
The Role of Bifidobacterium in COVID-19: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
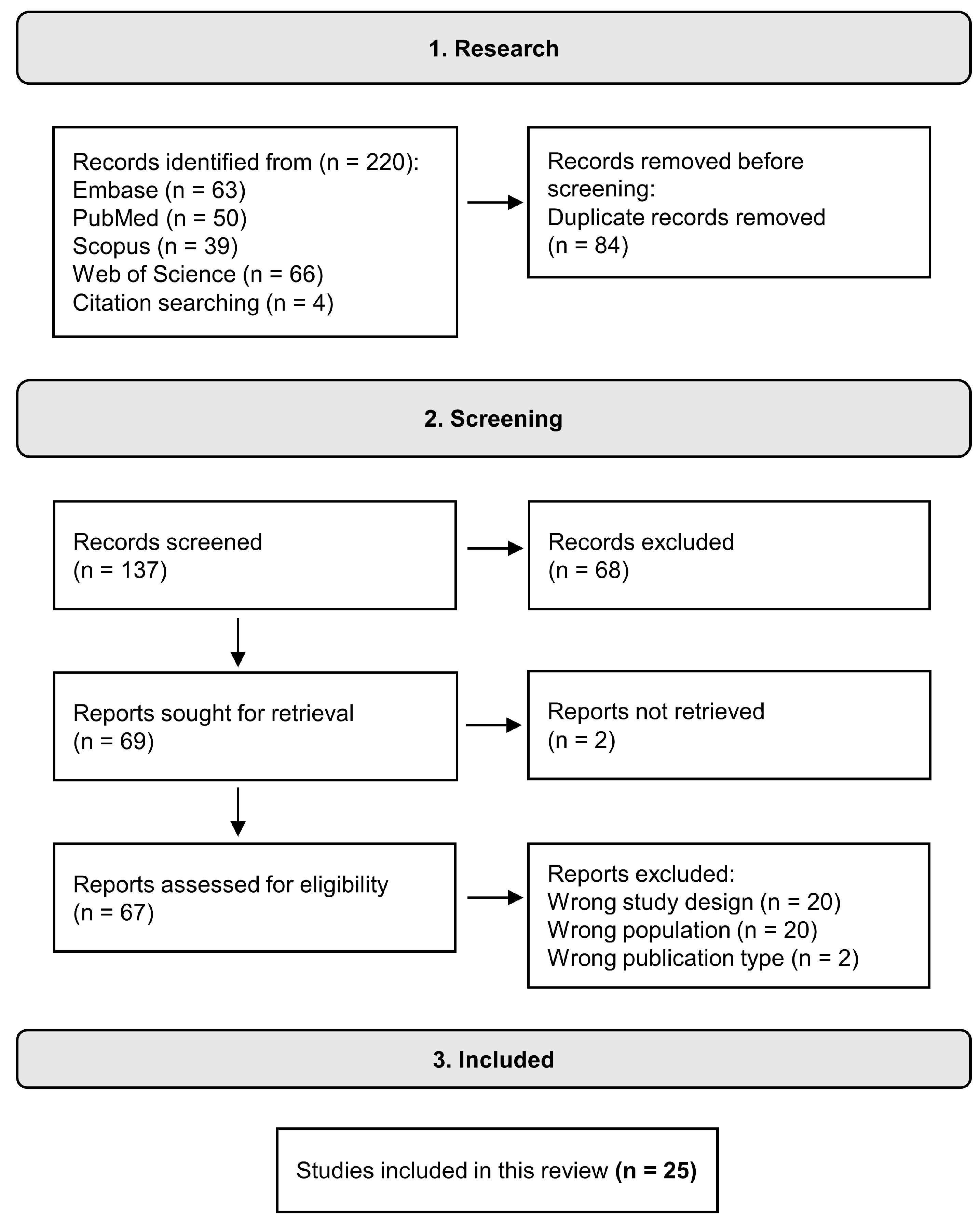
2.1. Search Strategy and Selection Criteria
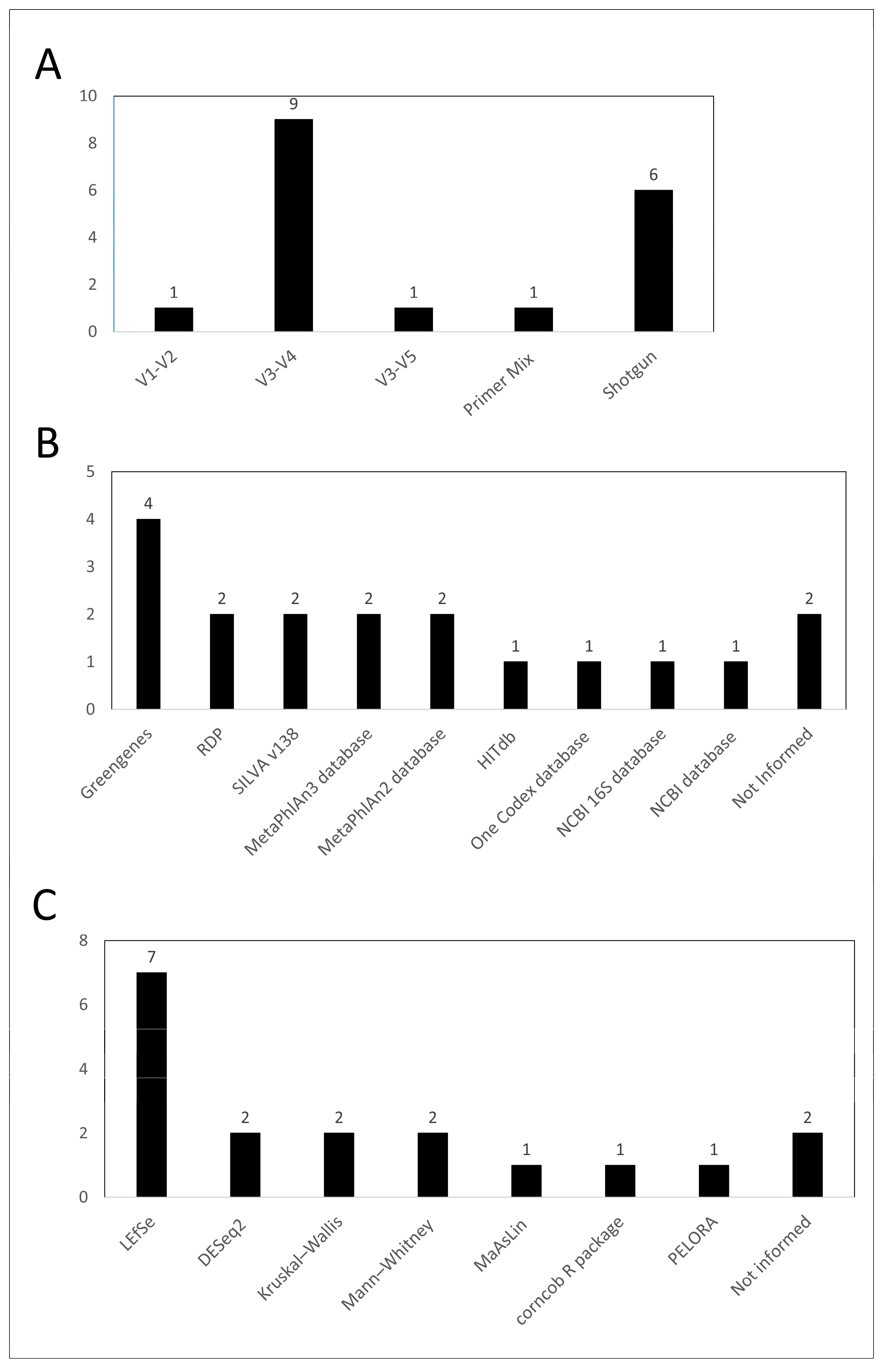
2.2. Data Extraction and Analysis

3. Results
3.1. Selected Studies
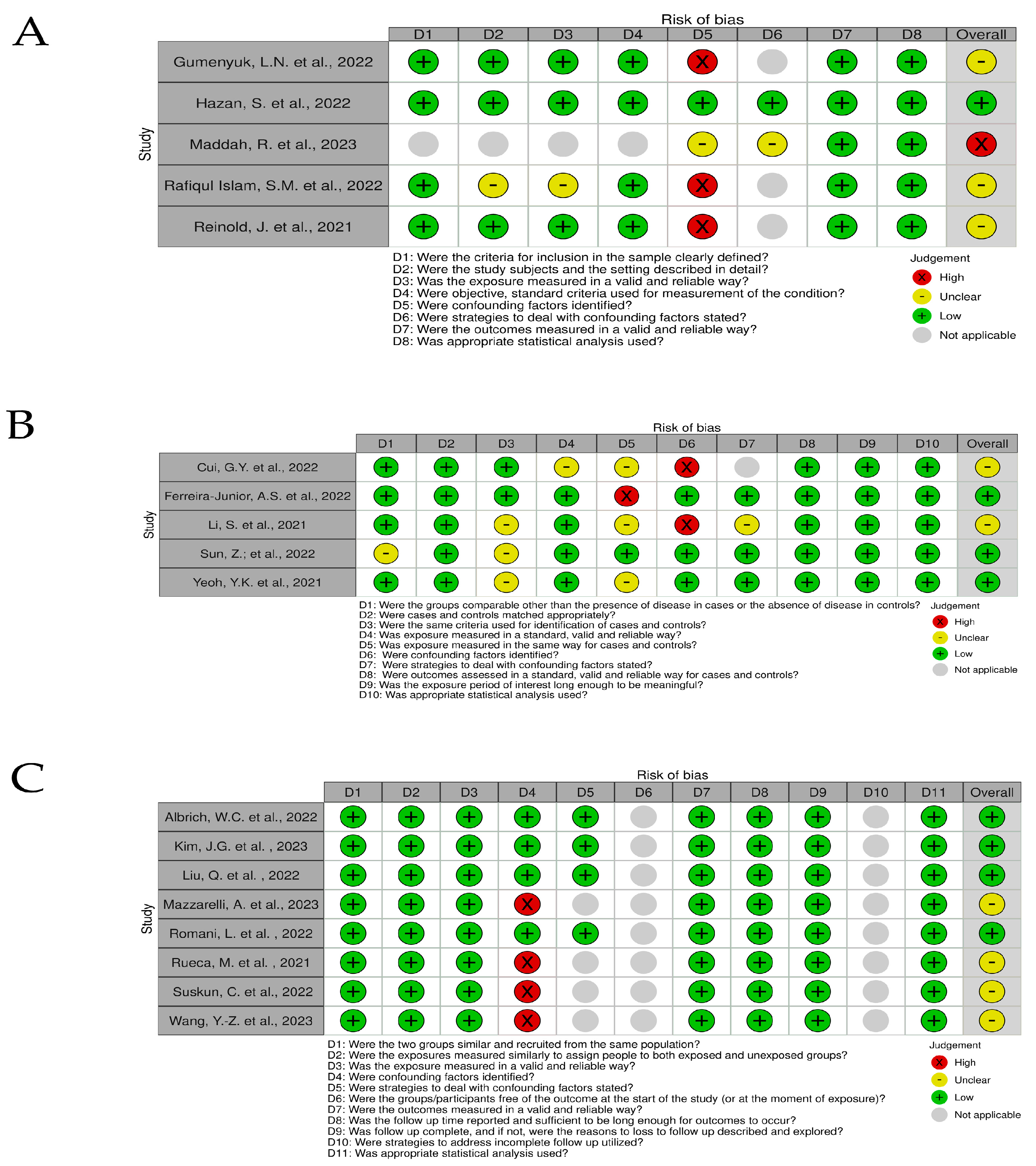
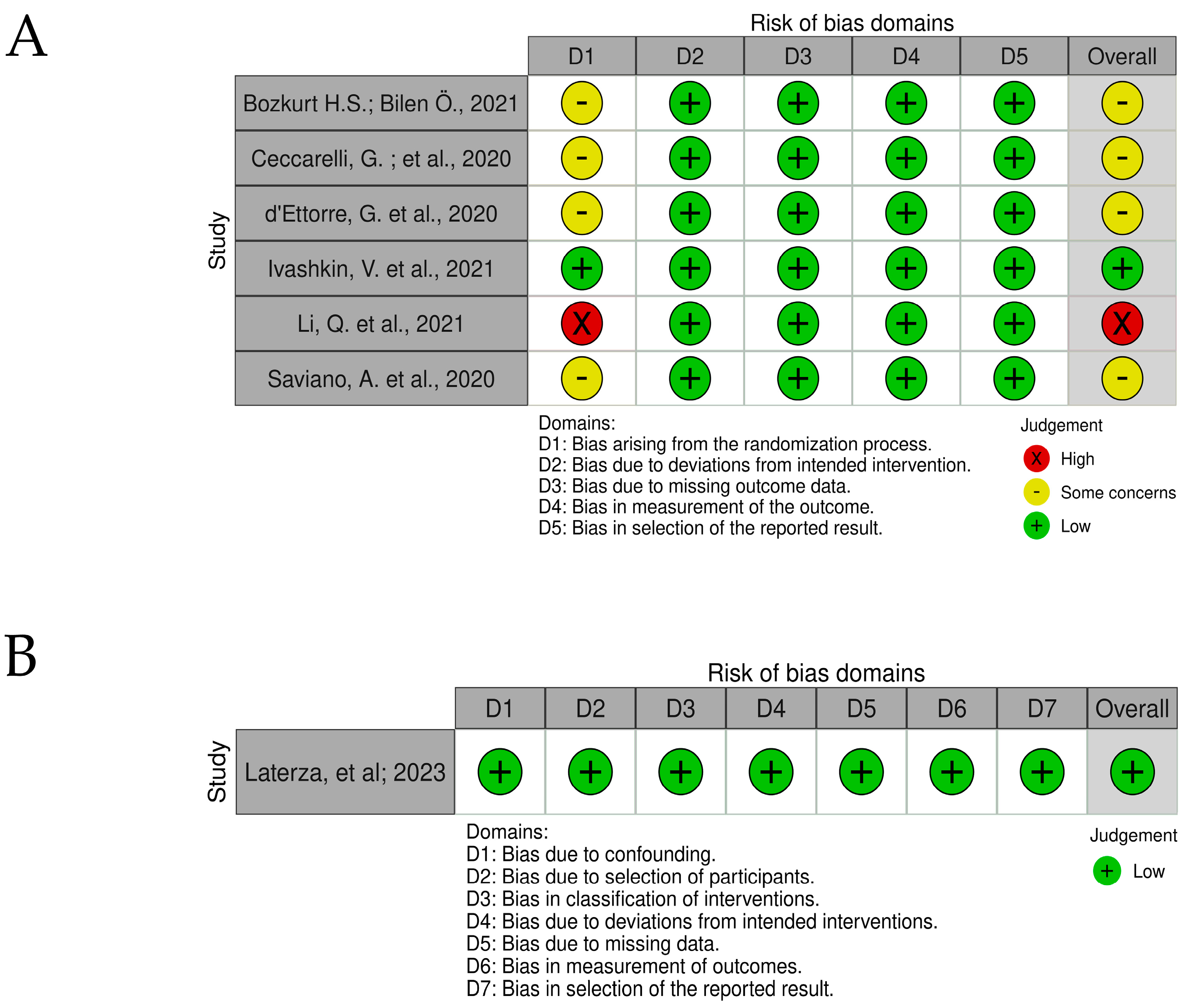
3.2. Risk of Bias and Quality Accessment
4. Discussion
4.1. The Bifidobacterium Genus
4.2. Evidence in COVID-19
4.3. The Probiotic Bifidobacterium in the Management of COVID-19
4.4. Risk of Bias and Quality Accessment
4.5. Evidence in Other Viral Infections
4.6. Mechanisms of Protection of Bifidobacterium in COVID-19
4.6.1. Modulation of the Immune Response
4.6.2. Reduction of Inflammation
4.6.3. Competitive Advantages with Pathogenic Microbes
4.6.4. Maintenance of Gut Barrier Function
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Segal, J.P.; Mak, J.W.Y.; Mullish, B.H.; Alexander, J.L.; Ng, S.C.; Marchesi, J.R. The Gut Microbiome: An under-Recognised Contributor to the COVID-19 Pandemic? Therap. Adv. Gastroenterol. 2020, 13, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Hidalgo-Cantabrana, C.; Delgado, S.; Ruiz, L.; Ruas-Madiedo, P.; Sánchez, B.; Margolles, A. Bifidobacteria and Their Health-Promoting Effects. Microbiol. Spectr. 2017, 5, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Lisy, K.; Qureshi, R.; Mattis, P.M.P. Chapter 7: Systematic Reviews of Etiology and Risk. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020. [Google Scholar]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A Tool for Assessing Risk of Bias in Non-Randomised Studies of Interventions. BMJ 2016, 355, 4–10. [Google Scholar] [CrossRef]
- Albrich, W.C.; Ghosh, T.S.; Ahearn-Ford, S.; Mikaeloff, F.; Lunjani, N.; Forde, B.; Suh, N.; Kleger, G.-R.; Pietsch, U.; Frischknecht, M.; et al. A High-Risk Gut Microbiota Configuration Associates with Fatal Hyperinflammatory Immune and Metabolic Responses to SARS-CoV-2. Gut Microbes 2022, 14. [Google Scholar] [CrossRef]
- Cui, G.Y.; Rao, B.C.; Zeng, Z.H.; Wang, X.M.; Ren, T.; Wang, H.Y.; Luo, H.; Ren, H.Y.; Liu, C.; Ding, S.Y.; et al. Characterization of Oral and Gut Microbiome and Plasma Metabolomics in COVID-19 Patients after 1-Year Follow-Up. Mil. Med. Res. 2022, 9, 32. [Google Scholar] [CrossRef]
- Ferreira-Junior, A.S.; Borgonovi, T.F.; De Salis, L.V.V.; Leite, A.Z.; Dantas, A.S.; De Salis, G.V.V.; Cruz, G.N.F.; De Oliveira, L.F.V.; Gomes, E.; Penna, A.L.B.; et al. Detection of Intestinal Dysbiosis in Post-COVID-19 Patients One to Eight Months after Acute Disease Resolution. Int. J. Environ. Res. Public Health 2022, 19, 10189. [Google Scholar] [CrossRef]
- Gumenyuk, L.N.; Golod, M.V.; Silaeva, N.V.; Sorokina, L.E.; Ilyasov, S.S.; Androschyuk, N.A.; Krivoshapko, O.R.; Velilyaev, A.M.; Asanova, L.N. Gut Microbiota Alterations and Their Relationship To the Disease Severity and Some Cytokine Profile Indicators in Patients With COVID-19. Bull. Russ. State Med. Univ. 2022, 22–29. [Google Scholar] [CrossRef]
