
Deciphering Lung Adenocarcinoma Heterogeneity: An Overview of Pathological and Clinical Features of Rare Subtypes

 , , ,
, , ,
Abstract
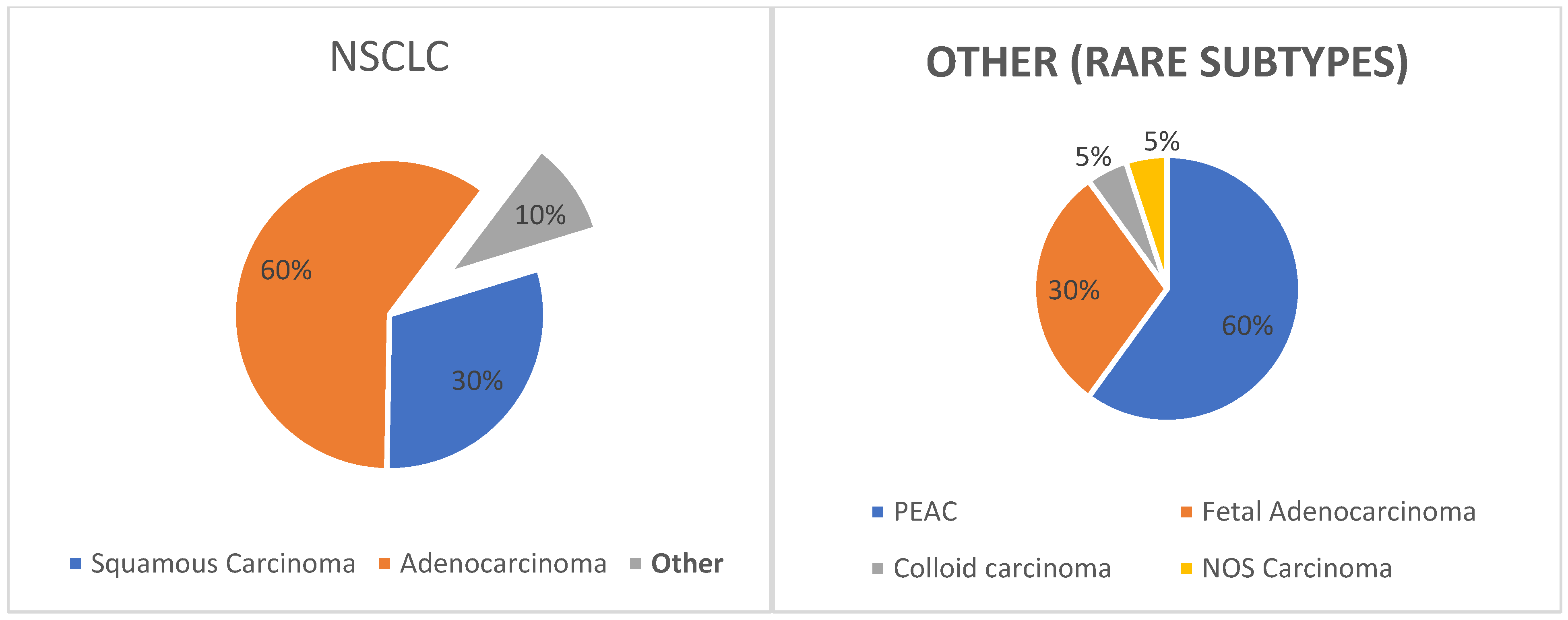
:1. Introduction
2. Methods
3. Pulmonary Enteric Adenocarcinoma
3.1. Epidemiology
3.2. Clinical Characteristics
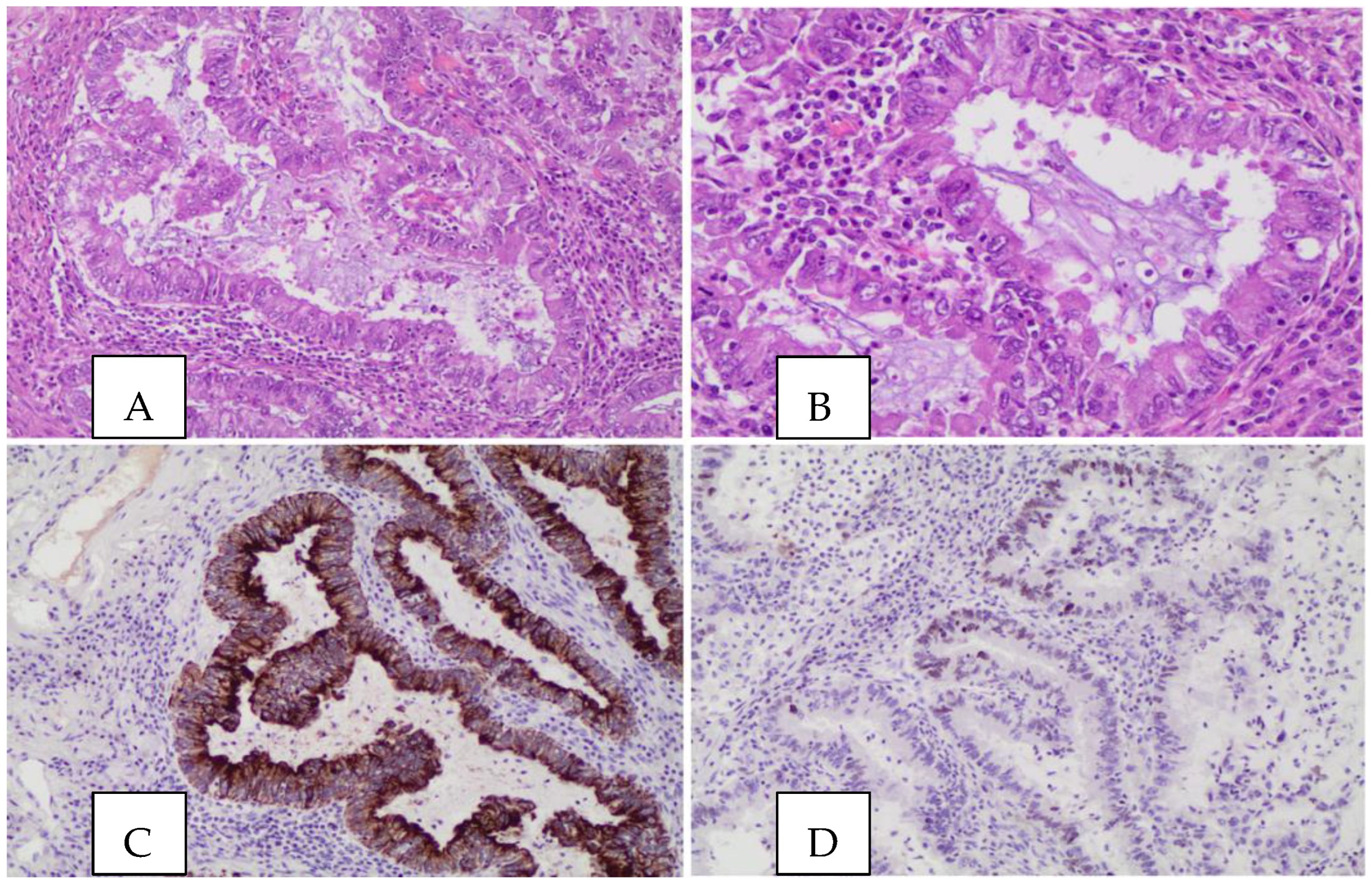
3.3. Morphology and Immunochemistry
3.4. Molecular Pathology
3.5. Treatment Strategies
4. Fetal Adenocarcinoma
5. Colloid Adenocarcinoma
6. NOS Carcinoma
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mao, Y.; Yang, D.; He, J.; Krasna, M.J. Epidemiology of Lung Cancer. Surg. Oncol. Clin. N. Am. 2016, 25, 439–445. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- Howlader, N.; Forjaz, G.; Mooradian, M.J.; Meza, R.; Kong, C.Y.; Cronin, K.A.; Mariotto, A.B.; Lowy, D.R.; Feuer, E.J. The Effect of Advances in Lung-Cancer Treatment on Population Mortality. N. Engl. J. Med. 2020, 383, 640–649. [Google Scholar] [CrossRef] [PubMed]
- Malvezzi, M.; Santucci, C.; Boffetta, P.; Collatuzzo, G.; Levi, F.; La Vecchia, C.; Negri, E. European cancer mortality predictions for the year 2023 with focus on lung cancer. Ann. Oncol. 2023, 34, 410–419. [Google Scholar] [CrossRef] [PubMed]
- Stapelfeld, C.; Dammann, C.; Maser, E. Sex-specificity in lung cancer risk. Int. J. Cancer 2020, 146, 2376–2382. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.; Schiller, J.H.; Gazdar, A.F. Lung cancer in never smokers—A different disease. Nat. Rev. Cancer 2007, 7, 778–790. [Google Scholar] [CrossRef]
- Malhotra, J.; Malvezzi, M.; Negri, E.; La Vecchia, C.; Boffetta, P. Risk factors for lung cancer worldwide. Eur. Respir. J. 2016, 48, 889–902. [Google Scholar] [CrossRef]
- Thai, A.A.; Solomon, B.J.; Sequist, L.V.; Gainor, J.F.; Heist, R.S. Lung cancer. Lancet 2021, 398, 535–554. [Google Scholar] [CrossRef]
- Travis, W.D.; Brambilla, E.; Nicholson, A.G.; Yatabe, Y.; Austin, J.H.M.; Beasley, M.B.; Chirieac, L.R.; Dacic, S.; Duhig, E.; Flieder, D.B.; et al. The 2015 World Health Organization Classification of Lung Tumors. J. Thorac. Oncol. 2015, 10, 1243–1260. [Google Scholar] [CrossRef]
