

Neuropancreatology: The Nervous System and Pain Management in Pancreatic Diseases

 , , , and
, , , and
Abstract
:1. Introduction
2. Anatomy and Physiology of the Pancreatic Nervous System
2.1. Spinal and Vagal Sensory Afferent Fibers
2.2. Sympathetic and Parasympathetic Autonomic Fibers
2.3. Fibers from the Enteric Nervous System (ENS)
2.4. Intrapancreatic Ganglia
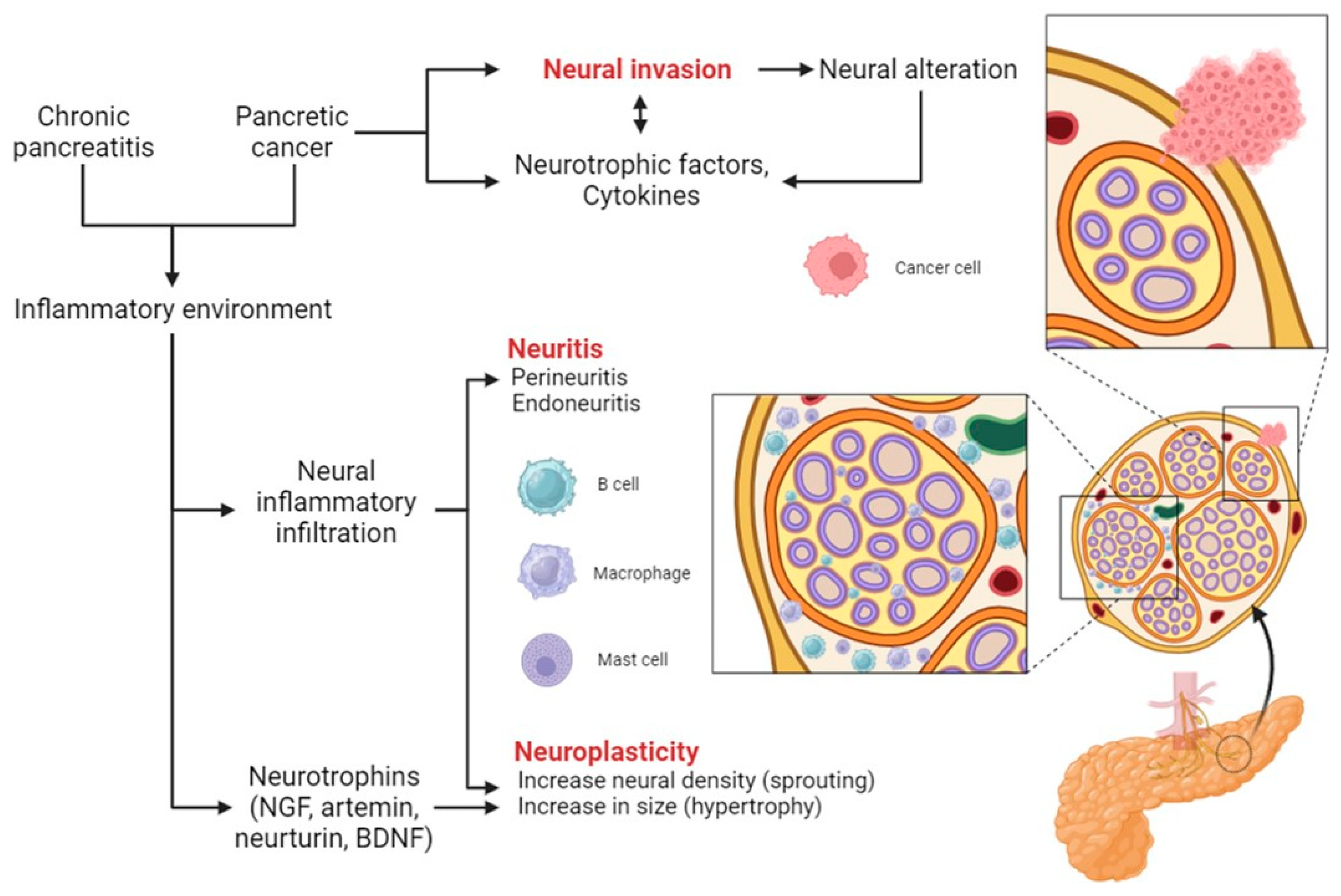
3. Neuroplasticity and Neural Invasion
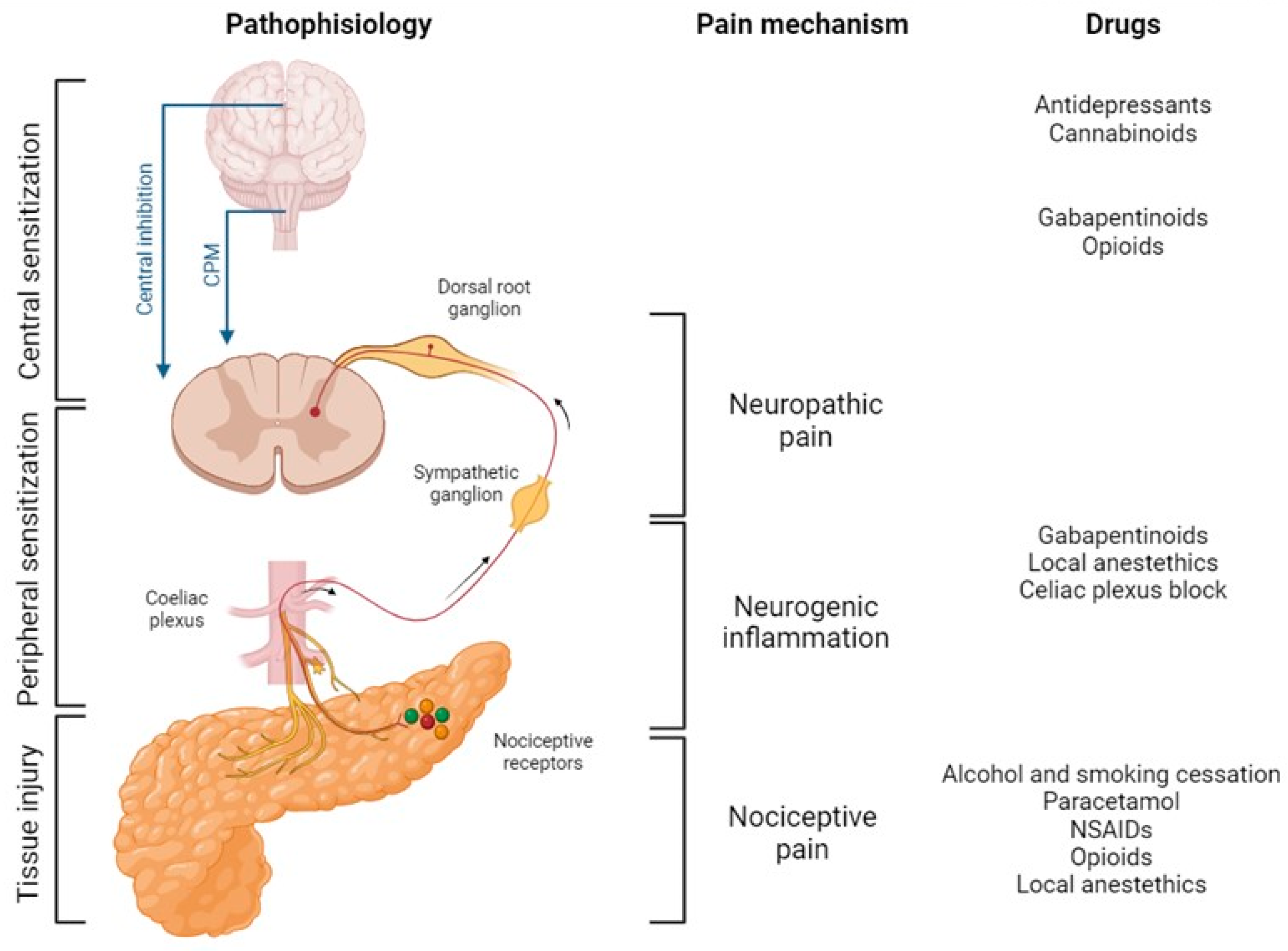
4. Pathophysiology of Pancreatic Pain
5. Lifestyle, Pharmacological, and Interventional Management of Pain in Pancreatic Diseases
5.1. Treatment of Complications
5.2. Lifestyle Interventions
5.2.1. Diet
5.2.2. Alcohol and Smoking Cessation
5.3. Pharmacological Strategies
5.3.1. Pancreatic Enzyme Replacement Therapy (PERT)
5.3.2. Paracetamol
5.3.3. Non-Steroidal Anti-Inflammatory Drugs (NSAIDs)
5.3.4. Opioids
5.3.5. Gabapentinoids
5.3.6. Local Anesthetics
5.3.7. Antidepressants
5.3.8. Cannabinoids
5.4. Interventional Approaches
5.4.1. Epidural Analgesia
5.4.2. Celiac Plexus Block (CPB)
5.4.3. Spinal Cord Stimulation
6. Future Trends in Neuropancreatology: Pharmacological Neuromodulation
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Iannuzzi, J.P.; King, J.A.; Leong, J.H.; Quan, J.; Windsor, J.W.; Tanyingoh, D.; Coward, S.; Forbes, N.; Heitman, S.J.; Shaheen, A.-A.; et al. Global Incidence of Acute Pancreatitis Is Increasing Over Time: A Systematic Review and Meta-Analysis. Gastroenterology 2022, 162, 122–134. [Google Scholar] [CrossRef]
- GBD2017 Pancreatic Cancer Collaborators. The global, regional, and national burden of pancreatic cancer and its attributable risk factors in 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2019, 4, 934–947. [Google Scholar] [CrossRef]
- Huang, J.; Lok, V.; Ngai, C.H.; Zhang, L.; Yuan, J.; Lao, X.Q.; Ng, K.; Chong, C.; Zheng, Z.-J.; Wong, M.C. Worldwide Burden of, Risk Factors for, and Trends in Pancreatic Cancer. Gastroenterology 2021, 160, 744–754. [Google Scholar] [CrossRef]
- Li, W.; Yu, G.; Liu, Y.; Sha, L. Intrapancreatic Ganglia and Neural Regulation of Pancreatic Endocrine Secretion. Front. Neurosci. 2019, 13, 21. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Diaz, R.; Caicedo, A. Neural control of the endocrine pancreas. Best Pract. Res. Clin. Endocrinol. Metab. 2014, 28, 745–756. [Google Scholar] [CrossRef]
- Love, J.A.; Yi, E.; Smith, T.G. Autonomic pathways regulating pancreatic exocrine secretion. Auton. Neurosci. 2007, 133, 19–34. [Google Scholar] [CrossRef]
- Makhmutova, M.; Caicedo, A. Optical Imaging of Pancreatic Innervation. Front. Endocrinol. 2021, 12, 663022. [Google Scholar] [CrossRef]
- Chandra, R.; Liddle, R.A. Modulation of pancreatic exocrine and endocrine secretion. Curr. Opin. Gastroenterol. 2013, 29, 517–522. [Google Scholar] [CrossRef] [PubMed]
- Ceyhan, G.O.; Michalski, C.W.; Demir, I.E.; Müller, M.W.; Friess, H. Pancreatic pain. Best Pract. Res. Clin. Gastroenterol. 2008, 22, 31–44. [Google Scholar] [CrossRef]
- Boxhoorn, L.; Voermans, R.P.; Bouwense, S.A.; Bruno, M.J.; Verdonk, R.C.; Boermeester, M.A.; van Santvoort, H.C.; Besselink, M.G. Acute pancreatitis. Lancet 2020, 396, 726–734. [Google Scholar] [CrossRef] [PubMed]
- Mederos, M.A.; Reber, H.A.; Girgis, M.D. Acute Pancreatitis: A Review. JAMA 2021, 325, 382–390. [Google Scholar] [CrossRef] [PubMed]
- Bapat, A.A.; Hostetter, G.; Von Hoff, D.D.; Han, H. Perineural invasion and associated pain in pancreatic cancer. Nat. Rev. Cancer 2011, 11, 695–707. [Google Scholar] [CrossRef] [PubMed]
- Greenwald, H.P.; Bonica, J.J.; Bergner, M. The prevalence of pain in four cancers. Cancer 1987, 60, 2563–2569. [Google Scholar] [CrossRef] [PubMed]
- Krech, R.L.; Walsh, D. Symptoms of pancreatic cancer. J. Pain Symptom Manag. 1991, 6, 360–367. [Google Scholar] [CrossRef] [PubMed]
- Caban, M.; Małecka-Wojciesko, E. Gaps and Opportunities in the Diagnosis and Treatment of Pancreatic Cancer. Cancers 2023, 15, 5577. [Google Scholar] [CrossRef] [PubMed]
- Yadav, D.; Askew, R.L.; Palermo, T.; Li, L.; Andersen, D.K.; Chen, M.; Fisher, W.E.; Fogel, E.L.; Forsmark, C.E.; Hart, P.A.; et al. Association of Chronic Pancreatitis Pain Features With Physical, Mental, and Social Health. Clin. Gastroenterol. Hepatol. 2022, 21, 1781–1791.e1784. [Google Scholar] [CrossRef] [PubMed]
- Damm, M.; Weniger, M.; Kölsch, A.-K.; Lampert, C.; Ceyhan, G.O.; Beer, S.; Schorn, S.; Moir, J.; Michl, P.; Rosendahl, J. The quality of pain management in pancreatic cancer: A prospective multi-center study. Pancreatology 2020, 20, 1511–1518. [Google Scholar] [CrossRef]
- Cai, W.; Liu, F.; Wen, Y.; Han, C.; Prasad, M.; Xia, Q.; Singh, V.K.; Sutton, R.; Huang, W. Pain Management in Acute Pancreatitis: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Front. Med. 2021, 8, 782151. [Google Scholar] [CrossRef]
- Pérez-Aguado, G.; de la Mata, D.M.-A.; Valenciano, C.M.-L.; Sainz, I.F.-U. Endoscopic ultrasonography-guided celiac plexus neurolysis in patients with unresectable pancreatic cancer: An update. World J. Gastrointest. Endosc. 2021, 13, 460–472. [Google Scholar] [CrossRef]
- Drewes, A.M.; Bouwense, S.A.W.; Campbell, C.M.; Ceyhan, G.O.; Delhaye, M.; Demir, I.E.; Garg, P.K.; van Goor, H.; Halloran, C.; Isaji, S.; et al. Guidelines for the understanding and management of pain in chronic pancreatitis. Pancreatology 2017, 17, 720–731. [Google Scholar] [CrossRef]
