

Effects of a Home-Based Physical Activity Program on Blood Biomarkers and Health-Related Quality of Life Indices in Saudi Arabian Type 2 Diabetes Mellitus Patients: A Randomized Controlled Trial
 , ,
, ,  ,
,
Abstract
:1. Introduction
1.1. Rationale
1.2. Aims
1.3. Hypotheses
2. Materials and Methods
2.1. Study Design and Setting
2.2. Inclusion and Exclusion Criteria
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
2.3. Sample Size
2.4. Ethical Approval
2.5. Participants and Recruitment
2.6. Intervention
2.6.1. Home Based Physical Activity
2.6.2. Control Group
2.7. Data Collection
2.7.1. Demographic and Health Information
2.7.2. Anthropometric Measurements
2.7.3. Blood Pressure
2.7.4. Blood Biomarkers
2.7.5. Physical Fitness
2.7.6. Patient-Reported Outcome Measures
2.8. Statistical Analysis
3. Results
3.1. Demographic and Health Information
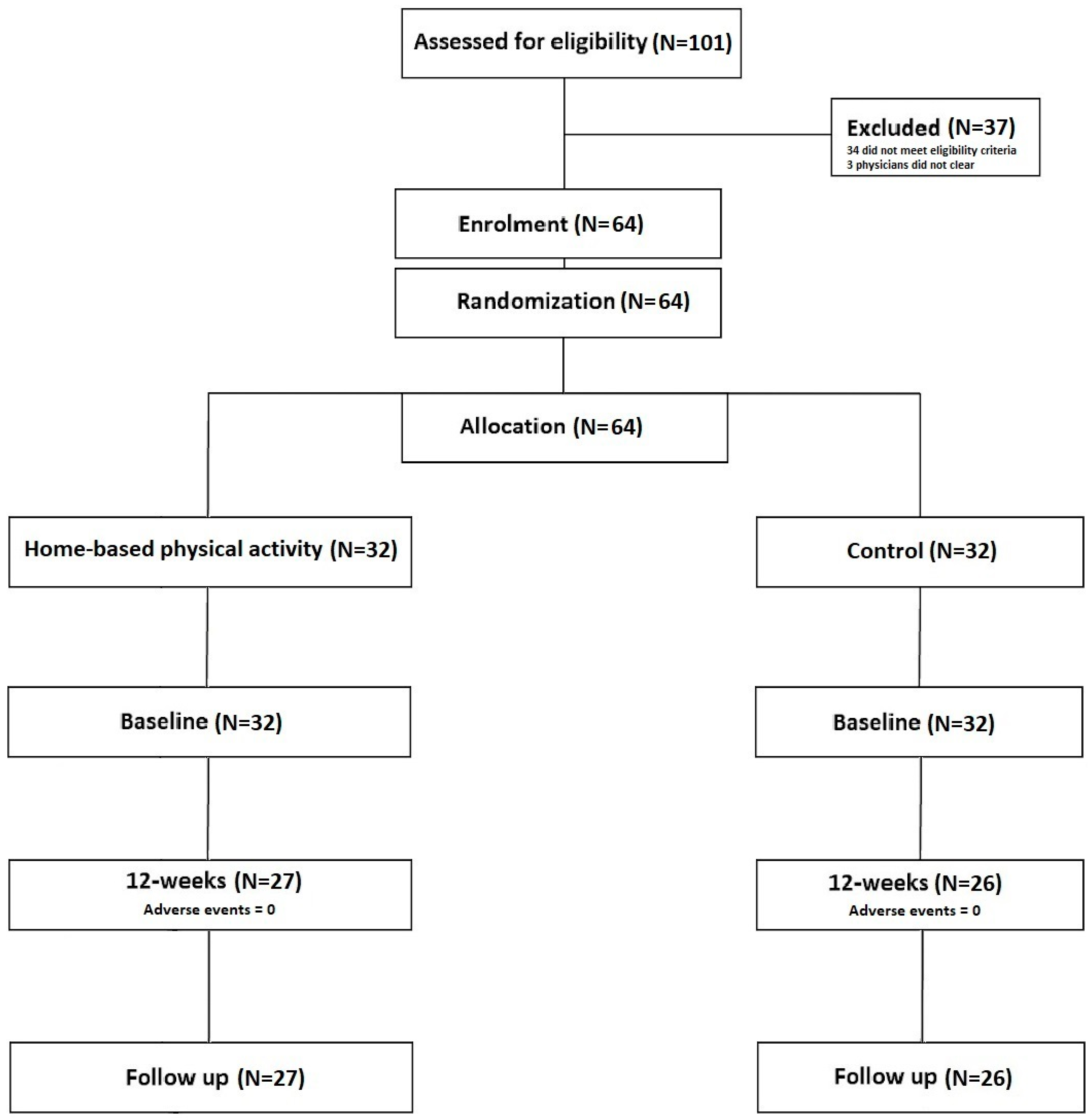
3.2. Compliance, Loss to Follow Up, and Adverse Events

{kind=link}
| Total | Control | Home-Based Physical Activity | ||||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |
| Sex | Male = 48.4% | Male = 46.9% | Male = 50.0% | |||
| Female = 51.6% | Female = 53.1% | Female = 50.0% | ||||
| Age (yrs) | 44.10 | 9.22 | 45.88 | 8.51 | 42.07 | 9.72 |
| Mass (kg) | 75.44 | 14.35 | 76.30 | 15.16 | 74.58 | 13.67 |
| Stature (cm) | 159.77 | 9.13 | 160.59 | 8.94 | 158.94 | 9.38 |
| BMI (kg/m2) | 29.59 | 5.35 | 29.73 | 6.24 | 29.44 | 4.38 |
| Smoking status | Yes = 12.5% | Yes = 15.6% | Yes = 9.4% | |||
| No = 78.1% | No = 78.1% | No = 78.1% | ||||
| Previous = 9.4% | Previous = 6.3% | Previous = 12.5% | ||||
| Marital status | Married = 84.4% Widowed = 4.7% Divorced = 3.1% Single = 7.8% | Married = 75.0% Widowed = 9.4% Divorced = 3.1 Single = 12.5% | Married = 93.8% Divorced = 3.1% Single = 3.1% | |||
| Children | 0 = 17.2% 1 = 3.1% 2 = 9.4% 3 = 14.1% 4 = 9.4% 5 = 9.4% 6+ = 37.5% | 0 = 21.9% 2 = 9.4% 3 = 14.1% 4 = 9.4% 5 = 9.4% 6+ = 37.5% | 0 = 12.5% 1 = 6.3% 2 = 9.4% 3 = 15.6% 4 = 12.5% 5 = 9.4% 6+ = 34.4% | |||
| Years since diagnosis | 9.77 | 7.38 | 8.12 | 6.22 | 12.17 | 8.38 |
| Ethnicity | Arab = 98.4%, African = 1.6% | Arab = 96.9%, African = 3.1% | Arab = 100% | |||
| Diabetes medication | Metformin = 81.3% | Metformin = 84.4% | Metformin = 78.1%, | |||
| Sitagliptin = 17.2% | Sitagliptin = 31.3% | Sitagliptin = 3.1% | ||||
| Insulin = 43.8%, | Insulin = 56.3% | Insulin = 31.3% | ||||
| Empagliflozin =9.4% | Empagliflozin =12.5% | Empagliflozin =6.3% | ||||
| Blood pressure lowering medication | Yes = 39.1% | Yes = 46.9% | Yes = 31.3% | |||
| No = 60.9% | No = 53.1% | No = 68.7% | ||||
| Education | Less than high school = 26.6% | Less than high school = 26.6% | Less than high school = 18.8% | |||
| High school = 20.3% | High school = 20.3% | High school = 21.9% | ||||
| Associates degree = 20.3% | Associates degree = 20.3% | Associates degree = 25.0% | ||||
| Bachelor’s degree = 31.3% | Bachelor’s degree = 31.3% | Bachelor’s degree = 31.3% | ||||
| Doctoral = 1.6% | Doctoral = 1.6% | Doctoral = 3.1% | ||||
3.3. Anthropometric Measurements
3.4. Blood Pressure
3.5. Physical Fitness
3.6. Patient-Reported Outcome Measures
3.7. Blood Biomarkers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Olokoba, A.B.; Obateru, O.A.; Olokoba, L.B. Type 2 diabetes mellitus: A review of current trends. Oman Med. J. 2012, 27, 269–274. [Google Scholar] [CrossRef]