- Hazan, S.; Stollman, N.; Bozkurt, H.S.; Dave, S.; Papoutsis, A.J.; Daniels, J.; Barrows, B.D.; Quigley, E.M.; Borody, T.J. Lost Microbes of COVID-19: Bifidobacterium, Faecalibacterium Depletion and Decreased Microbiome Diversity Associated with SARS-CoV-2 Infection Severity. BMJ Open Gastroenterol. 2022, 9, e000871. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.G.; Zhang, A.; Rauseo, A.M.; Goss, C.W.; Mudd, P.A.; O’Halloran, J.A.; Wang, L. The Salivary and Nasopharyngeal Microbiomes Are Associated with SARS-CoV-2 Infection and Disease Severity. J. Med. Virol. 2023, 95, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Yang, S.; Zhou, Y.; Disoma, C.; Dong, Z.; Du, A.; Zhang, Y.; Chen, Y.; Huang, W.; Chen, J.; et al. Microbiome Profiling Using Shotgun Metagenomic Sequencing Identified Unique Microorganisms in COVID-19 Patients with Altered Gut Microbiota. Front. Microbiol. 2021, 12, 712081. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Mak, J.W.Y.; Su, Q.; Yeoh, Y.K.; Lui, G.C.-Y.; Ng, S.S.S.; Zhang, F.; Li, A.Y.L.; Lu, W.; Hui, D.S.-C.; et al. Gut Microbiota Dynamics in a Prospective Cohort of Patients with Post-Acute COVID-19 Syndrome. Gut 2022, 71, 544–552. [Google Scholar] [CrossRef] [PubMed]
- Maddah, R.; Goodarzi, V.; Asadi-Yousefabad, S.-L.; Abbasluo, M.; Shariati, P.; Shafiei Kafraj, A. Evaluation of the Gut Microbiome Associated with COVID-19. Inform. Med. Unlocked 2023, 38, 101239. [Google Scholar] [CrossRef] [PubMed]
- Mazzarelli, A.; Giancola, M.L.; Fontana, A.; Piselli, P.; Binda, E.; Trivieri, N.; Mencarelli, G.; Marchioni, L.; Vulcano, A.; De Giuli, C.; et al. Gut Microbiota Composition in COVID-19 Hospitalized Patients with Mild or Severe Symptoms. Front. Microbiol. 2022, 13, 1049215. [Google Scholar] [CrossRef]
- Rafiqul Islam, S.M.; Foysal, M.J.; Hoque, M.N.; Mehedi, H.M.H.; Rob, M.A.; Salauddin, A.; Tanzina, A.Y.; Biswas, S.; Noyon, S.H.; Siddiki, A.M.A.M.Z.; et al. Dysbiosis of Oral and Gut Microbiomes in SARS-CoV-2 Infected Patients in Bangladesh: Elucidating the Role of Opportunistic Gut Microbes. Front. Med. 2022, 9, 821777. [Google Scholar] [CrossRef]
- Reinold, J.; Farahpour, F.; Fehring, C.; Dolff, S.; Konik, M.; Korth, J.; van Baal, L.; Hoffmann, D.; Buer, J.; Witzke, O.; et al. A Pro-Inflammatory Gut Microbiome Characterizes SARS-CoV-2 Infected Patients and a Reduction in the Connectivity of an Anti-Inflammatory Bacterial Network Associates With Severe COVID-19. Front. Cell. Infect. Microbiol. 2021, 11, 1–11. [Google Scholar] [CrossRef]
- Romani, L.; Del Chierico, F.; Macari, G.; Pane, S.; Ristori, M.V.; Guarrasi, V.; Gardini, S.; Pascucci, G.R.; Cotugno, N.; Perno, C.F.; et al. The Relationship Between Pediatric Gut Microbiota and SARS-CoV-2 Infection. Front. Cell. Infect. Microbiol. 2022, 12, 908492. [Google Scholar] [CrossRef]
- Rueca, M.; Fontana, A.; Bartolini, B.; Piselli, P.; Mazzarelli, A.; Copetti, M.; Binda, E.; Perri, F.; Gruber, C.E.M.; Nicastri, E.; et al. Investigation of Nasal/Oropharyngeal Microbial Community of COVID-19 Patients by 16S RDNA Sequencing. Int. J. Environ. Res. Public Health 2021, 18, 2174. [Google Scholar] [CrossRef]
