

Age and Sex-Related Differences in Teicoplanine Isoform Concentrations in SARS-CoV-2 Patients

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Inclusion Criteria
2.2. HPLC Analysis
2.3. Statistical Analysis
3. Results
3.1. Study Population
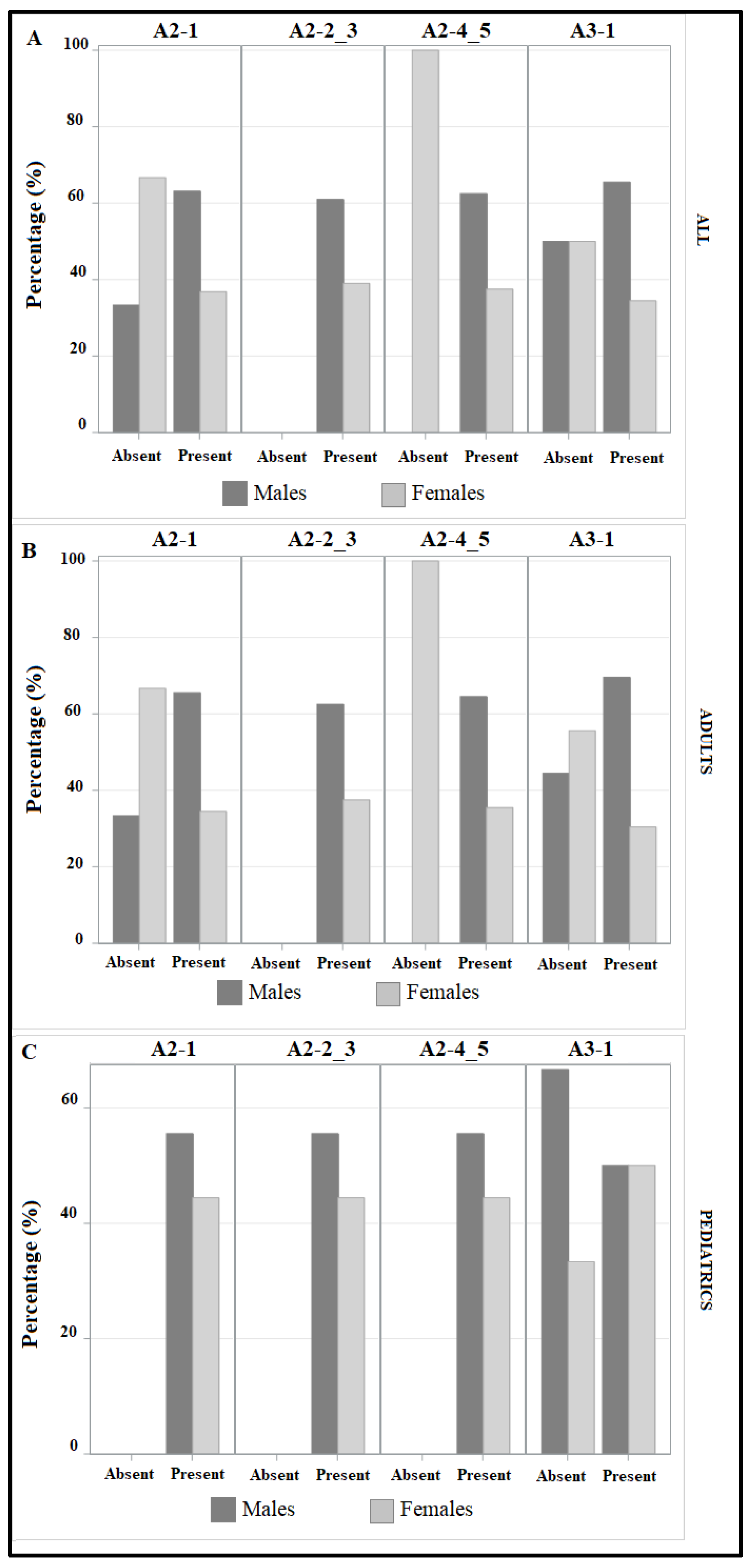
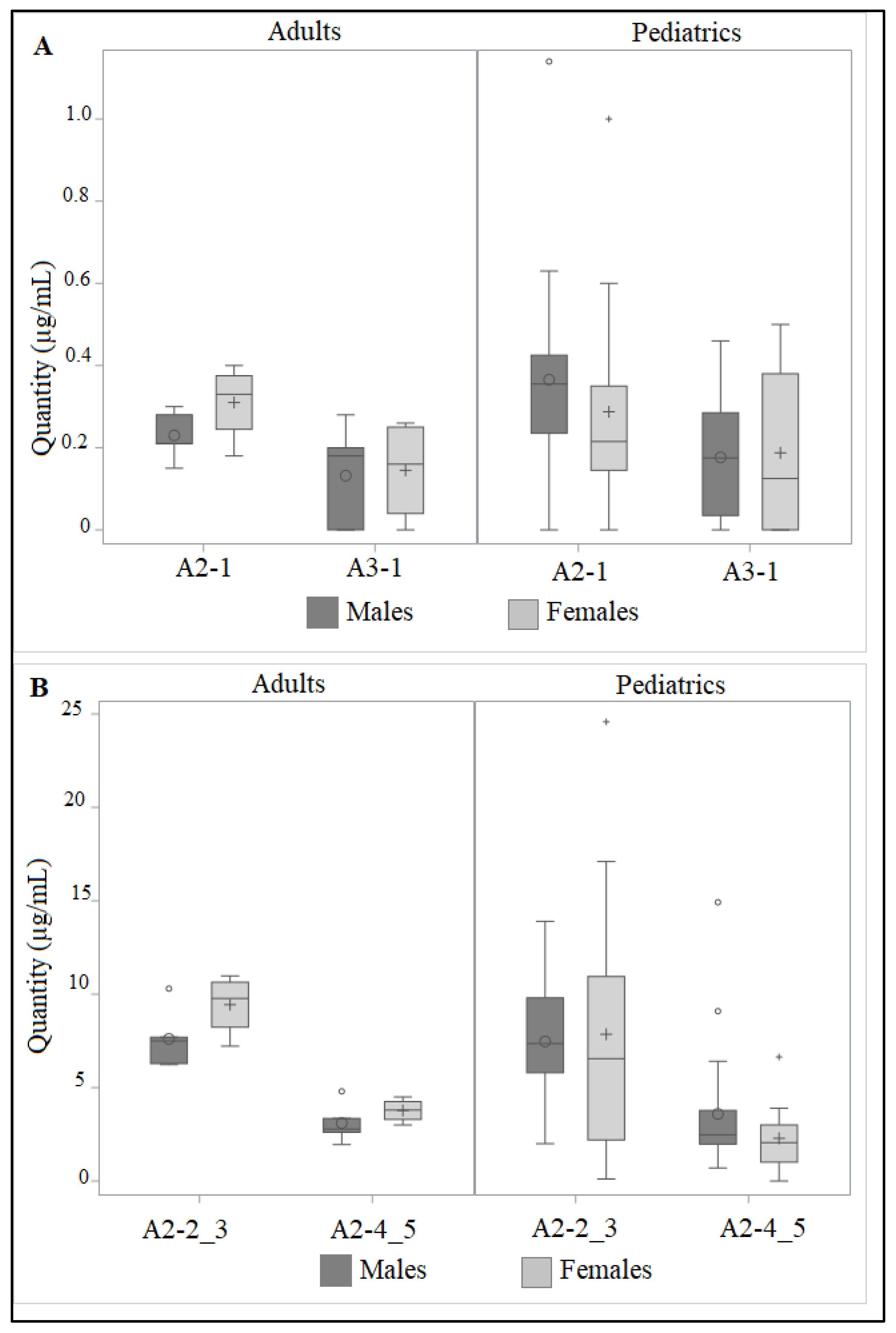
3.2. Effect of Age Ang Gender on Teicoplanin Isoforms
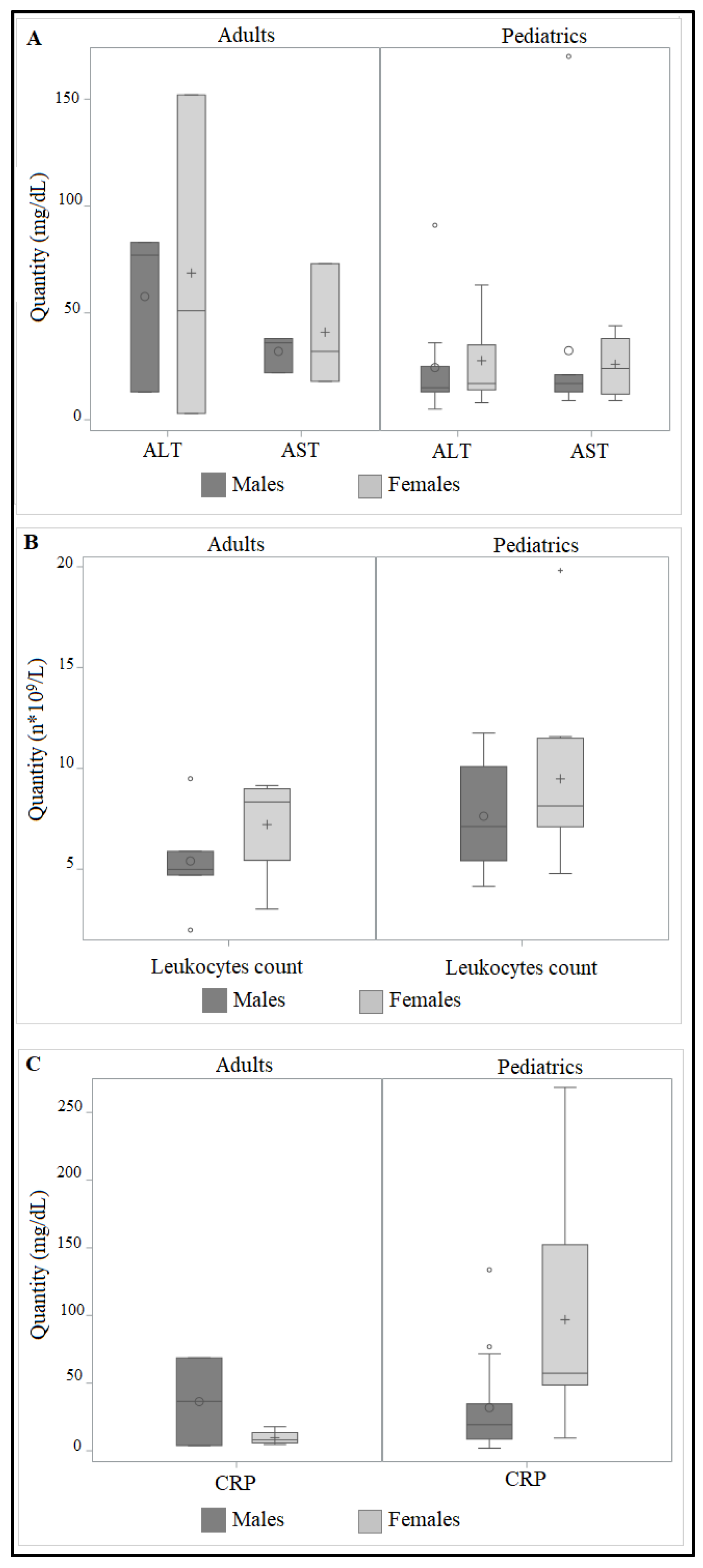
3.3. Correlation between ALT, AST, Leukocytes Count and CRP and Teicoplanin Isoforms
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Horton, R. Offline: 2019-nCoV outbreak-early lessons. Lancet 2020, 395, 322. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. Lancet 2020, 395, 565–574. [Google Scholar] [CrossRef]
- Rothe, C.; Schunk, M.; Sothmann, P.; Bretzel, G.; Froeschl, G.; Wallrauch, C.; Zimmer, T.; Thiel, V.; Janke, C.; Guggemos, W.; et al. Transmission of 2019-nCoV Infection from an Asymptomatic Contact in Germany. N. Engl. J. Med. 2020, 382, 970–971. [Google Scholar] [CrossRef]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Yushchuk, O.; Ostash, B.; Truman, A.W.; Marinelli, F.; Fedorenko, V. Teicoplanin biosynthesis: Unraveling the interplay of structural, regulatory, and resistance genes. Appl. Microbiol. Biotechnol. 2020, 104, 3279–3291. [Google Scholar] [CrossRef]
- Boger, D.L. Vancomycin, teicoplanin, and ramoplanin: Synthetic and mechanistic studies. Med. Res. Rev. 2001, 21, 356–381. [Google Scholar] [CrossRef]
- Butler, M.S.; Hansford, K.A.; Blaskovich, M.A.; Halai, R.; Cooper, M.A. Glycopeptide antibiotics: Back to the future. J. Antibiot. 2014, 67, 631–644. [Google Scholar] [CrossRef]
- Coronelli, C.; Gallo, G.G.; Cavalleri, B. Teicoplanin: Chemical, physico-chemical and biological aspects. Farmaco. Sci. 1987, 42, 767–786. [Google Scholar]