- Magliano, D.J.; Boyko, E.J.; Atlas, I.D. What is diabetes? In IDF DIABETES ATLAS, 10th ed.; International Diabetes Federation: Brussels, Belgium, 2021. [Google Scholar]
- Zimmet, P.Z.; Magliano, D.J.; Herman, W.H.; Shaw, J.E. Diabetes: A 21st century challenge. Lancet Diabetes Endocrinol. 2014, 2, 56–64. [Google Scholar] [CrossRef]
- Robertson, R.P. Antagonist: Diabetes and insulin resistance-philosophy, science, and the multiplier hypothesis. J. Lab. Clin. Med. 1995, 125, 560–564. [Google Scholar]
- Blas, E.; Kurup, A.S. Equity, Social Determinants and Public Health Programmes; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Galaviz, K.I.; Narayan, K.V.; Lobelo, F.; Weber, M.B. Lifestyle and the prevention of type 2 diabetes: A status report. Am. J. Lifestyle Med. 2018, 12, 4–20. [Google Scholar] [CrossRef]
- Schmidt, M.I.; Duncan, B.B.; Ishitani, L.; da Conceição Franco, G.; de Abreu, D.M.X.; Lana, G.C.; França, E. Trends in mortality due to diabetes in Brazil, 1996–2011. Diabetol. Metab. Syndr. 2015, 7, 109–116. [Google Scholar] [CrossRef] [Green Version]
- Majeed, A.; El-Sayed, A.A.; Khoja, T.; Alshamsan, R.; Millett, C.; Rawaf, S. Diabetes in the Middle-East and North Africa: An update. Diabetes Res. Clin. Pract. 2014, 103, 218–222. [Google Scholar] [CrossRef]
- Meo, S.A. Prevalence and future prediction of type 2 diabetes mellitus in the Kingdom of Saudi Arabia: A systematic review of published studies. JPMA J. Pak. Med. Assoc. 2016, 66, 722–725. [Google Scholar]
- Abdulaziz, A.L.; Dawish, M.; Alwin Robert, A.; Braham, R.; Abdallah Al Hayek, A.; Al Saeed, A.; Ahmed Ahmed, R.; Sulaiman Al Sabaan, F. Diabetes mellitus in Saudi Arabia: A review of the recent literature. Curr. Diabetes Rev. 2016, 12, 359–368. [Google Scholar] [CrossRef]
- Sherif, S.; Sumpio, B.E. Economic development and diabetes prevalence in MENA countries: Egypt and Saudi Arabia comparison. World J. Diabetes 2015, 6, 304–311. [Google Scholar] [CrossRef]
- Mokdad, A.H.; Tuffaha, M.; Hanlon, M.; El Bcheraoui, C.; Daoud, F.; Al Saeedi, M.; Basulaiman, M. Cost of diabetes in the Kingdom of Saudi Arabia, 2014. J. Diabetes Metab. 2015, 6, 575. [Google Scholar]
- Alwin Robert, A.; Abdulaziz Al Dawish, M.; Braham, R.; Ali Musallam, M.; Abdullah Al Hayek, A.; Hazza Al Kahtany, N. Type 2 diabetes mellitus in Saudi Arabia: Major challenges and possible solutions. Curr. Diabetes Rev. 2017, 13, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Al-Hazzaa, H.M. Physical inactivity in Saudi Arabia revisited: A systematic review of inactivity prevalence and perceived barriers to active living. Int. J. Health Sci. 2018, 12, 50–64. [Google Scholar]
- World Health Organization (WHO). Global Recommendations on Physical Activity for Health; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Lee, I.M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef] [Green Version]
- Silva, D.A.S.; Naghavi, M.; Duncan, B.B.; Schmidt, M.I.; de Souza, M.D.F.M.; Malta, D.C. Physical inactivity as risk factor for mortality by diabetes mellitus in Brazil in 1990, 2006, and 2016. Diabetol. Metab. Syndr. 2019, 11, 23–28. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Global Action Plan on Physical Activity 2018–2030; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- World Health Organization (WHO). Global Action Plan for the Prevention and Control of NCDs. 2013–2020; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- Al-Hazzaa, H.M. The public health burden of physical inactivity in Saudi Arabia. J. Fam. Community Med. 2004, 11, 45–51. [Google Scholar]
