

Tocilizumab Is Associated with Increased Risk of Fungal Infections among Critically Ill Patients with COVID-19 and Acute Renal Failure: An Observational Cohort Study

Abstract
:1. Background
2. Methods
3. Baseline Variables
4. Statistical Analysis
5. Results
5.1. Demographic and Clinical Characteristics
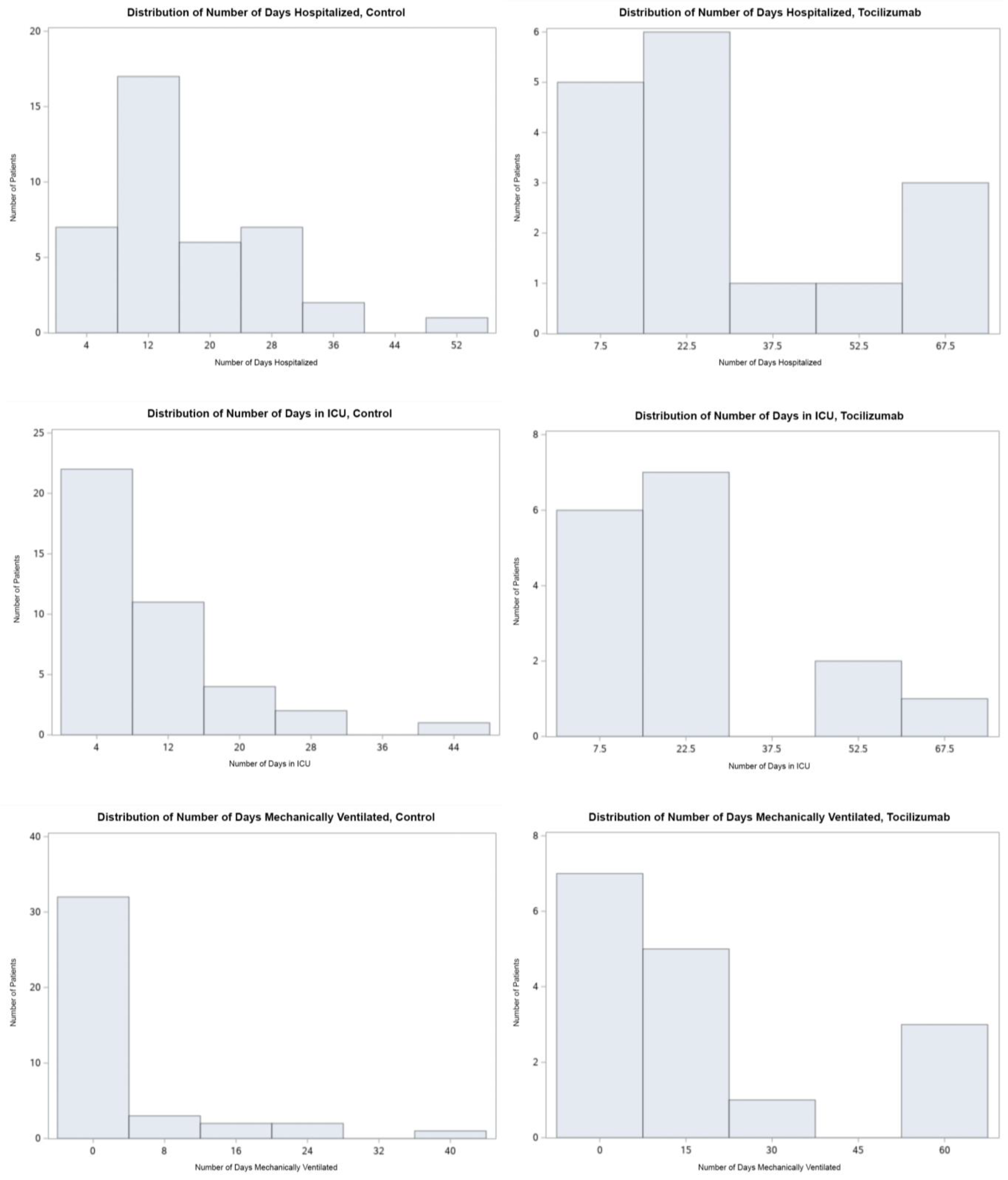
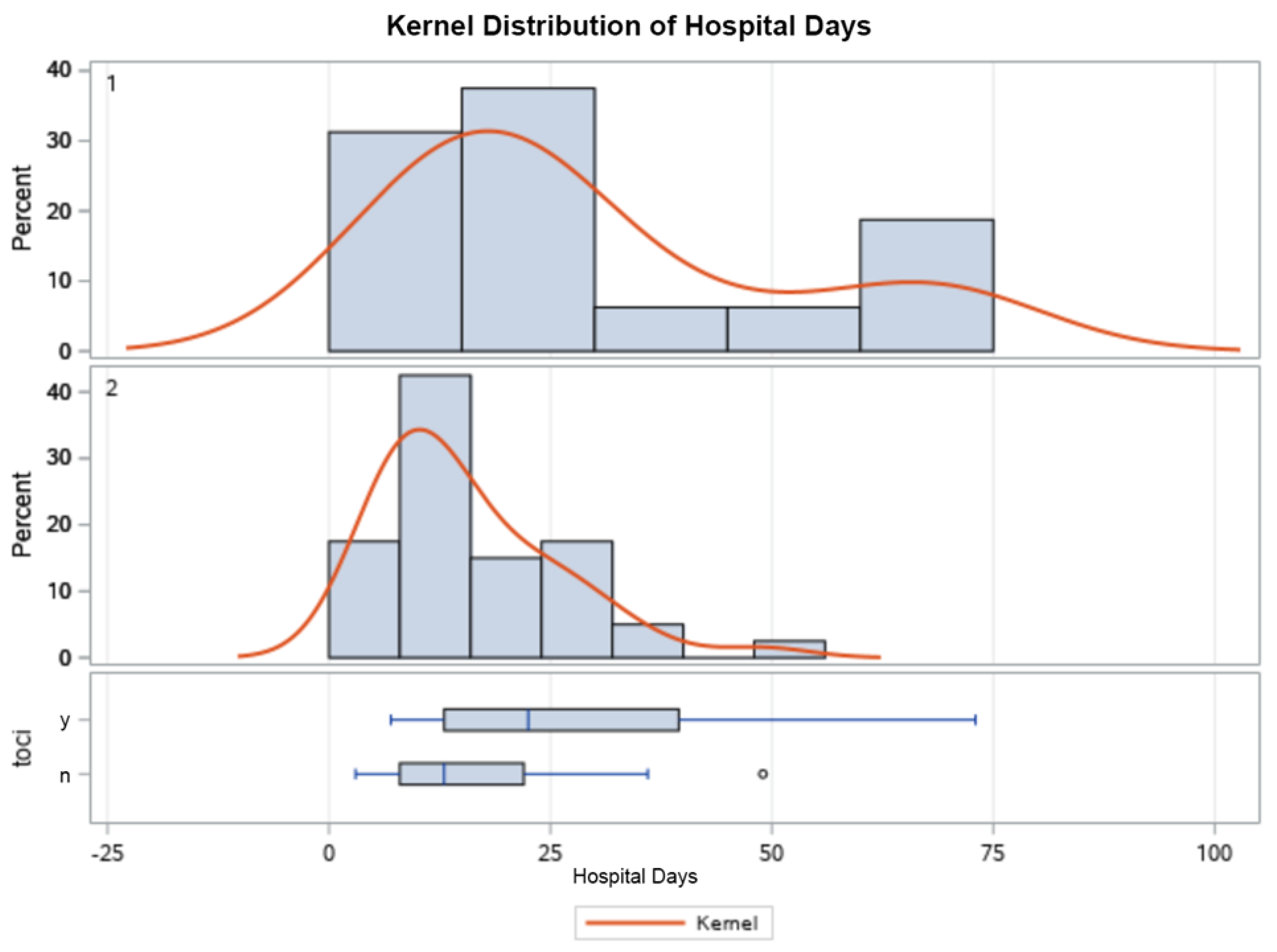
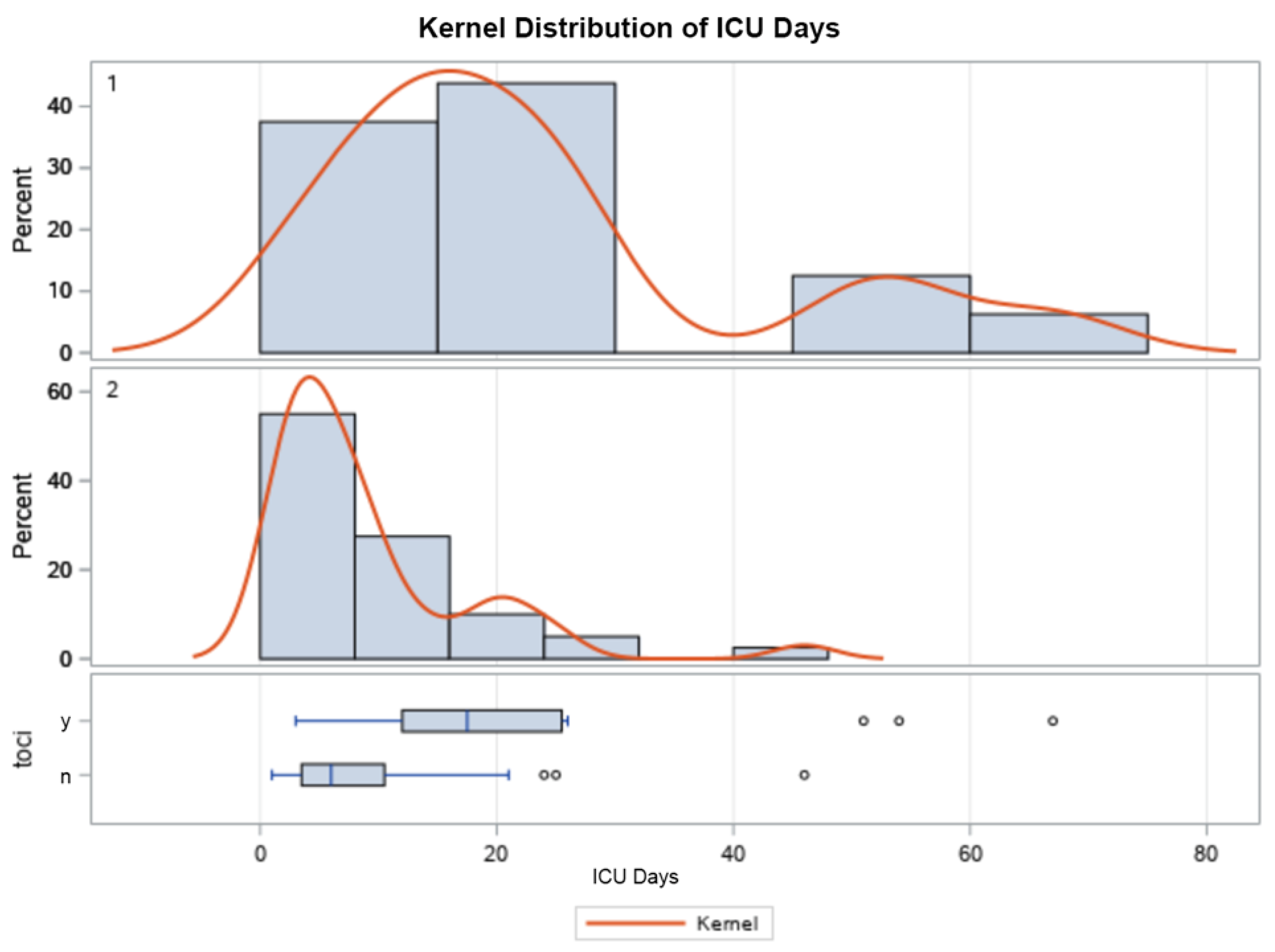
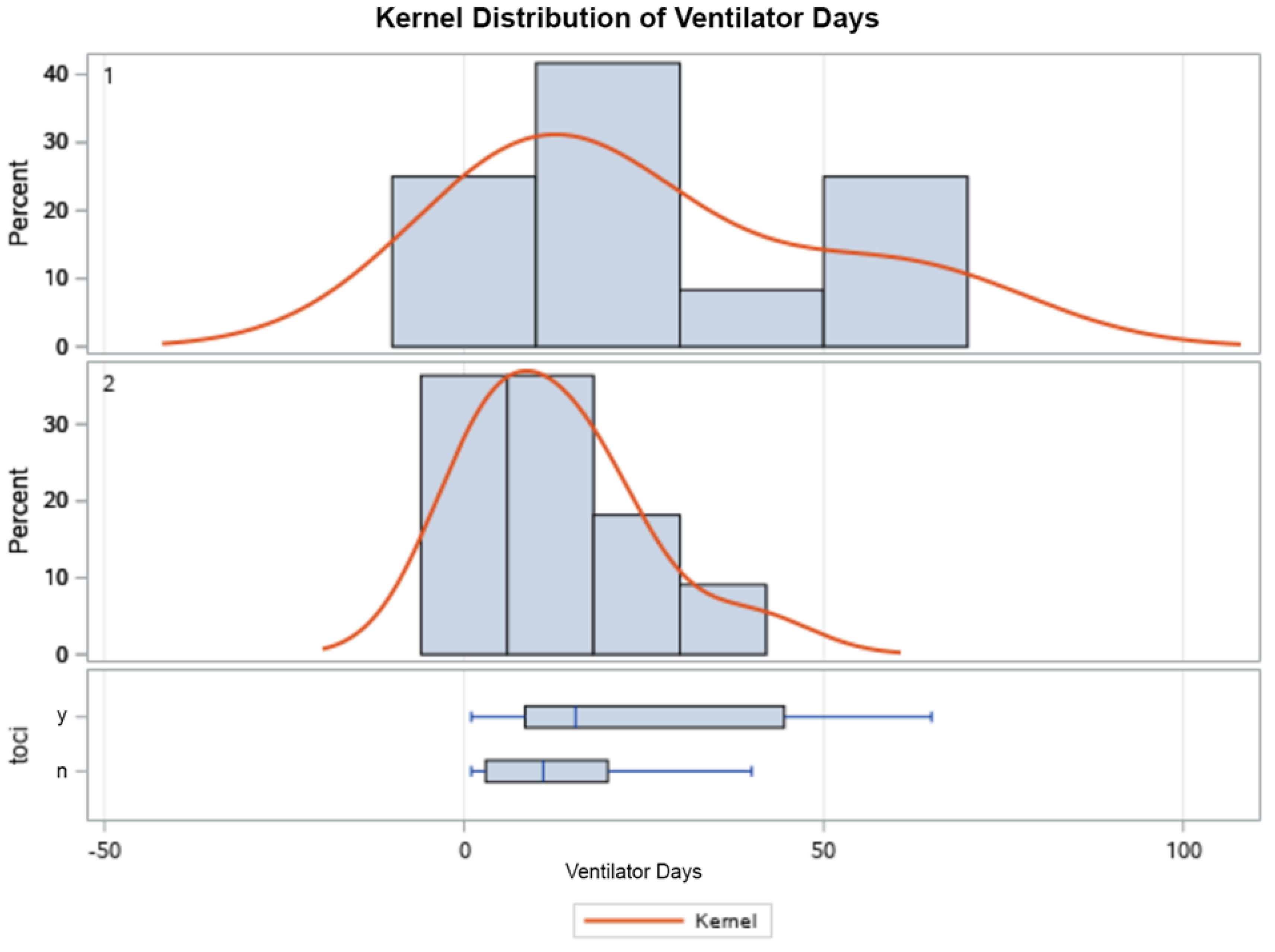
5.2. Clinical Outcomes
6. Interpretation
7. Discussion
8. Limitations
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| COVID-19 | coronavirus-2019 |
| SARS-CoV-2 | severe acute respiratory syndrome coronavirus-2 |
| IL-6 | interleukin-6 |
| ICU | intensive care unit |
| NIH | National Institutes of Health |
| MV | mechanical ventilation |
| LOS | length of stay |
| CRRT | continuous renal replacement therapy |
| RD | risk difference |
| WHO-CPS | World Health Organization-Combined Positive Score |
References
- Izda, V.; Jeffries, M.A.; Sawalha, A.H. COVID-19: A review of therapeutic strategies and vaccine candidates. Clin. Immunol. 2021, 222, 108634. [Google Scholar] [CrossRef]
- Campbell, L.; Chen, C.; Bhagat, S.; Parker, R.; Ostor, A. Risk of adverse events including serious infections in rheu-matoid arthritis patients treated with tocilizumab: A systematic literature review and meta-analysis of randomized controlled trials. Rheumatology 2011, 50, 552–562. [Google Scholar] [CrossRef]