- Yu, F.; Pan, T.; Huang, F.; Ying, R.; Liu, J.; Fan, H.; Zhang, J.; Liu, W.; Lin, Y.; Yuan, Y.; et al. Glycopeptide Antibiotic Teicoplanin Inhibits Cell Entry of SARS-CoV-2 by Suppressing the Proteolytic Activity of Cathepsin L. Front. Microbiol. 2022, 13, 884034. [Google Scholar] [CrossRef]
- Colson, P.; Raoult, D. Fighting viruses with antibiotics: An overlooked path. Int. J. Antimicrob. Agents 2016, 48, 349–352. [Google Scholar] [CrossRef] [PubMed]
- Zhou, N.; Pan, T.; Zhang, J.; Li, Q.; Zhang, X.; Bai, C.; Huang, F.; Peng, T.; Liu, C.; Tao, L.; et al. Glycopeptide Antibiotics Potently Inhibit Cathepsin L in the Late Endosome/Lysosome and Block the Entry of Ebola Virus, Middle East Respiratory Syndrome Coronavirus (MERS-CoV), and Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV). J. Biol. Chem. 2016, 291, 9218–9232. [Google Scholar] [CrossRef] [PubMed]
- Baron, S.A.; Devaux, C.; Colson, P.; Raoult, D.; Rolain, J.M. Teicoplanin: An alternative drug for the treatment of COVID-19? Int. J. Antimicrob. Agents 2020, 55, 105944. [Google Scholar] [CrossRef]
- Parenti, F.; Schito, G.C.; Courvalin, P. Teicoplanin Chemistry and Microbiology. J. Chemother. 2000, 12 (Suppl. S5), 5–14. [Google Scholar] [CrossRef]
- Esposito, S.; Noviello, S. What is the role of glycopeptides in intensive care? J. Chemother. 2003, 15 (Suppl. S3), 11–16. [Google Scholar] [CrossRef] [PubMed]
- Sabolić, I.; Asif, A.R.; Budach, W.E.; Wanke, C.; Bahn, A.; Burckhardt, G. Gender differences in kidney function. Pflug. Arch. 2007, 455, 397–429. [Google Scholar] [CrossRef]
- Rosenthal, P.; Pincus, M.; Fink, D. Sex- and age-related differences in bilirubin concentrations in serum. Clin. Chem. 1984, 30, 1380–1382. [Google Scholar] [CrossRef]