- Yavari, A. Glycosylated Hemoglobin: The importance in management of type 2 diabetes. J. Stress Physiol. Biochem. 2011, 7, 122–129. [Google Scholar]
- Najafipour, F.; Mobasseri, M.; Yavari, A.; Nadrian, H.; Aliasgarzadeh, A.; Abbasi, N.M.; Sadra, V. Effect of regular exercise training on changes in HbA1c, BMI and VO2max among patients with type 2 diabetes mellitus: An 8-year trial. BMJ Open Diabetes Res. Care 2017, 5, e000414. [Google Scholar] [CrossRef] [Green Version]
- Zinman, B.; Ruderman, N.; Campaigne, B.N.; Devlin, J.T.; Schneider, S.H. Physical activity/exercise and diabetes mellitus. Diabetes Care 2003, 26, 73–77. [Google Scholar]
- Yan, H.; Prista, A.; Ranadive, S.M.; Damasceno, A.; Caupers, P.; Kanaley, J.A.; Fernhall, B. Effect of aerobic training on glucose control and blood pressure in T2DDM East African males. Int. Sch. Res. Not. 2014, 2014, 864897. [Google Scholar] [CrossRef]
- Yavari, A.; Hajiyev, A.M.; Naghizadeh, F. The effect of aerobic exercise on glycosylated hemoglobin values in type 2 diabetes patients. J. Sport. Med. Phys. Fit. 2010, 50, 501–505. [Google Scholar]
- O’Donovan, G.; Kearney, E.M.; Nevill, A.M.; Woolf-May, K.; Bird, S.R. The effects of 24 weeks of moderate-or high-intensity exercise on insulin resistance. Eur. J. Appl. Physiol. 2005, 95, 522–528. [Google Scholar] [CrossRef]
- Winnick, J.J.; Sherman, W.M.; Habash, D.L.; Stout, M.B.; Failla, M.L.; Belury, M.A.; Schuster, D.P. Short-term aerobic exercise training in obese humans with type 2 diabetes mellitus improves whole-body insulin sensitivity through gains in peripheral, not hepatic insulin sensitivity. J. Clin. Endocrinol. Metab. 2008, 93, 771–778. [Google Scholar] [CrossRef] [Green Version]
- Motahari-Tabari, N.; Shirvani, M.A.; Shirzad-e-Ahoodashty, M.; Yousefi-Abdolmaleki, E.; Teimourzadeh, M. The effect of 8 weeks aerobic exercise on insulin resistance in type 2 diabetes: A randomized clinical trial. Glob. J. Health Sci. 2015, 7, 115–121. [Google Scholar] [CrossRef] [Green Version]
- Cuff, D.J.; Meneilly, G.S.; Martin, A.; Ignaszewski, A.; Tildesley, H.D.; Frohlich, J.J. Effective exercise modality to reduce insulin resistance in women with type 2 diabetes. Diabetes Care 2003, 26, 2977–2982. [Google Scholar] [CrossRef] [Green Version]
- Church, T.S.; Blair, S.N.; Cocreham, S.; Johannsen, N.; Johnson, W.; Kramer, K.; Earnest, C.P. Effects of aerobic and resistance training on hemoglobin A1c levels in patients with type 2 diabetes: A randomized controlled trial. JAMA 2010, 304, 2253–2262. [Google Scholar] [CrossRef] [Green Version]
- Tessier, D.; Ménard, J.; Fülöp, T.; Ardilouze, J.L.; Roy, M.A.; Dubuc, N.; Gauthier, P. Effects of aerobic physical exercise in the elderly with type 2 diabetes mellitus. Arch. Gerontol. Geriatr. 2000, 31, 121–132. [Google Scholar] [CrossRef]
- Balducci, S.; Iacobellis, G.; Parisi, L.; Di Biase, N.; Calandriello, E.; Leonetti, F.; Fallucca, F. Exercise training can modify the natural history of diabetic peripheral neuropathy. J. Diabetes Its Complicat. 2006, 20, 216–223. [Google Scholar] [CrossRef]