- Sheppard, M.; Laskou, F.; Stapleton, P.P.; Hadavi, S.; Dasgupta, B. Tocilizumab (Actemra). Hum. Vaccines Immunother. 2017, 13, 1972–1988. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Li, M.; Zhou, Z.; Guan, X.; Xiang, Y. Can we use interleukin-6 (IL-6) blockade for coronavirus disease 2019 (COVID-19)-induced cytokine release syndrome (CRS)? J. Autoimmun. 2020, 111, 102452. [Google Scholar] [CrossRef] [PubMed]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W.; et al. Dysregulation of Immune Response in Patients With Coronavirus 2019 (COVID-19) in Wuhan, China. Clin. Infect. Dis. 2020, 71, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Zeng, F.; Huang, Y.; Guo, Y.; Yin, M.; Chen, X.; Xiao, L.; Deng, G. Association of inflammatory markers with the severity of COVID-19: A meta-analysis. Int. J. Infect. Dis. 2020, 96, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Toniati, P.; Piva, S.; Cattalini, M.; Garrafa, E.; Regola, F.; Castelli, F.; Franceschini, F.; Airò, P.; Bazzani, C.; Beindorf, E.-A.; et al. Tocilizumab for the treatment of severe COVID-19 pneumonia with hyperinflammatory syndrome and acute respiratory failure: A single center study of 100 patients in Brescia, Italy. Autoimmun. Rev. 2020, 19, 102568. [Google Scholar] [CrossRef]
- Sciascia, S.; Aprà, F.; Baffa, A.; Baldovino, S.; Boaro, D.; Boero, R.; Bonora, S.; Calcagno, A.; Cecchi, I.; Cinnirella, G.; et al. Pilot prospective open, single-arm multicentre study on off-label use of to-cilizumab in patients with severe COVID-19. Clin. Exp. Rheumatol. 2020, 38, 529–532. [Google Scholar]
- Guaraldi, G.; Meschiari, M.; Cozzi-Lepri, A.; Milic, J.; Tonelli, R.; Menozzi, M.; Franceschini, E.; Cuomo, G.; Orlando, G.; Borghi, V.; et al. Tocilizumab in patients with severe COVID-19: A retrospective cohort study. Lancet Rheumatol. 2020, 2, e474–e484. [Google Scholar] [CrossRef]