- Sun, Z.; Song, Z.; Liu, C.; Tan, S.; Lin, S.; Zhu, J.; Dai, F.; Gao, J.; She, J.; Mei, Z.; et al. Gut Microbiome Alterations and Gut Barrier Dysfunction Are Associated with Host Immune Homeostasis in COVID-19 Patients. BMC Med. 2022, 20, 24. [Google Scholar] [CrossRef] [PubMed]
- Suskun, C.; Kilic, O.; Yilmaz Ciftdogan, D.; Guven, S.; Karbuz, A.; Ozkaya Parlakay, A.; Kara, Y.; Kacmaz, E.; Sahin, A.; Boga, A.; et al. Intestinal Microbiota Composition of Children with Infection with Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) and Multisystem Inflammatory Syndrome (MIS-C). Eur. J. Pediatr. 2022, 181, 3175–3191. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-Z.; Zhou, J.-G.; Lu, Y.-M.; Hu, H.; Xiao, F.-F.; Ge, T.; Wang, X.; Zheng, L.; Yu, L.-H.; Le, J.; et al. Altered Gut Microbiota Composition in Children and Their Caregivers Infected with the SARS-CoV-2 Omicron Variant. World J. Pediatr. 2023, 19, 478–488. [Google Scholar] [CrossRef] [PubMed]
- Yeoh, Y.K.; Zuo, T.; Lui, G.C.-Y.; Zhang, F.; Liu, Q.; Li, A.Y.; Chung, A.C.; Cheung, C.P.; Tso, E.Y.; Fung, K.S.; et al. Gut Microbiota Composition Reflects Disease Severity and Dysfunctional Immune Responses in Patients with COVID-19. Gut 2021, 70, 698–706. [Google Scholar] [CrossRef]
- Bozkurt, H.S.; Bilen, Ö. Oral Booster Probiotic Bifidobacteria in SARS-CoV-2 Patients. Int. J. Immunopathol. Pharmacol. 2021, 35, 205873842110596. [Google Scholar] [CrossRef]
- Ceccarelli, G.; Borrazzo, C.; Pinacchio, C.; Santinelli, L.; Innocenti, G.P.; Cavallari, E.N.; Celani, L.; Marazzato, M.; Alessandri, F.; Ruberto, F.; et al. Oral Bacteriotherapy in Patients With COVID-19: A Retrospective Cohort Study. Front. Nutr. 2021, 7, 1–8. [Google Scholar] [CrossRef]
- d’Ettorre, G.; Ceccarelli, G.; Marazzato, M.; Campagna, G.; Pinacchio, C.; Alessandri, F.; Ruberto, F.; Rossi, G.; Celani, L.; Scagnolari, C.; et al. Challenges in the Management of SARS-CoV2 Infection: The Role of Oral Bacteriotherapy as Complementary Therapeutic Strategy to Avoid the Progression of COVID-19. Front. Med. 2020, 7, 389. [Google Scholar] [CrossRef]
- Ivashkin, V.; Fomin, V.; Moiseev, S.; Brovko, M.; Maslennikov, R.; Ulyanin, A.; Sholomova, V.; Vasilyeva, M.; Trush, E.; Shifrin, O.; et al. Efficacy of a Probiotic Consisting of Lacticaseibacillus Rhamnosus PDV 1705, Bifidobacterium Bifidum PDV 0903, Bifidobacterium Longum Subsp. Infantis PDV 1911, and Bifidobacterium Longum Subsp. Longum PDV 2301 in the Treatment of Hospitalized Patients Wit. Probiotics Antimicrob. Proteins 2021, 15, 460–468. [Google Scholar] [CrossRef]
- Laterza, L.; Putignani, L.; Settanni, C.R.; Petito, V.; Varca, S.; De Maio, F.; Macari, G.; Guarrasi, V.; Gremese, E.; Tolusso, B.; et al. Ecology and Machine Learning-Based Classification Models of Gut Microbiota and Inflammatory Markers May Evaluate the Effects of Probiotic Supplementation in Patients Recently Recovered from COVID-19. Int. J. Mol. Sci. 2023, 24, 6623. [Google Scholar] [CrossRef]
- Li, Q.; Cheng, F.; Xu, Q.; Su, Y.; Cai, X.; Zeng, F.; Zhang, Y. The Role of Probiotics in Coronavirus Disease-19 Infection in Wuhan: A Retrospective Study of 311 Severe Patients. Int. Immunopharmacol. 2021, 95, 107531. [Google Scholar] [CrossRef]