- Dixit, S.; Maiya, A.G.; Shastry, B.A. Effect of aerobic exercise on peripheral nerve functions of population with diabetic peripheral neuropathy in type 2 diabetes: A single blind, parallel group randomized controlled trial. J. Diabetes Its Complicat. 2014, 28, 332–339. [Google Scholar] [CrossRef]
- Dunstan, D.W.; Daly, R.M.; Owen, N.; Jolley, D.; De Courten, M.; Shaw, J.; Zimmet, P. High-intensity resistance training improves glycemic control in older patients with type 2 diabetes. Diabetes Care 2002, 25, 1729–1736. [Google Scholar] [CrossRef] [Green Version]
- Castaneda, C.; Layne, J.E.; Munoz-Orians, L.; Gordon, P.L.; Walsmith, J.; Foldvari, M.; Nelson, M.E. A randomized controlled trial of resistance exercise training to improve glycemic control in older adults with type 2 diabetes. Diabetes Care 2002, 25, 2335–2341. [Google Scholar] [CrossRef] [Green Version]
- Sigal, R.J.; Kenny, G.P.; Boulé, N.G.; Wells, G.A.; Prud’homme, D.; Fortier, M.; Jaffey, J. Effects of aerobic training, resistance training, or both on glycemic control in type 2 diabetes: A randomized trial. Ann. Intern. Med. 2007, 147, 357–369. [Google Scholar] [CrossRef] [PubMed]
- Shenoy, S.; Arora, E.; Jaspal, S. Effects of progressive resistance training and aerobic exercise on type 2 diabetics in Indian population. Dubai Diabetes Endocrinol. J. 2009, 17, 27–30. [Google Scholar]
- Yavari, A.; Najafipoor, F.; Aliasgarzadeh, A.; Niafar, M.; Mobasseri, M. Effect of aerobic exercise, resistance training or combined training on glycaemic control and cardio-vascular risk factors in patients with type 2 diabetes. Biol. Sport 2012, 29, 135–143. [Google Scholar] [CrossRef] [Green Version]
- Dunstan, D.W.; Puddey, I.B.; Beilin, L.J.; Burke, V.; Morton, A.R.; Stanton, K.G. Effects of a short-term circuit weight training program on glycaemic control in NIDDM. Diabetes Res. Clin. Pract. 1998, 40, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Baldi, J.C.; Snowling, N. Resistance training improves glycaemic control in obese type 2 diabetic men. Int. J. Sport. Med. 2003, 24, 419–423. [Google Scholar]
- Tokmakidis, S.P.; Zois, C.E.; Volaklis, K.A.; Kotsa, K.; Touvra, A.M. The effects of a combined strength and aerobic exercise program on glucose control and insulin action in women with type 2 diabetes. Eur. J. Appl. Physiol. 2004, 92, 437–442. [Google Scholar] [CrossRef]
- Terauchi, Y.; Takada, T.; Yoshida, S. A randomized controlled trial of a structured program combining aerobic and resistance exercise for adults with type 2 diabetes in Japan. Diabetol. Int. 2022, 13, 75–84. [Google Scholar] [CrossRef]
- Amin, T.T.; Suleman, W.; Ali, A.; Gamal, A.; Al Wehedy, A. Pattern, prevalence, and perceived personal barriers toward physical activity among adult Saudis in Al-Hassa, KSA. J. Phys. Act. Health 2011, 8, 775–784. [Google Scholar] [CrossRef]
- Al-Otaibi, H.H. Measuring stages of change, perceived barriers and self efficacy for physical activity in Saudi Arabia. Asian Pac. J. Cancer Prev. 2013, 14, 1009–1016. [Google Scholar] [CrossRef] [Green Version]
- Al-Rafaee, S.A.; Al-Hazzaa, H.M. Physical activity profile of adult males in Riyadh City. Saudi Med. J. 2001, 22, 784–978. [Google Scholar]