- Price, C.C.; Altice, F.L.; Shyr, Y.; Koff, A.; Pischel, L.; Goshua, G.; Azar, M.M.; Mcmanus, D.; Chen, S.-C.; Gleeson, S.E.; et al. Tocilizumab Treatment for Cytokine Release Syndrome in Hospitalized Patients With Coronavirus Disease 2019. Chest 2020, 158, 1397–1408. [Google Scholar] [CrossRef]
- Narain, S.; Stefanov, D.G.; Chau, A.S.; Weber, A.G.; Marder, G.; Kaplan, B.; Malhotra, P.; Bloom, O.; Liu, A.; Lesser, M.L.; et al. Comparative Survival Analysis of Immunomodulatory Therapy for Coronavirus Disease 2019 Cytokine Storm. Chest 2020, 159, 933–948. [Google Scholar] [CrossRef] [PubMed]
- Rosas, I.O.; Bräu, N.; Waters, M.; Go, R.C.; Hunter, B.D.; Bhagani, S.; Skiest, D.; Aziz, M.S.; Cooper, N.; Douglas, I.S.; et al. Tocilizumab in Hospitalized Patients with Severe Covid-19 Pneumonia. N. Engl. J. Med. 2021, 384, 1503–1516. [Google Scholar] [CrossRef] [PubMed]
- Somers, E.C.; Eschenauer, G.A.; Troost, J.P.; Golob, J.L.; Gandhi, T.N.; Wang, L.; Zhou, N.; Petty, L.A.; Baang, J.H.; Dillman, N.O.; et al. Tocilizumab for Treatment of Mechanically Ventilated Patients With COVID-19. Clin. Infect. Dis. 2021, 73, e445–e454. [Google Scholar] [CrossRef] [PubMed]
- Gordon, A.C.; Mouncey, P.R.; Al-Beidh, F.; Rowan, K.M.; Nichol, A.D.; Arabi, Y.M.; Annane, D.; Beane, A.; Van Bentum-Puijk, W.; Berry, L.R.; et al. Interleukin-6 Receptor Antagonists in Critically Ill Patients with COVID-19. N. Engl. J. Med. 2021, 384, 1491–1502. [Google Scholar] [CrossRef]
