 5.83 ± 0.80 | 0.859 | 6.70 ± 1.03 | 6.12 ± 0.83 | 5.56 ± 1.33 | 0.028 * |
| 2nd Molar | 5.30 ± 1.39 | 5.12 ± 0.92 | 5.16 ± 0.82 | 0.808 | 5.62 ± 1.14 | 5.57 ± 1.13 | 4.86 ± 1.31 | 0.032 * | ||
| 1st Molar | 3.66 ± 1.26 | 3.44 ± 1.04 | 3.59 ± 0.70 | 0.633 | 3.82 ± 1.28 | 3.98 ± 1.48 | 3.44 ± 1.22 | 0.283 | ||
| 2nd Premolar | 2.17 ± 0.67 | 2.08 ± 0.45 | 1.67 ± 0.13 | 0.144 | 2.37 ± 1.55 | 2.14 ± 0.96 | 1.76 ± 0.67 | 0.437 | ||
| 1st Premolar | - | - | - | - | - | - | ||||
| LCPN | 3rd Molar | 2.13 ± 0.84 | 1.81 ± 0.66 | 1.56 ± 0.69 | 0.023 * | 2.17 ± 0.74 | 2.10 ± 0.70 | 1.87 ± 0.52 | 0.090 | |
| 2nd Molar | 2.66 ± 0.87 | 2.44 ± 0.97 | 2.14 ± 0.90 | 0.134 | 2.50 ± 0.84 | 2.57 ± 0.59 | 2.43 ± 0.65 | 0.789 | ||
| 1st Molar | 4.20 ± 1.33 | 4.15 ± 1.35 | 3.96 ± 0.97 | 0.09 | 3.86 ± 0.84 | 4.23 ± 1.12 | 3.53 ± 1.24 | 0.063 | ||
| 2nd Premolar | 6.56 ± 1.80 | 6.35 ± 1.64 | 6.16 ± 1.80 | 0.191 | 6.60 ± 1.49 | 6.15 ± 1.49 | 6.24 ± 1.78 | 0.004 ** | ||
| 1st Premolar | 6.83 ± 0.38 | 6.22 ± 0.24 | 6.03 ± 0.38 | 0.04 * | 6.51 ± 0.15 | 6.32 ± 1.61 | 6.06 ± 0.64 | 0.025 * | ||
| ACN | 3rd Molar | 17.52 ± 1.41 | 18.21 ± 1.27 | 15.09 ± 2.13 | 0.000 *** | 16.72 ± 1.33 | 17.44 ± 2.39 | 15.73 ± 2.82 | 0.027 * | |
| 2nd Molar | 17.51 ± 1.57 | 19.27 ± 1.56 | 16.86 ± 2.37 | 0.007 ** | 17.65 ± 1.71 | 18.68 ± 2.34 | 17.04 ± 3.04 | 0.059 | ||
| 1st Molar | 18.14 ± 3.15 | 19.12 ± 1.64 | 17.17 ± 2.04 | 0.000 *** | 18.38 ± 1.83 | 19.34 ± 2.46 | 18.30 ± 2.86 | 0.031 * | ||
| 2nd Premolar | 13.58 ± 0.51 | 13.25 ± 1.02 | 13.16 ± 0.60 | 0.101 | 13.93 ± 2.01 | 13.75 ± 1.61 | 13.61 ± 0.84 | 0.773 | ||
| 1st Premolar | 10.90 ± 0.00 | 10.88 ± 1.11 | 9.55 ± 0.00 | 0.169 | 12.88 ± 2.94 | 11.25 ± 0,82 | 11.50 ± 0.30 | 0.259 | ||
| Left | BCPN | 3rd Molar | 6.28 ± 1.20 | 6.16 ± 0.85 | 6.20 ± 0.61 | 0.310 | 6.60 ± 1.24 | 6.38 ± 0.76 | 6.00 ± 1.31 | 0.093 |
| 2nd Molar | 5.46 ± 0.69 | 5.88 ± 0.85 | 5.27 ± 0.77 | 0.180 | 5.88 ± 1.31 | 5.40 ± 0.94 | 5.28 ± 1.49 | 0.091 | ||
| 1st Molar | 3.94 ± 0.95 | 3.58 ± 0.57 | 3.28 ± 0.57 | 0.028 * | 3.47 ± 1.27 | 3.80 ± 0.99 | 3.25 ± 1.21 | 0.067 | ||
| 2nd Premolar | 1.95 ± 0.50 | 2.06 ± 0.97 | 1.85 ± 0.65 | 0.175 | 1.91 ± 0.67 | 1.66 ± 0.22 | 1.31 ± 0.67 | 0.042 * | ||
| 1st Premolar | - | - | - | - | - | - | - | |||
| LCPN | 3rd Molar | 2.30 ± 0.79 | 2.15 ± 0.71 | 2.11 ± 2.21 | 0.243 | 1.82 ± 0.54 | 1.66 ± 0.64 | 1.42 ± 0.54 | 0.010 * | |