- Mandil, A.M.; Alfurayh, N.A.; Aljebreen, M.A.; Aldukhi, S.A. Physical activity and major non-communicable diseases among physicians in Central Saudi Arabia. Saudi Med. J. 2016, 37, 1243–1250. [Google Scholar] [CrossRef]
- Benjamin, K.; Donnelly, T.T. Barriers and facilitators influencing the physical activity of Arabic adults: A literature review. Avicenna 2013, 2013, 8–13. [Google Scholar] [CrossRef]
- Lee, M.K.; Kim, N.K.; Jeon, J.Y. Effect of the 6-week home-based exercise program on physical activity level and physical fitness in colorectal cancer survivors: A randomized controlled pilot study. PLoS ONE 2018, 13, e0196220. [Google Scholar] [CrossRef] [Green Version]
- Sinclair, J.; Ageely, H.; Mahfouz, M.S.; Hummadi, A.A.; Darraj, H.; Solan, Y.; Bottoms, L. Effects of a home-based physical activity programme on blood biomarkers and health-related quality of life indices in Saudi Arabian type-2 diabetes mellitus patients: Protocol for a randomised controlled trial. Int. J. Environ. Res. Public Health 2022, 19, 4468. [Google Scholar] [CrossRef]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Altman, D.G. CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. Int. J. Surg. 2012, 10, 28–55. [Google Scholar] [CrossRef] [Green Version]
- Mahfouz, M.S.; Rahim, B.E.E.; Solan, Y.M.; Makeen, A.M.; Alsanosy, R.M. Khat chewing habits in the population of the Jazan region, Saudi Arabia: Prevalence and associated factors. PLoS ONE 2015, 10, e0134545. [Google Scholar] [CrossRef]
- Nano, J.A.N.A.; Carinci, F.; Okunade, O.; Whittaker, S.; Walbaum, M.; Barnard-Kelly, K.; Diabetes Working Group of the International Consortium for Health Outcomes Measurement (ICHOM). A standard set of person-centred outcomes for diabetes mellitus: Results of an international and unified approach. Diabet. Med. 2020, 37, 2009–2018. [Google Scholar] [CrossRef] [Green Version]
- Santos, A.; Lonsdale, C.; Lubans, D.; Vasconcellos, D.; Kapsal, N.; Vis-Dunbar, M.; Jung, M.E. Rates of compliance and adherence to high-intensity interval training in insufficiently active adults: A systematic review and meta-analysis protocol. Syst. Rev. 2020, 9, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Czernichow, S.; Kengne, A.P.; Huxley, R.R.; Batty, G.D.; De Galan, B.; Grobbee, D.; ADVANCE Collaborative Group. Comparison of waist-to-hip ratio and other obesity indices as predictors of cardiovascular disease risk in people with type-2 diabetes: A prospective cohort study from ADVANCE. Eur. J. Prev. Cardiol. 2011, 18, 312–319. [Google Scholar] [CrossRef]
- O’Brien, E.; Asmar, R.; Beilin, L.; Imai, Y.; Mallion, J.M.; Mancia, G.; European Society of Hypertension Working Group on Blood Pressure Monitoring. European Society of Hypertension recommendations for conventional, ambulatory and home blood pressure measurement. J. Hypertens. 2003, 21, 821–848. [Google Scholar] [CrossRef]
- Pickering, T.G.; Hall, J.E.; Appel, L.J.; Falkner, B.E.; Graves, J.; Hill, M.N.; Roccella, E.J. Recommendations for blood pressure measurement in humans and experimental animals: Part 1: Blood pressure measurement in humans: A statement for professionals from the Subcommittee of Professional and Public Education of the American Heart Association Council on High Blood Pressure Research. Hypertension 2005, 45, 142–161. [Google Scholar] [PubMed]