- Bartoletti, M.; Azap, O.; Barac, A.; Bussini, L.; Ergonul, O.; Krause, R.; Paño-Pardo, J.R.; Power, N.R.; Sibani, M.; Szabo, B.G.; et al. ESCMID COVID-19 living guidelines: Drug treatment and clinical management. Clin. Microbiol. Infect. 2022, 28, 222–238. [Google Scholar] [CrossRef] [PubMed]
- Tleyjeh, I.M.; Kashour, Z.; Damlaj, M.; Riaz, M.; Tlayjeh, H.; Altannir, M.; Altannir, Y.; Al-Tannir, M.; Tleyjeh, R.; Hassett, L.; et al. Efficacy and safety of tocilizumab in COVID-19 patients: A living systematic review and meta-analysis. Clin. Microbiol. Infect. 2020, 27, 215–227. [Google Scholar] [CrossRef]
- National Institutes of Health (n.d.). COVID-19 Treatment Guidelines. Therapeutic Management. Available online: https://www.covid19treatmentguidelines.nih.gov/therapeutic-management/ (accessed on 11 February 2021).
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Greenland, S.; Lash, T.; Rothman, K. Concepts of Interaction, 3rd ed.; Lippincott, Williams, and Wilkins: Philadelphia, PL, USA, 2008. [Google Scholar]
- Spiegelman, D.; Hertzmark, E. Easy SAS Calculations for Risk or Prevalence Ratios and Differences. Am. J. Epidemiol. 2005, 162, 199–200. [Google Scholar] [CrossRef]
- Bornstein, S.R.; Rubino, F.; Khunti, K.; Mingrone, G.; Hopkins, D.; Birkenfeld, A.L.; Boehm, B.; Amiel, S.; Holt, R.I.; Skyler, J.S.; et al. Practical recommendations for the management of diabetes in patients with COVID-19. Lancet Diabetes Endocrinol. 2020, 8, 546–550. [Google Scholar] [CrossRef]
- De Benedetti, F.; Brunner, H.I.; Ruperto, N.; Kenwright, A.; Wright, S.; Calvo, I.; Cuttica, R.; Ravelli, A.; Schneider, R.; Woo, P.; et al. Randomized Trial of Tocilizumab in Systemic Juvenile Idiopathic Arthritis. N. Engl. J. Med. 2012, 367, 2385–2395. [Google Scholar] [CrossRef] [PubMed]