- Mera, J.R.; Dickson, B.; Feldman, M. Influence of gender on the ratio of serum aspartate aminotransferase (AST) to alanine aminotransferase (ALT) in patients with and without hyperbilirubinemia. Dig. Dis. Sci. 2008, 53, 799–802. [Google Scholar] [CrossRef]
- Mijovic, V.; Contreras, M.; Barbara, J. Serum alanine aminotransferase (ALT) and gamma-glutamyltransferase (gamma-GT) activities in north London blood donors. J. Clin. Pathol. 1987, 40, 1340–1344. [Google Scholar] [CrossRef]
- Poustchi, H.; George, J.; Esmaili, S.; Esna-Ashari, F.; Ardalan, G.; Sepanlou, S.G.; Alavian, S.M. Gender differences in healthy ranges for serum alanine aminotransferase levels in adolescence. PLoS ONE 2011, 6, e21178. [Google Scholar] [CrossRef]
- Chen, S.C.; Yeh, J.J.; Chang, M.H.; Liao, Y.K.; Hsiao, L.C.; Neoh, C.A.; Tok, T.S.; Wang, J.D. Gender difference of alanine aminotransferase elevation may be associated with higher hemoglobin levels among male adolescents. PLoS ONE 2010, 5, e13269. [Google Scholar] [CrossRef] [PubMed]
- Moore, B.; Paterson, M.; Sturdee, D. Effect of oral hormone replacement therapy on liver function tests. Maturitas 1987, 9, 7–15. [Google Scholar] [CrossRef]
- Crippin, J.S.; Jorgensen, R.A.; Dickson, E.R.; Lindor, K.D. Hepatic osteodystrophy in primary biliary cirrhosis: Effects of medical treatment. Am. J. Gastroenterol. 1994, 89, 47–50. [Google Scholar] [PubMed]
- Guattery, J.M.; Faloon, W.W. Effect of estradiol upon serum enzymes in primary biliary cirrhosis. Hepatology 1987, 7, 737–742. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Giri, M.; Puri, A.; Wang, T.; Guo, S. Clinical features, comorbidities, complications and treatment options in severe and non-severe COVID-19 patients: A systemic review and meta-analysis. Nurs. Open 2021, 8, 1077–1088. [Google Scholar] [CrossRef]
- Yahia, A.I.O. Liver Injury and Dysfunction Associated with COVID-19: A Review Article. Clin. Lab. 2022, 68. [Google Scholar] [CrossRef]