- Millán, J.; Pintó, X.; Muñoz, A.; Zúñiga, M.; Rubiés-Prat, J.; Pallardo, L.F.; Pedro-Botet, J. Lipoprotein ratios: Physiological significance and clinical usefulness in cardiovascular prevention. Vasc. Health Risk Manag. 2009, 5, 757–765. [Google Scholar] [PubMed]
- Lopez-Jaramillo, P.; Gomez-Arbelaez, D.; Martinez-Bello, D.; Abat, M.E.M.; Alhabib, K.F.; Avezum, Á.; Barbarash, O.; Chifamba, J.; Diaz, M.L.; Gulec, S.; et al. Association of the triglyceride glucose index as a measure of insulin resistance with mortality and cardiovascular disease in populations from five continents (PURE study): A prospective cohort study. Lancet Healthy Longev. 2023, 4, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Colberg, S.R.; Sigal, R.J.; Fernhall, B.; Regensteiner, J.G.; Blissmer, B.J.; Rubin, R.R.; Braun, B. Exercise and type 2 diabetes: The American College of Sports Medicine and the American Diabetes Association: Joint position statement. Diabetes Care 2010, 33, 147–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buckley, J.P.; Sim, J.; Eston, R.G.; Hession, R.; Fox, R. Reliability and validity of measures taken during the Chester step test to predict aerobic power and to prescribe aerobic exercise. Br. J. Sport. Med. 2004, 38, 197–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khandelwal, D.; Dutta, D.; Chittawar, S.; Kalra, S. Sleep disorders in type 2 diabetes. Indian J. Endocrinol. Metab. 2017, 21, 758–761. [Google Scholar] [PubMed]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Well-Being Index: A systematic review of the literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Venkataraman, K.; Tan, L.S.M.; Bautista, D.C.T.; Griva, K.; Zuniga, Y.L.M.; Amir, M.; Wee, H.L. Psychometric properties of the problem areas in diabetes (PAID) instrument in Singapore. PLoS ONE 2015, 10, e0136759. [Google Scholar] [CrossRef] [Green Version]
- Backhaus, J.; Junghanns, K.; Broocks, A.; Riemann, D.; Hohagen, F. Test–retest reliability and validity of the Pittsburgh Sleep Quality Index in primary insomnia. J. Psychosom. Res. 2002, 53, 737–740. [Google Scholar] [CrossRef]
- Sinclair, J.; Stainton, P.; Dillon, S.; Taylor, P.J.; Richardson, C.; Bottoms, L.; Allan, R. The efficacy of a tart cherry drink for the treatment of patellofemoral pain in recreationally active individuals: A placebo randomized control trial. Sport Sci. Health 2002, 18, 1491–1504. [Google Scholar] [CrossRef]
- Sinclair, J.; Bottoms, L.; Dillon, S.; Allan, R.; Shadwell, G.; Butters, B. Effects of montmorency tart cherry and blueberry juice on cardiometabolic and other health-related outcomes: A three-arm placebo randomized controlled trial. Int. J. Environ. Res. Public Health 2022, 19, 5317. [Google Scholar] [CrossRef]
- Krousel-Wood, M.A.; Berger, L.; Jiang, X.; Blonde, L.; Myers, L.; Webber, L. Does home-based exercise improve body mass index in patients with type 2 diabetes?: Results of a feasibility trial. Diabetes Res. Clin. Pract. 2008, 79, 230–236. [Google Scholar] [CrossRef]
- Plotnikoff, R.C.; Eves, N.; Jung, M.; Sigal, R.J.; Padwal, R.; Karunamuni, N. Multicomponent, home-based resistance training for obese adults with type 2 diabetes: A randomized controlled trial. Int. J. Obes. 2010, 34, 1733–1741. [Google Scholar] [CrossRef] [Green Version]