- Lkhagvasuren, B.; Mee-Inta, O.; Zhao, Z.-W.; Hiramoto, T.; Boldbaatar, D.; Kuo, Y.-M. Pancreas-Brain Crosstalk. Front. Neuroanat. 2021, 15, 691777. [Google Scholar] [CrossRef] [PubMed]
- Renehan, W.E.; Zhang, X.; Beierwaltes, W.H.; Fogel, R. Neurons in the dorsal motor nucleus of the vagus may integrate vagal and spinal information from the GI tract. Am. J. Physiol. 1995, 268, G780–G790. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, T.H.; Halvorson, K.G.; Peters, C.M.; Ghilardi, J.R.; Kuskowski, M.A.; Wong, G.Y.; Mantyh, P.W. A quantitative analysis of the sensory and sympathetic innervation of the mouse pancreas. Neuroscience 2006, 137, 1417–1426. [Google Scholar] [CrossRef]
- Barreto, S.G.; Saccone, G.T. Pancreatic nociception—Revisiting the physiology and pathophysiology. Pancreatology 2012, 12, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Nathan, J.D.; Peng, R.Y.; Wang, Y.; McVey, D.C.; Vigna, S.R.; Liddle, R.A. Primary sensory neurons: A common final pathway for inflammation in experimental pancreatitis in rats. Am. J. Physiol.-Gastrointest. Liver Physiol. 2002, 283, G938–G946. [Google Scholar] [CrossRef]
- Liu, L.; Shenoy, M.; Pasricha, P.J. Substance P and calcitonin gene related peptide mediate pain in chronic pancreatitis and their expression is driven by nerve growth factor. JOP 2011, 12, 389–394. [Google Scholar]
- Payne, S.C.; Ward, G.; MacIsaac, R.J.; Hyakumura, T.; Fallon, J.B.; Villalobos, J. Differential effects of vagus nerve stimulation strategies on glycemia and pancreatic secretions. Physiol. Rep. 2020, 8, e14479. [Google Scholar] [CrossRef]
- Quinson, N.; Robbins, H.L.; Clark, M.J.; Furness, J.B. Locations and innervation of cell bodies of sympathetic neurons projecting to the gastrointestinal tract in the rat. Arch. Histol. Cytol. 2001, 64, 281–294. [Google Scholar] [CrossRef]
- Jansen, A.S.; Hoffman, J.L.; Loewy, A.D. CNS sites involved in sympathetic and parasympathetic control of the pancreas: A viral tracing study. Brain Res. 1997, 766, 29–38. [Google Scholar] [CrossRef]
- Borden, P.; Houtz, J.; Leach, S.D.; Kuruvilla, R. Sympathetic innervation during development is necessary for pancreatic islet architecture and functional maturation. Cell Rep. 2013, 4, 287–301. [Google Scholar] [CrossRef]
- Morton, G.J.; Muta, K.; Kaiyala, K.J.; Rojas, J.M.; Scarlett, J.M.; Matsen, M.E.; Nelson, J.T.; Acharya, N.K.; Piccinini, F.; Stefanovski, D.; et al. Evidence That the Sympathetic Nervous System Elicits Rapid, Coordinated, and Reciprocal Adjustments of Insulin Secretion and Insulin Sensitivity During Cold Exposure. Diabetes 2017, 66, 823–834. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Diaz, R.; Abdulreda, M.H.; Formoso, A.L.; Gans, I.; Ricordi, C.; Berggren, P.-O.; Caicedo, A. Innervation patterns of autonomic axons in the human endocrine pancreas. Cell Metab. 2011, 14, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Molina, J.; Rodriguez-Diaz, R.; Fachado, A.; Jacques-Silva, M.C.; Berggren, P.-O.; Caicedo, A. Control of insulin secretion by cholinergic signaling in the human pancreatic islet. Diabetes 2014, 63, 2714–2726. [Google Scholar] [CrossRef] [PubMed]
- Di Cairano, E.S.; Moretti, S.; Marciani, P.; Sacchi, V.F.; Castagna, M.; Davalli, A.; Folli, F.; Perego, C. Neurotransmitters and Neuropeptides: New Players in the Control of Islet of Langerhans’ Cell Mass and Function. J. Cell Physiol. 2016, 231, 756–767. [Google Scholar] [CrossRef] [PubMed]
- Powley, T.L.; Spaulding, R.A.; Haglof, S.A. Vagal afferent innervation of the proximal gastrointestinal tract mucosa: Chemoreceptor and mechanoreceptor architecture. J. Comp. Neurol. 2011, 519, 644–660. [Google Scholar] [CrossRef] [PubMed]
- Kirchgessner, A.; Gershon, M.D. Innervation of the pancreas by neurons in the gut. J. Neurosci. 1990, 10, 1626–1642. [Google Scholar] [CrossRef] [PubMed]
- Kirchgessner, A.L.; Gershon, M.D. Presynaptic inhibition by serotonin of nerve-mediated secretion of pancreatic amylase. Am. J. Physiol. 1995, 268, G339–G345. [Google Scholar] [CrossRef]
- Tang, S.-C.; Baeyens, L.; Shen, C.-N.; Peng, S.-J.; Chien, H.-J.; Scheel, D.W.; Chamberlain, C.E.; German, M.S. Human pancreatic neuro-insular network in health and fatty infiltration. Diabetologia 2018, 61, 168–181. [Google Scholar] [CrossRef]
- Krivova, Y.; Proshchina, A.; Barabanov, V.; Leonova, O.; Saveliev, S. Structure of neuro-endocrine and neuro-epithelial interactions in human foetal pancreas. Tissue Cell 2016, 48, 567–576. [Google Scholar] [CrossRef]
- Yi, E.; Smith, T.G.; Baker, R.C.; Love, J.A. Catecholamines and 5-hydroxytryptamine in tissues of the rabbit exocrine pancreas. Pancreas 2004, 29, 218–224. [Google Scholar] [CrossRef]
- Demir, I.E.; Friess, H.; Ceyhan, G.O. Neural plasticity in pancreatitis and pancreatic cancer. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 649–659. [Google Scholar] [CrossRef]
- Ceyhan, G.O.; Bergmann, F.; Kadihasanoglu, M.; Altintas, B.; Demir, I.E.; Hinz, U.; Müller, M.W.; Giese, T.; Büchler, M.W.; Giese, N.A.; et al. Pancreatic neuropathy and neuropathic pain--a comprehensive pathomorphological study of 546 cases. Gastroenterology 2009, 136, 177–186.e171. [Google Scholar] [CrossRef]