- Saviano, A.; Potenza, A.; Siciliano, V.; Petruzziello, C.; Tarli, C.; Migneco, A.; Nasella, F.; Franceschi, F.; Ojetti, V. COVID-19 Pneumonia and Gut Inflammation: The Role of a Mix of Three Probiotic Strains in Reducing Inflammatory Markers and Need for Oxygen Support. J. Clin. Med. 2022, 11, 3758. [Google Scholar] [CrossRef]
- Sgorbati, B.; Biavati, B.; Palenzona, D. The Genus Bifidobacterium. In The Genera of Lactic Acid Bacteria; Springer US: Boston, MA, USA, 1995; pp. 279–306. [Google Scholar]
- Turroni, F. Bifidobacteria: From Ecology to Genomics. Front. Biosci. 2009, 14, 4673–4684. [Google Scholar] [CrossRef] [PubMed]
- Alessandri, G.; van Sinderen, D.; Ventura, M. The Genus Bifidobacterium: From Genomics to Functionality of an Important Component of the Mammalian Gut Microbiota. Comput. Struct. Biotechnol. J. 2021, 19, 1472–1487. [Google Scholar] [CrossRef] [PubMed]
- Ewaschuk, J.B.; Diaz, H.; Meddings, L.; Diederichs, B.; Dmytrash, A.; Backer, J.; Van Langen, M.L.; Madsen, K.L. Secreted Bioactive Factors from Bifidobacterium Infantis Enhance Epithelial Cell Barrier Function. Am. J. Physiol. Gastrointest. Liver Physiol. 2008, 295, 1025–1034. [Google Scholar] [CrossRef] [PubMed]
- Alessandri, G.; Ossiprandi, M.C.; MacSharry, J.; van Sinderen, D.; Ventura, M. Bifidobacterial Dialogue With Its Human Host and Consequent Modulation of the Immune System. Front. Immunol. 2019, 10, 2348. [Google Scholar] [CrossRef] [PubMed]
- Tojo, R.; Suárez, A.; Clemente, M.G.; De Los Reyes-Gavilán, C.G.; Margolles, A.; Gueimonde, M.; Ruas-Madiedo, P. Intestinal Microbiota in Health and Disease: Role of Bifidobacteria in Gut Homeostasis. World J. Gastroenterol. 2014, 20, 15163–15176. [Google Scholar] [CrossRef] [PubMed]
- Usta-Gorgun, B.; Yilmaz-Ersan, L. Short-Chain Fatty Acids Production by Bifidobacterium Species in the Presence of Salep. Electron. J. Biotechnol. 2020, 47, 29–35. [Google Scholar] [CrossRef]
- Mirzayi, C.; Renson, A.; Furlanello, C.; Sansone, S.-A.; Zohra, F.; Elsafoury, S.; Geistlinger, L.; Kasselman, L.J.; Eckenrode, K.; van de Wijgert, J.; et al. Reporting Guidelines for Human Microbiome Research: The STORMS Checklist. Nat. Med. 2021, 27, 1885–1892. [Google Scholar] [CrossRef]
- Qin, N.; Zheng, B.; Yao, J.; Guo, L.; Zuo, J.; Wu, L.; Zhou, J.; Liu, L.; Guo, J.; Ni, S.; et al. Influence of H7N9 Virus Infection and Associated Treatment on Human Gut Microbiota. Sci. Rep. 2015, 5, 14771. [Google Scholar] [CrossRef]
- Wang, Z.; Usyk, M.; Sollecito, C.C.; Qiu, Y.; Williams-Nguyen, J.; Hua, S.; Gradissimo, A.; Wang, T.; Xue, X.; Kurland, I.J.; et al. Altered Gut Microbiota and Host Metabolite Profiles in Women with Human Immunodeficiency Virus. Clin. Infect. Dis. 2020, 71, 2345–2353. [Google Scholar] [CrossRef]
- Yitbarek, A.; Weese, J.S.; Alkie, T.N.; Parkinson, J.; Sharif, S. Influenza A Virus Subtype H9N2 Infection Disrupts the Composition of Intestinal Microbiota of Chickens. FEMS Microbiol. Ecol. 2018, 94, 1–10. [Google Scholar] [CrossRef]
- Zhang, Q.; Hu, J.; Feng, J.; Hu, X.; Wang, T.; Gong, W.; Huang, K.; Guo, Y.; Zou, Z.; Lin, X.; et al. Influenza Infection Elicits an Expansion of Gut Population of Endogenous Bifidobacterium Animalis Which Protects Mice against Infection. Genome Biol. 2020, 21, 99. [Google Scholar] [CrossRef] [PubMed]