- Mustapa, A.; Justine, M.; Latir, A.A.; Manaf, H. Home-based physical activity in patients with type 2 diabetes mellitus: A scoping review. Ann. Rehabil. Med. 2022, 45, 345–358. [Google Scholar] [CrossRef]
- Bădescu, S.V.; Tătaru, C.; Kobylinska, L.; Georgescu, E.L.; Zahiu, D.M.; Zăgrean, A.M.; Zăgrean, L. The association between diabetes mellitus and depression. J. Med. Life 2016, 9, 120–125. [Google Scholar]
- Gonzalez, J.S.; Peyrot, M.; McCarl, L.A.; Collins, E.M.; Serpa, L.; Mimiaga, M.J.; Safren, S.A. Depression and diabetes treatment nonadherence: A meta-analysis. Diabetes Care 2008, 31, 2398–2403. [Google Scholar] [CrossRef] [Green Version]
- Baumeister, H.; Hutter, N.; Bengel, J.; Härter, M. Quality of life in medically ill persons with comorbid mental disorders: A systematic review and meta-analysis. Psychother. Psychosom. 2011, 80, 275–286. [Google Scholar] [CrossRef]
- Egede, L.E.; Nietert, P.J.; Zheng, D. Depression and all-cause and coronary heart disease mortality among adults with and without diabetes. Diabetes Care 2005, 28, 1339–1345. [Google Scholar] [CrossRef] [Green Version]
- Craft, L.L.; Perna, F.M. The benefits of exercise for the clinically depressed. Prim. Care Companion J. Clin. Psychiatry 2004, 6, 104–111. [Google Scholar] [CrossRef] [Green Version]
- Ley, S.H.; Hamdy, O.; Mohan, V.; Hu, F.B. Prevention and management of type 2 diabetes: Dietary components and nutritional strategies. Lancet 2014, 383, 1999–2007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shim, J.S.; Oh, K.; Kim, H.C. Dietary assessment methods in epidemiologic studies. Epidemiol. Health 2014, 36, e2014009. [Google Scholar] [CrossRef] [PubMed] [Green Version]

| Stage | Resistance Exercises | Duration | Equipment |
|---|---|---|---|
| 1 (weeks 1–4) | Squat Lunge Press-Up Cross Body Reach Reverse Fly Lateral Raise Biceps Curl Triceps Extension Frontal Raise Bridge | Rest for 30′s between each type of TheraBand exercise. Rest for 2 min before repeating the stage again. Sets: 2, Repetitions: 10–12 | Latex free resistance band |
| 2 (weeks 5–8) | Rest for 30 s between each type of TheraBand exercise. Rest for 2 min before repeating the stage again. Sets: 2, Repetitions: 15 | Latex free resistance band | |
| 3 (weeks 9–12) | Rest for 30 s between each type of TheraBand exercise. Rest for 2 min before repeating the stage again. Sets: 3, Repetitions: 10–15 | Latex free resistance band |
| Sunday | Monday | Tuesday | Wednesday | Thursday | Friday | Saturday |
|---|---|---|---|---|---|---|
| Resistance Exercise | Resistance Exercise | |||||
| Walking (+2500 over daily step count) | Walking (+2500 over daily step count) | Walking (+2500 over daily step count) | Walking (+2500 over daily step count) | Walking (+2500 over daily step count) | Walking (+2500 over daily step count) | Walking (+2500 over daily step count) |
| Control | Home Based Physical Activity | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | 12-Weeks | Follow-Up | Baseline | 12-Weeks | Follow-Up | |||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| Waist circumference (cm) | 94.24 | 19.33 | 97.22 | 13.63 | 104.60 | 20.31 | 99.93 | 8.40 | 100.65 | 10.03 | 101.04 | 10.71 |
| Waist-to-hip ratio | 0.99 | 0.11 | 1.00 | 0.11 | 1.03 | 0.17 | 0.98 | 0.06 | 0.98 | 0.06 | 0.98 | 0.07 |