- Demir, I.E.; Friess, H.; Ceyhan, G.O. Nerve-cancer interactions in the stromal biology of pancreatic cancer. Front. Physiol. 2012, 3, 97. [Google Scholar] [CrossRef] [PubMed]
- Elitt, C.M.; McIlwrath, S.L.; Lawson, J.J.; Malin, S.A.; Molliver, D.C.; Cornuet, P.K.; Koerber, H.R.; Davis, B.M.; Albers, K.M. Artemin overexpression in skin enhances expression of TRPV1 and TRPA1 in cutaneous sensory neurons and leads to behavioral sensitivity to heat and cold. J. Neurosci. 2006, 26, 8578–8587. [Google Scholar] [CrossRef]
- Wang, K.; Demir, I.E.; D’haese, J.G.; Tieftrunk, E.; Kujundzic, K.; Schorn, S.; Xing, B.; Kehl, T.; Friess, H.; Ceyhan, G.O. The neurotrophic factor neurturin contributes toward an aggressive cancer cell phenotype, neuropathic pain and neuronal plasticity in pancreatic cancer. Carcinogenesis 2014, 35, 103–113. [Google Scholar] [CrossRef]
- Ceyhan, G.O.; Bergmann, F.; Kadihasanoglu, M.; Erkan, M.; Park, W.; Hinz, U.; Giese, T.; Müller, M.W.; Büchler, M.W.; Giese, N.A.; et al. The neurotrophic factor artemin influences the extent of neural damage and growth in chronic pancreatitis. Gut 2007, 56, 534–544. [Google Scholar] [CrossRef] [PubMed]
- Demir, I.E.; Schorn, S.; Schremmer-Danninger, E.; Wang, K.; Kehl, T.; Giese, N.A.; Algül, H.; Friess, H.; Ceyhan, G.O. Perineural mast cells are specifically enriched in pancreatic neuritis and neuropathic pain in pancreatic cancer and chronic pancreatitis. PLoS ONE 2013, 8, e60529. [Google Scholar] [CrossRef] [PubMed]
- Bauer, O.; Razin, E. Mast Cell-Nerve Interactions. News Physiol. Sci. 2000, 15, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Stead, R.H.; Tomioka, M.; Quinonez, G.; Simon, G.T.; Felten, S.Y.; Bienenstock, J. Intestinal mucosal mast cells in normal and nematode-infected rat intestines are in intimate contact with peptidergic nerves. Proc. Natl. Acad. Sci. USA 1987, 84, 2975–2979. [Google Scholar] [CrossRef]
- Barbara, G.; Stanghellini, V.; De Giorgio, R.; Cremon, C.; Cottrell, G.S.; Santini, D.; Pasquinelli, G.; Morselli-Labate, A.M.; Grady, E.F.; Bunnett, N.W.; et al. Activated mast cells in proximity to colonic nerves correlate with abdominal pain in irritable bowel syndrome. Gastroenterology 2004, 126, 693–702. [Google Scholar] [CrossRef]
- Di Sebastiano, P.; di Mola, F.F.; Di Febbo, C.; Baccante, G.; Porreca, E.; Innocenti, P.; Friess, H.; Büchler, M.W. Expression of interleukin 8 (IL-8) and substance P in human chronic pancreatitis. Gut 2000, 47, 423–428. [Google Scholar] [CrossRef]
- Olesen, S.S.; Brock, C.; Krarup, A.L.; Funch–Jensen, P.; Arendt–Nielsen, L.; Wilder–Smith, O.H.; Drewes, A.M. Descending inhibitory pain modulation is impaired in patients with chronic pancreatitis. Clin. Gastroenterol. Hepatol. 2010, 8, 724–730. [Google Scholar] [CrossRef] [PubMed]
- Olesen, S.S.; Hansen, T.M.; Graversen, C.; Steimle, K.; Wilder-Smith, O.H.; Drewes, A.M. Slowed EEG rhythmicity in patients with chronic pancreatitis: Evidence of abnormal cerebral pain processing? Eur. J. Gastroenterol. Hepatol. 2011, 23, 418–424. [Google Scholar] [CrossRef] [PubMed]
- de Vries, M.; Wilder-Smith, O.H.; Jongsma, M.L.; van den Broeke, E.N.; Arns, M.; van Goor, H.; van Rijn, C.M. Altered resting state EEG in chronic pancreatitis patients: Toward a marker for chronic pain. J. Pain Res. 2013, 6, 815–824. [Google Scholar] [CrossRef] [PubMed]
- Olesen, S.; Hansen, T.; Graversen, C.; Valeriani, M.; Drewes, A. Cerebral excitability is abnormal in patients with painful chronic pancreatitis. Eur. J. Pain 2013, 17, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Olesen, S.S.; Frøkjær, J.B.; Lelic, D.; Valeriani, M.; Drewes, A.M. Pain-associated adaptive cortical reorganisation in chronic pancreatitis. Pancreatology 2010, 10, 742–751. [Google Scholar] [CrossRef] [PubMed]
- Lelic, D.; Olesen, S.S.; Hansen, T.M.; Valeriani, M.; Drewes, A.M. Functional reorganization of brain networks in patients with painful chronic pancreatitis. Eur. J. Pain 2014, 18, 968–977. [Google Scholar] [CrossRef]
- Frokjaer, J.B.; Olesen, S.S.; Gram, M.; Yavarian, Y.; Bouwense, S.A.W.; Wilder-Smith, O.H.G.; Drewes, A.M. Altered brain microstructure assessed by diffusion tensor imaging in patients with chronic pancreatitis. Gut 2011, 60, 1554–1562. [Google Scholar] [CrossRef]
- Frøkjær, J.B.; Bouwense, S.A.; Olesen, S.S.; Lundager, F.H.; Eskildsen, S.F.; van Goor, H.; Wilder–Smith, O.H.; Drewes, A.M. Reduced cortical thickness of brain areas involved in pain processing in patients with chronic pancreatitis. Clin. Gastroenterol. Hepatol. 2012, 10, 434–438.e431. [Google Scholar] [CrossRef]
- Magnon, C.; Hall, S.J.; Lin, J.; Xue, X.; Gerber, L.; Freedland, S.J.; Frenette, P.S. Autonomic nerve development contributes to prostate cancer progression. Science 2013, 341, 1236361. [Google Scholar] [CrossRef]
- Zhao, C.-M.; Hayakawa, Y.; Kodama, Y.; Muthupalani, S.; Westphalen, C.B.; Andersen, G.T.; Flatberg, A.; Johannessen, H.; Friedman, R.A.; Renz, B.W.; et al. Denervation suppresses gastric tumorigenesis. Sci. Transl. Med. 2014, 6, 250ra115. [Google Scholar] [CrossRef] [PubMed]
- Pour, P.M.; Bell, R.H.; Batra, S.K. Neural invasion in the staging of pancreatic cancer. Pancreas 2003, 26, 322–325. [Google Scholar] [CrossRef] [PubMed]