- Gong, J.; Fan, Y. Pulmonary enteric adenocarcinoma. Transl. Oncol. 2021, 14, 101123. [Google Scholar] [CrossRef]
- Bose, P.; Shaffi, M.Z.; Raizada, N.; Vanere, V.; Sharma, K. Pulmonary Enteric Adenocarcinoma Lung-Case Series and Approach to Diagnosis. Ann. Case Rep. 2022, 7, 818. [Google Scholar] [CrossRef]
- Zhao, L.; Huang, S. Clinicopathological, radiographic, and oncogenic features of primary pulmonary enteric adenocarcinoma in comparison with invasive adenocarcinoma in resection specimens. Medicine 2017, 96, e8153. [Google Scholar] [CrossRef] [PubMed]
- Okada, F.; Takeda, M. Clinicopathological and genetic analyses of pulmonary enteric adenocarcinoma. J. Clin. Pathol. 2022. [Google Scholar] [CrossRef]
- Xie, M.; Chen, D.; Li, Y.; Liu, X.; Kuang, D.; Li, X. Genetic mutation profiles and immune microenvironment analysis of pulmonary enteric adenocarcinoma. Diagn. Pathol. 2022, 17, 30. [Google Scholar] [CrossRef] [PubMed]
- Matsushima, J. Clinicopathological, immunohistochemical, and mutational analyses of pulmonary enteric adenocarcinoma: Usefulness of SATB2 and β -catenin immunostaining for differentiation from metastatic colorectal carcinoma. Hum. Pathol. 2017, 64, 179–185. [Google Scholar] [CrossRef]
- Li, H.; Cao, W. Pulmonary enteric adenocarcinoma: A literature review. J. Thorac. Dis. 2020, 12, 3217–3226. [Google Scholar] [CrossRef]
- Satoh, Y.; Hoshi, R. Cytology of Pulmonary Adenocarcinomas Showing Enteric Differentiation. Acta Cytol. 2006, 50, 250–256. [Google Scholar] [CrossRef]
- Palmirotta, R.; Lovero, D. Pulmonary enteric adenocarcinoma: An overview. Expert Rev. Mol. Med. 2020, 22, e1. [Google Scholar] [CrossRef]
- Caliò, A.; Lever, V. Increased frequency of bronchiolar histotypes in lung carcinomas associated with idiopathic pulmonary fibrosis. Histopathology 2017, 71, 725–735. [Google Scholar] [CrossRef]
- Wang, C.-X.; Liu, B. Pulmonary enteric adenocarcinoma: A study of the clinicopathologic and molecular status of nine cases. Int. J. Clin. Exp. Pathol. 2014, 7, 1266–1274. [Google Scholar]