- Leo, M.; Galante, A.; Pagnamenta, A.; Ruinelli, L.; Ponziani, F.R.; Gasbarrini, A.; De Gottardi, A. Hepatocellular liver injury in hospitalized patients affected by COVID-19: Presence of different risk factors at different time points. Dig. Liver Dis. 2022, 54, 565–571. [Google Scholar] [CrossRef]
- Yu, D.; Du, Q.; Yan, S.; Guo, X.G.; He, Y.; Zhu, G.; Zhao, K.; Ouyang, S. Liver injury in COVID-19: Clinical features and treatment management. Virol. J. 2021, 18, 121. [Google Scholar] [CrossRef]
- Ekpanyapong, S.; Bunchorntavakul, C.; Reddy, K.R. COVID-19 and the Liver: Lessons Learnt from the EAST and the WEST, A Year Later. J. Viral. Hepat. 2022, 29, 4–20. [Google Scholar] [CrossRef]
- Xu, X.W.; Wu, X.X.; Jiang, X.G.; Xu, K.J.; Ying, L.J.; Ma, C.L.; Li, S.B.; Wang, H.Y.; Zhang, S.; Gao, H.N.; et al. Clinical findings in a group of patients infected with the 2019 novel coronavirus (SARS-Cov-2) outside of Wuhan, China: Retrospective case series. BMJ 2020, 368, m606. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Lei, J.; Li, Z.; Yan, L. Potential Effects of Coronaviruses on the Liver: An Update. Front. Med. 2021, 8, 651658. [Google Scholar] [CrossRef]
- Fara, A.; Mitrev, Z.; Rosalia, R.A.; Assas, B.M. Cytokine storm and COVID-19: A chronicle of pro-inflammatory cytokines. Open Biol. 2020, 10, 200160. [Google Scholar] [CrossRef]
- Abate, B.B.; Kassie, A.M.; Kassaw, M.W.; Aragie, T.G.; Masresha, S.A. Sex difference in coronavirus disease (COVID-19): A systematic review and meta-analysis. BMJ Open 2020, 10, e040129. [Google Scholar] [CrossRef]
- Meng, Y.; Wu, P.; Lu, W.; Liu, K.; Ma, K.; Huang, L.; Cai, J.; Zhang, H.; Qin, Y.; Sun, H.; et al. Sex-specific clinical characteristics and prognosis of coronavirus disease-19 infection in Wuhan, China: A retrospective study of 168 severe patients. PLoS Pathog. 2020, 16, e1008520. [Google Scholar] [CrossRef]