- Demir, I.E.; Ceyhan, G.O.; Liebl, F.; D’haese, J.G.; Maak, M.; Friess, H. Neural invasion in pancreatic cancer: The past, present and future. Cancers 2010, 2, 1513–1527. [Google Scholar] [CrossRef]
- Bockman, D.E.; Büchler, M.; Beger, H.G. Interaction of pancreatic ductal carcinoma with nerves leads to nerve damage. Gastroenterology 1994, 107, 219–230. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.-W.; Friess, H.; Wang, L.; Zimmermann, A.; Bũchler, M.W. Brain-derived neurotrophic factor (BDNF) is upregulated and associated with pain in chronic pancreatitis. Dig. Dis. Sci. 2001, 46, 1633–1639. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.; Friess, H.; Dimola, F.F.; Zimmermann, A.; Graber, H.U.; Korc, M.; Büchler, M.W. Nerve growth factor expression correlates with perineural invasion and pain in human pancreatic cancer. J. Clin. Oncol. 1999, 17, 2419–2428. [Google Scholar] [CrossRef]
- Gil, Z.; Cavel, O.; Kelly, K.; Brader, P.; Rein, A.; Gao, S.P.; Carlson, D.L.; Shah, J.P.; Fong, Y.; Wong, R.J. Paracrine regulation of pancreatic cancer cell invasion by peripheral nerves. J. Natl. Cancer Inst. 2010, 102, 107–118. [Google Scholar] [CrossRef]
- Airaksinen, M.S.; Saarma, M. The GDNF family: Signalling, biological functions and therapeutic value. Nat. Rev. Neurosci. 2002, 3, 383–394. [Google Scholar] [CrossRef]
- Marchesi, F.; Piemonti, L.; Fedele, G.; Destro, A.; Roncalli, M.; Albarello, L.; Doglioni, C.; Anselmo, A.; Doni, A.; Bianchi, P.; et al. The chemokine receptor CX3CR1 is involved in the neural tropism and malignant behavior of pancreatic ductal adenocarcinoma. Cancer Res 2008, 68, 9060–9069. [Google Scholar] [CrossRef]
- Ali, U.A.; Nieuwenhuijs, V.B.; van Eijck, C.H.; Gooszen, H.G.; van Dam, R.M.; Busch, O.R.; Dijkgraaf, M.G.; Mauritz, F.A.; Jens, S.; Mast, J.; et al. Clinical outcome in relation to timing of surgery in chronic pancreatitis: A nomogram to predict pain relief. Arch. Surg. 2012, 147, 925–932. [Google Scholar] [CrossRef]
- Moran, R.A.; Sinha, A.; Chen, P.H.; Quesada-Vázquez, N.; Hernaez, R.; Hirose, K.; Makary, M.A.; Khashab, M.; Kalloo, A.N.; Singh, V.K. Tu1492 characteristics and predictors of large duct chronic calcific pancreatitis: A cross sectional analysis from a tertiary referral center. Gastroenterology 2015, 148, S-908. [Google Scholar] [CrossRef]
- Ebbehøj, N.; Borly, L.; Madsen, P.; Svendsen, L.B. Pancreatic tissue pressure and pain in chronic pancreatitis. Pancreas 1986, 1, 556–558. [Google Scholar] [CrossRef] [PubMed]
- Ebbehøj, N.; Borly, L.; Bülow, J.; Rasmussen, S.G.; Madsen, P. Evaluation of pancreatic tissue fluid pressure and pain in chronic pancreatitis. A longitudinal study. Scand. J. Gastroenterol. 1990, 25, 462–466. [Google Scholar] [CrossRef] [PubMed]
- Díte, P.; Ružicka, M.; Zboril, V.; Novotný, I. A prospective, randomized trial comparing endoscopic and surgical therapy for chronic pancreatitis. Endoscopy 2003, 35, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Alles, S.R.A.; Smith, P.A. Etiology and Pharmacology of Neuropathic Pain. Pharmacol. Rev. 2018, 70, 315–347. [Google Scholar] [CrossRef] [PubMed]
- Liddle, R.A.; Nathan, J.D. Neurogenic inflammation and pancreatitis. Pancreatology 2004, 4, 551–559; discussion 559–560. [Google Scholar] [CrossRef] [PubMed]
- Vera-Portocarrero, L.; Westlund, K.N. Role of neurogenic inflammation in pancreatitis and pancreatic pain. Neurosignals 2005, 14, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Weihe, E.; Nohr, D.; Müller, S.; Büchler, M.; Friess, H.; Zentel, H. The tachykinin neuroimmune connection in inflammatory pain. Ann. N. Y. Acad. Sci. 1991, 632, 283–295. [Google Scholar] [CrossRef]
- Shrikhande, S.V.; Friess, H.; di Mola, F.F.; Tempia-Caliera, A.; Garcia, J.R.C.; Zhu, Z.; Zimmermann, A.; Büchler, M.W. NK-1 receptor gene expression is related to pain in chronic pancreatitis. Pain 2001, 91, 209–217. [Google Scholar] [CrossRef]
- Michalski, C.W.; Shi, X.; Reiser, C.; Fachinger, P.; Zimmermann, A.; Büchler, M.W.; Di Sebastiano, P.; Friess, H. Neurokinin-2 receptor levels correlate with intensity, frequency, and duration of pain in chronic pancreatitis. Ann. Surg. 2007, 246, 786–793. [Google Scholar] [CrossRef]
- Friess, H.; Zhu, Z.-W.; di Mola, F.F.; Kulli, C.; Graber, H.U.; Andren-Sandberg, A.; Zimmermann, A.; Korc, M.; Reinshagen, M.; Büchler, M.W. Nerve growth factor and its high-affinity receptor in chronic pancreatitis. Ann. Surg. 1999, 230, 615–624. [Google Scholar] [CrossRef]
- Pasricha, P.J. Unraveling the mystery of pain in chronic pancreatitis. Nat. Rev. Gastroenterol. Hepatol. 2012, 9, 140–151. [Google Scholar] [CrossRef]
- Knowles, C.H.; Aziz, Q. Basic and clinical aspects of gastrointestinal pain. Pain 2009, 141, 191–209. [Google Scholar] [CrossRef] [PubMed]
- Fregni, F.; Pascual-Leone, A.; Freedman, S.D. Pain in chronic pancreatitis: A salutogenic mechanism or a maladaptive brain response? Pancreatology 2007, 7, 411–422. [Google Scholar] [CrossRef] [PubMed]
- Rattner, D.W.; Fernandez-del Castillo, C.; Warshaw, A.L. Pitfalls of distal pancreatectomy for relief of pain in chronic pancreatitis. Am. J. Surg. 1996, 171, 142–145; discussion 145–146. [Google Scholar] [CrossRef] [PubMed]
- Ikeura, T.; Kataoka, Y.; Wakabayashi, T.; Mori, T.; Takamori, Y.; Takamido, S.; Okazaki, K.; Yamada, H. Effects of sensory denervation by neonatal capsaicin administration on experimental pancreatitis induced by dibutyltin dichloride. Med. Mol. Morphol. 2007, 40, 141–149. [Google Scholar] [CrossRef]