- Todisco, A.; Internò, V. Cutaneous metastasis as a primary presentation of a pulmonary enteric adenocarcinoma. Int. J. Biol. Mrk. 2019, 34, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.-W.; Xu, Z.-H. Pulmonary enteric adenocarcinoma with pancreatic metastasis: A case report. Oncol. Lett. 2017, 13, 4651–4656. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Liu, P. Distinctive features of immunostaining and mutational load in primary pulmonary enteric adenocarcinoma: Implications for differential diagnosis and immunotherapy. J. Transl. Med. 2018, 16, 81. [Google Scholar] [CrossRef]
- Jurmeister, P.; Schöler, A. DNA methylation profiling reliably distinguishes pulmonary enteric adenocarcinoma from metastatic colorectal cancer. Mod. Pathol. 2019, 32, 855–865. [Google Scholar] [CrossRef]
- Ueno, T.; Linder, S. Aspartic proteinase napsin is a useful marker for diagnosis of primary lung adenocarcinoma. Br. J. Cancer 2003, 88, 1229–1233. [Google Scholar] [CrossRef]
- Hu, C.-H.; Shi, S. Hyperprogressive Disease After Immunotherapy: A Case Report of Pulmonary Enteric Adenocarcinoma. Front. Oncol. 2022, 12, 799549. [Google Scholar] [CrossRef]
- Zhang, J.; Xiang, C. Differential diagnosis of pulmonary enteric adenocarcinoma and metastatic colorectal carcinoma with the assistance of next-generation sequencing and immunohistochemistry. J. Cancer Res. Clin. Oncol. 2019, 145, 269–279. [Google Scholar] [CrossRef] [PubMed]
- Zuo, Y.; Zhong, J. Genomic and epigenomic profiles distinguish pulmonary enteric adenocarcinoma from lung metastatic colorectal cancer. EBioMedicine 2022, 82, 104165. [Google Scholar] [CrossRef]
- Chang, J.C.; Offin, M. Comprehensive Molecular and Clinicopathologic Analysis of 200 Pulmonary Invasive Mucinous Adenocarcinomas Identifies Distinct Characteristics of Molecular Subtypes. Clin. Cancer Res. 2021, 27, 4066–4076. [Google Scholar] [CrossRef]
- Sugano, M.; Nagasaka, T. HNF4α as a Marker for Invasive Mucinous Adenocarcinoma of the Lung. Am. J. Surg. Pathol. 2013, 37, 211–218. [Google Scholar] [CrossRef]