- Yasui, H.; Kiyoshima, J.; Hori, T.; Shida, K. Protection against Influenza Virus Infection of Mice Fed Bifidobacterium Breve YIT4064. Clin. Diagn. Lab. Immunol. 1999, 6, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Groeger, D.; Schiavi, E.; Grant, R.; Kurnik-Łucka, M.; Michalovich, D.; Williamson, R.; Beinke, S.; Kiely, B.; Akdis, C.A.; Hessel, E.M.; et al. Intranasal Bifidobacterium Longum Protects against Viral-Induced Lung Inflammation and Injury in a Murine Model of Lethal Influenza Infection. eBioMedicine 2020, 60, 102981. [Google Scholar] [CrossRef] [PubMed]
- Kawahara, T.; Takahashi, T.; Oishi, K.; Tanaka, H.; Masuda, M.; Takahashi, S.; Takano, M.; Kawakami, T.; Fukushima, K.; Kanazawa, H.; et al. Consecutive Oral Administration of Bifidobacterium Longum MM-2 Improves the Defense System against Influenza Virus Infection by Enhancing Natural Killer Cell Activity in a Murine Model. Microbiol. Immunol. 2015, 59, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Erdoǧan, Ö.; Tanyeri, B.; Torun, E.; Gönüllü, E.; Arslan, H.; Erenberk, U.; Öktem, F. The Comparition of the Efficacy of Two Different Probiotics in Rotavirus Gastroenteritis in Children. J. Trop. Med. 2012, 2012, 787240. [Google Scholar] [CrossRef]
- Leyer, G.J.; Li, S.; Mubasher, M.E.; Reifer, C.; Ouwehand, A.C. Probiotic Effects on Cold and Influenza-like Symptom Incidence and Duration in Children. Pediatrics 2009, 124, e172–e179. [Google Scholar] [CrossRef]
- de Vrese, M.; Winkler, P.; Rautenberg, P.; Harder, T.; Noah, C.; Laue, C.; Ott, S.; Hampe, J.; Schreiber, S.; Heller, K.; et al. Effect of Lactobacillus Gasseri PA 16/8, Bifidobacterium Longum SP 07/3, B. bifidum MF 20/5 on Common Cold Episodes: A Double Blind, Randomized, Controlled Trial. Clin. Nutr. 2005, 24, 481–491. [Google Scholar] [CrossRef]
- Lu, W.; Fang, Z.; Liu, X.; Li, L.; Zhang, P.; Zhao, J.; Zhang, H.; Chen, W. The Potential Role of Probiotics in Protection against Influenza a Virus Infection in Mice. Foods 2021, 10, 902. [Google Scholar] [CrossRef]
- Mahooti, M.; Abdolalipour, E.; Salehzadeh, A.; Mohebbi, S.R.; Gorji, A.; Ghaemi, A. Immunomodulatory and Prophylactic Effects of Bifidobacterium Bifidum Probiotic Strain on Influenza Infection in Mice. World J. Microbiol. Biotechnol. 2019, 35, 91. [Google Scholar] [CrossRef]
- Fattahi, Y.; Heidari, H.R.; Khosroushahi, A.Y. Review of Short-Chain Fatty Acids Effects on the Immune System and Cancer. Food Biosci. 2020, 38, 100793. [Google Scholar] [CrossRef]
- Marfia, G.; Navone, S.; Guarnaccia, L.; Campanella, R.; Mondoni, M.; Locatelli, M.; Barassi, A.; Fontana, L.; Palumbo, F.; Garzia, E.; et al. Decreased Serum Level of Sphingosine-1-phosphate: A Novel Predictor of Clinical Severity in COVID-19. EMBO Mol. Med. 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Yao, S.; Zhao, Z.; Wang, W.; Liu, X. Bifidobacterium Longum: Protection against Inflammatory Bowel Disease. J. Immunol. Res. 2021, 2021, 8030297. [Google Scholar] [CrossRef]
- Gopal, P.K.; Prasad, J.; Smart, J.; Gill, H.S. In Vitro Adherence Properties of Lactobacillus Rhamnosus DR20 and Bifidobacterium Lactis DR10 Strains and Their Antagonistic Activity against an Enterotoxigenic Escherichia Coli. Int. J. Food Microbiol. 2001, 67, 207–216. [Google Scholar] [CrossRef]