- Bouwense, S.A.; De Vries, M.; Schreuder, L.T.; Olesen, S.S.; Frøkjær, J.B.; Drewes, A.; van Goor, H.; Wilder-Smith, O.H. Systematic mechanism-orientated approach to chronic pancreatitis pain. World J. Gastroenterol. 2015, 21, 47–59. [Google Scholar] [CrossRef] [PubMed]
- Wilder-Smith, O.H. A Paradigm-Shift in Pain Medicine; River Publishers: Chicago, IL, USA, 2013. [Google Scholar]
- Ducreux, M.; Cuhna, A.S.; Caramella, C.; Hollebecque, A.; Burtin, P.; Goéré, D.; Seufferlein, T.; Haustermans, K.; Van Laethem, J.L.; Conroy, T.; et al. Cancer of the pancreas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2015, 26 (Suppl. S5), v56–v68. [Google Scholar] [CrossRef] [PubMed]
- Jadad, A.R.; Browman, G.P. The WHO analgesic ladder for cancer pain management. Stepping up the quality of its evaluation. JAMA 1995, 274, 1870–1873. [Google Scholar] [CrossRef] [PubMed]
- Ushe, T.; Lakhan, S.E.; Locklear, T.; Muthukattil, R.; Whitehead, P.; Benson, A.; Ladak, A.A.; Carter, K.F. Pain management consultation for acute pancreatitis: Impact on length of stay and opioid utilization. Pain Manag. 2022, 12, 159–166. [Google Scholar] [CrossRef]
- Working Group IAP/APA Acute Pancreatitis Guidelines. IAP/APA evidence-based guidelines for the management of acute pancreatitis. Pancreatology 2013, 13, e1–e15. [Google Scholar] [CrossRef]
- Arvanitakis, M.; Ockenga, J.; Bezmarevic, M.; Gianotti, L.; Krznarić, Ž.; Lobo, D.N.; Löser, C.; Madl, C.; Meier, R.; Phillips, M.; et al. ESPEN guideline on clinical nutrition in acute and chronic pancreatitis. Clin. Nutr. 2020, 39, 612–631. [Google Scholar] [CrossRef] [PubMed]
- Horibe, M.; Nishizawa, T.; Suzuki, H.; Minami, K.; Yahagi, N.; Iwasaki, E.; Kanai, T. Timing of oral refeeding in acute pancreatitis: A systematic review and meta-analysis. United Eur. Gastroenterol. J. 2015, 4, 725–732. [Google Scholar] [CrossRef]
- Ramírez-Maldonado, E.; Gordo, S.L.; Pueyo, E.M.; Sánchez-García, A.; Mayol, S.; González, S.; Elvira, J.; Memba, R.; Fondevila, C.; Jorba, R. Immediate Oral Refeeding in Patients With Mild and Moderate Acute Pancreatitis: A Multicenter, Randomized Controlled Trial (PADI trial). Ann. Surg. 2021, 274, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Bevan, M.G.; Asrani, V.M.; Bharmal, S.; Wu, L.M.; Windsor, J.A.; Petrov, M.S. Incidence and predictors of oral feeding intolerance in acute pancreatitis: A systematic review, meta-analysis, and meta-regression. Clin. Nutr. 2017, 36, 722–729. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Midha, S.; Singh, N.; Joshi, Y.K.; Garg, P.K. Dietary counseling versus dietary supplements for malnutrition in chronic pancreatitis: A randomized controlled trial. Clin. Gastroenterol. Hepatol. 2008, 6, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Löhr, J.M.; Dominguez-Munoz, E.; Rosendahl, J.; Besselink, M.; Mayerle, J.; Lerch, M.M.; Haas, S.; Akisik, F.; Kartalis, N.; Iglesias-Garcia, J.; et al. United European Gastroenterology evidence-based guidelines for the diagnosis and therapy of chronic pancreatitis (HaPanEU). United Eur. Gastroenterol. J. 2017, 5, 153–199. [Google Scholar] [CrossRef]
- Muscaritoli, M.; Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN practical guideline: Clinical Nutrition in cancer. Clin. Nutr. 2021, 40, 2898–2913. [Google Scholar] [CrossRef]
- Samokhvalov, A.V.; Rehm, J.; Roerecke, M. Alcohol Consumption as a Risk Factor for Acute and Chronic Pancreatitis: A Systematic Review and a Series of Meta-analyses. EBioMedicine 2015, 2, 1996–2002. [Google Scholar] [CrossRef]
- Yuhara, H.; Ogawa, M.; Kawaguchi, Y.; Igarashi, M.; Mine, T. Smoking and risk for acute pancreatitis: A systematic review and meta-analysis. Pancreas 2014, 43, 1201–1207. [Google Scholar] [CrossRef]
- Alexandre, M.; Pandol, S.J.; Gorelick, F.S.; Thrower, E.C. The emerging role of smoking in the development of pancreatitis. Pancreatology 2011, 11, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Nikkola, J.; Räty, S.; Laukkarinen, J.; Seppänen, H.; Lappalainen-Lehto, R.; Järvinen, S.; Nordback, I.; Sand, J. Abstinence after first acute alcohol-associated pancreatitis protects against recurrent pancreatitis and minimizes the risk of pancreatic dysfunction. Alcohol Alcohol. 2013, 48, 483–486. [Google Scholar] [CrossRef] [PubMed]
- Edderkaoui, M.; Thrower, E. Smoking and Pancreatic Disease. J. Cancer Ther. 2013, 4, 34–40. [Google Scholar] [CrossRef]
- de la Iglesia, D.; Avci, B.; Kiriukova, M.; Panic, N.; Bozhychko, M.; Sandru, V.; de Madaria, E.; Capurso, G. Pancreatic exocrine insufficiency and pancreatic enzyme replacement therapy in patients with advanced pancreatic cancer: A systematic review and meta-analysis. United Eur. Gastroenterol. J. 2020, 8, 1115–1125. [Google Scholar] [CrossRef] [PubMed]
- Thavanesan, N.; White, S.; Lee, S.; Ratnayake, B.; Oppong, K.W.; Nayar, M.K.; Sharp, L.; Drewes, A.M.; Capurso, G.; De-Madaria, E.; et al. Analgesia in the Initial Management of Acute Pancreatitis: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. World J. Surg. 2022, 46, 878–890. [Google Scholar] [CrossRef]
- Puylaert, M.; Kapural, L.; Van Zundert, J.; Peek, D.; Lataster, A.; Mekhail, N.; van Kleef, M.; Keulemans, Y.C.A. 26. Pain in chronic pancreatitis. Pain Pract. 2011, 11, 492–505. [Google Scholar] [CrossRef]