- Leung, G.M.; Hedley, A.J.; Ho, L.M.; Chau, P.; Wong, I.O.; Thach, T.Q.; Ghani, A.C.; Donnelly, C.A.; Fraser, C.; Riley, S.; et al. The epidemiology of severe acute respiratory syndrome in the 2003 Hong Kong epidemic: An analysis of all 1755 patients. Ann. Intern. Med. 2004, 141, 662–673. [Google Scholar] [CrossRef]
- De Francia, S.; Ferretti, A.; Chiara, F.; Allegra, S.; Mancardi, D.; Allice, T.G.; Milia, M.G.; Gregori, G.; Burdino, E.; Avanzini, C.; et al. The Influence of Sex, Gender, and Age on COVID-19 Data in the Piedmont Region (Northwest Italy): The Virus Prefers Men. Life 2022, 12, 643. [Google Scholar] [CrossRef]
- Scully, E.P.; Haverfield, J.; Ursin, R.L.; Tannenbaum, C.; Klein, S.L. Considering how biological sex impacts immune responses and COVID-19 outcomes. Nat. Rev. Immunol. 2020, 20, 442–447. [Google Scholar] [CrossRef]
- Qi, S.; Ngwa, C.; Morales Scheihing, D.A.; Al Mamun, A.; Ahnstedt, H.W.; Finger, C.E.; Colpo, G.D.; Sharmeen, R.; Kim, Y.; Choi, H.A.; et al. Sex differences in the immune response to acute COVID-19 respiratory tract infection. Biol. Sex Differ. 2021, 12, 66. [Google Scholar] [CrossRef] [PubMed]
- Cheng, R.; Liu, C.; Yang, J.; Yang, Y.; Chen, R.; Ding, X.; Gao, X.; Ke, J.; Yuan, F.; He, C.; et al. Sex Differences in the Incidence and Risk Factors of Myocardial Injury in COVID-19 Patients: A Retrospective Cohort Study. Front. Physiol. 2021, 12, 632123. [Google Scholar] [CrossRef]
- Yoshida, Y.; Gillet, S.A.; Brown, M.I.; Zu, Y.; Wilson, S.M.; Ahmed, S.J.; Tirumalasetty, S.; Lovre, D.; Krousel-Wood, M.; Denson, J.L.; et al. Clinical characteristics and outcomes in women and men hospitalized for coronavirus disease 2019 in New Orleans. Biol. Sex Differ. 2021, 12, 20. [Google Scholar] [CrossRef]