- Grøn, K.L.; Glintborg, B.; Nørgaard, M.; Mehnert, F.; Østergaard, M.; Dreyer, L.; Krogh, N.S.; Hetland, M.L. Overall infection risk in rheumatoid arthritis during treatment with abatacept, rituximab and tocilizumab; an observational cohort study. Rheumatology 2020, 59, 1949–1956. [Google Scholar] [CrossRef]
- Hermine, O.; Mariette, X.; Tharaux, P.-L.; Resche-Rigon, M.; Porcher, R.; Ravaud, P.; Bureau, S.; Dougados, M.; Tibi, A.; CORIMUNO-19 Collaborative Group; et al. Effect of Tocilizumab vs. Usual Care in Adults Hospitalized With COVID-19 and Moderate or Severe Pneumonia: A Randomized Clinical Trial. JAMA Intern. Med. 2020, 181, 32–40. [Google Scholar] [CrossRef]
- WHO Working Group. A minimal common outcome measure set for COVID-19 clinical research. Lancet Infect. Dis. 2020, 20, e192–e197. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Wang, W.; Hayek, S.S.; Chan, L.; Mathews, K.S.; Melamed, M.L.; Brenner, S.K.; Leonberg-Yoo, A.; Schenck, E.J.; Radbel, J.; et al. Association Between Early Treatment With Tocilizumab and Mortality Among Critically Ill Patients With COVID-19. JAMA Intern. Med. 2020, 181, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Salvarani, C.; Dolci, G.; Massari, M.; Merlo, D.F.; Cavuto, S.; Savoldi, L.; Bruzzi, P.; Boni, F.; Braglia, L.; Turrà, C.; et al. Effect of Tocilizumab vs. Standard Care on Clinical Worsening in Patients Hospitalized With COVID-19 Pneumonia: A Randomized Clinical Trial. JAMA Intern. Med. 2020, 181, 24–31. [Google Scholar] [CrossRef]