- Leppäniemi, A.; Tolonen, M.; Tarasconi, A.; Segovia-Lohse, H.; Gamberini, E.; Kirkpatrick, A.W.; Ball, C.G.; Parry, N.; Sartelli, M.; Wolbrink, D.; et al. 2019 WSES guidelines for the management of severe acute pancreatitis. World J. Emerg. Surg. 2019, 14, 27. [Google Scholar] [CrossRef] [PubMed]
- Stein, C. Opioid Receptors. Annu. Rev. Med. 2016, 67, 433–451. [Google Scholar] [CrossRef] [PubMed]
- Stein, C.; Machelska, H. Modulation of peripheral sensory neurons by the immune system: Implications for pain therapy. Pharmacol. Rev. 2011, 63, 860–881. [Google Scholar] [CrossRef]
- Sherman, S.; Lehman, G.A. Opioids and the sphincter of Oddi. Gastrointest. Endosc. 1994, 40, 105–106. [Google Scholar] [CrossRef]
- Thompson, D.R. Narcotic analgesic effects on the sphincter of Oddi: A review of the data and therapeutic implications in treating pancreatitis. Am. J. Gastroenterol. 2001, 96, 1266–1272. [Google Scholar] [CrossRef]
- Saini, M.; Samanta, J.; Kumar, A.; Choudhury, A.; Dhar, J.; Jafra, A.; Chauhan, R.; Muktesh, G.; Gupta, P.; Gupta, V.; et al. Buprenorphine Versus Diclofenac for Pain Relief in Acute Pancreatitis: A Double-Blinded Randomized Controlled Trial. Clin. Gastroenterol. Hepatol. 2024, 22, 532–541.e8. [Google Scholar] [CrossRef]
- O’Brien, T.; Christrup, L.L.; Drewes, A.M.; Fallon, M.T.; Kress, H.G.; McQuay, H.J.; Mikus, G.; Morlion, B.J.; Perez-Cajaraville, J.; Pogatzki-Zahn, E.; et al. European Pain Federation position paper on appropriate opioid use in chronic pain management. Eur. J. Pain 2017, 21, 3–19. [Google Scholar] [CrossRef]
- Drewes, A.M.; Munkholm, P.; Simrén, M.; Breivik, H.; Kongsgaard, U.E.; Hatlebakk, J.G.; Agreus, L.; Friedrichsen, M.; Christrup, L.L. Definition, diagnosis and treatment strategies for opioid-induced bowel dysfunction–Recommendations of the Nordic Working Group. Scand. J. Pain 2016, 11, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Drossman, D.; Szigethy, E. The narcotic bowel syndrome: A recent update. Am. J. Gastroenterol. Suppl. 2014, 2, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Grond, S.; Sablotzki, A. Clinical pharmacology of tramadol. Clin. Pharmacokinet. 2004, 43, 879–923. [Google Scholar] [CrossRef] [PubMed]
- Wilder-Smith, C.H.; Hill, L.; Osler, W.; O’Keefe, S. Effect of tramadol and morphine on pain and gastrointestinal motor function in patients with chronic pancreatitis. Dig. Dis. Sci. 1999, 44, 1107–1116. [Google Scholar] [CrossRef] [PubMed]
- Hameed, M.; Hameed, H.; Erdek, M. Pain management in pancreatic cancer. Cancers 2010, 3, 43–60. [Google Scholar] [CrossRef]
- Zylberberg, H.M.; Woodrell, C.; Rustgi, S.D.; Aronson, A.; Kessel, E.; Amin, S.; Lucas, A.L. Opioid Prescription Is Associated With Increased Survival in Older Adult Patients With Pancreatic Cancer in the United States: A Propensity Score Analysis. JCO Oncol. Pract. 2022, 18, e659–e668. [Google Scholar] [CrossRef] [PubMed]
- Fishbain, D.A.; Cole, B.; Lewis, J.E.; Gao, J.; Rosomoff, R.S. Do opioids induce hyperalgesia in humans? An evidence-based structured review. Pain Med. 2009, 10, 829–839. [Google Scholar] [CrossRef] [PubMed]
- Schneider, J.P.; Kirsh, K.L. Defining clinical issues around tolerance, hyperalgesia, and addiction: A quantitative and qualitative outcome study of long-term opioid dosing in a chronic pain practice. J. Opioid Manag. 2010, 6, 385–395. [Google Scholar] [CrossRef] [PubMed]
- Spahn, V.; Fischer, O.; Endres-Becker, J.; Schäfer, M.; Stein, C.; Zöllner, C. Opioid withdrawal increases transient receptor potential vanilloid 1 activity in a protein kinase A-dependent manner. Pain 2013, 154, 598–608. [Google Scholar] [CrossRef]
- Olesen, S.S.; Bouwense, S.A.; Wilder–Smith, O.H.; van Goor, H.; Drewes, A.M. Pregabalin reduces pain in patients with chronic pancreatitis in a randomized, controlled trial. Gastroenterology 2011, 141, 536–543. [Google Scholar] [CrossRef] [PubMed]
- Liao, X.-Z.; Zhou, M.-T.; Mao, Y.-F.; Xu, H.; Chen, H.; Sun, J.-H.; Xiong, Y.-C. Analgesic effects of gabapentin on mechanical hypersensitivity in a rat model of chronic pancreatitis. Brain Res. 2010, 1337, 104–112. [Google Scholar] [CrossRef]
- Layer, P.; Bronisch, H.-J.; Henniges, U.M.; Koop, I.; Kahl, M.; Dignass, A.; Ell, C.; Freitag, M.; Keller, J. Effects of systemic administration of a local anesthetic on pain in acute pancreatitis: A randomized clinical trial. Pancreas 2011, 40, 673–679. [Google Scholar] [CrossRef]
- Wilms, B.; Meffert, K.S.; Schultes, B. Procaine infusion for pain treatment of acute pancreatitis: A randomized, placebo-controlled double-blind trial. Dtsch. Med. Wochenschr. 2010, 135, 2290–2295. [Google Scholar] [CrossRef]
- Jakobs, R.; Adamek, M.U.; von Bubnoff, A.C.; Riemann, J.F. Buprenorphine or procaine for pain relief in acute pancreatitis. A prospective randomized study. Scand. J. Gastroenterol. 2000, 35, 1319–1323. [Google Scholar] [CrossRef] [PubMed]
- Kahl, S.; Zimmermann, S.; Pross, M.; Schulz, H.-U.; Schmidt, U.; Malfertheiner, P. Procaine hydrochloride fails to relieve pain in patients with acute pancreatitis. Digestion 2004, 69, 5–9. [Google Scholar] [CrossRef]