- Awad, M.M.; Gadgeel, S.M. Long-Term Overall Survival From KEYNOTE-021 Cohort G: Pemetrexed and Carboplatin with or Without Pembrolizumab as First-Line Therapy for Advanced Nonsquamous NSCLC. J. Thorac. Oncol. 2021, 16, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Kodama, T.; Shimosato, Y. Six cases of well-differentiated adenocarcinoma simulating fetal lung tubules in pseudoglandular stage. Am. J. Surg. Pathol. 1984, 8, 735–744. [Google Scholar] [CrossRef] [PubMed]
- Geisinger, K.R.; Travis, W.D. Aspiration Cytomorphology of Fetal Adenocarcinoma of the Lung. Am. J. Clin. Pathol. 2010, 134, 894–902. [Google Scholar] [CrossRef] [PubMed]
- Hakiri, S.; Fukui, T. Well-differentiated fetal adenocarcinoma of the lung: Positron emission tomography features and diagnostic difficulties in frozen section analysis—A case report. Surg. Case Rep. 2020, 6, 152. [Google Scholar] [CrossRef]
- Patnayak, R.; Jena, A. Well-differentiated fetal adenocarcinoma of the lung in an adult male: Report of an unusual tumor with a brief review of literature. J. Cancer Res. Ther. 2014, 10, 419. [Google Scholar] [CrossRef]
- Atoini, F.; Ouarssani, A. A well-differentiated fetal adenocarcinoma of the lung with early local recurrence after limited resection. Thorac. Cancer 2011, 2, 123–127. [Google Scholar] [CrossRef]
- Kalhor, N. Colloid carcinoma of the lung: Current views. Semin. Diagn. Pathol. 2014, 31, 265–270. [Google Scholar] [CrossRef]
- Zenali, M.J.; Weissferdt, A. An update on clinicopathological, immunohistochemical, and molecular profiles of colloid carcinoma of the lung. Hum. Pathol. 2015, 46, 836–842. [Google Scholar] [CrossRef]
- Rossi, G.; Murer, B. Primary Mucinous (So-called Colloid) Carcinomas of the Lung. Am. J. Surg. Pathol. 2004, 28, 442–452. [Google Scholar] [CrossRef]
- Ou, S.-H.I.; Zell, J.A. Carcinoma NOS is a Common Histologic Diagnosis and is Increasing in Proportion Among Non-small Cell Lung Cancer Histologies. J. Thorac. Oncol. 2009, 4, 1202–1211. [Google Scholar] [CrossRef]
- Tane, S.; Nishio, W. Clinical significance of the ‘not otherwise specified’ subtype in candidates for resectable non-small cell lung cancer. Oncol. Lett. 2014, 8, 1017–1024. [Google Scholar] [CrossRef] [PubMed]