| 2nd Molar | 2.87 ± 0.84 | 2.38 ± 0.72 | 2.25 ± 0.38 | 0.004 ** | 2.93 ± 0.57 | 2.27 ± 0.57 | 2.02 ± 0.57 | 0.002 ** | ||
| 1st Molar | 4.01 ± 1.05 | 3.85 ± 1.14 | 3.76 ± 0.88 | 0.681 | 3.29 ± 0.70 | 4.85 ± 1.09 | 3.18 ± 0.37 | 0.000 *** | ||
| 2nd Premolar | 6.25 ± 0.90 | 6.15 ± 1.59 | 6.05 ± 1.76 | 0.774 | 6.53 ± 0.68 | 6.24 ± 1.54 | 6.08 ± 1.47 | 0.01 * | ||
| 1st Premolar | 6.58 ± 0.00 | 6.22 ± 1.64 | 6.37 ± 0.81 | 0.176 | 6.40 ± 0.82 | 6.11 ± 0.96 | 6.03 ± 0.82 | 0.04 * | ||
| ACN | 3rd Molar | 16.69 ± 1.80 | 17.15 ± 2.36 | 15.22 ± 2.08 | 0.009 ** | 16.76 ± 1.15 | 17.56 ± 2.37 | 16.40 ± 2.79 | 0.152 | |
| 2nd Molar | 17.66 ± 1.74 | 18.00 ± 2.02 | 14.92 ± 2.40 | 0.000 *** | 17.47 ± 2.46 | 17.52 ± 2.43 | 17.45 ± 1.54 | 0.126 | ||
| 1st Molar | 16.36 ± 1.72 | 16.79 ± 5.38 | 15.36 ± 1.72 | 0.366 | 18.59 ± 2.21 | 19.60 ± 0.98 | 18.41 ± 1.61 | 0.128 | ||
| 2nd Premolar | 12.82 ± 0.69 | 13.53 ± 0.56 | 12.82 ± 0.69 | 0.04 * | 14.07 ± 1.72 | 13.63 ± 1.47 | 13.69 ± 0.88 | 0.473 | ||
| 1st Premolar | 10.30 ± 1.22 | 10.22 ± 0.00 | 9.08 ± 1.22 | 0.669 | 12.54 ± 1.65 | 11.91 ± 0.60 | 10.23 ± 0.00 | 0.065 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sghaireen, M.G.; Srivastava, K.C.; Shrivastava, D.; Ganji, K.K.; Patil, S.R.; Abuonq, A.; Mousa, M.A.; Dar-Odeh, N.; Sghaireen, G.M.; Kamal, M.A.; et al. A CBCT Based Three-Dimensional Assessment of Mandibular Posterior Region for Evaluating the Possibility of Bypassing the Inferior Alveolar Nerve While Placing Dental Implants. Diagnostics 2020, 10, 406. https://doi.org/10.3390/diagnostics10060406
Sghaireen MG, Srivastava KC, Shrivastava D, Ganji KK, Patil SR, Abuonq A, Mousa MA, Dar-Odeh N, Sghaireen GM, Kamal MA, et al. A CBCT Based Three-Dimensional Assessment of Mandibular Posterior Region for Evaluating the Possibility of Bypassing the Inferior Alveolar Nerve While Placing Dental Implants. Diagnostics. 2020; 10(6):406. https://doi.org/10.3390/diagnostics10060406
Chicago/Turabian StyleSghaireen, Mohammed G., Kumar Chandan Srivastava, Deepti Shrivastava, Kiran Kumar Ganji, Santosh R. Patil, Anas Abuonq, Mohammed Assayed Mousa, Najla Dar-Odeh, Ghazi M. Sghaireen, Mohammad Amjad Kamal, and et al. 2020. "A CBCT Based Three-Dimensional Assessment of Mandibular Posterior Region for Evaluating the Possibility of Bypassing the Inferior Alveolar Nerve While Placing Dental Implants" Diagnostics 10, no. 6: 406. https://doi.org/10.3390/diagnostics10060406