- Finnerup, N.B.; Attal, N.; Haroutounian, S.; McNicol, E.; Baron, R.; Dworkin, R.H.; Gilron, I.; Haanpää, M.; Hansson, P.; Jensen, T.S.; et al. Pharmacotherapy for neuropathic pain in adults: A systematic review and meta-analysis. Lancet Neurol. 2015, 14, 162–173. [Google Scholar] [CrossRef]
- Lohse, I.; Wildermuth, E.; Brothers, S.P. Naturally occurring compounds as pancreatic cancer therapeutics. Oncotarget 2018, 9, 35448–35457. [Google Scholar] [CrossRef]
- Kapral, M.; Wawszczyk, J.; Jesse, K.; Paul-Samojedny, M.; Kuśmierz, D.; Węglarz, L. Inositol Hexaphosphate Inhibits Proliferation and Induces Apoptosis of Colon Cancer Cells by Suppressing the AKT/mTOR Signaling Pathway. Molecules 2017, 22, 1657. [Google Scholar] [CrossRef]
- Abrams, D. Integrating cannabis into clinical cancer care. Curr. Oncol. 2016, 23, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Sadowski, S.M.; Andres, A.; Morel, P.; Schiffer, E.; Frossard, J.-L.; Platon, A.; Poletti, P.-A.; Bühler, L. Epidural anesthesia improves pancreatic perfusion and decreases the severity of acute pancreatitis. World J. Gastroenterol. 2015, 21, 12448–12456. [Google Scholar] [CrossRef] [PubMed]
- Jabaudon, M.; Belhadj-Tahar, N.; Rimmelé, T.; Joannes-Boyau, O.; Bulyez, S.; Lefrant, J.-Y.; Malledant, Y.; Leone, M.; Abback, P.-S.; Tamion, F.; et al. Thoracic Epidural Analgesia and Mortality in Acute Pancreatitis: A Multicenter Propensity Analysis. Crit. Care Med. 2018, 46, e198–e205. [Google Scholar] [CrossRef]
- Jabaudon, M.; Genevrier, A.; Jaber, S.; Windisch, O.; Bulyez, S.; Laterre, P.-F.; Escudier, E.; Sossou, A.; Guerci, P.; Bertrand, P.-M.; et al. Thoracic epidural analgesia in intensive care unit patients with acute pancreatitis: The EPIPAN multicenter randomized controlled trial. Crit. Care 2023, 27, 213. [Google Scholar] [CrossRef]
- Arcidiacono, P.G.G.; Calori, G.; Carrara, S.; McNicol, E.D.; Testoni, P.A. Celiac plexus block for pancreatic cancer pain in adults. Cochrane. Database. Syst. Rev. 2011, 2019, CD007519. [Google Scholar] [CrossRef] [PubMed]
- Okita, M.; Otani, K.; Gibo, N.; Matsui, S. Systematic review and meta-analysis of celiac plexus neurolysis for abdominal pain associated with unresectable pancreatic cancer. Pain Pract. 2022, 22, 652–661. [Google Scholar] [CrossRef] [PubMed]
- Gress, F.; Schmitt, C.; Sherman, S.; Ikenberry, S.; Lehman, G. A Prospective Randomized Comparison of Endoscopic Ultrasound- and Computed Tomography-Guided Celiac Plexus Block for Managing Chronic Pancreatitis Pain. Am. J. Gastroenterol. 1999, 94, 900–905. [Google Scholar] [CrossRef] [PubMed]
- Ratnayake, C.B.; Bunn, A.; Pandanaboyana, S.; Windsor, J.A. Spinal Cord Stimulation for Management of Pain in Chronic Pancreatitis: A Systematic Review of Efficacy and Complications. Neuromodulation 2020, 23, 19–25. [Google Scholar] [CrossRef]
- Ciapała, K.; Mika, J. Advances in Neuropathic Pain Research: Selected Intracellular Factors as Potential Targets for Multidirectional Analgesics. Pharmaceuticals 2023, 16, 1624. [Google Scholar] [CrossRef]
- van Westerloo, D.J.; Giebelen, I.A.; Florquin, S.; Bruno, M.J.; LaRosa, G.J.; Ulloa, L.; Tracey, K.J.; van der Poll, T. The vagus nerve and nicotinic receptors modulate experimental pancreatitis severity in mice. Gastroenterology 2006, 130, 1822–1830. [Google Scholar] [CrossRef] [PubMed]
- Schneider, L.; Jabrailova, B.; Soliman, H.; Hofer, S.; Strobel, O.; Hackert, T.; Büchler, M.W.; Werner, J. Pharmacological cholinergic stimulation as a therapeutic tool in experimental necrotizing pancreatitis. Pancreas 2014, 43, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.-M.; Yang, X.-Y.; Wan, J.-H. Multiple roles for cholinergic signaling in pancreatic diseases. World J. Gastroenterol. 2022, 28, 2910–2919. [Google Scholar] [CrossRef] [PubMed]
- Hefti, F.F.; Rosenthal, A.; Walicke, P.A.; Wyatt, S.; Vergara, G.; Shelton, D.L.; Davies, A.M. Novel class of pain drugs based on antagonism of NGF. Trends Pharmacol. Sci. 2006, 27, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Watson, J.J.; Allen, S.J.; Dawbarn, D. Targeting nerve growth factor in pain: What is the therapeutic potential? BioDrugs 2008, 22, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Ugolini, G.; Marinelli, S.; Covaceuszach, S.; Cattaneo, A.; Pavone, F. The function neutralizing anti-TrkA antibody MNAC13 reduces inflammatory and neuropathic pain. Proc. Natl. Acad. Sci. USA 2007, 104, 2985–2990. [Google Scholar] [CrossRef]
- Ghilardi, J.R.; Freeman, K.T.; Jimenez-Andrade, J.M.; Mantyh, W.G.; Bloom, A.P.; Bouhana, K.S.; Trollinger, D.; Winkler, J.; Lee, P.; Andrews, S.W.; et al. Sustained blockade of neurotrophin receptors TrkA, TrkB and TrkC reduces non-malignant skeletal pain but not the maintenance of sensory and sympathetic nerve fibers. Bone 2011, 48, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Brasca, M.G.; Amboldi, N.; Ballinari, D.; Cameron, A.; Casale, E.; Cervi, G.; Colombo, M.; Colotta, F.; Croci, V.; D’alessio, R.; et al. Identification of N,1,4,4-tetramethyl-8-{[4-(4-methylpiperazin-1-yl)phenyl]amino}-4,5-dihydro-1H-pyrazolo[4,3-h]quinazoline-3-carboxamide (PHA-848125), a potent, orally available cyclin dependent kinase inhibitor. J. Med. Chem. 2009, 52, 5152–5163. [Google Scholar] [CrossRef]
- Hartel, M.; di Mola, F.F.; Selvaggi, F.; Mascetta, G.; Wente, M.N.; Felix, K.; Giese, N.A.; Hinz, U.; Di Sebastiano, P.; Büchler, M.W.; et al. Vanilloids in pancreatic cancer: Potential for chemotherapy and pain management. Gut 2006, 55, 519–528. [Google Scholar] [CrossRef]