- Fujiwara, S.; Hashiba, H.; Hirota, T.; Forstner, J.F. Proteinaceous Factor(s) in Culture Supernatant Fluids of Bifidobacteria Which Prevents the Binding of Enterotoxigenic Escherichia Coli to Gangliotetraosylceramide. Appl. Environ. Microbiol. 1997, 63, 506–512. [Google Scholar] [CrossRef]
- Liu, C.; Zhang, Z.Y.; Dong, K.; Guo, X.K. Adhesion and Immunomodulatory Effects of Bifidobacterium Lactis HN019 on Intestinal Epithelial Cells INT-407. World J. Gastroenterol. 2010, 16, 2283–2290. [Google Scholar] [CrossRef] [PubMed]
- Lievin, V.; Peiffer, I.; Hudault, S.; Rochat, F.; Brassart, D.; Neeser, J.R.; Servin, A.L. Bifidobacterium Strains from Resident Infant Human Gastrointestinal Microflora Exert Antimicrobial Activity. Gut 2000, 47, 646–652. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Xiao, G.; Yao, Y.; Guo, S.; Lu, K.; Sheng, Z. The Role of Bifidobacteria in Gut Barrier Function after Thermal Injury in Rats. J. Trauma Inj. Infect. Crit. Care 2006, 61, 650–657. [Google Scholar] [CrossRef] [PubMed]
- Yan, S.; Yang, B.; Ross, R.P.; Stanton, C.; Zhang, H.; Zhao, J.; Chen, W. Bifidobacterium Longum Subsp. Longum YS108R Fermented Milk Alleviates DSS Induced Colitis via Anti-Inflammation, Mucosal Barrier Maintenance and Gut Microbiota Modulation. J. Funct. Foods 2020, 73, 104153. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country | Type of Study | Type of Sample | NGS Tecnology | Type of Sequencing | N | Groups | Abundance in COVID-19 Group | Clinical Relevance |
|---|---|---|---|---|---|---|---|---|---|
| Albrich et al., 2022 [8] | Switzerland and Ireland | Cohort | Stool | MiSeq | V3–V4 | 128 1 | 32 mild/ moderate 45 severe/non-fatal 22 severe/fatal COVID-19 29 healthy controls | Decreased | Associated with severity |
| Cui et al., 2022 [9] | China | Case-control | Tongue-coating and stool | MiSeq | V3–V5 | 195 | 35 patients post-COVID-19 160 healthy controls | No statistical difference observed | Not associated with recovery process |
| Ferreira-Junior et al., 2022 [10] | Brazil | Case-control | Stool | MiSeq | V3–V4 | 220 | 149 post-COVID-19 71 healthy controls | Decreased in post-COVID-19 and antibiotic-treated | Associated with disease and antibiotic treatment |
| Gumenyuk et al., 2022 [11] | Russia | Cross-sectional | Stool | SOLiD 5500 | Shotgun | 208 | 110 COVID-19 patients 98 healthy controls | Decrease of B. adolescentis | Associated with disease |
| Hazan et al., 2022 [12] | USA | Cross-sectional | Stool | NextSeq 500/550 | Shotgun | 70 | 50 COVID-19 patients 20 exposed controls | Decreased | Associated with severity |
| Kim et al., 2023 [13] | USA | Cohort | Saliva and nasopharyngeal | MiSeq | V1–V2 | 144 | 114 samples COVID-19 positive 30 samples COVID-19 negative | Decreased in ICU group. The genus was associated with lower levels of IL-17F and MCP-1 | Associated with severity |
| Li et al., 2021 [14] | China | Case-control | Stool | BGISEQ-500 | Shotgun | 66 | 47 COVID-19 patients 19 healthy controls | Increase of B. longum in COVID-19. B. bifidum was negatively correlated with the severity and B. animalis was positively correlated. | Associated with severity |