| Systolic blood pressure (mmHg) | 132.87 | 14.76 | 131.58 | 9.34 | 131.73 | 8.51 | 121.80 | 15.61 | 124.11 | 15.76 | 129.56 | 13.78 |
| Diastolic blood pressure (mmHg) | 80.27 | 9.83 | 78.50 | 10.31 | 79.13 | 7.75 | 82.72 | 13.32 | 78.37 | 9.46 | 81.56 | 11.34 |
| Chester step test (Stages) | 2.71 | 0.73 | 3.29 | 1.16 | 3.33 | 0.62 | 3.00 | 0.77 | 3.28 | 1.28 | 3.54 | 0.71 |
| WHO-5 | 72.39 | 21.23 | 70.77 | 21.76 | 74.93 | 27.19 | 68.75 | 17.64 | 72.74 | 19.12 | 78.31 | 16.94 |
| PHQ-9 | 6.81 | 5.10 | 5.73 | 5.14 | 8.53 | 4.37 | 6.84 | 2.71 | 5.96 | 3.48 | 5.00 | 3.53 |
| PAID | 22.10 | 15.56 | 21.49 | 19.21 | 15.83 | 14.11 | 21.33 | 13.70 | 19.26 | 20.06 | 17.12 | 19.29 |
| PSQI | 9.10 | 3.08 | 7.85 | 2.98 | 9.93 | 3.63 | 10.56 | 4.10 | 9.56 | 3.36 | 8.22 | 3.79 |
| Control | Home Based Physical Activity | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | 12-Weeks | Follow-Up | Baseline | 12-Weeks | Follow-Up | |||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| Glucose (mg/dL) | 181.63 | 111.44 | 151.00 | 54.93 | 155.07 | 97.19 | 157.47 | 69.68 | 151.93 | 61.11 | 162.36 | 61.97 |
| LDL cholesterol (mg/dL) | 145.59 | 43.10 | 130.08 | 35.38 | 130.00 | 28.14 | 152.69 | 45.72 | 122.29 | 43.79 | 129.29 | 40.38 |
| HDL cholesterol (mg/dL) | 55.17 | 31.56 | 46.42 | 13.67 | 47.73 | 9.86 | 57.03 | 15.66 | 49.14 | 11.71 | 54.96 | 15.36 |
| Total cholesterol (mg/dL) | 228.43 | 46.75 | 204.65 | 39.52 | 204.47 | 27.03 | 247.84 | 51.36 | 195.00 | 51.51 | 207.07 | 48.04 |
| Triglycerides (mg/dL) | 146.10 | 84.23 | 142.85 | 90.05 | 160.48 | 61.19 | 129.32 | 59.15 | 117.64 | 57.80 | 144.06 | 70.72 |
| HbA1c (%) | 8.71 | 1.39 | 8.35 | 1.32 | 8.72 | 1.79 | 8.32 | 1.76 | 8.06 | 1.81 | 8.39 | 1.85 |
| TyG index | 9.25 | 0.75 | 9.12 | 0.57 | 9.26 | 0.68 | 9.05 | 0.66 | 8.93 | 0.69 | 9.20 | 0.61 |
| Total cholesterol:HDL cholesterol ratio | 4.68 | 1.50 | 4.72 | 1.53 | 4.43 | 0.99 | 4.64 | 1.48 | 4.14 | 1.28 | 3.96 | 1.26 |
| LDL cholesterol:HDL cholesterol ratio | 3.03 | 1.21 | 2.93 | 1.07 | 2.81 | 0.74 | 2.92 | 1.26 | 2.63 | 1.09 | 2.55 | 1.06 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sinclair, J.; Ageely, H.; Mahfouz, M.S.; Hummadi, A.A.; Darraj, H.; Solan, Y.; Allan, R.; Bahsan, F.; Hafaf, H.A.; Abohadash, A.; et al. Effects of a Home-Based Physical Activity Program on Blood Biomarkers and Health-Related Quality of Life Indices in Saudi Arabian Type 2 Diabetes Mellitus Patients: A Randomized Controlled Trial. Life 2023, 13, 1413. https://doi.org/10.3390/life13061413
Sinclair J, Ageely H, Mahfouz MS, Hummadi AA, Darraj H, Solan Y, Allan R, Bahsan F, Hafaf HA, Abohadash A, et al. Effects of a Home-Based Physical Activity Program on Blood Biomarkers and Health-Related Quality of Life Indices in Saudi Arabian Type 2 Diabetes Mellitus Patients: A Randomized Controlled Trial. Life. 2023; 13(6):1413. https://doi.org/10.3390/life13061413
Chicago/Turabian StyleSinclair, Jonathan, Hussein Ageely, Mohamed Salih Mahfouz, Abdulrahman Ahmed Hummadi, Hussain Darraj, Yahia Solan, Robert Allan, Fatma Bahsan, Hassan AL Hafaf, Ali Abohadash, and et al. 2023. "Effects of a Home-Based Physical Activity Program on Blood Biomarkers and Health-Related Quality of Life Indices in Saudi Arabian Type 2 Diabetes Mellitus Patients: A Randomized Controlled Trial" Life 13, no. 6: 1413. https://doi.org/10.3390/life13061413