- Stone, J.H.; Frigault, M.J.; Serling-Boyd, N.J.; Fernandes, A.D.; Harvey, L.; Foulkes, A.S.; Horick, N.K.; Healy, B.C.; Shah, R.; Bensaci, A.M.; et al. Efficacy of Tocilizumab in Patients Hospitalized with Covid-19. N. Engl. J. Med. 2020, 383, 2333–2344. [Google Scholar] [CrossRef] [PubMed]
- Veiga, V.C.; Prats, J.A.G.G.; Farias, D.L.C.; Rosa, R.G.; Dourado, L.K.; Zampieri, F.G.; Machado, F.R.; Lopes, R.D.; Berwanger, O.; Azevedo, L.C.P.; et al. Effect of tocilizumab on clinical outcomes at 15 days in patients with severe or critical coronavirus disease 2019: Randomised controlled trial. BMJ 2021, 372. [Google Scholar] [CrossRef]
- Antinori, S.; Bonazzetti, C.; Gubertini, G.; Capetti, A.; Pagani, C.; Morena, V.; Rimoldi, S.; Galimberti, L.; Sarzi-Puttini, P.; Ridolfo, A.L. Tocilizumab for cytokine storm syndrome in COVID-19 pneumonia: An increased risk for candidemia? Autoimmun. Rev. 2020, 19, 102564. [Google Scholar] [CrossRef]
- Minihan, B.; McAuliffe, E.; Powell, J.; Wong, S.; Wilkie, K.; Murphy, C.; Maher, A.; Power, L.; O’Connell, N.; Dunne, C. Association between tocilizumab treatment of hyperinflammatory patients with COVID-19 in a critical care setting and elevated incidence of hospital-acquired bacterial and invasive fungal infections. J. Hosp. Infect. 2022, 126, 29–36. [Google Scholar] [CrossRef]
- Ronco, C.; Reis, T.; Husain-Syed, F. Management of acute kidney injury in patients with COVID-19. Lancet Respir. Med. 2020, 8, 738–742. [Google Scholar] [CrossRef]
- E Leaf, D.; Gupta, S.; Wang, W. Tocilizumab in Covid-19. N. Engl. J. Med. 2021, 384, 86–87. [Google Scholar] [CrossRef]