- Lukas, J.C.; Karikas, G.; Gazouli, M.; Kalabalikis, P.; Hatzis, T.; Macheras, P. Pharmacokinetics of teicoplanin in an ICU population of children and infants. Pharm. Res. 2004, 21, 2064–2071. [Google Scholar] [CrossRef]
- Reed, M.D.; Yamashita, T.S.; Myers, C.M.; Blumer, J.L. The pharmacokinetics of teicoplanin in infants and children. J. Antimicrob. Chemother. 1997, 39, 789–796. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, A.; López-Herce, J.; Cueto, E.; Carrillo, A.; Moral, R. Teicoplanin pharmacokinetics in critically ill paediatric patients. J. Antimicrob. Chemother. 1999, 44, 407–409. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Martín, V.; Paulus, S.; Siner, S.; Scott, E.; Padmore, K.; Newland, P.; Drew, R.J.; Felton, T.W.; Docobo-Pérez, F.; Pizer, B.; et al. Population pharmacokinetics of teicoplanin in children. Antimicrob. Agents Chemother. 2014, 58, 6920–6927. [Google Scholar] [CrossRef]
- Tarral, E.; Jehl, F.; Tarral, A.; Simeoni, U.; Monteil, H.; Willard, D.; Geisert, J. Pharmacokinetics of teicoplanin in children. J. Antimicrob. Chemother. 1988, 21 (Suppl. A), 47–51. [Google Scholar] [CrossRef]
- Matthews, K.A.; Crawford, S.L.; Chae, C.U.; Everson-Rose, S.A.; Sowers, M.F.; Sternfeld, B.; Sutton-Tyrrell, K. Are changes in cardiovascular disease risk factors in midlife women due to chronological aging or to the menopausal transition? J. Am. Coll. Cardiol. 2009, 54, 2366–2373. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Time | Flow (mL/min) | Mobile Phase A | Mobile Phase B |
|---|---|---|---|
| 0.01 | 0.3 | 95 | 5 |
| 3.00 | 0.3 | 95 | 5 |
| 4.50 | 0.3 | 38 | 62 |
| 5.50 | 0.3 | 38 | 62 |
| 7.50 | 0.3 | 25 | 75 |
| 8.00 | 0.3 | 25 | 75 |
| 8.50 | 0.3 | 0 | 100 |
| 9.00 | 0.3 | 0 | 100 |
| 9.50 | 0.3 | 95 | 5 |
| Pediatrics | Adults | ||||