| Liu et al., 2022 [15] | China | Cohort | Stool | NextSeq 550 | Shotgun | 174 | 106 COVID-19 (50 PACS) 68 non-COVID-19 | Decreased. B. pseudocatenulatum was inversely correlated with PACS at 6 months | Associated with severity and PACS |
| Maddah et al., 2023 [16] | China 2/Iran 3 | Cross-sectional | Stool | MiSeq | V3–V4 | 30 | 30 COVID-19 patients 30 healthy controls | Decrease of B. adolescentis | Associated with disease |
| Mazzarelli et al., 2022 [17] | Italy | Cohort | Stool | MiSeq | V3–V4 | 97 | 47 mild COVID-19 50 severe COVID-19 | No statistical difference observed | Not associated with severity |
| Rafiqul Islam et al., 2022 [18] | Bangladesh | Cross-secctional | Stool and saliva | MiSeq | V3–V4 | 37 | 22 COVID-19 patients 15 healthy controls | Decreased | Associated with disease |
| Reinold et al., 2021 [19] | Germany | Cross-secctional | Stool | Novaseq 6000 | V3–V4 | 212 | 44 mild COVID-19 35 moderate COVID-19 38 severe/critical COVID-19 95 SARS-CoV-2 negative controls | Decreased | Associated with disease |
| Romani et al., 2022 [20] | Italy | Cohort | Stool | MiSeq | V3–V4 | 183 | 68 COVID-19 children 16 non-COVID-19 4 children with MIS | Decreased | Associated with disease |
| Rueca et al., 2021 [21] | Italy | Cohort | Nasal/ oropharyngeal | IonS5 | V2-4-8 e V3-6 e 7-8 | 39 | 21 COVID-19 patients 8 HCoV patients 10 healthy controls | Complete depletion in ICU patients | Associated with severity |
| Sun et al., 2022 [22] | China | Case-control | Stool | Novaseq 6000 | Shotgun | 71 | 63 COVID-19 patients 8 non-infected controls | Increase of B. longum and depletion of B. pseudocatenulatum in COVID-19 | Associated with severity |
| Suskun et al., 2022 [23] | Turkey | Cohort | Stool | NovaSeq 6000 | V3–V4 | 39 | 20 COVID-19 children 25 MIS-C children 19 healthy controls | Increase of B. adolescentis in COVID-19 | Associated with severity |
| Wang et al., 2023 [24] | China | Cohort | Stool | MiSeq | V3–V4 | 186 | 59 COVID-19 children 50 asymptomatic caregivers 52 healthy children 25 healthy adults | Decreased | Associated with disease |
| Yeoh et al., 2021 [25] | China | Case-control | Stool | NovaSeq 6000 | Shotgun | 178 | 100 COVID-19 patients 78 non-COVID-19 patients | Depletion of B. adolescentis in COVID-19. B. bifidum was negatively correlated with severity. Increase of B. dentium and depleted B. longum in recovered patients. | Associated with disease severity and recovery process |
| Study | Country | N | Groups | Probiotics | Outcome | Clinical Relevance |
|---|---|---|---|---|---|---|
| Bozkurt & Bilen, 2021 [26] | Turkey | 44 | probiotic group (20) non-probiotic group (24) | Bifidobacterium BB-12 | Reduction of hospitalization days; thorax resolution at 6 days and 3 weeks; reduction in IL-6 plasma levels. | Beneficial |
| Ceccarelli et al., 2020 [27] | Italy | 200 | probiotic group (88) non-probiotic group (112) | Sivomixx® containing Streptococcus thermophilus DSM 32245, Bifidobacterium lactis DSM 32246, Bifidobacterium lactis DSM 32247, Lactobacillus acidophilus DSM 32241, Lactobacillus helveticus DSM 32242, Lactobacillus paracasei DSM 32243, Lactobacillus plantarum DSM 32244, and Lactobacillus brevis DSM 27961 | Significant reduction in the risk of death. | Beneficial |