- Kimmig, L.M.; Wu, D.; Gold, M.; Pettit, N.N.; Pitrak, D.; Mueller, J.; Husain, A.N.; Mutlu, E.A.; Mutlu, G.M. IL-6 Inhibition in Critically Ill COVID-19 Patients Is Associated With Increased Secondary Infections. Front. Med. 2020, 28, 583897. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 56) | Control (n = 40) | Tocilizumab (n = 16) | |
|---|---|---|---|
| Demographics | |||
| Gender, n (%) | |||
| Female, n (%) | 27 (48.2) | 21 (52.5) | 6 (37.5) |
| Age, median (IQR) | 60 (22.0) | 60 (24.5) | 58 (19.5) |
| Race, n (%) | |||
| Black, n (%) | 20 (35.7) | 14 (35.0) | 6 (37.5) |
| White, n (%) | 23 (41.1) | 19 (47.5) | 4 (25.0) |
| Hispanic, n (%) | 10 (17.9) | 4 (10.0) | 6 (37.5) |
| Other, n (%) | 3 (5.3) | 3 (7.5) | 0 (0) |
| Comorbid disease, n (%) | |||
| Diabetes, n (%) | 25 (44.6) | 17 (42.5) | 8 (50) |
| Chronic liver disease, n (%) | 1 (1.8) | 1 (2.5) | 0 (0) |
| Renal failure, requiring replacement therapy, n (%) | 10 (17.9) | 4 (10.0) | 6 (37.5) |
| Laboratory results, maximum value while in ICU, median (IQR) | |||
| AST U/L (IQR) | 44 (62) | 48.5 (63) | 42.5 (67) |
| ALT U/L (IQR) | 47 (70) | 45 (66) | 48 (82) |
| Total bilirubin mg/dL (IQR) | 0.9 (0.7) | 0.9 (0.7) | 1.1 (0.8) |
| Received TPN while inpatient, n (%) | 1 (1.9) | 1 (2.5) | 0 (0) |
| Indwelling central catheter, n (%) | 26 (65) | 15 (37.5) | 11 (73.3) |
| APACHE II score > 20, n (%) | 7 (12.5) | 3 (15.0) | 4 (28.6) |
| APACHE II score (IQR) | 14 (9) | 15 (9) | 12.5 (8) |
| Continuous Renal Replacement Therapy (CRRT) | Tocilizumab | RDs (95% CI) for Tocilizumab within CRRT Strata | |||
|---|---|---|---|---|---|
| No | Yes | ||||
| Fungal Infection | Patients | Fungal Infections | Patients | ||
| No | 1 | 36 | 0 | 9 | −2.8 (−8.1, 2.6) |