|---|---|---|---|---|---|
| F | M | F | M | ||
| Age (years) | Median | 13.50 | 14.00 | 81.00 | 63.00 |
| QRange | 10.50 | 4.00 | 9.00 | 20.00 | |
| ALT (mg/dL) | Median | 51.00 | 77.00 | 17.00 | 15.00 |
| QRange | 149.00 | 70.00 | 21.00 | 12.00 | |
| AST (mg/dL) | Median | 32.00 | 36.00 | 24.00 | 17.00 |
| QRange | 55.00 | 16.00 | 26.00 | 8.00 | |
| LEUKOCYTES COUNT (number * 109/L) | Median | 8.34 | 4.99 | 8.14 | 7.12 |
| QRange | 3.55 | 1.18 | 4.40 | 4.67 | |
| CRP (mg/dL) | Median | 8.05 | 36.50 | 57.30 | 19.30 |
| QRange | 7.55 | 64.90 | 103.70 | 26.00 | |
| ISOFORM (µg/mL) | Pediatrics | Adults | |||
|---|---|---|---|---|---|
| F | M | F | M | ||
| A2-1 | Median | 0.33 | 0.21 | 0.22 | 0.36 |
| QRange | 0.13 | 0.07 | 0.21 | 0.19 | |
| A2-2_3 | Median | 9.78 | 7.50 | 6.55 | 7.36 |
| QRange | 2.41 | 1.41 | 8.75 | 4.00 | |
| A2-4_5 | Median | 3.80 | 2.78 | 2.06 | 2.48 |
| QRange | 0.95 | 0.74 | 1.99 | 1.80 | |
| A3-1 | Median | 0.16 | 0.18 | 0.13 | 0.18 |
| QRange | 0.21 | 0.20 | 0.38 | 0.2 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Allegra, S.; Chiara, F.; Zanatta, M.; Mengozzi, G.; Puccinelli, M.P.; De Francia, S. Age and Sex-Related Differences in Teicoplanine Isoform Concentrations in SARS-CoV-2 Patients. Life 2023, 13, 1792. https://doi.org/10.3390/life13091792
Allegra S, Chiara F, Zanatta M, Mengozzi G, Puccinelli MP, De Francia S. Age and Sex-Related Differences in Teicoplanine Isoform Concentrations in SARS-CoV-2 Patients. Life. 2023; 13(9):1792. https://doi.org/10.3390/life13091792
Chicago/Turabian StyleAllegra, Sarah, Francesco Chiara, Marina Zanatta, Giulio Mengozzi, Maria Paola Puccinelli, and Silvia De Francia. 2023. "Age and Sex-Related Differences in Teicoplanine Isoform Concentrations in SARS-CoV-2 Patients" Life 13, no. 9: 1792. https://doi.org/10.3390/life13091792