| d’Ettorre et al., 2020 [28] | Italy | 70 | probiotic group (28) non-probiotic group (42) | Sivomixx® containing Streptococcus thermophilus DSM 32345, Lactobacillus acidophilus DSM 32241, Lactobacillus helveticus DSM 32242 Lactobacillus paracasei DSM 32243, Lactobacillus plantarum DSM 32244, Lactobacillus brevis DSM 27961, Bifidobacterium lactis DSM 32246, and Bifidobacterium lactis DSM 32247 | Remission of diarrhea in almost all patients treated within 72 h, reduction in other symptoms, 8x lower risk of developing respiratory failure. | Beneficial |
| Ivashkin et al., 2021 [29] | Russian | 202 | probiotic group (101) non-probiotic group (101) | Florasan-D containing Lacticaseibacillus rhamnosus PDV 1705, Bifidobacterium bifidum PDV 0903, Bifidobacterium longum subsp. infantis PDV 1911, and Bifidobacterium longum subsp. longum PDV 2301 | Average reduction of two days in the duration of viral diarrhea and prevention of hospital-acquired diarrhea for patients receiving a single antibiotic. | Beneficial |
| Laterza et al., 2023 [30] | Italy | 19 | post-COVID-19 patients (19) | VSL#3® (lot number 909031) containing Lactobacillus paracasei BP07, Lactobacillus plantarum BP06, Lactobacillus acidophilus BA05, Lactobacillus helveticus BD08 (previously identified as L. delbrueckii subsp. bulgaricus), Bifidobacterium animalis subsp. lactis BL03 (previously identified as B. longum), Bifidobacterium animalis subsp. lactis BI04 (previously identified as B. infantis), Bifidobacterium breve BB02, and Streptococcus thermophilus BT01 | Significant reduction of IL-6, TNF-ALFA, IL-12RA, and citrulline. | Beneficial |
| Li et al., 2021 [31] | China | 311 | probiotic group (123) non-probiotic group (188) | Bifidobacterium infantis, Lactobacillus acidophilus, Dung enterococcus, Bacillus cereus, Bifidobacterium longum, Lactobacillus bulgaricus, Streptococcus termófilos, Bacillus subtilis, Enterococcus faecium, and Bacillus subtilis | No significant differences were observed. | No difference |
| Saviano et al., 2022 [32] | Italy | 80 | probiotic group (40) non-probiotic group (40) | Lactibiane Iki® containing Bifidobacterium lactis LA 304, Lactobacillus salivarius LA 302, and Lactobacillus acidophilus LA 201 | Lower values of fecal calprotectin, reduction of the inflammatory marker CRP, faster and continuous reduction needed for O2 support, and lower mean length of hospitalization. | Beneficial |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taufer, C.R.; Rampelotto, P.H. The Role of Bifidobacterium in COVID-19: A Systematic Review. Life 2023, 13, 1847. https://doi.org/10.3390/life13091847
Taufer CR, Rampelotto PH. The Role of Bifidobacterium in COVID-19: A Systematic Review. Life. 2023; 13(9):1847. https://doi.org/10.3390/life13091847
Chicago/Turabian StyleTaufer, Clarissa Reginato, and Pabulo Henrique Rampelotto. 2023. "The Role of Bifidobacterium in COVID-19: A Systematic Review" Life 13, no. 9: 1847. https://doi.org/10.3390/life13091847