| RD (95% CI) | 0 | −2.8 (−8.1, 2.6) | p = 1.0 | ||
| (Referent) | p = 1.0 | ||||
| Yes | 0 | 4 | 5 | 6 | 83.3 (53.5, 113.2) |
| RD (95% CI) | −2.8 (−8.1, 2.6) | 80.6 (50.3, 100.0) | p < 0.01 | ||
| p = 1.0 | p < 0.01 | ||||
| Characteristic | All Patients (n = 56) | Control (n = 40) | Tocilizumab (n = 16) |
|---|---|---|---|
| Hospital LOS, median days (IQR) | 14 (15.5) | 13 (14) | 22.5 (26) |
| ICU LOS, median days (IQR) | 8 (14.5) | 6 (7) | 17.5 (16) |
| Mechanically ventilated, n (%) | 23 (41.1) | 11 (27.5) | 12 (75) |
| Duration of MV 1, median days (IQR) | 14 (16) | 11 (17) | 15.5 (35) |
| Death 2, n (%) | 18 (32) | 11 (27.5) | 7 (43.7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burger, B.J.; Epps, S.M.; Cardenas, V.M.; Jagana, R.; Meena, N.K.; Atchley, W.T. Tocilizumab Is Associated with Increased Risk of Fungal Infections among Critically Ill Patients with COVID-19 and Acute Renal Failure: An Observational Cohort Study. Life 2023, 13, 1752. https://doi.org/10.3390/life13081752
Burger BJ, Epps SM, Cardenas VM, Jagana R, Meena NK, Atchley WT. Tocilizumab Is Associated with Increased Risk of Fungal Infections among Critically Ill Patients with COVID-19 and Acute Renal Failure: An Observational Cohort Study. Life. 2023; 13(8):1752. https://doi.org/10.3390/life13081752
Chicago/Turabian StyleBurger, Barrett J., Sarenthia M. Epps, Victor M. Cardenas, Rajani Jagana, Nikhil K. Meena, and William T. Atchley. 2023. "Tocilizumab Is Associated with Increased Risk of Fungal Infections among Critically Ill Patients with COVID-19 and Acute Renal Failure: An Observational Cohort Study" Life 13, no. 8: 1752. https://doi.org/10.3390/life13081752