- Righi, L.; Vavalà, T. Impact of Non–Small-Cell Lung Cancer-Not Otherwise Specified Immunophenotyping on Treatment Outcome. J. Thorac. Oncol. 2014, 9, 1540–1546. [Google Scholar] [CrossRef] [PubMed]
- Ota, T.; Kirita, K. Validity of using immunohistochemistry to predict treatment outcome in patients with non-small cell lung cancer not otherwise specified. J. Cancer Res. Clin. Oncol. 2019, 145, 2495–2506. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Subtypes | Epidemiology | Gender | Smoking Status | IHC | Molecular Pathology | Treatment |
|---|---|---|---|---|---|---|
| PEAC | 0.5% | Males > females | Smokers | CK7, CDX-2, villin | KRAS G12V, ERBB2, EGFR (del ex19 and L8S8R) | Surgery/systemic treatment ** |
| Fetal adenocarcinoma | 0.5% | Young females * | Smokers | Synaptophysin, vimentin | WNT signal | Surgery *** |
| Colloid carcinoma | 0.1% | Females > males | Smokers | CK7, CDX-2, CK20, MUC2 | KRAS codons 12 and 13 | Surgery/systemic treatment |
| NOS carcinoma | 0.1% | Males > females | Unknown | TTF-1 and p40 or none **** | EGFR and ALK-EML4 | Systemic treatment |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mogavero, A.; Bironzo, P.; Righi, L.; Merlini, A.; Benso, F.; Novello, S.; Passiglia, F. Deciphering Lung Adenocarcinoma Heterogeneity: An Overview of Pathological and Clinical Features of Rare Subtypes. Life 2023, 13, 1291. https://doi.org/10.3390/life13061291
Mogavero A, Bironzo P, Righi L, Merlini A, Benso F, Novello S, Passiglia F. Deciphering Lung Adenocarcinoma Heterogeneity: An Overview of Pathological and Clinical Features of Rare Subtypes. Life. 2023; 13(6):1291. https://doi.org/10.3390/life13061291
Chicago/Turabian StyleMogavero, Andrea, Paolo Bironzo, Luisella Righi, Alessandra Merlini, Federica Benso, Silvia Novello, and Francesco Passiglia. 2023. "Deciphering Lung Adenocarcinoma Heterogeneity: An Overview of Pathological and Clinical Features of Rare Subtypes" Life 13, no. 6: 1291. https://doi.org/10.3390/life13061291