- Al-Wadei, H.A.; Al-Wadei, M.H.; Schuller, H.M. Prevention of pancreatic cancer by the beta-blocker propranolol. Anti-Cancer Drugs 2009, 20, 477–482. [Google Scholar] [CrossRef]
- Zhang, D.; Ma, Q.Y.; Hu, H.-T.; Zhang, M. β2-adrenergic antagonists suppress pancreatic cancer cell invasion by inhibiting CREB, NF-κB and AP-1. Cancer Biol. Ther. 2010, 10, 19–29. [Google Scholar] [CrossRef]
- Matsushita, Y.; Araki, K.; Omotuyi, O.I.; Mukae, T.; Ueda, H. HDAC inhibitors restore C-fibre sensitivity in experimental neuropathic pain model. Br. J. Pharmacol. 2013, 170, 991–998. [Google Scholar] [CrossRef] [PubMed]
- Lohse, I.; Brothers, S.P. Pathogenesis and Treatment of Pancreatic Cancer Related Pain. Anticancer Res. 2020, 40, 1789–1796. [Google Scholar] [CrossRef] [PubMed]
- Phillips, A.E.; Faghih, M.; Singh, V.K.M.; Olesen, S.S.; Kuhlmann, L.; Novovic, S.; Bick, B.; Hart, P.A.; Ramsey, M.L.; Talukdar, R.; et al. Rationale for and Development of the Pancreatic Quantitative Sensory Testing Consortium to Study Pain in Chronic Pancreatitis. Pancreas 2021, 50, 1298–1304. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Complication | Indication for Treatment | First-Line Treatment | Alternative Therapies |
|---|---|---|---|
| Pseudocyst Fluid collection Walled-off necrosis | Symptoms (e.g., pain, gastric outlet obstruction, intestinal obstruction) Vascular obstruction Infection | EUS-guided stent positioning | US/CT-guided percutaneous drainage Surgery |
| Main biliary duct obstruction | Jaundice Increased cholestatic LFTs Infection | ERCP | EUS-guided stent positioning US-guided percutaneous biliary drainage |
| Pancreatic ductal stones | Pain, evidence of duct dilation, and inadequate pain control | ESWL | ESWL + ERCP |
| Pancreatic ductal stricture | Pain, evidence of duct dilation, and inadequate pain control | ERCP | Surgery |
| Gastric outlet obstruction | Symptoms (vomiting, pain) | Surgical gastroenterostomy Endoscopic stenting (pancreatic cancer) | EUS-guided gastroenterostomy Surgical gastroenterostomy |
| Pharmacological Class | Drug and Dosage | Possible Side Effects | Disease |
|---|---|---|---|
| Antipyretics | Paracetamol 1000 mg (usually t.i.d. to obtain analgesic effect) | Thrombocytopenia, leukopenia, anemia, acute hepatitis, anaphylactic shock, hypotension, dizziness | Acute pancreatitis Chronic pancreatitis Pancreatic cancer |
| NSAIDs | Ibuprofen 600 mg qd. (up to t.i.d.) Ketoprofen 50 mg qd. (up to q.i.d.) Ketorolac 10 mg qd. (up to q.i.d.) | Peptic ulcer, gastrointestinal bleeding, vomiting, nausea, diarrhea, dyspepsia, skin rash, fatigue, acute kidney injury, hypertension | Acute pancreatitis Chronic pancreatitis Pancreatic cancer |
| Opioids | Tramadol 50 mg qd. (up to q.i.d.) Oxycodone 10 mg (up to 80 mg) b.i.d. Fentanyl 100 mcg sublingual route (up to 400 mcg) q.i.d. Fentanyl transdermal route 25 (up to 100) mcg/h | Drowsiness, headache, dizziness, constipation, nausea, fatigue, dry mouth, vomiting, hyperhidrosis | Acute pancreatitis Chronic pancreatitis Pancreatic cancer |
| Gabapentinoids | Pregabalin 150 mg (up to 300 mg) b.i.d. | Viral infections, leukopenia, anorexia, increased appetite, confusion, depression, anxiety, drowsiness, dizziness, diplopia, nausea, vomiting, dyspepsia, dry mouth, arthromyalgia, incontinence, impotence | Chronic pancreatitis Pancreatic cancer |
| Local anesthetics | Procaine 2 g/24 h i.v. | Nausea, vomiting, diarrhea, dizziness, headache, tachycardia, hypertension, rash, severe allergic reactions | Acute pancreatitis |
| Antidepressants | Duloxetin 30 mg (up to 60 mg) qd. | Headache, drowsiness, dry mouth, nausea, erectile dysfunction, ejaculation disorder, weight loss, constipation, insomnia, vomiting, lack of appetite | Chronic pancreatitis Pancreatic cancer |
| Cannabinoids | Dronabinol 1 mg (up to 2 mg) qd. Nabilone 1 mg (up to 2 mg) b.i.d. | Psychosis, hallucinations, depersonalization, mood alterations and paranoia, vertigo, drowsiness, dry mouth, ataxia, blurred vision, euphoria | Pancreatic cancer |
| PERT | Pancrelipase 40,000–50,000 (up to 150,000) IU per meal | Nausea, vomiting, constipation, abdominal swelling, diarrhea | Acute necrotizing pancreatitis with PEI Chronic pancreatitis with PEI Pancreatic cancer with PEI |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nicoletti, A.; Vitale, F.; Paratore, M.; Quero, G.; Negri, M.; Nista, E.C.; Alfieri, S.; Gasbarrini, A.; Zileri Dal Verme, L. Neuropancreatology: The Nervous System and Pain Management in Pancreatic Diseases. Life 2024, 14, 299. https://doi.org/10.3390/life14030299
Nicoletti A, Vitale F, Paratore M, Quero G, Negri M, Nista EC, Alfieri S, Gasbarrini A, Zileri Dal Verme L. Neuropancreatology: The Nervous System and Pain Management in Pancreatic Diseases. Life. 2024; 14(3):299. https://doi.org/10.3390/life14030299
Chicago/Turabian StyleNicoletti, Alberto, Federica Vitale, Mattia Paratore, Giuseppe Quero, Marcantonio Negri, Enrico Celestino Nista, Sergio Alfieri, Antonio Gasbarrini, and Lorenzo Zileri Dal Verme. 2024. "Neuropancreatology: The Nervous System and Pain Management in Pancreatic Diseases" Life 14, no. 3: 299. https://doi.org/10.3390/life14030299